Blockade of ALDH in Cisplatin-Resistant Ovarian Cancer Stem Cells In Vitro Synergistically Enhances Chemotherapy-Induced Cell Death


Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Lines and Cell Culture
2.2. Drug Sensitivity Measuring by MTT Assay
2.3. Clonogenicity Assay
2.4. Flow Cytometric Analysis of ALDH Activity
2.5. Flow Cytometric Analysis of Cell Cycle
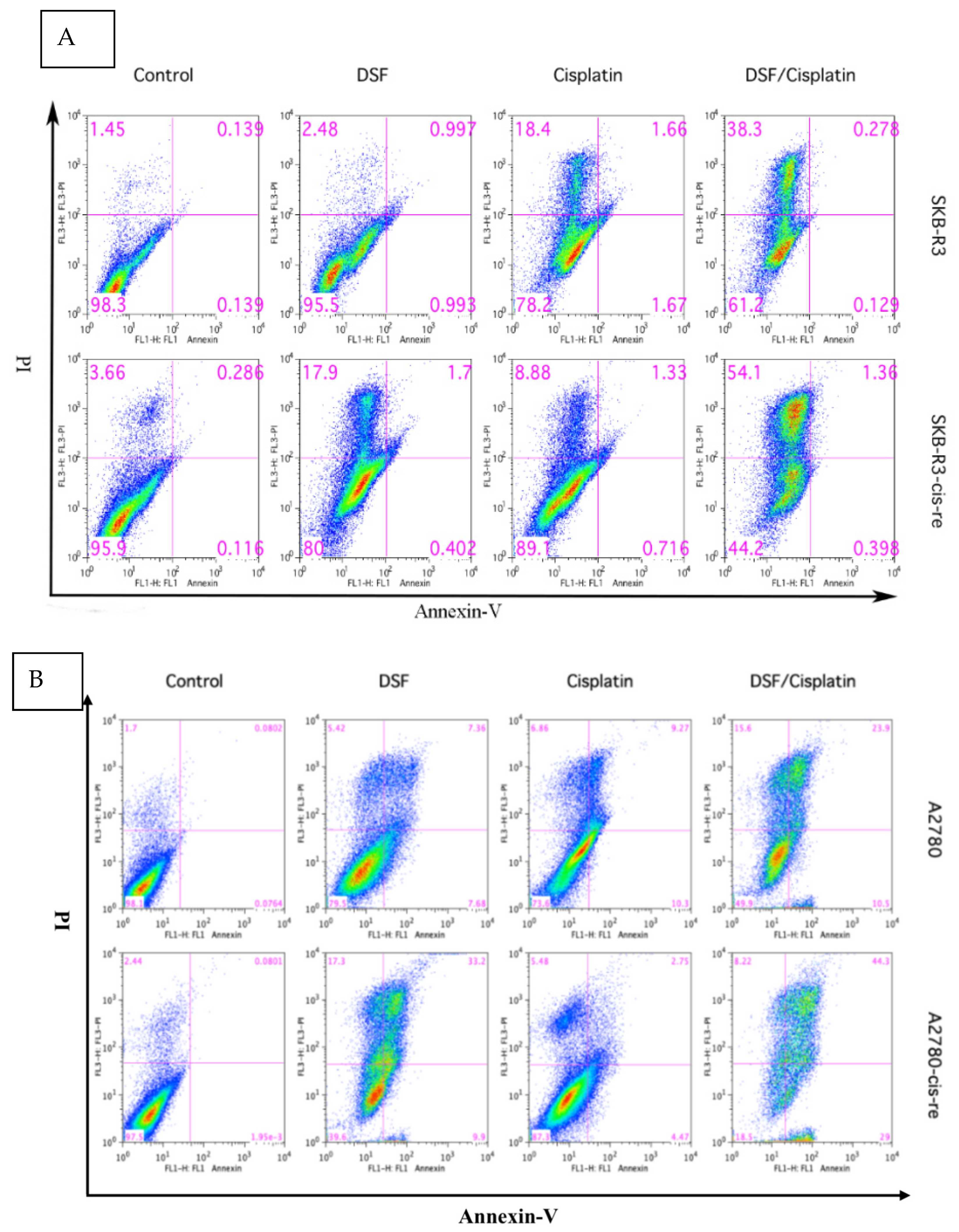
2.6. Flow Cytometric Analysis of Cellular Apoptosis
2.7. Two- and Three-Drug Combination Treatment
2.8. Combination Effect Analyses
2.9. Further Verification of DSF Potentiation of Chemotherapeutic Drug Sensitivity
2.10. Patient Selection
2.11. Droplet-Based scRNA-Seq
2.12. Statistical Analysis
3. Results
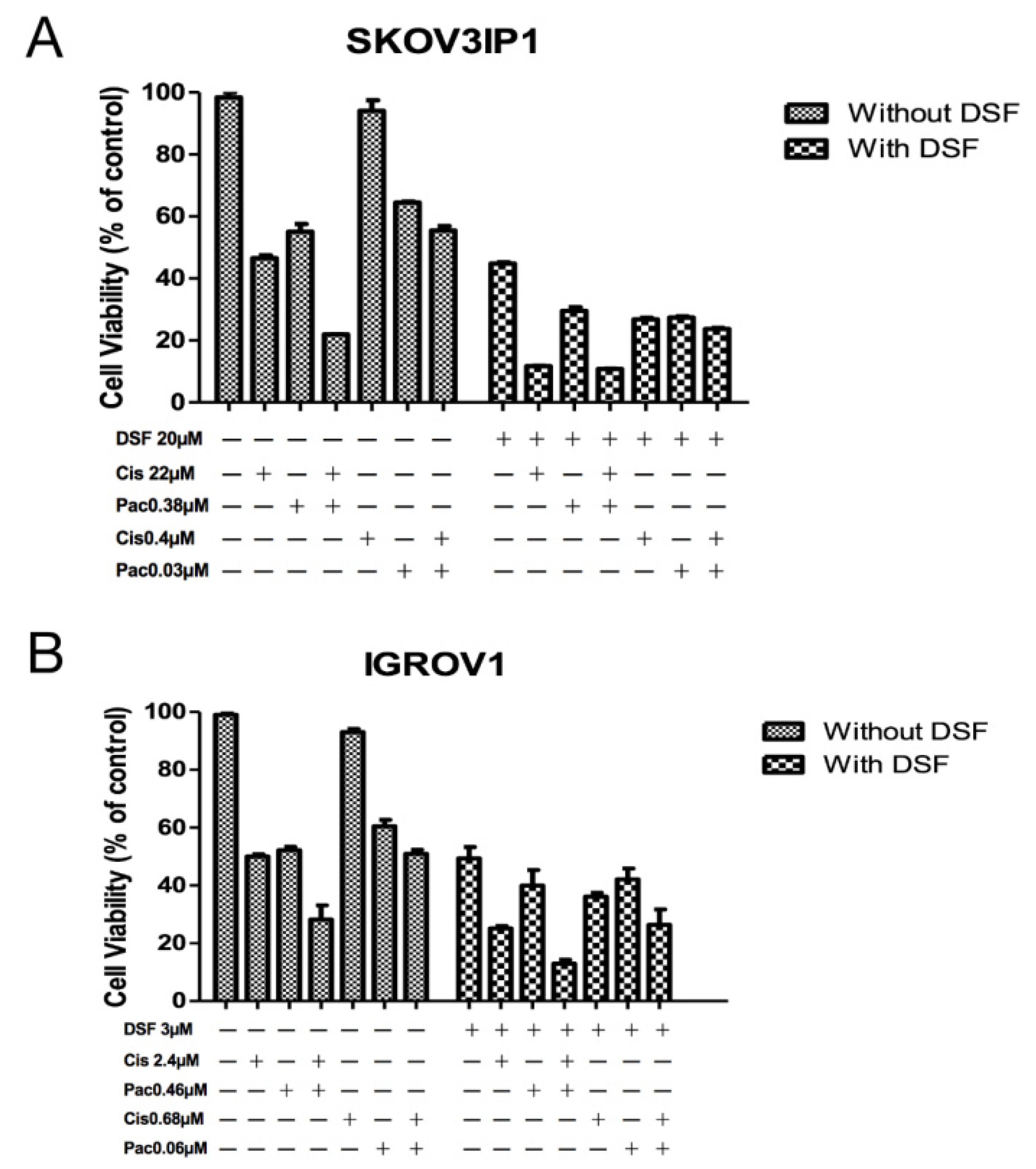
3.1. Quantitative Analysis of Enhanced Cell Line Sensitivity to Two- and Three-Drug Combinations
3.2. Verification of Chemotherapy Drug Effect Potentiation by DSF
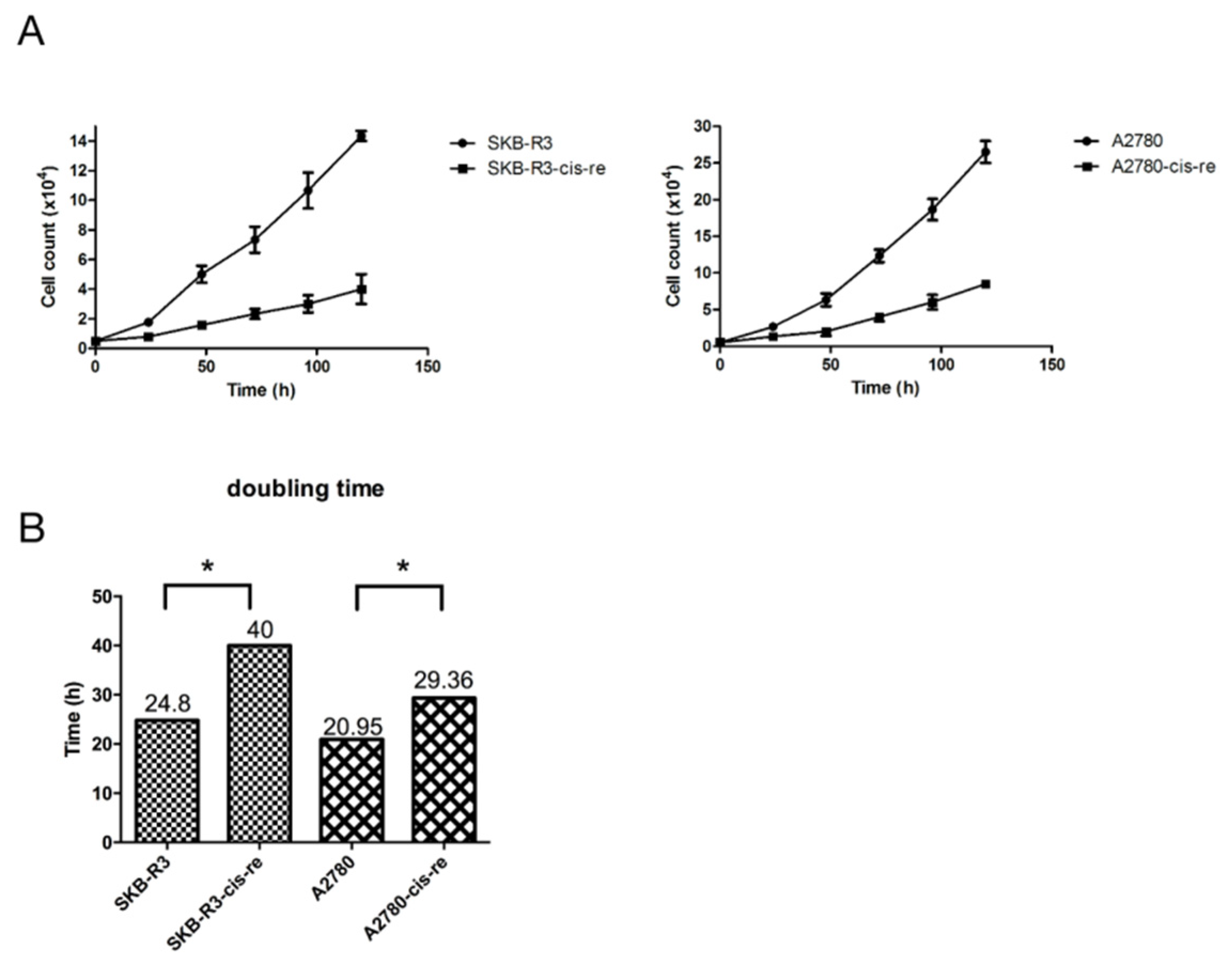
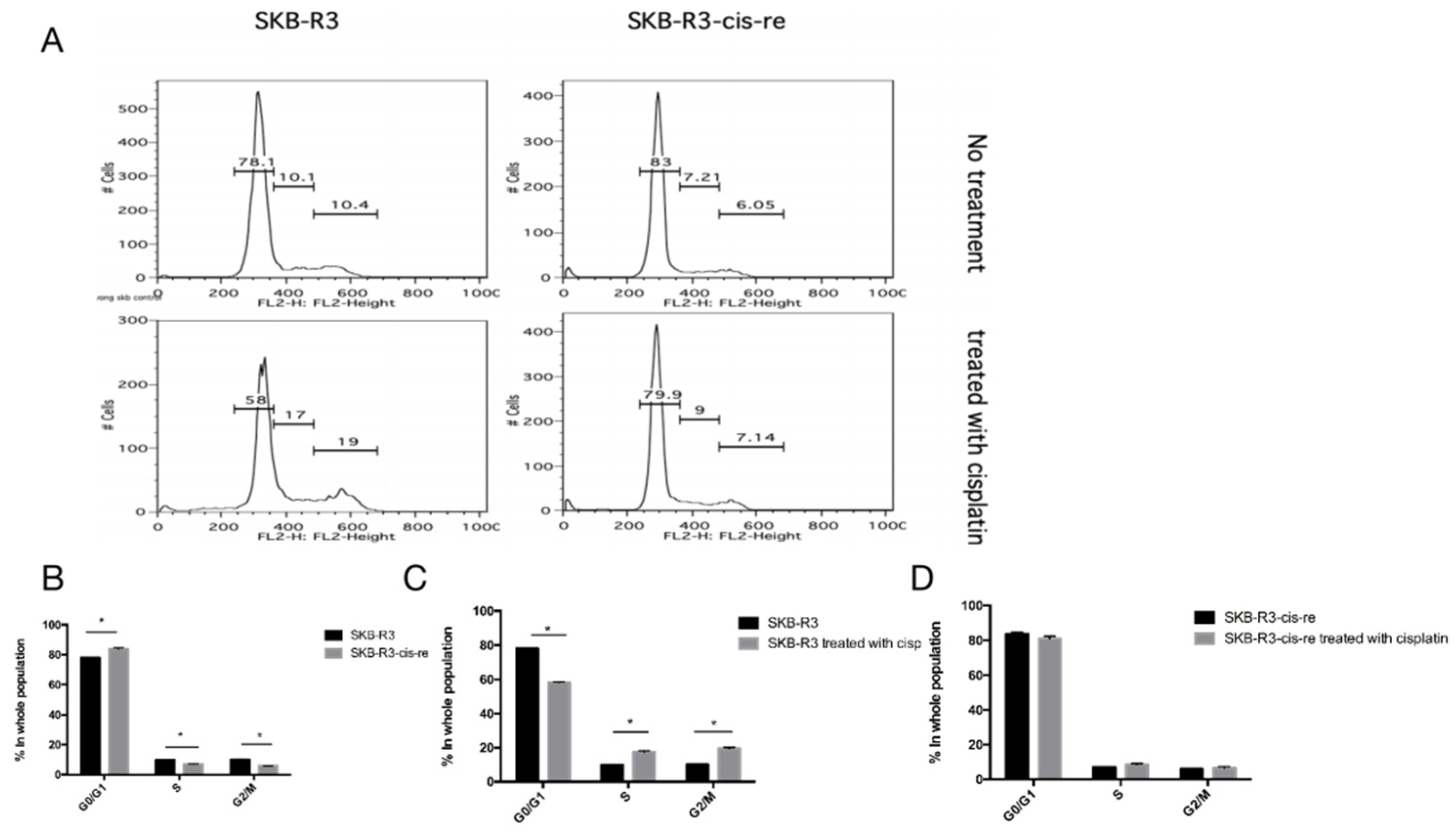
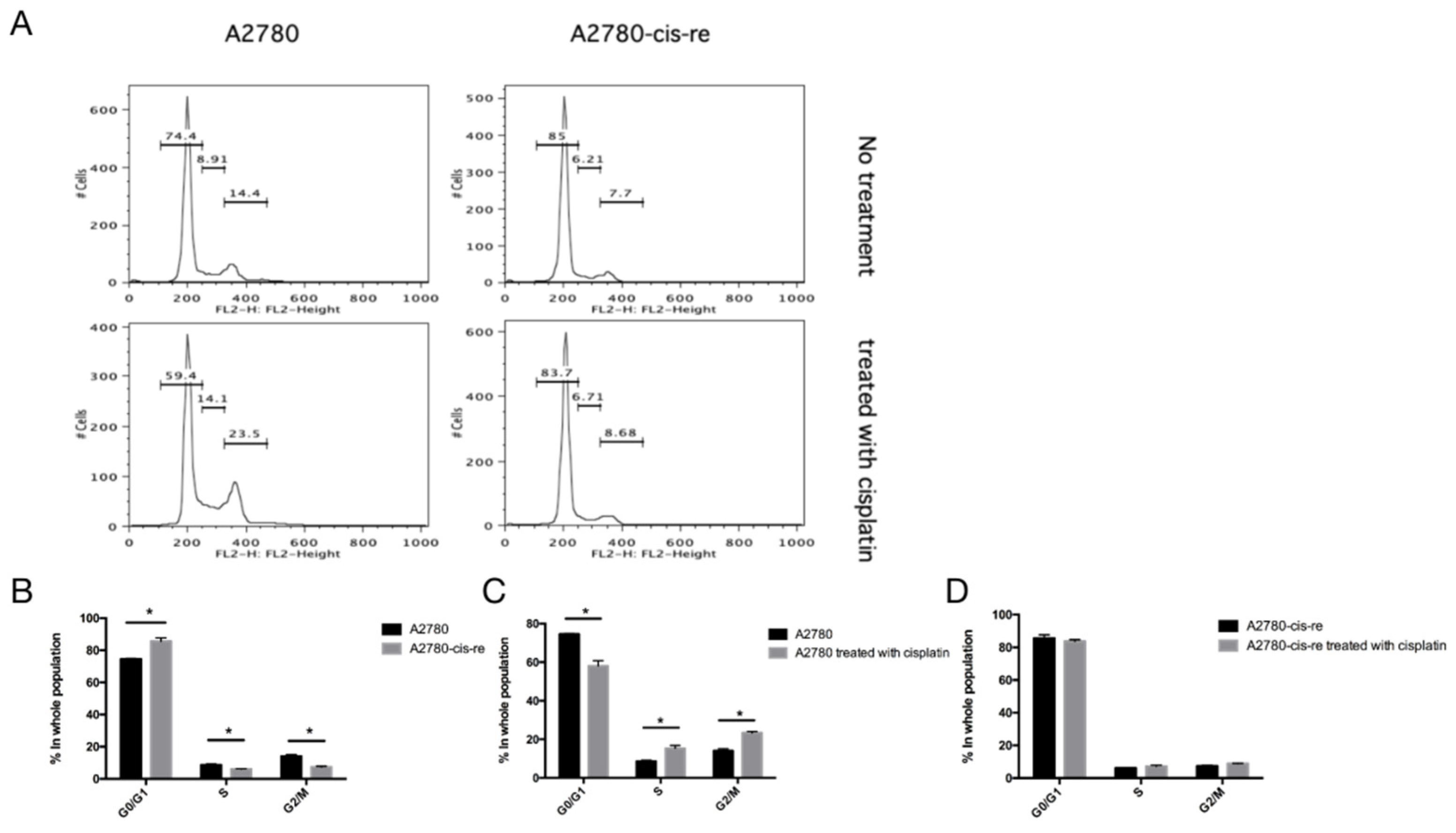
3.3. Characterization of Cisplatin-Resistant Cell Lines for Proliferation and ALDH Expression
3.4. Disulfiram Is Highly Cytotoxic in Cisplatin-Resistant Cells
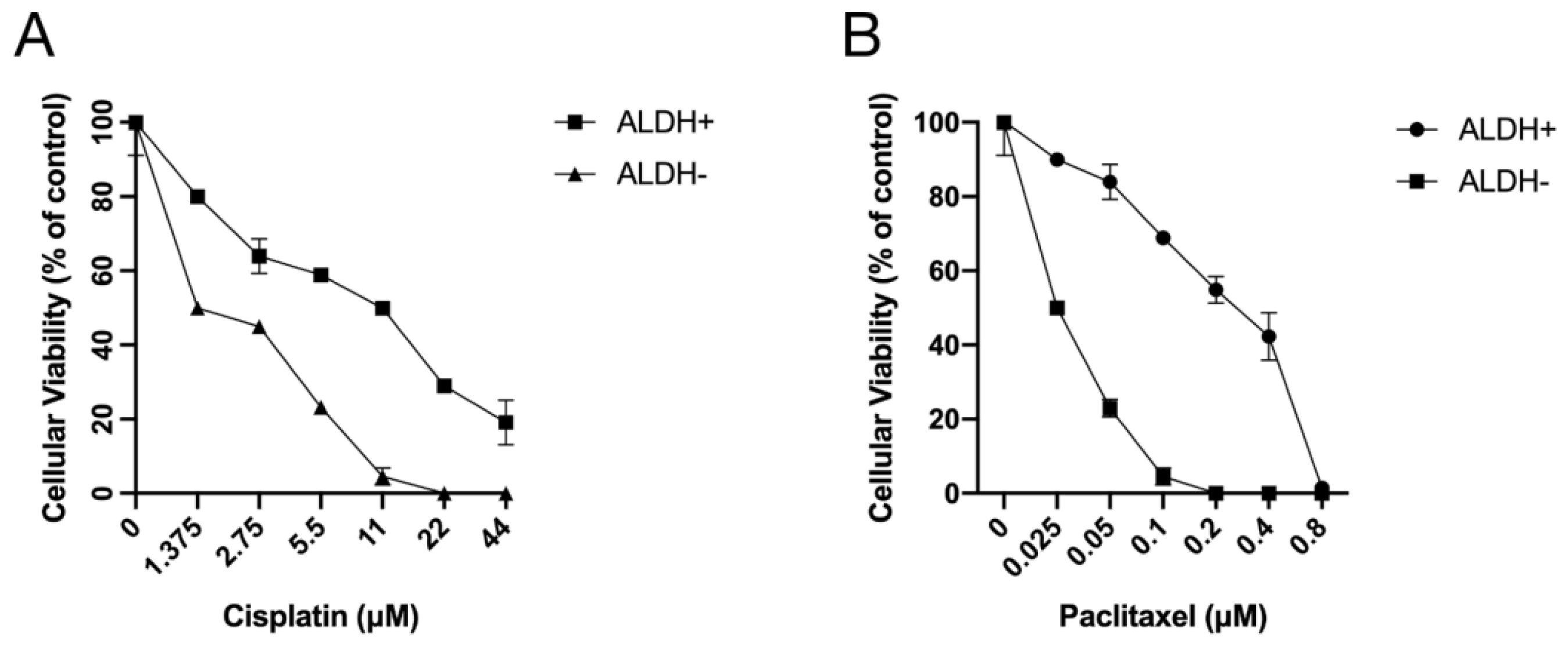
3.5. ALDH+ Cells were Relatively More Resistant to Chemotherapeutics
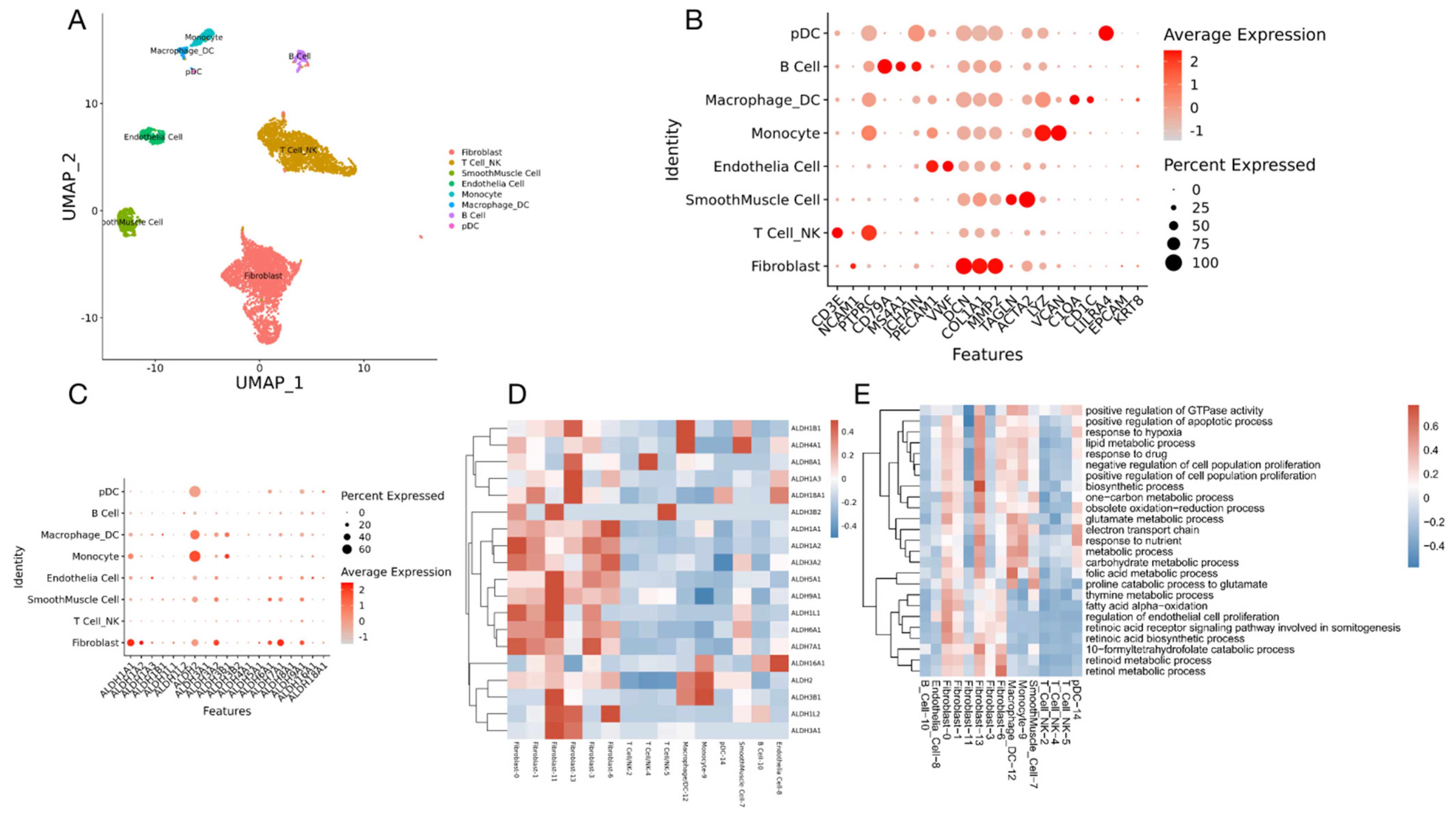
3.6. scRNA-Seq Analysis of High-Grade Serous Ovarian Cancer
