Selective Internal Radiation Therapy with Yttrium-90 for Intrahepatic Cholangiocarcinoma: A Systematic Review on Post-Treatment Dosimetry and Concomitant Chemotherapy

 , and
, and 
Abstract
1. Introduction
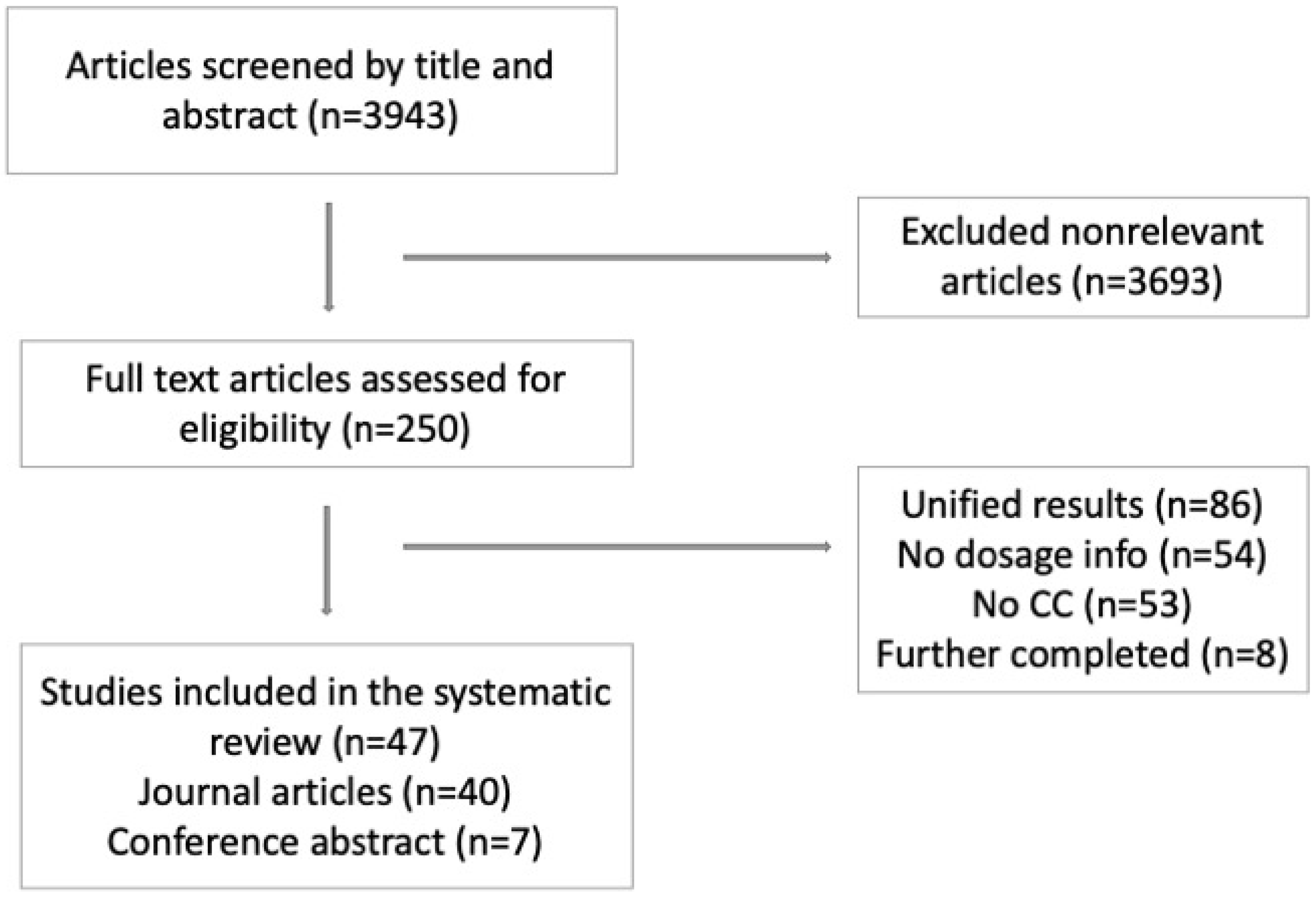
2. Material and Methods
3. Results
4. Discussion
4.1. Dosimetry and Dose-Response Relationship
4.2. Types of 90Y Microspheres
4.3. Concomitant Chemotherapy
4.4. Treatment Outcome
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rizvi, S.; Khan, S.A.; Hallemeier, C.L.; Kelley, R.K.; Gores, G.J. Cholangiocarcinoma—Evolving concepts and therapeutic strategies. Nat. Rev. Clin. Oncol. 2018, 15, 95. [Google Scholar] [CrossRef] [PubMed]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.-W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [PubMed]
- Hyder, O.; Hatzaras, I.; Sotiropoulos, G.C.; Paul, A.; Alexandrescu, S.; Marques, H.; Pulitano, C.; Barroso, E.; Clary, B.M.; Aldrighetti, L. Recurrence after operative management of intrahepatic cholangiocarcinoma. Surgery 2013, 153, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Sommer, C.M.; Kauczor, H.U.; Pereira, P.L. Locoregional therapies of cholangiocarcinoma. Visc. Med. 2016, 32, 414–420. [Google Scholar] [CrossRef]
- Edeline, J.; Lamarca, A.; McNamara, M.G.; Jacobs, T.; Hubner, R.A.; Palmer, D.; Koerkamp, B.G.; Johnson, P.; Guiu, B.; Valle, J.W. Locoregional therapies in patients with intrahepatic cholangiocarcinoma: A systematic review and pooled analysis. Cancer Treat. Rev. 2021, 99, 102258. [Google Scholar] [CrossRef]
- Ariel, I.M. Treatment of inoperable primary pancreatic and liver cancer by the intra-arterial administration of radioactive isotopes (Y90 radiating microspheres). Ann. Surg. 1965, 162, 267. [Google Scholar] [CrossRef]
- Cucchetti, A.; Cappelli, A.; Mosconi, C.; Zhong, J.H.; Cescon, M.; Pinna, A.D.; Golfieri, R. Improving patient selection for selective internal radiation therapy of intra-hepatic cholangiocarcinoma: A meta-regression study. Liver Int. 2017, 37, 1056–1064. [Google Scholar] [CrossRef]
- Rizzo, A.; Frega, G.; Ricci, A.D.; Palloni, A.; Abbati, F.; De Lorenzo, S.; Deserti, M.; Tavolari, S.; Brandi, G. Anti-EGFR Monoclonal Antibodies in Advanced Biliary Tract Cancer: A Systematic Review and Meta-analysis. In Vivo 2020, 34, 479–488. [Google Scholar] [CrossRef]
- Rizzo, A.; Brandi, G. First-line Chemotherapy in Advanced Biliary Tract Cancer Ten Years after the ABC-02 Trial: “And Yet It Moves!”. Cancer Treat. Res. Commun. 2021, 27, 100335. [Google Scholar] [CrossRef]
- Dawson, L.A.; McGinn, C.J.; Normolle, D.; Ten Haken, R.K.; Walker, S.; Ensminger, W.; Lawrence, T.S. Escalated focal liver radiation and concurrent hepatic artery fluorodeoxyuridine for unresectable intrahepatic malignancies. J. Clin. Oncol. 2000, 18, 2210–2218. [Google Scholar] [CrossRef]
- Cremonesi, M.; Chiesa, C.; Strigari, L.; Ferrari, M.; Botta, F.; Guerriero, F.; De Cicco, C.; Bonomo, G.; Orsi, F.; Bodei, L. Radioembolization of hepatic lesions from a radiobiology and dosimetric perspective. Front. Oncol. 2014, 4, 210. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.L.; Zhang, J.; Tweedle, M.F.; Knopp, M.V.; Hall, N.C. Theranostic imaging of Yttrium-90. BioMed Res. Int. 2015, 2015, 481279. [Google Scholar] [CrossRef] [PubMed]
- Levillain, H.; Bagni, O.; Deroose, C.M.; Dieudonné, A.; Gnesin, S.; Grosser, O.S.; Kappadath, S.C.; Kennedy, A.; Kokabi, N.; Liu, D.M. International recommendations for personalised selective internal radiation therapy of primary and metastatic liver diseases with yttrium-90 resin microspheres. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1570–1584. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.; Lau, W.Y.; Leung, T.W.; Chan, M.; Ngar, Y.K.; Johnson, P.J.; Li, A.K. Partition model for estimating radiation doses from yttrium-90 microspheres in treating hepatic tumours. Eur. J. Nucl. Med. 1996, 23, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Garin, E.; Lenoir, L.; Rolland, Y.; Edeline, J.; Mesbah, H.; Laffont, S.; Porée, P.; Clément, B.; Raoul, J.-L.; Boucher, E. Dosimetry based on 99mTc-macroaggregated albumin SPECT/CT accurately predicts tumor response and survival in hepatocellular carcinoma patients treated with 90Y-loaded glass microspheres: Preliminary results. J. Nucl. Med. 2012, 53, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Toskich, B.B.; Liu, D.M. Y90 radioembolization dosimetry: Concepts for the interventional radiologist. Tech. Vasc. Interv. Radiol. 2019, 22, 100–111. [Google Scholar] [CrossRef]
- Song, Y.S.; Paeng, J.C.; Kim, H.-C.; Chung, J.W.; Cheon, G.J.; Chung, J.-K.; Lee, D.S.; Kang, K.W. PET/CT-based dosimetry in 90Y-microsphere selective internal radiation therapy: Single cohort comparison with pretreatment planning on 99mTc-MAA imaging and correlation with treatment efficacy. Medicine 2015, 94, e945. [Google Scholar] [CrossRef]
- Wondergem, M.; Smits, M.L.; Elschot, M.; de Jong, H.W.; Verkooijen, H.M.; van den Bosch, M.A.; Nijsen, J.F.; Lam, M.G. 99mTc-macroaggregated albumin poorly predicts the intrahepatic distribution of 90Y resin microspheres in hepatic radioembolization. J. Nucl. Med. 2013, 54, 1294–1301. [Google Scholar] [CrossRef]
- Moher, D.; Altman, D.G.; Liberati, A.; Tetzlaff, J. PRISMA statement. Epidemiology 2011, 22, 128. [Google Scholar] [CrossRef]
- Boehm, L.M.; Jayakrishnan, T.T.; Miura, J.T.; Zacharias, A.J.; Johnston, F.M.; Turaga, K.K.; Gamblin, T.C. Comparative effectiveness of hepatic artery based therapies for unresectable intrahepatic cholangiocarcinoma. J. Surg. Oncol. 2015, 111, 213–220. [Google Scholar] [CrossRef]
