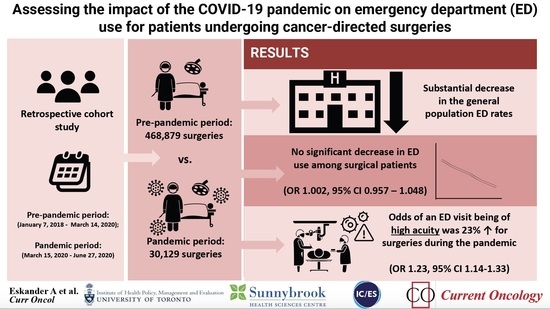
Assessing the Impact of the COVID-19 Pandemic on Emergency Department Use for Patients Undergoing Cancer-Directed Surgeries

 , ,
, ,  , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Sources
2.3. Main Exposure, Outcome and Other Covariates
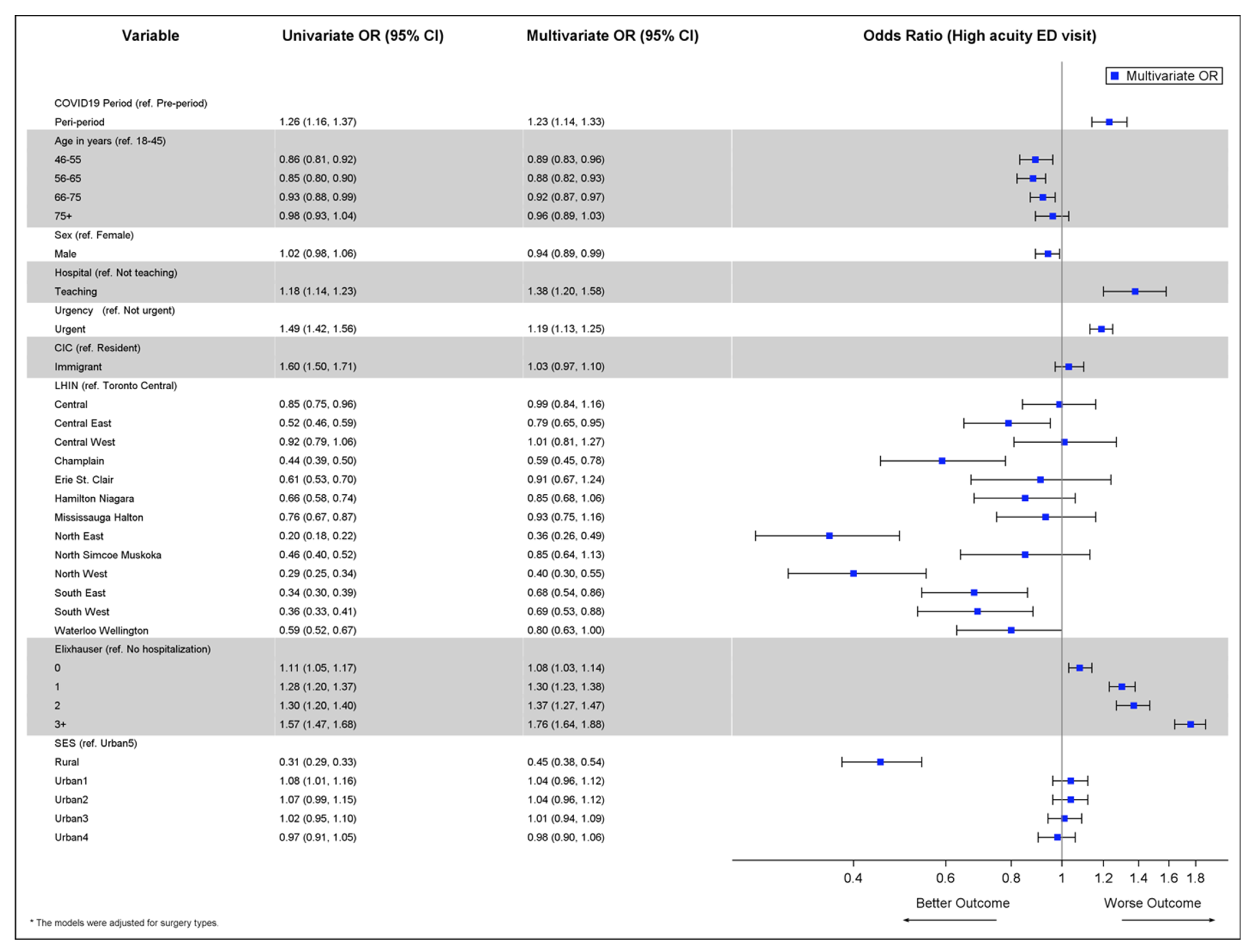
2.4. Statistical Analysis
2.5. Ethical Standards
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-CoV-2: A multicenter study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef]
- Yang, F.; Shi, S.; Zhu, J.; Shi, J.; Dai, K.; Chen, X. Clinical characteristics and outcomes of cancer patients with COVID-19. J. Med. Virol. 2020, 92, 2067–2073. [Google Scholar] [CrossRef] [PubMed]
- Al-Shamsi, H.O.; Alhazzani, W.; Alhuraiji, A.; Coomes, E.A.; Chemaly, R.F.; Almuhanna, M.; Wolff, R.A.; Ibrahim, N.K.; Chua, M.L.; Hotte, S.J.; et al. A Practical Approach to the Management of Cancer Patients During the Novel Coronavirus Disease 2019 (COVID-19) Pandemic: An International Collaborative Group. Oncologist 2020, 25, e936–e945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, H.; Liu, K.; Li, M.; Tang, S.; Monte, A.A.; Wang, J.; Nie, S.; Rui, Q.; Liu, W.; Qin, H.; et al. The influence of coronavirus disease 2019 on emergency department visits in Nanjing, China: A multicentre cross-sectional study. Am. J. Emerg. Med. 2020, 38, 2101–2109. [Google Scholar] [CrossRef] [PubMed]
- Butt, A.A.; Azad, A.M.; Kartha, A.B.; Masoodi, N.A.; Bertollini, R.; Abou-Samra, A.-B. Volume and Acuity of Emergency Department Visits Prior To and After COVID-19. J. Emerg. Med. 2020, 59, 730–734. [Google Scholar] [CrossRef] [PubMed]
- Glazier, R.H.; Green, M.E.; Wu, F.C.; Frymire, E.; Kopp, A.; Kiran, T. Shifts in office and virtual primary care during the early COVID-19 pandemic in Ontario, Canada. Can. Med. Assoc. J. 2021, 193, E200–E210. [Google Scholar] [CrossRef]
- Hanna, T.P.; King, W.D.; Thibodeau, S.; Jalink, M.; Paulin, G.A.; Harvey-Jones, E.; O’Sullivan, D.E.; Booth, C.M.; Sullivan, R.; Aggarwal, A. Mortality due to cancer treatment delay: Systematic review and meta-analysis. BMJ 2020, 371, m4087. [Google Scholar] [CrossRef]
- Eskander, A.; Li, Q.; Hallet, J.; Coburn, N.; Hanna, T.P.; Irish, J.; Sutradhar, R. Access to Cancer Surgery in a Universal Health Care System During the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e211104. [Google Scholar] [CrossRef]
- Juurlink, D.; Preyra, C.; Croxford, R.; Chong, A.; Austin, P.; Tu, J.; Laupacis, A. Canadian Institute for Health Information Discharge Abstract Database: A Validation Study; Institute for Clinical Evaluative Sciences: Toronto, ON, Canada, 2006; Available online: https://www.ices.on.ca/publications/atlases-and-reports/2006/canadian-institute-for-health-information (accessed on 30 November 2021).