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grabowski, J.P.; Sehouli, J. Current management of ovarian cancer. Minerva Med. 2015, 106, 151–156. [Google Scholar] [PubMed]
- Wefers, C.; Lambert, L.J.; Torensma, R.; Hato, S.V. Cellular immunotherapy in ovarian cancer: Targeting the stem of recurrence. Gynecol. Oncol. 2015, 137, 335–342. [Google Scholar] [CrossRef] [PubMed]
- David, H. Ovarian cancer: Beyond resistance. Nature 2015, 527, 7579. [Google Scholar]
- Hennessy, B.T.; Coleman, R.L.; Markman, M. Ovarian cancer. Lancet 2009, 374, 1371–1382. [Google Scholar] [CrossRef]
- Parmar, M.K.; Ledermann, J.A.; Colombo, N.; du Bois, A.; Delaloye, J.F.; Kristensen, G.B.; Wheeler, S.; Swart, A.M.; Qian, W.; Torri, V.; et al. Paclitaxel plus platinum-based chemotherapy versus conventional platinum-based chemotherapy in women with relapsed ovarian cancer: The ICON4/AGO-OVAR-2.2 trial. Lancet 2003, 361, 2099–2106. [Google Scholar] [PubMed]
- Parte, S.C.; Batra, S.K.; Kakar, S.S. Characterization of stem cell and cancer stem cell populations in ovary and ovarian tumors. J. Ovarian Res. 2018, 11, 69. [Google Scholar] [CrossRef]
- Guo, F.; Yang, Z.; Kulbe, H.; Albers, A.E.; Sehouli, J.; Kaufmann, A.M. Inhibitory effect on ovarian cancer ALDH+ stem-like cells by Disulfiram and Copper treatment through ALDH and ROS modulation. Biomed. Pharmacother. 2019, 118, 109371. [Google Scholar] [CrossRef]