- Al-Adra, D.; Gill, R.; Axford, S.; Shi, X.; Kneteman, N.; Liau, S.-S. Treatment of unresectable intrahepatic cholangiocarcinoma with yttrium-90 radioembolization: A systematic review and pooled analysis. Eur. J. Surg. Oncol. 2015, 41, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Willowson, K.P.; Eslick, E.M.; Bailey, D.L. Individualised dosimetry and safety of SIRT for intrahepatic cholangiocarcinoma. EJNMMI Phys. 2021, 8, 65. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, A.; Ali, A.; Ljuboja, D.; Weinstein, J.L.; Shenoy-Bhangle, A.S.; Nasser, I.A.; Morrow, M.K.; Faintuch, S.; Curry, M.P.; Bullock, A.J.; et al. Neoadjuvant Yttrium-90 Transarterial Radioembolization with Resin Microspheres Prescribed Using the Medical Internal Radiation Dose Model for Intrahepatic Cholangiocarcinoma. J. Vasc. Interv. Radiol. 2021, 32, 1560–1568. [Google Scholar] [CrossRef] [PubMed]
- Paprottka, K.J.; Galiè, F.; Ingrisch, M.; Geith, T.; Ilhan, H.; Todica, A.; Michl, M.; Nadjiri, J.; Paprottka, P.M. Outcome and Safety after 103 Radioembolizations with Yttrium-90 Resin Microspheres in 73 Patients with Unresectable Intrahepatic Cholangiocarcinoma-An Evaluation of Predictors. Cancers 2021, 13, 5399. [Google Scholar] [CrossRef] [PubMed]
- Depalo, T.; Traino, A.C.; Bargellini, I.; Lorenzoni, G.; Bozzi, E.; Vivaldi, C.; Lamastra, R.; Masi, G.; Cioni, R.; Boni, G.; et al. Assessment of radiation sensitivity of unresectable intrahepatic cholangiocarcinoma in a series of patients submitted to radioembolization with yttrium-90 resin microspheres. Sci. Rep. 2021, 11, 19745. [Google Scholar] [CrossRef]
- Paz-Fumagalli, R.; Core, J.; Padula, C.; Montazeri, S.; McKinney, J.; Frey, G.; Devcic, Z.; Lewis, A.; Ritchie, C.; Mody, K.; et al. Safety and initial efficacy of ablative radioembolization for the treatment of unresectable intrahepatic cholangiocarcinoma. Oncotarget 2021, 12, 2075–2088. [Google Scholar] [CrossRef]
- Cheng, B.; Villalobos, A.; Sethi, I.; Wagstaff, W.; Galt, J.; Brandon, D.; Schuster, D.M.; Bercu, Z.; Majdalany, B.; Kokabi, N. Determination of Tumor Dose Response Thresholds in Patients with Chemorefractory Intrahepatic Cholangiocarcinoma Treated with Resin and Glass-based Y90 Radioembolization. Cardiovasc. Interv. Radiol. 2021, 44, 1194–1203. [Google Scholar] [CrossRef]
- Bozkurt, M.; Eldem, G.; Bozbulut, U.B.; Bozkurt, M.F.; Kılıçkap, S.; Peynircioğlu, B.; Çil, B.; Lay Ergün, E.; Volkan-Salanci, B. Factors affecting the response to Y-90 microsphere therapy in the cholangiocarcinoma patients. Radiol. Med. 2021, 126, 323–333. [Google Scholar] [CrossRef]
- Riby, D.; Mazzotta, A.D.; Bergeat, D.; Verdure, L.; Sulpice, L.; Bourien, H.; Lièvre, A.; Rolland, Y.; Garin, E.; Boudjema, K.; et al. Downstaging with Radioembolization or Chemotherapy for Initially Unresectable Intrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2020, 27, 3729–3737. [Google Scholar] [CrossRef]
- Mosconi, C.; Cucchetti, A.; Bruno, A.; Cappelli, A.; Bargellini, I.; De Benedittis, C.; Lorenzoni, G.; Gramenzi, A.; Tarantino, F.P.; Parini, L.; et al. Radiomics of cholangiocarcinoma on pretreatment CT can identify patients who would best respond to radioembolisation. Eur. Radiol. 2020, 30, 4534–4544. [Google Scholar] [CrossRef]
- Köhler, M.; Harders, F.; Lohöfer, F.; Paprottka, P.M.; Schaarschmidt, B.M.; Theysohn, J.; Herrmann, K.; Heindel, W.; Schmidt, H.H.; Pascher, A.; et al. Prognostic factors for overall survival in advanced intrahepatic cholangiocarcinoma treated with yttrium-90 radioembolization. J. Clin. Med. 2019, 9, 56. [Google Scholar] [CrossRef]
- Filippi, L.; Di Costanzo, G.G.; Tortora, R.; Pelle, G.; Saltarelli, A.; Marsilia, G.M.; Cianni, R.; Schillaci, O.; Bagni, O. Prognostic value of neutrophil-to-lymphocyte ratio and its correlation with fluorine-18-fluorodeoxyglucose metabolic parameters in intrahepatic cholangiocarcinoma submitted to 90Y-radioembolization. Nucl. Med. Commun. 2020, 41, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Edeline, J.; Touchefeu, Y.; Guiu, B.; Farge, O.; Tougeron, D.; Baumgaertner, I.; Ayav, A.; Campillo-Gimenez, B.; Beuzit, L.; Pracht, M.; et al. Radioembolization Plus Chemotherapy for First-line Treatment of Locally Advanced Intrahepatic Cholangiocarcinoma: A Phase 2 Clinical Trial. JAMA Oncol. 2020, 6, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Buettner, S.; Braat, A.J.A.T.; Margonis, G.A.; Brown, D.B.; Taylor, K.B.; Borgmann, A.J.; Kappadath, S.C.; Mahvash, A.; Ijzermans, J.N.M.; Weiss, M.J.; et al. Yttrium-90 Radioembolization in Intrahepatic Cholangiocarcinoma: A Multicenter Retrospective Analysis. J. Vasc. Interv. Radiol. 2020, 31, 1035–1043.e2. [Google Scholar] [CrossRef] [PubMed]
- Bargellini, I.; Mosconi, C.; Pizzi, G.; Lorenzoni, G.; Vivaldi, C.; Cappelli, A.; Vallati, G.E.; Boni, G.; Cappelli, F.; Paladini, A.; et al. Yttrium-90 Radioembolization in Unresectable Intrahepatic Cholangiocarcinoma: Results of a Multicenter Retrospective Study. Cardiovasc. Interv. Radiol. 2020, 43, 1305–1314. [Google Scholar] [CrossRef]
- Azar, A.; Devcic, Z.; Paz-Fumagalli, R.; Vidal, L.L.C.; McKinney, J.M.; Frey, G.; Lewis, A.R.; Ritchie, C.; Starr, J.S.; Mody, K.; et al. Albumin-bilirubin grade as a prognostic indicator for patients with non-hepatocellular primary and metastatic liver malignancy undergoing Yttrium-90 radioembolization using resin microspheres. J. Gastrointest. Oncol. 2020, 11, 715–723. [Google Scholar] [CrossRef]
