Living-Donor Liver Transplantation for Hepatocellular Carcinoma: Impact of the MELD Score and Predictive Value of NLR on Survival

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Population
2.2. Liver Transplantation Protocol
2.3. Clinical Outcomes Assessment
2.4. Statistical Analysis
3. Results
3.1. Demographics of the Enrolled Recipients
3.2. Prognostic Factors Affecting Post-LT Outcomes
3.3. Comparisons of the Characteristics between the High and the Low MELD Score Groups
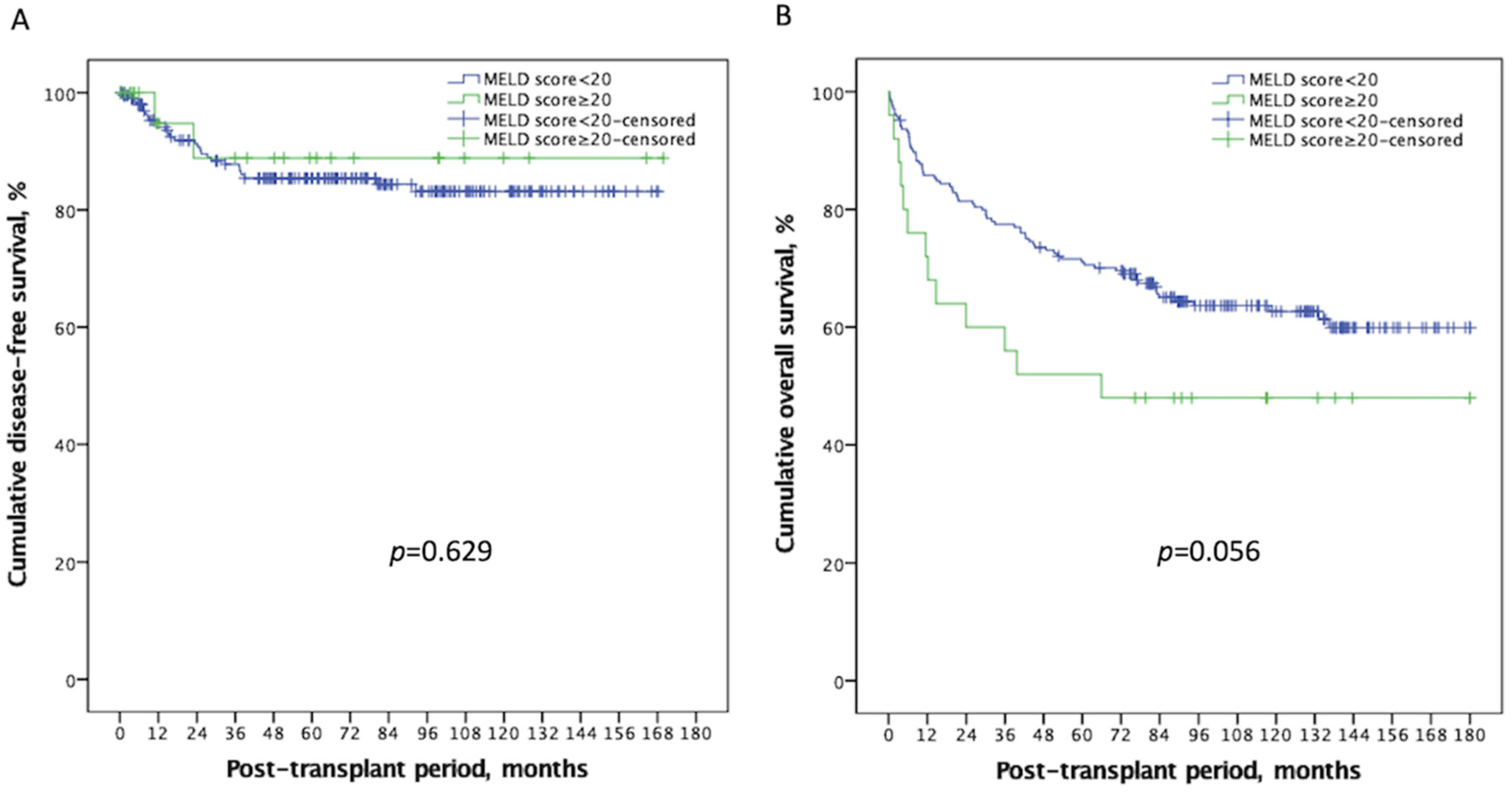
3.4. Comparisons of Clinical Outcomes between the High and the Low MELD Score Groups
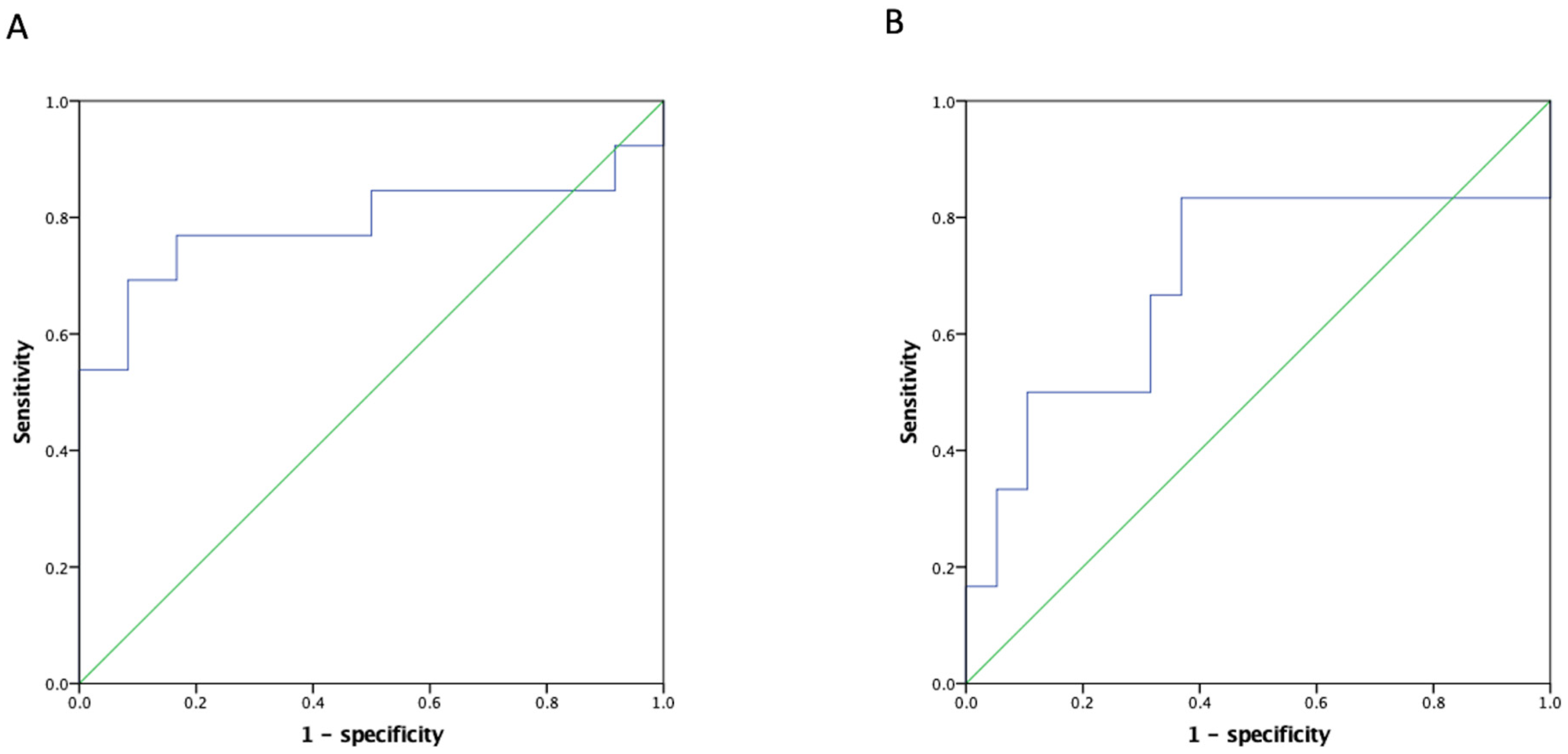
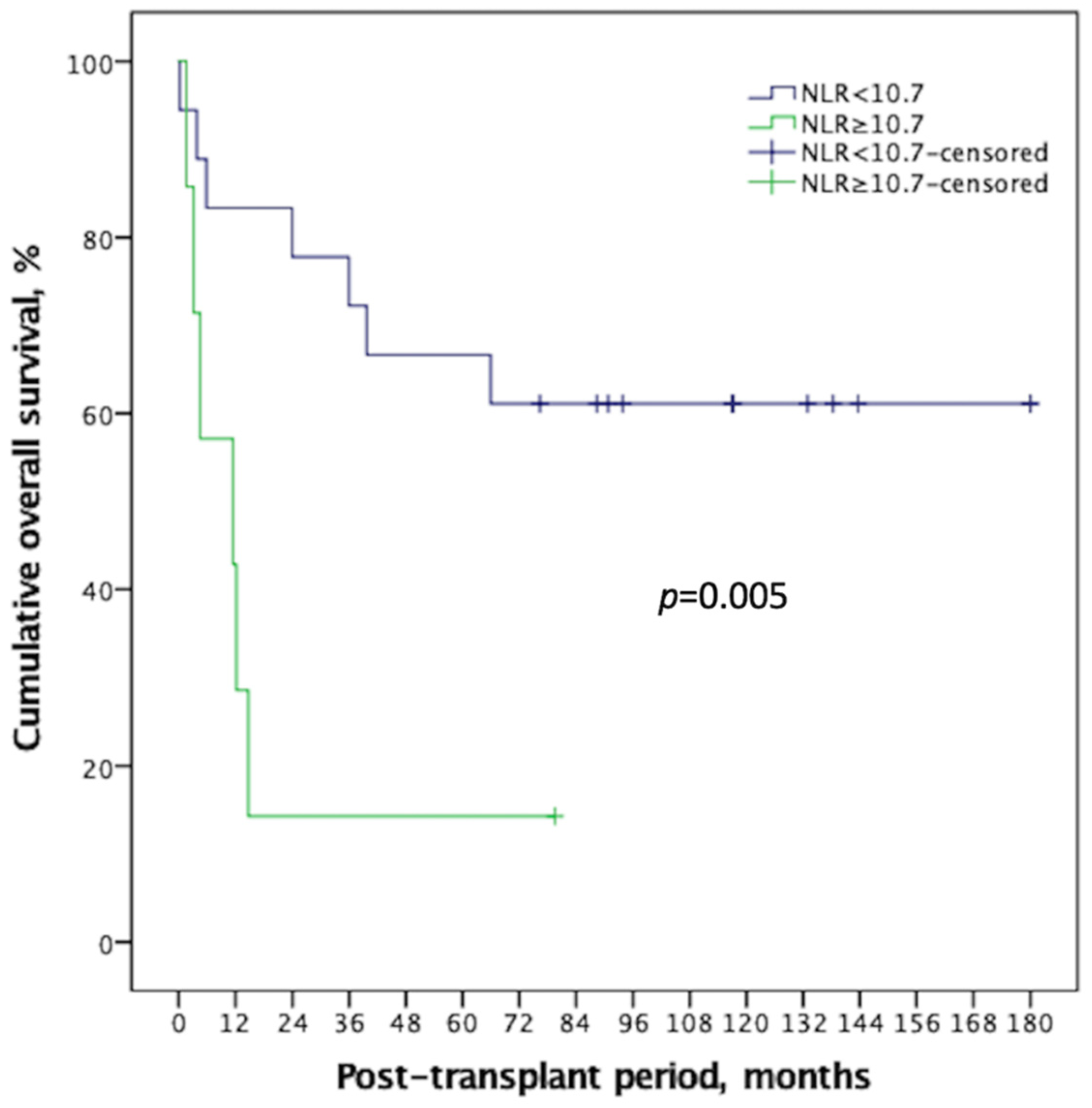
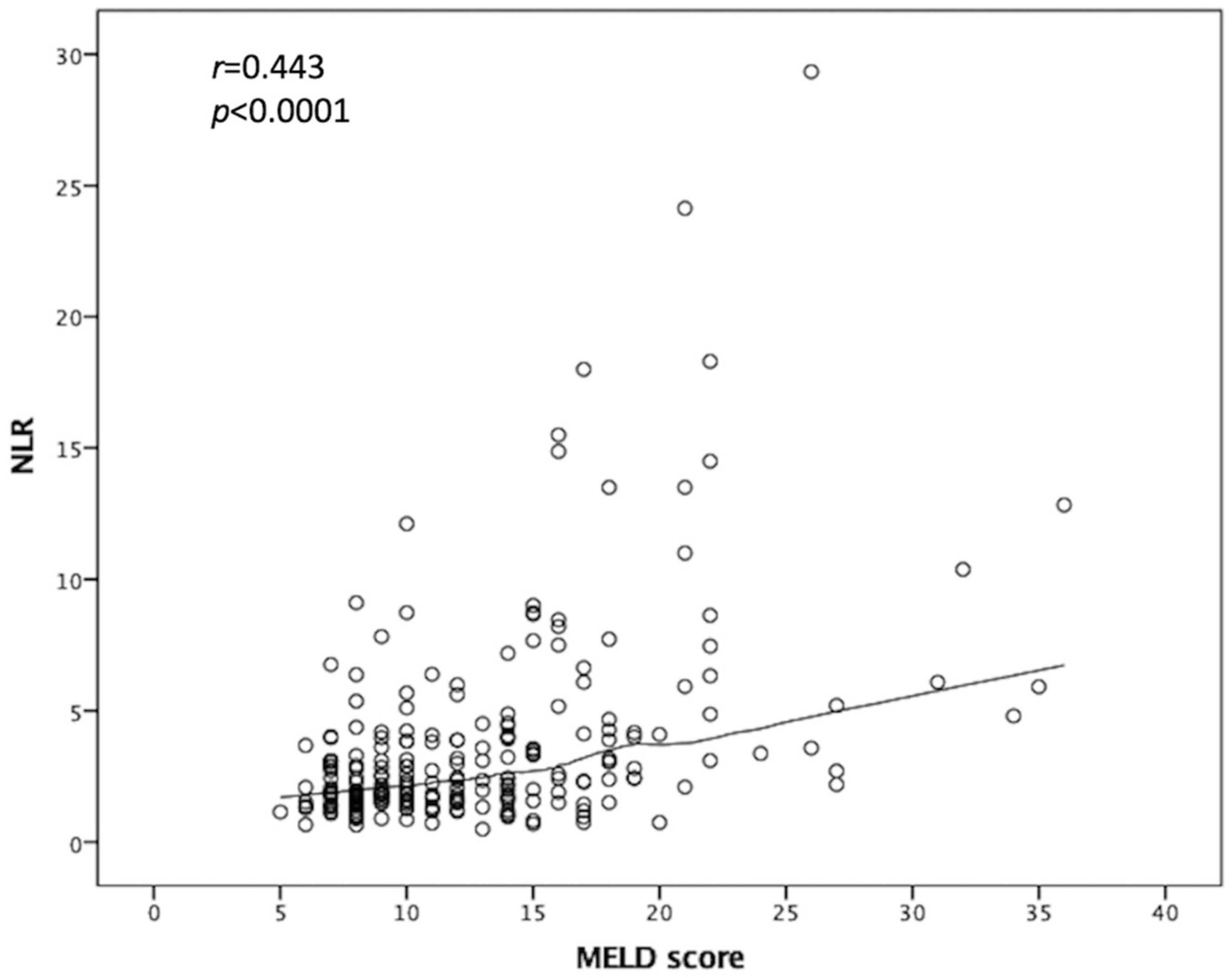
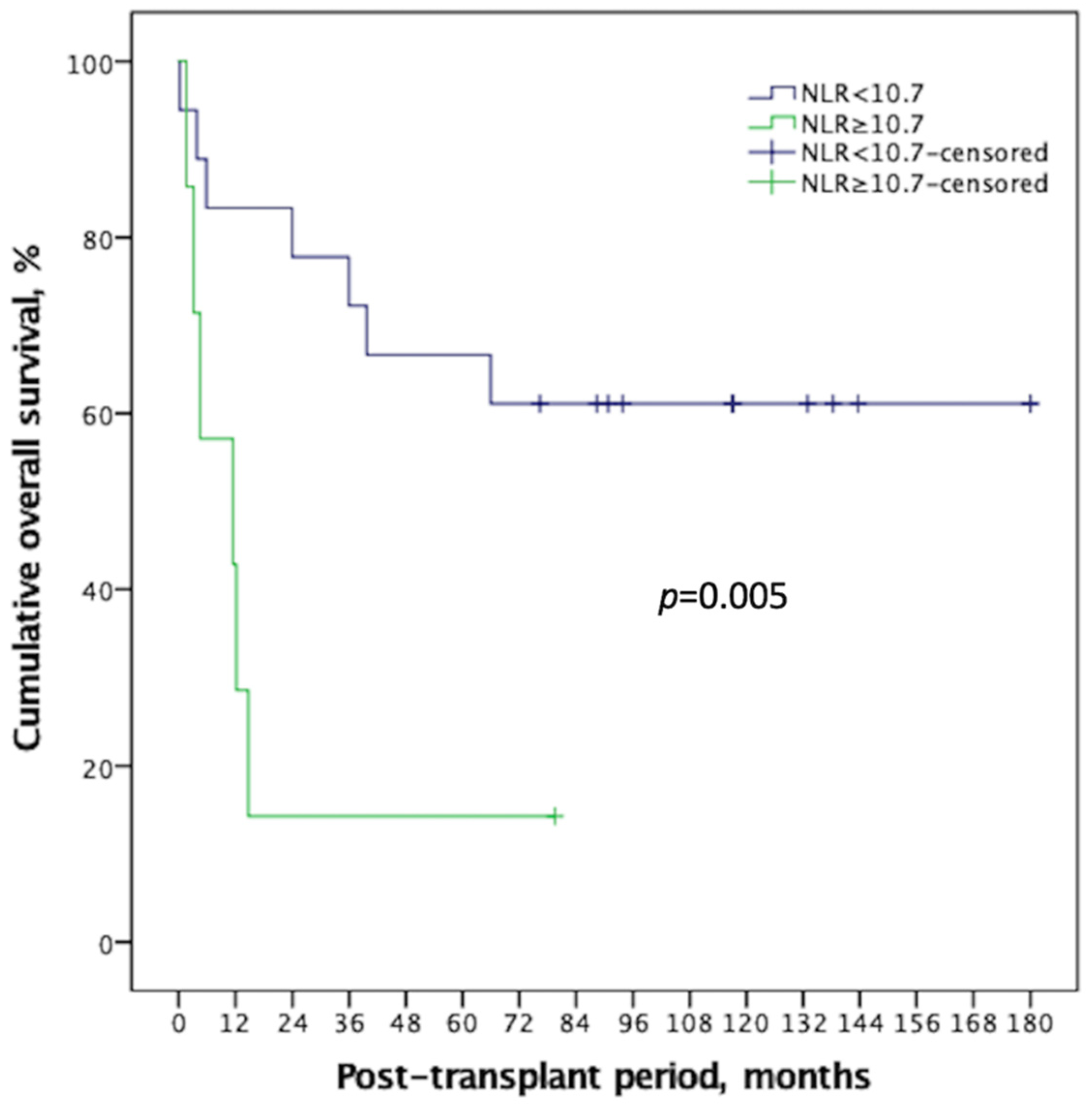
3.5. Impact of NLR Affecting Outcomes in HCC Recipients with MELD Score ≥ 20
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ALT | alanine aminotransferase |
| AST | aspartate aminotransferase |
| AUROC | area under the receiver operating characteristic curve |
| CMV | cytomegalovirus |
| DFS | disease-free survival |
| GRWR | graft-to-recipient weight ratio |
| HCC | hepatocellular carcinoma |
| LDLT | living-donor liver transplantation |
| LT | liver transplantation |
| MELD | Model of End-Stage Liver Disease |
| NLR | neutrophil-to-lymphocyte ratio |
| OS | overall survival |
| ROC | receiver operating characteristic |
| UCSF | University of California San Francisco |
References
- Mazzaferro, V.M.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Watson, J.J.; Bacchetti, P.; Venook, A.; Ascher, N.L.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: Expansion of the tumor size limits does not adversely impact survival. Hepatology 2001, 33, 1394–1403. [Google Scholar] [CrossRef] [PubMed]