- Rodriguez-Torres, M.; Allan, A.L. Aldehyde dehydrogenase as a marker and func- tional mediator of metastasis in solid tumors. Clin. Exp. Metastasis 2016, 33, 97–113. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Liao, Y.; Liu, N.; Hua, X.; Cai, J.; Yang, C.; Long, H.; Zhao, C.; Chen, X.; Lan, X.; et al. Two clinical drugs deubiquitinase inhibitor auranofin and aldehyde dehydrogenase inhibitor disulfiram triggersynergistic anti-tumor effects in vitro and in vivo. Oncotarget 2016, 7, 2796–2808. [Google Scholar] [CrossRef] [Green Version]
- Saw, Y.-T.; Yang, J.; Ng, S.-K.; Liu, S.; Singh, S.; Singh, M.; Welch, W.R.; Tsuda, H.; Fong, W.-P.; Thompson, D.; et al. Characterization of aldehyde dehydrogenase isozymes in ovarian cancer tissues and sphere cultures. BMC Cancer 2012, 12, 329. [Google Scholar] [CrossRef] [Green Version]
- Wintzell, M.; Lofstedt, L.; Johansson, J.; Pedersen, A.B.; Fuxe, J.; Shoshan, M. Repeated cisplatin treatment can lead to a multiresistant tumor cell population with stem cell features and sensitivity to 3-bromopyruvate. Cancer Biol. Ther. 2012, 13, 1454–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahar, E.; Kim, J.-Y.; Kim, H.-S.; Yoon, H. Establishment of acquired cisplatin resistance in ovarian cancer cell lines characterized by enriched metastatic properties with increased twist expression. Int. J. Mol. Sci. 2020, 21, 7613. [Google Scholar] [CrossRef] [PubMed]