- White, J.; Carolan-Rees, G.; Dale, M.; Patrick, H.E.; See, T.C.; Bell, J.K.; Manas, D.M.; Crellin, A.; Slevin, N.J.; Sharma, R.A. Yttrium-90 Transarterial Radioembolization for Chemotherapy-Refractory Intrahepatic Cholangiocarcinoma: A Prospective, Observational Study. J. Vasc. Interv. Radiol. 2019, 30, 1185–1192. [Google Scholar] [CrossRef]
- Galiè, F.; Paprottka, K.J.; Ingrisch, M.; Todica, A.; Ilhan, H.; Michl, M.; Geith, T.; Fabritius, M.; De Toni, E.; Paprottka, P.M. Impact of Baseline Cholinesterase in Patients with Primary Liver Tumors Undergoing Radioembolization: Impact on Outcome. SN Compr. Clin. Med. 2019, 1, 85–92. [Google Scholar] [CrossRef]
- Bourien, H.; Palard, X.; Rolland, Y.; Le Du, F.; Beuzit, L.; Uguen, T.; Le Sourd, S.; Pracht, M.; Manceau, V.; Lièvre, A.; et al. Yttrium-90 glass microspheres radioembolization (RE) for biliary tract cancer: A large single-center experience. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 669–676. [Google Scholar] [CrossRef]
- Levillain, H.; Derijckere, I.D.; Ameye, L.; Guiot, T.; Braat, A.; Meyer, C.; Vanderlinden, B.; Reynaert, N.; Hendlisz, A.; Lam, M. Personalised radioembolization improves outcomes in refractory intra-hepatic cholangiocarcinoma: A multicenter study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2270–2279. [Google Scholar] [CrossRef]
- Shaker, T.M.; Chung, C.; Varma, M.K.; Doherty, M.G.; Wolf, A.M.; Chung, M.H.; Assifi, M.M. Is there a role for Ytrrium-90 in the treatment of unresectable and metastatic intrahepatic cholangiocarcinoma? Am. J. Surg. 2018, 215, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Reimer, P.; Virarkar, M.K.; Binnenhei, M.; Justinger, M.; Schön, M.R.; Tatsch, K. Prognostic Factors in Overall Survival of Patients with Unresectable Intrahepatic Cholangiocarcinoma Treated by Means of Yttrium-90 Radioembolization: Results in Therapy-Naïve Patients. Cardiovasc. Interv. Radiol. 2018, 41, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Nezami, N.; Kokabi, N.; Camacho, J.C.; Schuster, D.M.; Xing, M.; Kim, H.S. 90Y radioembolization dosimetry using a simple semi-quantitative method in intrahepatic cholangiocarcinoma: Glass versus resin microspheres. Nucl. Med. Biol. 2018, 59, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Manceau, V.; Palard, X.; Rolland, Y.; Pracht, M.; Le Sourd, S.; Laffont, S.; Boudjema, K.; Lievre, A.; Mesbah, H.; Haumont, L.A.; et al. A MAA-based dosimetric study in patients with intrahepatic cholangiocarcinoma treated with a combination of chemotherapy and 90Y-loaded glass microsphere selective internal radiation therapy. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1731–1741. [Google Scholar] [CrossRef] [PubMed]
- Gangi, A.; Shah, J.; Hatfield, N.; Smith, J.; Sweeney, J.; Choi, J.; El-Haddad, G.; Biebel, B.; Parikh, N.; Arslan, B.; et al. Intrahepatic Cholangiocarcinoma Treated with Transarterial Yttrium-90 Glass Microsphere Radioembolization: Results of a Single Institution Retrospective Study. J. Vasc. Interv. Radiol. 2018, 29, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Swinburne, N.C.; Biederman, D.M.; Besa, C.; Tabori, N.E.; Fischman, A.M.; Patel, R.S.; Nowakowski, F.S.; Gunasekaran, G.; Schwartz, M.E.; Lookstein, R.A.; et al. Radioembolization for Unresectable Intrahepatic Cholangiocarcinoma: Review of Safety, Response Evaluation Criteria in Solid Tumors 1.1 Imaging Response and Survival. Cancer Biother. Radiopharm. 2017, 32, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.; Paz-Fumagalli, R.; Frey, G.; Sella, D.M.; McKinney, J.M.; Wang, W. Resin-based Yttrium-90 microspheres for unresectable and failed first-line chemotherapy intrahepatic cholangiocarcinoma: Preliminary results. J. Cancer Res. Clin. Oncol. 2017, 143, 481–489. [Google Scholar] [CrossRef]
- Akinwande, O.; Shah, V.; Mills, A.; Noda, C.; Weiner, E.; Foltz, G.; Saad, N. Chemoembolization versus radioembolization for the treatment of unresectable intrahepatic cholangiocarcinoma in a single institution image-based efficacy and comparative toxicity. Hepat. Oncol. 2017, 4, 75–81. [Google Scholar] [CrossRef]
- Soydal, C.; Kucuk, O.N.; Bilgic, S.; Ibis, E. Radioembolization with 90Y resin microspheres for intrahepatic cholangiocellular carcinoma: Prognostic factors. Ann. Nucl. Med. 2016, 30, 29–34. [Google Scholar] [CrossRef]
- Pieper, C.C.; Willinek, W.A.; Thomas, D.; Ahmadzadehfar, H.; Essler, M.; Nadal, J.; Wilhelm, K.E.; Schild, H.H.; Meyer, C. Incidence and risk factors of early arterial blood flow stasis during first radioembolization of primary and secondary liver malignancy using resin microspheres: An initial single-center analysis. Eur. Radiol. 2016, 26, 2779–2789. [Google Scholar] [CrossRef]
- Mosconi, C.; Gramenzi, A.; Ascanio, S.; Cappelli, A.; Renzulli, M.; Pettinato, C.; Brandi, G.; Monari, F.; Cucchetti, A.; Trevisani, F.; et al. Yttrium-90 radioembolization for unresectable/recurrent intrahepatic cholangiocarcinoma: A survival, efficacy and safety study. Br. J. Cancer 2016, 115, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.G.E.H.; Banerjee, A.; Goris, M.L.; Iagaru, A.H.; Mittra, E.S.; Louie, J.D.; Sze, D.Y. Fusion dual-tracer SPECT-based hepatic dosimetry predicts outcome after radioembolization for a wide range of tumour cell types. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1192–1201. [Google Scholar] [CrossRef] [PubMed]