- Herrero, J.I.; Sangro, B.; Quiroga, J.; Pardo, F.; Herraiz, M.; Cienfuegos, J.A.; Prieto, J. Influence of tumor characteristics on the outcome of liver transplantation among patients with liver cirrhosis and hepatocellular carcinoma. Liver Transplant. 2001, 7, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Marsh, J.; Dvorchik, I. Liver organ allocation for hepatocellular carcinoma: Are we sure? Liver Transplant. 2003, 9, 693–696. [Google Scholar] [CrossRef]
- Yadav, S.K.; Saraf, N.; Saigal, S.; Choudhary, N.S.; Goja, S.; Rastogi, A.; Bhangui, P.; Soin, A.S. High MELD score does not adversely affect outcome of living donor liver transplantation: Experience in 1000 recipients. Clin. Transplant. 2017, 31, e13006. [Google Scholar] [CrossRef]
- Selzner, M.; Kashfi, A.; Cattral, M.S.; Selzner, N.; McGilvray, I.D.; Greig, P.D.; Levy, G.A.; Renner, E.L.; Grant, D.R. Live Donor Liver Transplantation in High MELD Score Recipients. Ann. Surg. 2010, 251, 153–157. [Google Scholar] [CrossRef]
- Wang, Z.-X.; Yan, L.-N.; Wang, W.-T.; Xu, M.-Q.; Yang, J.-Y. Impact of Pretransplant MELD Score on Posttransplant Outcome in Orthotopic Liver Transplantation for Patients with Acute-on-Chronic Hepatitis B Liver Failure. Transplant. Proc. 2007, 39, 1501–1504. [Google Scholar] [CrossRef]
- Marubashi, S.; Dono, K.; Asaoka, T.; Hama, N.; Gotoh, K.; Miyamoto, A.; Takeda, Y.; Nagano, H.; Umeshita, K.; Monden, M. Risk Factors for Graft Dysfunction After Adult-to-Adult Living Donor Liver Transplantation. Transplant. Proc. 2006, 38, 1407–1410. [Google Scholar] [CrossRef]
- Oberkofler, C.E.; Dutkowski, P.; Stocker, R.; Schuepbach, R.A.; Stover, J.F.; Clavien, P.-A.; Béchir, M. Model of end stage liver disease (MELD) score greater than 23 predicts length of stay in the ICU but not mortality in liver transplant recipients. Crit. Care 2010, 14, R117. [Google Scholar] [CrossRef] [Green Version]
- Foxton, M.R.; Al-Freah, M.A.B.; Portal, A.J.; Sizer, E.; Bernal, W.; Auzinger, G.; Rela, M.; Wendon, J.A.; Heaton, N.D.; O’Grady, J.G.; et al. Increased model for end-stage liver disease score at the time of liver transplant results in prolonged hospitalization and overall intensive care unit costs. Liver Transplant. 2010, 16, 668–677. [Google Scholar] [CrossRef]