- Chou, T.C.; Talalay, P. Quantitative analysis of dose-effect relationships: The combined effects of multiple drugs or enzyme inhibitors. Adv. Enzyme Regul. 1984, 22, 27–55. [Google Scholar] [CrossRef]
- Chou, T.C.; Motzer, R.J.; Tong, Y.; Bosl, G.J. Computerized quantitation of synergism and antagonism of taxol, topotecan, and cisplatin against human teratocarcinoma cell growth: A rational approach to clinical protocol design. J. Natl. Cancer Inst. 1994, 86, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, S.; Mehta, P.; Xie, Y.; Lei, Y.L.; Mehta, G. Ovarian cancer stem cells and macrophages reciprocally interact through the WNT pathway to promote pro-tumoral and malignant phenotypes in 3D engineered microenvironments. J. Immunother. Cancer 2019, 7, 190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Z.; Guo, F.; Albers, A.E.; Sehouli, J.; Kaufmann, A.M. Disulfiram modulates ROS accumulation and overcomes synergistically cisplatin resistance in breast cancer cell lines. Biomed. Pharmacother. 2019, 113, 108727. [Google Scholar] [CrossRef]
- Cannistra, S.A. Cancer of the ovary. N. Engl. J. Med. 2004, 351, 2519–2529. [Google Scholar] [CrossRef]
- Colombo, P.E.; Fabbro, M.; Theillet, C. Sensitivity and resistance to treatment in the primary management of epithelial ovarian cancer. Crit. Rev. Oncol. Hematol. 2014, 89, 207–216. [Google Scholar] [CrossRef]