- Filippi, L.; Pelle, G.; Cianni, R.; Scopinaro, F.; Bagni, O. Change in total lesion glycolysis and clinical outcome after (90)Y radioembolization in intrahepatic cholangiocarcinoma. Nucl. Med. Biol. 2015, 42, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Edeline, J.; Du, F.L.; Rayar, M.; Rolland, Y.; Beuzit, L.; Boudjema, K.; Rohou, T.; Latournerie, M.; Campillo-Gimenez, B.; Garin, E.; et al. Glass microspheres 90Y selective internal radiation therapy and chemotherapy as first-line treatment of intrahepatic cholangiocarcinoma. Clin. Nucl. Med. 2015, 40, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Camacho, J.C.; Kokabi, N.; Xing, M.; Prajapati, H.J.; El-Rayes, B.; Kim, H.S. Modified response evaluation criteria in solid tumors and european association for the study of the liver criteria using delayed-phase imaging at an early time point predict survival in patients with unresectable intrahepatic cholangiocarcinoma following yttrium-90 radioembolization. J. Vasc. Interv. Radiol. 2014, 25, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Rafi, S.; Piduru, S.M.; El-Rayes, B.; Kauh, J.S.; Kooby, D.A.; Sarmiento, J.M.; Kim, H.S. Yttrium-90 radioembolization for unresectable standard-chemorefractory intrahepatic cholangiocarcinoma: Survival, efficacy, and safety study. Cardiovasc. Interv. Radiol. 2013, 36, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Mouli, S.; Memon, K.; Baker, T.; Benson Iii, A.B.; Mulcahy, M.F.; Gupta, R.; Ryu, R.K.; Salem, R.; Lewandowski, R.J. Yttrium-90 radioembolization for intrahepatic cholangiocarcinoma: Safety, response, and survival analysis. J. Vasc. Interv. Radiol. 2013, 24, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, R.T.; Paprottka, P.M.; Schön, A.; Bamberg, F.; Haug, A.; Dürr, E.M.; Rauch, B.; Trumm, C.T.; Jakobs, T.F.; Helmberger, T.K.; et al. Transarterial hepatic yttrium-90 radioembolization in patients with unresectable intrahepatic cholangiocarcinoma: Factors associated with prolonged survival. Cardiovasc. Interv. Radiol. 2012, 35, 105–116. [Google Scholar] [CrossRef]
- Haug, A.R.; Heinemann, V.; Bruns, C.J.; Hoffmann, R.; Jakobs, T.; Bartenstein, P.; Hacker, M. 18 F-FDG PET independently predicts survival in patients with cholangiocellular carcinoma treated with 90Y microspheres. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1037–1045. [Google Scholar] [CrossRef]
- Saxena, A.; Bester, L.; Chua, T.C.; Morris, D.L. Yttrium-90 radiotherapy for unresectable intrahepatic cholangiocarcinoma: A preliminary assessment of this novel treatment option. Ann. Surg. Oncol. 2010, 17, S103. [Google Scholar] [CrossRef]
- Ibrahim, S.M.; Mulcahy, M.F.; Lewandowski, R.J.; Sato, K.T.; Ryu, R.K.; Masterson, E.J.; Newman, S.B.; Benson Iii, A.; Omary, R.A.; Salem, R. Treatment of unresectable cholangiocarcinoma using yttrium-90 microspheres: Results from a pilot study. Cancer 2008, 113, 2119–2128. [Google Scholar] [CrossRef] [PubMed]
- Helmberger, T.; Arnold, D.; Balli, T.; Golfieri, R.; Pech, M.; Ronot, M.; De Jong, N.; Sangro, B. Real-world outcomes of patients with intrahepatic cholangiocarcinoma treated with trans-arterial radioembolization: Results from the CIRSE Registry for SIR-Spheres Therapy (CIRT), alarge European prospective multi-center observational study. J. Clin. Oncol. 2021, 39, 308. [Google Scholar] [CrossRef]
- Lorenzoni, A.; Mazzaglia, S.; Spreafico, C.; Scalorbi, F.; Argiroffi, G.; Bhoori, S.; Chiesa, C.; Fuoco, V.; Cascella, T.; Seregni, E.; et al. Transarterial radioembolization of unresectable intrahepatic cholangiocarcinoma with 90Y glass microspheres: Results of a single institution study. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, S278–S279. [Google Scholar] [CrossRef]
- Core, J.; Padula, C.; Elboraey, M.; Devcic, Z.; Ritchie, C.; Lewis, A.; McKinney, J.; Paz-Fumagalli, R.; Frey, G.; Toskich, B. Abstract No. 560 Safety and efficacy of radioembolization for intrahepatic cholangiocarcinoma with ≥150 Gy MIRD: A single-center review. J. Vasc. Interv. Radiol. 2020, 31, S244. [Google Scholar] [CrossRef]
- Pettinato, C.; Mosconi, C.; Cappelli, A.; Tabacchi, E.; Lodi Rizzini, E.; Monari, F.; Civollani, S.; Fanti, S.; Strigari, L. Yttrium-90 radioembolization for unresectable/recurrent intrahepatic cholangiocarcinoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, S632–S633. [Google Scholar] [CrossRef]
- Schatka, I.; Jochens, H.; Rogasch, J.; Huang, K.; Wedel, F.; Heimann, U.; Bartel, C.; Furth, C.; Brenner, W.; Gebauer, B.; et al. Radioembolization in patients with intrahepatic cholangiocarcinoma-a prognostic risk stratification model. J. Nucl. Med. 2017, 58, 459. [Google Scholar]
- Boni, G.; Depalo, T.; Bargellini, I.; Vivaldi, C.; Mazzarri, S.; Guidoccio, F.; Bozzi, E.; Caponi, L.; Traino, C.; Manca, G.; et al. Effectiveness and safety of transarterial Y-90 radioembolization for unresectable intrahepatic cholangiocarcinoma. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, S803. [Google Scholar] [CrossRef]
- Peterson, J.; Vallow, L.; Johnson, D.; Heckman, M.; Diehl, N.; Gale, A.; Tzou, K.; Kim, S.; Brown, N.; Paz-Fumagalli, R.; et al. Initial experience with sirspheres Yttrium-90 microsphere radioembolization for cholangiocarcinoma. HPB 2010, 12, 286–287. [Google Scholar] [CrossRef][Green Version]
- Nezami, N.; Camacho, J.C.; Kokabi, N.; El-Rayes, B.F.; Kim, H.S. Phase Ib trial of gemcitabine with yttrium-90 in patients with hepatic metastasis of pancreatobiliary origin. J. Gastrointest. Oncol. 2019, 10, 944. [Google Scholar] [CrossRef]
- Kao, Y.-H.; Steinberg, J.D.; Tay, Y.-S.; Lim, G.K.; Yan, J.; Townsend, D.W.; Takano, A.; Burgmans, M.C.; Irani, F.G.; Teo, T.K. Post-radioembolization yttrium-90 PET/CT-part 1: Diagnostic reporting. EJNMMI Res. 2013, 3, 56. [Google Scholar] [CrossRef]