- Harding-Theobald, E.; Yao, F.Y.; Mehta, N. Neutrophil-to-Lymphocyte Ratio Predicts High-Risk Explant Features and Waitlist Survival But Is Not Independently Associated With Recurrence or Survival Following Liver Transplantation for Hepatocellular Carcinoma. Liver Transplant. 2021, 27, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Lee, S.-H.; Gwak, M.S.; Ko, J.S.; Han, S.; Choi, G.-S.; Joh, J.W.; Kim, J.; Kim, G.S. Association between neutrophil–lymphocyte ratio change during living donor liver transplantation and graft survival. Sci. Rep. 2021, 11, 4199. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Choi, Y.; Cho, J.Y.; Yoon, Y.-S.; Han, H.-S. Neutrophil-to-lymphocyte ratio predicts early acute cellular rejection in living donor liver transplantation. Ann. Surg. Treat. Res. 2020, 99, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.-Y.; Zhou, L.; Geng, L.; Zheng, Z.-Y.; Jia, J.-J.; Zhang, J.; Yao, J.; Zheng, S.-S. High neutrophil-lymphocyte ratio indicates poor prognosis for acute-on-chronic liver failure after liver transplantation. World J. Gastroenterol. 2015, 21, 3317–3324. [Google Scholar] [CrossRef] [PubMed]
- Aranzana, E.; Coppini, A.; Ribeiro, M.; Massarollo, P.; Szutan, L.; Ferreira, F. Model for End-Stage Liver Disease, Model for Liver Transplantation Survival and Donor Risk Index as predictive models of survival after liver transplantation in 1006 patients. Clinics 2015, 70, 413–418. [Google Scholar] [CrossRef]
- Templeton, A.J.; Mcnamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Solid Tumors: A Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [Green Version]
- Zahorec, R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl Lek List. 2021, 122, 474–488. [Google Scholar] [CrossRef]
- Wu, T.-J.; Dahiya, D.; Lee, C.-S.; Lee, C.-F.; Chou, H.-S.; Chan, K.-M.; Lee, W.-C. Impact of portal venous hemodynamics on indices of liver function and graft regeneration after right lobe living donor liver transplantation. Liver Transplant. 2011, 17, 1035–1045. [Google Scholar] [CrossRef]