- Zheng, Z.-G.; Xu, H.; Suo, S.-S.; Xu, X.-L.; Ni, M.-W.; Gu, L.-H.; Chen, W.; Wang, L.-Y.; Zhao, Y.; Tian, B.; et al. The essential role of H19 contributing to cisplatin resistance by regulating glutathione metabolism in high-grade serous ovarian cancer. Sci. Rep. 2016, 6, 26093. [Google Scholar] [CrossRef] [Green Version]
- Galluzzi, L.; Senovilla, L.; Vitale, I.; Michels, J.; Martins, I.; Kepp, O.; Castedo, M.; Kroemer, G. Molecular mechanisms of cisplatin resistance. Oncogene 2012, 31, 1869–1883. [Google Scholar] [CrossRef] [Green Version]
- Pacioni, S.; D’Alessandris, Q.G.; Giannetti, S.; Morgante, L.; De Pascalis, I.; Coccè, V.; Bonomi, A.; Pascucci, L.; Alessandri, G.; Pessina, A.; et al. Mesenchymal stromal cells loaded with paclitaxel induce cytotoxic damage in glioblastoma brain xenografts. Stem. Cell Res. Ther. 2015, 6, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gornstein ESchwarz, T.L. The paradox of paclitaxel neurotoxicity: Mechanisms and unanswered questions. Neuropharmacology 2014, 76, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Tambe, M.; Pruikkonen, S.; Mäki-Jouppila, J.; Chen, P.; Elgaaen, B.V.; Straume, A.H.; Huhtinen, K.; Cárpen, O.; Lønning, P.E.; Davidson, B.; et al. Novel Mad2-targeting miR-493-3p controls mitotic fidelity and cancer cells’ sensitivity to paclitaxel. Oncotarget 2016, 7, 12267–12285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergmann, T.K.; Brasch-Andersen, C.; Gréen, H.; Mirza, M.R.; Skougaard, K.; Wihl, J.; Keldsen, N.; Damkier, P.; Peterson, C.; Vach, W.; et al. Impact of ABCB1 variants on neutrophil depression: A pharmacogenomics study of paclitaxel in 92 women with ovarian cancer. Basis Clin. Pharmacol. Toxicol. 