- Padia, S.A.; Alessio, A.; Kwan, S.W.; Lewis, D.H.; Vaidya, S.; Minoshima, S. Comparison of positron emission tomography and bremsstrahlung imaging to detect particle distribution in patients undergoing yttrium-90 radioembolization for large hepatocellular carcinomas or associated portal vein thrombosis. J. Vasc. Interv. Radiol. 2013, 24, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Gulec, S.A.; Sztejnberg, M.L.; Siegel, J.A.; Jevremovic, T.; Stabin, M. Hepatic structural dosimetry in (90)Y microsphere treatment: A Monte Carlo modeling approach based on lobular microanatomy. J. Nucl Med. 2010, 51, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Zhen, Y.; Liu, B.; Chang, Z.; Ren, H.; Liu, Z.; Zheng, J. A pooled analysis of transarterial radioembolization with yttrium-90 microspheres for the treatment of unresectable intrahepatic cholangiocarcinoma. Onco Targets Ther. 2019, 12, 4489–4498. [Google Scholar] [CrossRef] [PubMed]
- Park, J.O.; Oh, D.-Y.; Hsu, C.; Chen, J.-S.; Chen, L.-T.; Orlando, M.; Kim, J.S.; Lim, H.Y. Gemcitabine plus cisplatin for advanced biliary tract cancer: A systematic review. Cancer Res. Treat. 2015, 47, 343–361. [Google Scholar] [CrossRef]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [PubMed]
- Small, W., Jr.; Berlin, J.; Freedman, G.M.; Lawrence, T.; Talamonti, M.S.; Mulcahy, M.F.; Chakravarthy, A.B.; Konski, A.A.; Zalupski, M.M.; Philip, P.A. Full-dose gemcitabine with concurrent radiation therapy in patients with nonmetastatic pancreatic cancer: A multicenter phase II trial. J. Clin. Oncol. 2008, 26, 942–947. [Google Scholar] [CrossRef]
- Zhu, C.-P.; Shi, J.; Chen, Y.-X.; Xie, W.-F.; Lin, Y. Gemcitabine in the chemoradiotherapy for locally advanced pancreatic cancer: A meta-analysis. Radiother. Oncol. 2011, 99, 108–113. [Google Scholar] [CrossRef]
- Mosconi, C.; Solaini, L.; Vara, G.; Brandi, N.; Cappelli, A.; Modestino, F.; Cucchetti, A.; Golfieri, R. Transarterial Chemoembolization and Radioembolization for Unresectable Intrahepatic Cholangiocarcinoma—A Systemic Review and Meta-Analysis. Cardiovasc. Interv. Radiol. 2021, 44, 728–738. [Google Scholar] [CrossRef]


{kind=link}
| Author (Year), Type of Study | Patient Population | Radiation Dosage, Gy | Activity, GBq | Microsphere Type: Number of Patients Treated | RECIST, WHO, EASL at 1st Assessment | Survival Outcomes | Follow-Up Information | Notes and Other Findings |
|---|---|---|---|---|---|---|---|---|
| Willowson KP, et al. (2021) RS [22] | 18 pts 23 SIRTs (5 pts with multiple SIRTs) Refractory | - | Median: 1.5 Mean: 1.62 | Resin: 18 | - | - | - | Lesion-based analysis with 18F-FDG PET/CT was done. |
| Sarwar, A. et al. (2021) RS [23] | 31 pts 40 SIRTs (7 pts with multiple SIRTs) Mixed † | Median: 150 | Median: 1.9 | Resin: 31 | RECIST 1.1 at 2–3 mo (29 pts) CR:0, PR: 17.24%, SD: 68.96%, PD: 13.79% RECIST 1.1 at 6 mo (21 pts) CR: 0, PR: 23.8%, SD: 61.9%, PD: 14.28% | Median OS: 22 mo Median PFS: 5.4 mo Median TTP: 6.3 mo | Median FU: 14 mo 15 deaths | Post-SIRT 90Y SPECT-CT done qualitatively. Higher PFS in treatment-naïve vs. refractory patients, 7.4 vs. 2.7 mo (p = 0.00) as well as the TTP: 13 vs. 3 mo (p = 0.00) |
| Paprottka, K. J. et al. (2021) RS [24] | 73 pts 103 SIRTs (6 pts with multiple SIRTs) Refractory | - | Median: 1.5 | Resin: 73 | RECIST at 3 mo CR: 0 PR: 24.65% SD: 49.31% PD: 26.02% | Median OS: 11.8 mo Mean OS: 18.9 mo Median PFS: 6.4 mo Mean PFS: 10.1 mo | - | Post-SIRT 90Y SPECT-CT done qualitatively. Median PFS higher with multiple SIRTs 24.4 vs. 5.8 mo (p = 0.04) |
| Depalo, T. et al. (2021) RS [25] | 15 pts 21 SIRTs (Number of pts with multiple SIRT treatments unspecified) Mixed | Mean TD: 93 LD: 42 | Mean: 1.16 | Resin: 15 | RECIST 1.1 at 3 mo CR: 0 PR: 20% SD: 40% PD: 40% | Median TTP: 7.3 mo | - | Tumor absorbed dose showed positive effect on TTP (p = 0.05). No difference found in radio-sensitivity (α parameter) in SIRT + concomitant chemo vs. SIRT alone. |
| Paz-Fumagalli, R. et al. (2021) RS [26] | 28 pts 37 SIRTs (5 pts with multiple SIRTs) Mixed | Median: 256.8 | Mean: 2.53 | Glass: 28 | mRECIST at 3 mo (25 pts) CR: 44.1% PR: 50% SD: 2.9% PD: 2.9% Response rate: 94.1% Control Rate: 97.1% | Median OS not reached. Median PFS: 8.8. mo OS in 3yrs: 59% PFS in 3yrs: 25% | Median FU: 13.4 mo 9 deaths | Post-SIRT 90Y SPECT-CT done qualitatively. Multifocal, bilobar, and larger tumors had a worse PFS (p = 0.00, p = 0.00, p = 0.04). Mass-forming tumors had a longer OS (p = 0.002) |
| Cheng B, et al. (2021) RS [27] | 38 pts 45 SIRTs (Number of pts with multiple SIRT treatments unspecified) Refractory | Mean TD Resin: 78.9 Glass: 254.7 | - | Resin: 18 Glass: 20 | mRECIST at 3 mo CR: 15.78%, PR: 39.47%, SD: 23.68%, PD: 21.10% OR: Glass: 50% Resin: 61.11% (p = 0.47) | Median OS: Resin: 11.2 mo Glass: 10.9 mo (p = 0.54) | - | Dose response study is done. Microsphere type had no effect on survival for Resin 11.2 mo vs. Glass 10.9 mo (p = 0.54). Glass and resin had a similar toxicity profile. |
| Bozkurt, M. et al. (2021) RS [28] | 19 pts * 24 SIRT (5 with multiple SIRT treatments) mixed | - | Mean Glass: 3.4 resin: 1.0 (p = 0.03) | Resin: 11 Glass: 13 | RECIST 1.1 at unspecified time: CR: 7.7% PR: 15.4% SD: 30.8% PD: 46.2% | Mean OS: 11.1 mo resin: 8.6 mo glass: 10.1 mo (p = 0.63) | - | 90Y SPECT-CT done qualitatively after SIRT. OS not different for naïve vs. refractory cases (p = 0.47) |
| Riby, D. et al. (2020) RS [29] | 19 pts naïve | Median TD: 258 Median NTD: 73.4 | Median: 1.9 | Resin: 19 | RECIST 1.1 at 3–6 mo (No separate results for SIRT cases) | Median OS not reached. Median RFS: 18.5 mo | Median FU: 44.0 mo | SIRT was applied to downstage the disease for surgical resection. |
| Mosconi, C. et al. (2020) RS [30] | 55 pts mixed | - | Median: 1.2 | Resin: 55 | RECIST 1.1 at unspecified time (53 pts): CR: 7.6% PR: 49.1% SD: 35.9% PD:7.6% | Median OS: 16.7 mo Median PFS: 6 mo | Median FU: 12.5 mo | Two pts died within 3 mo |