- Iron, K.; Zagorski, B.; Sykora, K.; Manuel, D. Living and Dying in Ontario: An Opportunity to Improve Health Information; Institute of Clinical Evaluative Sciences: Toronto, ON, Canada, 2008; Available online: https://www.ices.on.ca/Publications/Atlases-and-Reports/2008/Living-and-dying-in-Ontario (accessed on 30 November 2021).
- Matheson, F.; Dunn, J.; Smith, K.; Moineddin, R.; Glazier, R. Ontario Marginalization Index (ON-Marg): User Guide; Centre for Research in Inner City Health, St Michael’s Hospital: Toronto, ON, Canada, 2011. [Google Scholar]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity Measures for Use with Administrative Data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Hall, S.F. A user’s guide to selecting a comorbidity index for clinical research. J. Clin. Epidemiol. 2006, 59, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, K.A.; Sutradhar, R.; Borkhoff, C.M.; Baxter, N.; Lofters, A.; Rabeneck, L.; Tinmouth, J.; Paszat, L.; Ontario Cancer Screening Research Network. Small-area variation in screening for cancer, glucose and cholesterol in Ontario: A cross-sectional study. CMAJ Open 2015, 3, E373–E381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beveridge, R. The Canadian Triage and Acuity Scale: A new and critical element in health care reform. Canadian Association of Emergency Physicians. J. Emerg. Med. 1998, 16, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Sutradhar, R.; Agha, M.M.; Pole, J.; Greenberg, M.; Guttmann, A.; Hodgson, D.C.; Nathan, P.C. Specialized survivor clinic attendance is associated with decreased rates of emergency department visits in adult survivors of childhood cancer. Cancer 2015, 121, 4389–4397. [Google Scholar] [CrossRef] [PubMed]
- Boyle, L.I.; Boyle, A.; Jay, S.; Marnewick, J. COVID-19 lockdown impact on common general surgical acute presentations to a regional centre in New Zealand. N. Z. Med. J. 2020, 133, 96–105. [Google Scholar] [PubMed]
- McLean, R.C.; Young, J.; Musbahi, A.; Lee, J.X.; Hidayat, H.; Abdalla, N.; Chowdhury, S.; Baker, E.A.; Etherson, K.J. A single-centre observational cohort study to evaluate volume and severity of emergency general surgery admissions during the COVID-19 pandemic: Is there a “lockdown” effect? Int. J. Surg. 2020, 83, 259–266. [Google Scholar] [CrossRef]
- Metelmann, I.B.; Busemann, A. Elective surgery in times of COVID-19: A two-centre analysis of postponed operations and disease-related morbidity and mortality. Z. Evid. Fortbild. Qual. Gesundh. Wesen 2020, 158, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Knisely, A.; Zhou, Z.N.; Wu, J.; Huang, Y.; Holcomb, K.; Melamed, A.; Advincula, A.P.; Lalwani, A.; Khoury-Collado, F.; Tergas, A.I.; et al. Perioperative Morbidity and Mortality of Patients With COVID-19 Who Undergo Urgent and Emergent Surgical Procedures. Ann. Surg. 2021, 273, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Hakim, A.A.; Kellish, A.S.; Atabek, U.; Spitz, F.R.; Hong, Y.K. Implications for the use of telehealth in surgical patients during the COVID-19 pandemic. Am. J. Surg. 2020, 220, 48–49. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Pre-COVID-19 * (N = 65,309) | COVID-19 (N = 30,129) | Standardized Difference a |