2012, 110, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Amini, A.; Masoumi-Moghaddam, S.; Ehteda, A.; Liauw, W.; Morris, D.L. Potentiation of chemotherapeutics by bromelain and N-acetylcysteine: Sequential and combination therapy of gastrointestinal cancer cells. Am. J. Cancer Res. 2016, 6, 350–369. [Google Scholar]
- Bergmann, T.K.; Brasch-Andersen, C.; Gréen, H.; Mirza, M.R.; Skougaard, K.; Wihl, J.; Keldsen, N.; Damkier, P.; Peterson, C.; Vach, W.; et al. Targeting aldehyde dehydrogenase Cancer stem cells in ovarian Cancer. Mol. Cancer Ther. 2010, 9, 3186–3199. [Google Scholar]
- Hu, H.; Cui, L.; Lu, J.; Wei, K.; Wei, J.; Li, S.; Zou, C.; Chen, T. Intestinal microbiota regulates anti-tumor effect of disulfiram combined with Cu2+ in a mice model. Cancer Med. 2020, 9, 6791–6801. [Google Scholar] [CrossRef]
- Zhao, Y.Z.; Lin, M.T.; Lan, Q.H.; Zhai, Y.Y.; Xu, H.L.; Xiao, J.; Kou, L.; Yao, Q. Silk fibroin-modified disulfiram/zinc oxide nanocomposites for pH triggered release of Zn2+ and synergistic antitumor efficacy. Mol. Pharm. 2020, 17, 3857–3869. [Google Scholar] [CrossRef]