| Köhler, M. et al. (2020) RS [31] | 46 pts mixed | - | Median: 1.7 | Resin: 46 | RECIST 1.1 at 3 mo (44 pts): CR: 0 PR: 34.8% SD: 15.2% PD: 26.1% | Median OS: 9.5 mo (37 pts) | 9 pts lost to FU. 37 pts underwent survival analysis. | 90Y PET-CT done qualitatively after SIRT. Refractory cases had decreased survival (p = 0.00). |
| Filippi, L. et al. (2020) RS [32] | 20 pts mixed | - | Mean: 1.6 | Resin: 20 | - | Mean OS: 12.5 mo | - | 90Y PET-CT done qualitatively after SIRT. |
| Edeline, J. et al. (2020) PS [33] | 41 pts (15 with multiple SIRT treatments) mixed | Median TD: 317 Median NTD: 87 | - | Glass: 41 | RECIST 1.1 at 3 mo RR: 39% * Control rate: 98% | Median OS: 22 mo Median PFS: 14 mo | Median FU: 36 mo 23 deaths. | SIRT and chemotherapy were concomitant. |
| Buettner, S. et al. (2020) RS [34] | 114 pts refractory | Median Glass: 2.6 Resin: 1.6 (p = 0.00) Overall: 1.7 | Resin: 92 Glass: 22 | RECIST 1.1 at 6 mo (98 pts): Resin: PD: 26% SD: 69% PR: 3% Glass: PD: 30% SD: 45% PR: 25% (p = 0.00) | Median OS: 11 mo Resin: 11 mo Glass: 9 mo (p = 0.47) Median PFS: 5 mo Resin: 5 mo Glass: 3 mo (p = 0.85) Median liver-specific PFS: 6 mo | Median FU: Resin: 10 mo Glass: 14 mo 89 deaths. | One patient received both resin and glass microspheres and was excluded from analysis. Resin and glass microspheres had similar toxicity profiles (p = 0.35). | |
| Bargellini, I. et al. (2020) RS [35] | 81 pts mixed | Mean TD: 136.6 | Mean: 1.4 | Resin: 81 | RECIST 1.1 at unspecified time (79 pts) CR: 5% PR: 36% SD: 41% PD:16% OR: 41% Control rate: 83% | Median OS: 14.6 mo | Median FU: 11.1 mo | OS and tumor response did not differ in naïve vs. chemo-refractory cases. |
| Azar, A. et al. (2020) RS [36] | 22 pts mixed | - | Mean: 1.5 | Resin: 22 | - | Median OS: 9 mo | Median FU: 9.0 mo | - |
| White, J. et al. (2019) RS [37] | 61 pts mixed | Median Resin: 1.5 Glass: 2.8 | Resin: 45 Glass: 16 | Median OS: 8.7 mo Median PFS: 2.8 mo Median LPFS: 3.1 mo | Median FU: 13.9 mo 33 deaths | No analysis was done based on type of microspheres used. | ||
| Galiè, F. et al. (2019) RS [38] | 35 pts refractory | - | Median: 1.3 | Resin: 35 | RECIST 1.1 at 3 mo CR:0 PR: 25% SD: 47% PD: 28% | Median OS: 429 days | - | - |
| Bourien, H. et al. (2019) RS [39] | 64 pts (20 with multiple SIRT treatments) mixed | Median TD: 269 Median NTD: 85 | Median: 2.5 | Glass: 64 | RECIST 1.1 at unspecified time CR:0 PR: 15% SD: 61% PD: 24% | Median OS: 16.4 mo Median PFS: 7.6 mo | Median FU: 37.5 mo | OS was higher in those receiving radiation doses >260 Gy (p = 0.01). |
| Levillain, H. et al. (2019) PS [40] | 58 pts refractory | Median BSA NTD: 26 TD: 38 Median partition NTD: 35 TD: 86 | - | Resin: 58 | - | Median OS: 10.3 mo | Median FU: 6.3 mo | - |
| Shaker, T. M. et al. (2018) RS [41] | 17 pts (2 pts with multiple SIRT treatments) mixed | Mean TD, glass: 158.2 Mean TD, resin: 34.5 (p < 0.00) | - | Resin: 9 Glass: 8 | - | Median OS: 33.6 mo LPFS: 4 mo glass: 2.4 mo resin: 15.6 mo (p = 0.46) | Median FU: 21.3 mo | 90Y SPECT-CT done qualitatively after SIRT. |
| Reimer, P. et al. (2018) RS [42] | 21 pts naïve | - | - | Resin: 21 | RECIST at unspecified time CR:0 PR: 4.8% PD: 42.9% SD: 52.4% | Median OS: 15 mo | 11 deaths | 90Y PET-CT done qualitatively after SIRT. |
| Nezami, N. et al. (2018) RS [43] | 10 pts naïve | Mean TD, glass: 205.7 Mean TD, resin:128.9 (p < 0.00) Mean NTD, glass: 42.4 Mean NTD, resin: 53.6 (p < 0.00) | Mean Glass: 2.7 Resin: 1.6 (p < 0.00) | Resin: 5 Glass: 5 | - | - | - | Resin and glass microspheres had similar toxicity profiles (all p > 0.05). |
| Manceau, V. et al. (2018) RS [44] | 35 pts 55 SIRT (20 pts with multiple SIRTs) naïve | Mean TD: 322 Mean NTD: 74 | Mean: 2.6 | Glass: 35 | EASL at 3 mo CR: 47% PR: 49% SD: 4% PD: 0 | Median OS: 28.6 mo Median PFS: 12.7 mo | Median FU: 20.7 mo | The mean TD for responding lesions (CR + PR) was 310 Gy. |
| Gangi, A. et al. (2018) RS [45] | 85 pts 140 SIRT (40 pts with multiple SIRT treatments) mixed | Mean: 172.4 Median: 136.0 | - | Glass: 85 | RECIST at 3 mo (81 pts) CR: 0 PR: 6.2% SD: 64.2% PD: 29.6% | Median OS: 12.0 mo | Median FU: 9.8 mo | 90Y PET-CT done qualitatively after SIRT. Median OS was significantly higher in pts with well-differentiated tumors (p = 0.01). |
| Swinburne, N. C. et al. (2017) RS [46] | 29 pts (1 pt with multiple SIRT treatments) mixed | - | Mean: 1.6 | Resin: 17 Glass: 12 | RECIST 1.1 at 3 mo (26 pts) CR: 0 PR: 11.5% SD: 61.5% PD: 26.9% OR: 11.5% | Median OS: 9.1 mo Median TTP: 5.6 mo | Mean FU: 8.4 mo | 90Y SPECT-CT done qualitatively after SIRT. OS correlated with the imaging-based response (p = 0.02). No analysis was done based on the type of microspheres used. |
| Jia, Z. et al. (2017) RS [47] | 24 pts (3 with multiple SIRT treatments) refractory | Mean: 1.6 | Resin: 24 | mRECIST at 3 mo (22 pts): CR: 0 PR: 36.4% SD: 45.5% PD: 18.2% Control rate: 81.8% ‡ | Median OS: 9.0 mo | Mean FU: 11.3 mo 19 deaths | ||
| Akinwande, O. et al. (2017) RS [48] | 25 pts 37 SIRTs (number of pts with multiple SIRT treatments unspecified) mixed | - | Median: 1.5 | Resin: 11 Glass: 26 | mRECIST at 1 mo (19 pts): CR: 5.2% PR: 0 SD: 57.8% PD: 36.8% | - | - | - |
| Soydal, C. et al. (2016) RS [49] | 16 pts (2 with multiple SIRT treatments) mixed | - | Mean: 1.7 | Resin: 16 | RECIST at 3 mo OR: 31.2% | Median OS: 293 days | FU: 243 days 12 deaths | 90Y SPECT-CT done qualitatively after SIRT. |
| Pieper, C. C. et al. (2016) RS [50] | 26 pts mixed | - | Mean: 1.2 | Resin: 26 | - | - | - | Mean intended activity was 1.4 GBq; due to stasis, 86.9% was delivered. |