- Chan, K.-M.; Cheng, C.-H.; Wu, T.-H.; Wu, T.-J.; Chou, H.-S.; Lee, C.-S.; Lee, W.-C. Clinical Strategy for the Reconstruction of Middle Hepatic Vein Tributaries in Right Liver Living Donor Liver Transplantation. World J. Surg. 2014, 38, 2927–2933. [Google Scholar] [CrossRef]
- Lee, C.-F.; Cheng, C.-H.; Wang, Y.-C.; Soong, R.-S.; Wu, T.-H.; Chou, H.-S.; Wu, T.-J.; Chan, K.-M.; Lee, C.-S.; Lee, W.-C. Adult Living Donor Liver Transplantation Across ABO-Incompatibility. Medicine 2015, 94, e1796. [Google Scholar] [CrossRef]
- Ljungman, P.; Boeckh, M.; Hirsch, H.H.; Josephson, F.; Lundgren, J.; Nichols, G.; Pikis, A.; Razonable, R.R.; Miller, V.; Griffiths, P.D. Definitions of Cytomegalovirus Infection and Disease in Transplant Patients for Use in Clinical Trials. Clin. Infect. Dis. 2017, 64, 87–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, H.; Hsu, P.; Lee, J.; Wang, Y.; Cheng, C.H.; Wu, T.-J.; Wu, T.-H.; Chou, H.; Chan, K.; Lee, W.; et al. Plasma cytomegalovirus DNA load predicts outcomes in liver transplant recipients. Immun. Inflamm. Dis. 2021, 9, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Bouami, S.F.; Gwiasda, J.; Beneke, J.; Kaltenborn, A.; Liersch, S.; Suero, E.M.; Koch, H.-F.; Krauth, C.; Klempnauer, J.; Schrem, H. Prognostic factors for long-term survival after adult liver transplantation. Langenbecks Arch. Surg. 2018, 403, 495–508. [Google Scholar] [CrossRef]
- Zhang, W.; Wang, W.; Kang, M.; Wu, S.; Liu, Y.; Liao, Q.; Xiao, Y.; Ma, Y.; Xie, Y. Bacterial and Fungal Infections After Liver Transplantation: Microbial Epidemiology, Risk Factors for Infection and Death with Infection. Ann. Transplant. 2020, 25, e921591. [Google Scholar] [CrossRef] [PubMed]
- Candel, F.; Grima, E.; Matesanz, M.; Cervera, C.; Soto, G.; Almela, M.; Martínez, J.; Navasa, M.; Cofán, F.; Ricart, M.; et al. Bacteremia and Septic Shock After Solid-Organ Transplantation. Transplant. Proc. 2005, 37, 4097–4099. [Google Scholar] [CrossRef] [PubMed]