- Chen, D.; Wu, M.; Li, Y.; Chang, I.; Yuan, Q.; Ekimyan-Salvo, M.; Deng, P.; Yu, B.; Yu, Y.; Dong, J.; et al. Targeting BMI1+ cancer stem cells overcomes chemoresistance and inhibits metastases in squamous cell carcinoma. Cell Stem Cell 2017, 20, 621–634.e6. [Google Scholar] [CrossRef] [Green Version]
- Keeratichamroen, S.; Lirdprapamongkol, K.; Svasti, J. Mechanism of ECM-induced dormancy and chemoresistance in A549 human lung carcinoma cells. Oncol. Rep. 2018, 39, 1765–1774. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.H.; Wang, H.S.; Soong, Y.K. Paclitaxel-induced cell death: Where the cell cycle and apoptosis come together. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2000, 88, 2619–2628. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Combination | Combination Index at | Dose-Reduction Index at | ||||
|---|---|---|---|---|---|---|
| IC50 | IC75 | IC90 | IC50 | IC75 | IC90 | |
| Cis + Pac | 0.104 | 0.267 | 3.170 | 51.06 11.89 | 4.02 54.81 | 0.32 252.58 |
| Cis + DSF | 0.123 | 0.176 | 0.311 | 11.74 37.36 | 4.80 156.08 | 1.97 652.05 |
| Pac + DSF | 1.021 | 0.048 | 0.004 | 1.05 14.36 | 29.81 70.96 | 845.61 350.68 |
| Cis + Pac + DSF | 0.286 | 0.110 | 0.196 | 49.80 11.60 158.48 | 5.39 73.59 175.17 | 1 466.87 193.61 |
| Drug Combination | Combination Index at | Dose-Reduction Index at | ||||
|---|---|---|---|---|---|---|
| IC50 | IC75 | IC90 | IC50 | IC75 | IC90 | |
| Cis + Pac | 0.42 | 0.36 | 0.36 | 3.50 7.38 | 3.23 18.88 | 2.97 48.29 |
| Cis + DSF | 0.24 | 0.33 | 0.52 | 5.09 25.38 | 3.15 57.17 | 1.95 128.76 |