| Mosconi, C. et al. (2016) RS [51] | 23 pts mixed | - | Mean: 1.5 | Resin: 23 | RECIST 1.1 at 3 mo (20 pts): CR:0 PR: 15.0% SD: 30.0% PD: 55.0% mRECIST at 3 mo (20 pts): CR: 5.0% PR: 40.0% SD: 15.0% PD: 40.0% EASL at 3 mo (20 pts): CR: 5.0% PR: 55.0% SD: 25.0% PD: 15.0% | Median OS: 17.9 mo | Median FU: 16.0 mo 17 deaths | OS was higher in treatment-naïve vs. refractory cases (p = 0.00). |
| Lam, M. G. E. H. et al. (2015) RS [52] | 18 pts mixed | Median TD: 35 Median NTD: 24.9 | - | Both (numbers not mentioned) | RECIST 1.1 at 3 mo OR: 18% | Median OS: 5.7 mo | - | - |
| Filippi, L. et al. (2015) PS [53] | 17 pts mixed | - | Mean: 1.3 | Resin: 17 | PERCIST at 6 w CR: 0 PR: 82.3% SD: 17.6% PD: 0 | Mean OS: 64.5 w Mean TTP: 28.9 w | - | - |
| Edeline, J. et al. (2015) RS [54] | 24 pts naïve | Median TD: 256 Median NTD: 98 | Median: 2.2 | Glass: 24 | RECIST at unspecified time: CR: 0 PR: 25.0% SD: 62.5% PD: 12.5% Control rate: 87.5% | Median OS was not reached. Median PFS: 10.3 mo | Median FU: 19.0 mo | Median PFS was higher with concomitant than with SIRT given before chemotherapy (p = 0.00) |
| Camacho, J. C. et al. (2014) PS [55] | 21 pts refractory | - | - | Resin: 21 | RECIST 1.1 at 1 mo: CR:0 PR: 4.7% SD: 76.2% PD: 19.1% mRECIST at 1 mo: CR:0 PR: 62.0% SD:19.0% PD:19.0% EASL at 1 mo: CR: 0 PR: 9.5% SD: 71.4% PD: 19.1% | Median OS: 16.3 mo | - | OS correlated with the modified target mRECIST and EASL scores at 3 mo (p = 0.00 for both). |
| Rafi, S. et al. (2013) PS [56] | 19 pts 24 SIRT (4 with multiple SIRT treatments) refractory | - | Mean: 1.2 | Resin: 24 | RECIST at 3 mo: CR:0 PR: 10.5% SD: 68.4% PD: 21.0% | Median OS: 11.5 mo Median TTP: 4.8 mo | Median FU: 15 mo 12 deaths | - |
| Mouli, S. et al. (2013) PS [57] | 46 pts 92 SIRT (32 pts with multiple SIRT treatments) mixed | Median: 90.9 Right Lobe of liver: 95.4 Left lobe of liver: 114.7 | - | Glass: 46 | WHO at unspecified time: CR: 0 PR: 23.9% SD: 71.7% PD: 2.1% EASL at unspecified time: CR: 9% PR: 64% PD: 0 | No median OS | Median FU: 29 mo 39 deaths | - |
| Hoffman, R. T. et al. (2012) RS [58] | 33 pts (1 with multiple SIRT treatments) mixed | - | Mean: 1.5 | Resin: 33 | RECIST at 3 mo: CR: 0 PR: 36.4% SD: 51.5% PD: 15.2% | Median OS: 22 mo Median TTP: 9.8 mo | - | - |
| Haug, A. R. et al. (2011) RS [59] | 26 pts mixed | - | Mean: 1.7 | Resin: 26 | RECIST at 3 mo (23 pts): CR: 0 PR: 21.7% SD: 65.2% PD: 13.0% | Median OS: 11.7 mo | - | - |
| Saxena, A. et al. (2010) PS [60] | 25 pts mixed | - | Mean: 1.7 | Resin: 25 | RECIST at 8.1 mo (23 pts): CR: 0 PR: 26.0% SD: 47.8% PD: 21.7% | Median OS: 9.3 mo | Median FU: 8.1 mo 2 deaths | - |
| Ibrahim, S. M. et al. (2008) PS [61] | 24 pts mixed | Median: 105.1 | - | Glass: 24 | WHO at 1 mo (22 pts): CR: 0 PR: 27.2% SD: 68.1% PD: 4.5% | Median OS: 14.9 mo | Median FU: 17.7 mo 13 deaths | - |
| Author, Type of Study | Patient Population | Radiation Dosage, Gy | Activity, GBq | Microsphere Type: Number of Patients Treated | RECIST, WHO | Survival Outcomes | Follow-Up Information | Notes and Other Findings |
|---|---|---|---|---|---|---|---|---|
| Helmberger, T. et al. (2021) PS [62] | 120 pts NM | - | Median (entire liver): 1.3 Right lobe of liver: 1.2 Left lobe of liver: 0.8 | Resin: 120 | - | Median OS: 14.7 mo Median PFS: 5.7 mo | 24 mo | - |
| Lorenzoni, A. et al. (2020) RS [63] | 23 pts 30 SIRTs (7 pts with multiple SIRT treatments) Mixed * | Mean TD: 309 NTD: 42.4 | 2.5 | Glass: 30 | mRECIST at unspecified time: CR: 3% PR: 3% SD: 87% PD: 7% | Median OS: 21 mo Median PFS: 9 mo | - | Mean TD stable disease lesions: 280 Gy, responding lesions (CR + PR): 384 Gy |
| Core, J. et al. (2020) RS [64] | 32 pts 42 SIRT (Number of pts with multiple SIRT treatments unspecified) NM | Median TD: 253 | - | - | mRECIST at 3 mo (36 pts): CR: 33.3% PR: 58.3% SD: 8.3% PD: 0 | Median OS not reached. | Median FU: 10.9 mo | - |
| Pettinato, C. et al. (2019) RS [65] | 35 pts mixed | Mean TD: 455.7 Mean NTD: 13.9 | Mean: 1.4 | Resin: 35 | RECIST 1.1 at unspecified time: OR: 20% mRECIST at unspecified time: OR: 70% EASL at unspecified time: OR: 60% | Mean OS: 15.3 mo | 4 deaths | - |
| Schatka, I. et al. (2017) RS [66] | 33 pts refractory | - | Median: 1.8 | Resin: 33 | - | Median OS: 8 mo | - | - |
| Boni, G. et al. (2017) PS [67] | 20 pts, 29 SIRT (3 pts with multiple SIRT treatments) mixed | - | Mean: 0.97 | Resin: 29 | - | Median TTP: 7.3 mo | - | - |
| Peterson, J. et al. (2010) RS [68] | 9 pts NM | - | Median: 41 mCi † | Resin: 9 | (Criteria not mentioned) (7 pts) PR: 57%PD: 43% | OS at 9 mo: 89% | - | - |
| Author, Year, Type of Study | No. of Patients Receiving Concomitant Chemotherapy/Total Number of Patients | Chemotherapy Regimen | Definition | Analysis |
|---|---|---|---|---|
| Depalo, T. et al. (2021) RS [25] | 7/15 | - | No definitions available. Concomitant chemotherapy was distinct from chemotherapy given before SIRT. | No significant difference in SIRT + chemo vs. SIRT alone, in terms of radiosensitivity (p value not available). |
| Paz-Fumagalli, R. et al. (2021) RS [26] | - | Cisplatin + gemcitabine | Concomitant chemotherapy was administered in 45 days before or after SIRT. | Unified results |
| Riby, D. et al. (2020) RS [29] | 18/19 |
| Concomitant chemotherapy was administered on the day before or the day after SIRT, but not on the same day. | SIRT + chemo vs. chemo vs. surgery: RFS and recurrence rate statistically the same (p = 0.28 and p = 0.21, respectively). |