- Wan, Q.; Ye, Q.; Su, T.; Zhou, J. The epidemiology and distribution of pathogens and risk factors for mortality in liver transplant recipients with Gram negative bacteremia. Hepatogastroenterology 2014, 61, 1730–1733. [Google Scholar] [PubMed]
- Klein, K.B.; Stafinski, T.D.; Menon, D. Predicting Survival after Liver Transplantation Based on Pre-Transplant MELD Score: A Systematic Review of the Literature. PLoS ONE 2013, 8, e80661. [Google Scholar] [CrossRef]
- Hoffmann, K.; Hinz, U.; Hillebrand, N.; Radeleff, B.A.; Ganten, T.M.; Schirmacher, P.; Schmidt, J.; Büchler, M.W.; Schemmer, P. Risk factors of survival after liver transplantation for HCC: A multivariate single-center analysis. Clin. Transplant. 2011, 25, E541–E551. [Google Scholar] [CrossRef]
- Pillai, V.G.; Chen, C.-L. Living donor liver transplantation in Taiwan—Challenges beyond surgery. Hepatobiliary Surg. Nutr. 2016, 5, 145–150. [Google Scholar] [CrossRef]
- Howard, R.; Kanetsky, P.A.; Egan, K.M. Exploring the prognostic value of the neutrophil-to-lymphocyte ratio in cancer. Sci. Rep. 2019, 9, 19673. [Google Scholar] [CrossRef] [Green Version]
- Jung, M.R.; Park, Y.K.; Jeong, O.; Seon, J.W.; Ryu, S.Y.; Kim, D.Y.; Kim, Y.J. Elevated preoperative neutrophil to lymphocyte ratio predicts poor survival following resection in late-stage gastric cancer. J. Surg. Oncol. 2011, 104, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Malietzis, G.; Giacometti, M.; Askari, A.; Nachiappan, S.; Kennedy, R.H.; Faiz, O.D.; Aziz, O.; Jenkins, J.T. A Preoperative Neutrophil to Lymphocyte Ratio of 3 Predicts Disease-Free Survival After Curative Elective Colorectal Cancer Surgery. Ann. Surg. 2014, 260, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Fu, Z.; Huang, W.; Huang, K. Prognostic value of neutrophil-to-lymphocyte ratio in sepsis: A meta-analysis. Am. J. Emerg. Med. 2020, 38, 641–647. [Google Scholar] [CrossRef]