| Pac + DSF | 2.99 | 24.49 | 202.63 | 0.47 1.12 | 0.05 0.17 | 0.006 0.02 |
| Cis + Pac + DSF | 0.32 | 0.19 | 0.16 | 5.28 11.12 26.30 | 6.24 36.49 113.13 | 7.38 119.78 486.71 |
| Cell Line | IC50 (uM) |
|---|---|
| SKB-R3 | 2.87 ± 0.72 |
| SKB-R3-cis-re | 7.38 ± 1.23 |
| A2780 | 3.39 ± 1.12 |
| A2780-cis-re | 8.64 ± 2.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, F.; Yang, Z.; Sehouli, J.; Kaufmann, A.M. Blockade of ALDH in Cisplatin-Resistant Ovarian Cancer Stem Cells In Vitro Synergistically Enhances Chemotherapy-Induced Cell Death. Curr. Oncol. 2022, 29, 2808-2822. https://doi.org/10.3390/curroncol29040229
Guo F, Yang Z, Sehouli J, Kaufmann AM. Blockade of ALDH in Cisplatin-Resistant Ovarian Cancer Stem Cells In Vitro Synergistically Enhances Chemotherapy-Induced Cell Death. Current Oncology. 2022; 29(4):2808-2822. https://doi.org/10.3390/curroncol29040229
Chicago/Turabian StyleGuo, Fang, Zhi Yang, Jalid Sehouli, and Andreas M. Kaufmann. 2022. "Blockade of ALDH in Cisplatin-Resistant Ovarian Cancer Stem Cells In Vitro Synergistically Enhances Chemotherapy-Induced Cell Death" Current Oncology 29, no. 4: 2808-2822. https://doi.org/10.3390/curroncol29040229
APA StyleGuo, F., Yang, Z., Sehouli, J., & Kaufmann, A. M. (2022). Blockade of ALDH in Cisplatin-Resistant Ovarian Cancer Stem Cells In Vitro Synergistically Enhances Chemotherapy-Induced Cell Death. Current Oncology, 29(4), 2808-2822. https://doi.org/10.3390/curroncol29040229