| Edeline, J. et al. (2020) PS [33] | 41/41 | Cisplatin 25 mg/m2 + gemcitabine 1000 mg/m2 (Gemcitabine reduced to 300 mg/m2 for concomitant administration) | SIRT administered in cycle 1 for ICC (one hemi-liver) or in cycles 1 and 3 (both hemi-livers) | 9 patients (22%) successfully down-staged to surgical resection. |
| Buettner, S. et al. (2020) RS [34] | 4/114 |
| No definitions available. Concomitant chemotherapy was distinct from chemotherapy given before or after SIRT. | - |
| White, J. et al. (2019) RS [37] | 7/61 | - | No definitions available. Concomitant chemotherapy was distinct from chemotherapy given before or after SIRT. | - |
| Bourien, H. et al. (2019) RS [39] | 33/64 |
| Chemotherapy was administered at most 3 months before SIRT. Chemotherapy administered more than 3 months before SIRT was considered induction chemotherapy. | Median PFS and median OS were not statistically different for the concomitant chemotherapy vs. induction vs. no chemotherapy groups (p = 0.90; p = 0.37, respectively). |
| Manceau, V. et al. (2018) RS [44] | 35/35 |
| Chemotherapy administered at most 3 months before SIRT. | The exact tumor dose threshold for response in SIRT concomitant with chemotherapy could not be defined, but was below 158 Gy. 17 patients (49%) had successful downstaging. |
| Akinwande, O. et al. (2017) RS [48] | 4/25 | - | - | The disease control rate was not affected by concomitant chemotherapy administration (p = 0.99) |
| Pieper, C. C. et al. (2016) RS [50] | 1/26 | - | - | Unified analysis of SIRT application for different malignancies revealed concurrent chemotherapy is a predictor of stasis in SIRT (OR, 8.69; p = 0.00) |
| Edeline, J. et al. (2015) RS [54] | 10/24 |
| Chemotherapy administered at most 3 months before SIRT. | The median PFS was higher in the concomitant chemotherapy group than in the induction group (p = 0.00). |
| Nezami, N. et al. (2019) PS [69] | 5/5 | Gemcitabine Dose level 1: 400 mg/m2 Dose level 2: 600 mg/m2 Dose level 3: 800 mg/m2 Dose level 4: 1000 mg/m2 | Chemotherapy on one day before SIRT for 1-lobe treatment and 38 days before SIRT for 2-lobe treatment. | No gemcitabine-related toxicity on dose levels 1 and 2. All hepatic toxicities were on dose level 4. RECIST at 3 m: 100% stable disease. |
| Authors (Year) | No. of Patients, Microsphere Type | Dosimetry after Treatment | Delivered Dose (Gy) | Activity (GBq) | Dose-Response Analysis |
|---|---|---|---|---|---|
| Willowson KP, et al. (2021) [22] | 18 pts Resin | 90Y PET-CT | No mean tumor dose is reported for the whole study participants. Dose to normal liver is measured with 99mTc-mebrofenin scintigraphy and is only reported as unified results with some HCC patients. | Median: 1.5 Mean: 1.62 | Average dose and minimum dose to 70% of lesion volume (Davg, D70) were not associated with lesion response (based on Total Lesion Glycolysis (TLG)) (p = 0.31, p = 0.60, respectively). TLG reduction of at least 50% was considered as significant response, with mean Davg of 74 Gy for responding vs. 61 Gy for non-responding lesions (p = 0.29) and D70 42 Gy vs. 27 Gy, respectively (p = 0.61). |
| Depalo, T. et al. (2021) [25] | 15 pts Resin | 90Y PET-CT | Mean TD: 93 NTD: 42 D70: 61 | Mean: 1.16 | Tumor Dose (Gy) showed positive effect on TTP on multivariate analysis (p = 0.05). D70 did not show any significant effect on TTP (p = 0.88) |
| Cheng B, et al. (2021) [27] | 38 pts Glass & Resin | 90Y SPECT-CT | Mean TD Resin: 78.9 Glass: 254.7 | - | Tumor Dose (Gy) thresholds to reach at least 80% specificity for tumor objective response Mean TD: Resin: 78.9 Glass: 254.7 Minimum TD: Resin: 53.7 Glass: 149.1 Maximum TD: Resin: 162.9 Glass: 591 D70: Resin: 68.1 Glass: 221.7. Resin: Median OS of 20.2 m vs. 6.5 m for those with mean TD ≥75 Gy vs. less (p = 0.00). Glass: Median OS of 14.6 vs. 2.6 Gy for the mean TD ≥150 vs. less (p = 0.03) |
| Nezami, N. (2018) [43] | 10 pts Glass & Resin | 90Y SPECT-CT | Mean TD: Glass: 205.7, Resin:128.9 (p < 0.001) Mean NTD: Glass: 42.4, Resin:53.6 (p < 0.001) Tumor to normal parenchyma ratio: Glass: 4.9, Resin: 2.4 (p < 0.001) | Mean Glass: 2.75 Resin: 1.67 (p < 0.001) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosseini Shabanan, S.; Nezami, N.; Abdelsalam, M.E.; Sheth, R.A.; Odisio, B.C.; Mahvash, A.; Habibollahi, P. Selective Internal Radiation Therapy with Yttrium-90 for Intrahepatic Cholangiocarcinoma: A Systematic Review on Post-Treatment Dosimetry and Concomitant Chemotherapy. Curr. Oncol. 2022, 29, 3825-3848. https://doi.org/10.3390/curroncol29060306
Hosseini Shabanan S, Nezami N, Abdelsalam ME, Sheth RA, Odisio BC, Mahvash A, Habibollahi P. Selective Internal Radiation Therapy with Yttrium-90 for Intrahepatic Cholangiocarcinoma: A Systematic Review on Post-Treatment Dosimetry and Concomitant Chemotherapy. Current Oncology. 2022; 29(6):3825-3848. https://doi.org/10.3390/curroncol29060306
Chicago/Turabian StyleHosseini Shabanan, Sedighe, Nariman Nezami, Mohamed E. Abdelsalam, Rahul Anil Sheth, Bruno C. Odisio, Armeen Mahvash, and Peiman Habibollahi. 2022. "Selective Internal Radiation Therapy with Yttrium-90 for Intrahepatic Cholangiocarcinoma: A Systematic Review on Post-Treatment Dosimetry and Concomitant Chemotherapy" Current Oncology 29, no. 6: 3825-3848. https://doi.org/10.3390/curroncol29060306
APA StyleHosseini Shabanan, S., Nezami, N., Abdelsalam, M. E., Sheth, R. A., Odisio, B. C., Mahvash, A., & Habibollahi, P. (2022). Selective Internal Radiation Therapy with Yttrium-90 for Intrahepatic Cholangiocarcinoma: A Systematic Review on Post-Treatment Dosimetry and Concomitant Chemotherapy. Current Oncology, 29(6), 3825-3848. https://doi.org/10.3390/curroncol29060306