- Mouchli, M.; Reddy, S.; Gerrard, M.; Boardman, L.; Rubio, M. Usefulness of neutrophil-to-lymphocyte ratio (NLR) as a prognostic predictor after treatment of hepatocellular carcinoma.” Review article. Ann. Hepatol. 2020, 22, 100249. [Google Scholar] [CrossRef] [PubMed]
- Verna, E.C.; De Martin, E.; Burra, P.; Neri, D.; Gaglio, P.J.; Emond, J.C.; Brown, J.R.S. The Impact of Hepatitis C and Biliary Complications on Patient and Graft Survival Following Liver Transplantation. Am. J. Transplant. 2009, 9, 1398–1405. [Google Scholar] [CrossRef] [PubMed]
- Aguilera, V.; Berenguer, M.; Rubín, A.; San-Juan, F.; Rayón, J.-M.; Prieto, M.; Mir, J. Cirrhosis of mixed etiology (hepatitis C virus and alcohol): Posttransplantation outcome—Comparison with hepatitis C virus-related cirrhosis and alcoholic-related cirrhosis. Liver Transplant. 2009, 15, 79–87. [Google Scholar] [CrossRef]
- Aljumah, A.A.; Kuriry, H.; Faisal, N.; Alghamdi, H. Clinicopathologic characteristics and outcomes of hepatocellular carcinoma associated with chronic hepatitis B versus hepatitis C infection. Ann. Saudi Med. 2018, 38, 358–365. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| General Information of Recipients | MELD < 20, n = 205 | MELD ≥ 20, n = 25 | p-Value |
|---|---|---|---|
| Recipient age, year-old | 55.3 ± 7.4 | 56.8 ± 6.3 | 0.312 |
| Recipient age ≥ 60-year-old | 59 (28.8%) | 10 (40.0%) | 0.248 |
| Recipient sex, male | 169 (82.4%) | 17 (68.0%) | 0.083 |
| Viral hepatitis | 0.018 | ||
| None | 7 (3.4%) | 4 (16.0%) | |
| Chronic HBV infection | 138 (67.3%) | 11 (44.0%) | |
| Chronic HCV infection | 49 (23.9%) | 8 (32.0%) | |
| Co-infection of HBV and HCV | 11 (5.4%) | 2 (8.0%) | |
| Child-Pugh score | 7.3 ± 2.1 | 10.4 ± 1.2 | <0.001 |
| MELD score | 11.4 ± 3.7 | 25.0 ± 5.0 | <0.001 |
| NLR | 3.3 ± 4.0 | 8.4 ± 7.1 | 0.001 |
| NLR ≥ 5 | 29 (14.1%) | 15 (60.0%) | <0.001 |
| Locoregional treatment before LT Curative-intent Bridge therapy Down-staging therapy | 175 (85.4%) 11 (5.4%) 143 (69.8%) 21 (10.2%) | 14 (56.0%) 1 (4.0%) 11 (44.0%) 2 (8.0%) | <0.001 |
| Beyond UCSF criteria, by radiology | 16 (7.8%) | 3 (12.0%) | 0.472 |
| Beyond UCSF criteria, by pathology | 56 (27.3%) | 7 (28.0%) | 0.942 |
| AFP, ng/dL | 13.0 | 9.9 | 0.672 |
| AFP ≥ 200 ng/mL | 29 (14.1%) | 1 (4.0%) | 0.155 |
| Recipient CMV IgG, positive | 191 (93.2%) | 24 (96.0%) | 0.588 |
| Donor and Operative factors | |||
| Donor age, year-old | 30.5 ± 8.4 | 30.5 ± 9.5 | 0.968 |
| Donor age ≥ 45-year-old | 12 (5.9%) | 2 (8.0%) | 0.672 |
| Donor sex, male | 116 (56.6%) | 18 (72.0%) | 0.140 |
| Graft type, right liver | 193 (94.1%) | 25 (100.0%) | 0.214 |
| Ascites amount, mL, intraoperative | 1200 | 2500 | <0.001 |
| Blood loss, mL, intraoperative | 50 | 1600 | 0.011 |
| Clinical Outcomes | MELD < 20, n = 205 | MELD ≥ 20, n = 25 | p-Value |
|---|---|---|---|
| Post-LT HCC DFS rate, at 1-, 3-, 5-year, % | 93.1, 85.7, 83.4% | 94.7, 82.9, 82.9% | 0.973 |
| Post-LT HCC recurrence, number | 33 (16.1%) | 3 (12.0%) | 0.594 |
| Post-LT HCC recurrence, months | 23.4 ± 21.7 | 20.5 ± 8.7 | 0.825 |
| Acute rejection | 55 (26.8%) | 7 (28.0%) | 0.900 |
| Post-LT infection Urine tract infection Intraabdominal infection Pneumonia Blood stream or catheter related infection | 95 (46.3%) 8 (3.9%) 29 (14.1%) 28 (13.7%) 30 (14.6%) | 15 (60.0%) 1 (4.0%) 3 (12.0%) 3 (12.0%) 8 (32.0%) | 0.197 |
| CMV disease | 30 (14.6%) | 9 (36.0%) | 0.007 |
| Severe CMV disease | 10 (4.9%) | 4 (16.0%) | 0.028 |
| Septic shock | 18 (8.8%) | 6 (24.0%) | 0.019 |
| Major post-LT complication | 20 (9.8%) | 8 (32.0%) | 0.001 |
| Post-LT OS rate, at 1-, 3-, 5-year, % | 85.8, 77.5, 71.1% | 72.0, 56.0, 52.0% | 0.056 |
| Cumulative mortalities Infection-related | 76 (37.1%) 41 (53.9%) | 13 (52.0%) 7 (53.8%) | 0.148 |
| HCC-related | 18 (23.7%) | 1 (7.7%) | |
| Rejection-related | 8 (10.5%) | 3 (23.1%) | |
| Cardiovascular disease | 3 (3.9%) | 1 (7.7%) | |
| Bleeding | 2 (2.6%) | 1 (7.7%) | |
| Others | 4 (5.3%) | 0 (0.0%) |
| Parameters | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 90%CI | p-Value | HR | 90%CI | p-Value | |
| MELD score ≥ 20 | 3.28 | 1.37–7.84 | 0.025 | 3.28 | 1.37–7.84 | 0.025 |
| NLR ≥ 5 | 2.36 | 1.09–5.12 | 0.068 | |||
| Pre-LT locoregional treatment | 0.44 | 0.21–0.93 | 0.071 | |||
| Predicted Event | Post-LT Septic Shock | Post-LT Mortality | ||||
|---|---|---|---|---|---|---|
| HR | 90%CI | p-Value | HR | 90%CI | p-Value | |
| NLR | 1.13 | 1.02–1.27 | 0.027 | 1.07 | 1.02–1.13 | 0.029 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, H.-C.; Lee, J.-C.; Wang, Y.-C.; Cheng, C.-H.; Wu, T.-H.; Wu, T.-J.; Chou, H.-S.; Chan, K.-M.; Lee, W.-C.; Lee, C.-F. Living-Donor Liver Transplantation for Hepatocellular Carcinoma: Impact of the MELD Score and Predictive Value of NLR on Survival. Curr. Oncol. 2022, 29, 3881-3893. https://doi.org/10.3390/curroncol29060310
Hung H-C, Lee J-C, Wang Y-C, Cheng C-H, Wu T-H, Wu T-J, Chou H-S, Chan K-M, Lee W-C, Lee C-F. Living-Donor Liver Transplantation for Hepatocellular Carcinoma: Impact of the MELD Score and Predictive Value of NLR on Survival. Current Oncology. 2022; 29(6):3881-3893. https://doi.org/10.3390/curroncol29060310
Chicago/Turabian StyleHung, Hao-Chien, Jin-Chiao Lee, Yu-Chao Wang, Chih-Hsien Cheng, Tsung-Han Wu, Ting-Jung Wu, Hong-Shiue Chou, Kun-Ming Chan, Wei-Chen Lee, and Chen-Fang Lee. 2022. "Living-Donor Liver Transplantation for Hepatocellular Carcinoma: Impact of the MELD Score and Predictive Value of NLR on Survival" Current Oncology 29, no. 6: 3881-3893. https://doi.org/10.3390/curroncol29060310
APA StyleHung, H.-C., Lee, J.-C., Wang, Y.-C., Cheng, C.-H., Wu, T.-H., Wu, T.-J., Chou, H.-S., Chan, K.-M., Lee, W.-C., & Lee, C.-F. (2022). Living-Donor Liver Transplantation for Hepatocellular Carcinoma: Impact of the MELD Score and Predictive Value of NLR on Survival. Current Oncology, 29(6), 3881-3893. https://doi.org/10.3390/curroncol29060310