|---|---|---|---|
| Age (Mean ± SD) | 56.2 ± 16.9 | 57.9 ± 17.2 | 0.10 |
| Female | 40,341 (61.8%) | 17,488 (58.0%) | 0.08 |
| Rural Score (Rio 2008)—0–9 | 42,447 (65.8%) | 19,203 (64.6%) | 0.03 |
| 10–30 | 11,996 (18.6%) | 5689 (19.2%) | 0.01 |
| 31–50 | 7176 (11.1%) | 3435 (11.6%) | 0.01 |
| 51–70 | 1962 (3.0%) | 929 (3.1%) | 0 |
| 71+ (more rural) | 902 (1.4%) | 456 (1.5%) | 0.01 |
| Immigrant | 9583 (14.7%) | 3813 (12.7%) | 0.06 |
| Elixhauser Grouping b—0 | 9380 (14.4%) | 4262 (14.1%) | 0.01 |
| 1 | 5664 (8.7%) | 3089 (10.3%) | 0.05 |
| 2 | 3426 (5.2%) | 1955 (6.5%) | 0.05 |
| 3+ | 4572 (7.0%) | 2689 (8.9%) | 0.07 |
| No Hospitalization | 42,267 (64.7%) | 18,134 (60.2%) | 0.09 |
| Material Deprivation Quintile 1—Least Deprived | 14,252 (22.0%) | 6602 (22.1%) | 0 |
| 2 | 13,916 (21.5%) | 6108 (20.5%) | 0.03 |
| 3 | 12,377 (19.1%) | 5763 (19.3%) | 0 |
| 4 | 12,018 (18.6%) | 5626 (18.9%) | 0.01 |
| 5—Most Deprived | 12,146 (18.8%) | 5734 (19.2%) | 0.01 |
| Inpatient Surgery c | 28,080 (43.0%) | 17,779 (59.0%) | 0.32 |
| Non-Teaching Hospital Status | 47,657 (73.0%) | 20,384 (67.7%) | 0.12 |
| Urgent d | 9451 (14.5%) | 8410 (27.9%) | 0.33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eskander, A.; Li, Q.; Yu, J.; Hallet, J.; Coburn, N.; Dare, A.; Chan, K.K.W.; Singh, S.; Parmar, A.; Earle, C.C.; et al. Assessing the Impact of the COVID-19 Pandemic on Emergency Department Use for Patients Undergoing Cancer-Directed Surgeries. Curr. Oncol. 2022, 29, 1877-1889. https://doi.org/10.3390/curroncol29030153
Eskander A, Li Q, Yu J, Hallet J, Coburn N, Dare A, Chan KKW, Singh S, Parmar A, Earle CC, et al. Assessing the Impact of the COVID-19 Pandemic on Emergency Department Use for Patients Undergoing Cancer-Directed Surgeries. Current Oncology. 2022; 29(3):1877-1889. https://doi.org/10.3390/curroncol29030153
Chicago/Turabian StyleEskander, Antoine, Qing Li, Jiayue Yu, Julie Hallet, Natalie Coburn, Anna Dare, Kelvin K. W. Chan, Simron Singh, Ambica Parmar, Craig C. Earle, and et al. 2022. "Assessing the Impact of the COVID-19 Pandemic on Emergency Department Use for Patients Undergoing Cancer-Directed Surgeries" Current Oncology 29, no. 3: 1877-1889. https://doi.org/10.3390/curroncol29030153
APA StyleEskander, A., Li, Q., Yu, J., Hallet, J., Coburn, N., Dare, A., Chan, K. K. W., Singh, S., Parmar, A., Earle, C. C., Lapointe-Shaw, L., Krzyzanowska, M. K., Hanna, T. P., Finelli, A., Louie, A. V., Look-Hong, N., Irish, J. C., Witterick, I., Mahar, A., ... on behalf of the Pandemic—Ontario Collaborative in Cancer Research (POCCR). (2022). Assessing the Impact of the COVID-19 Pandemic on Emergency Department Use for Patients Undergoing Cancer-Directed Surgeries. Current Oncology, 29(3), 1877-1889. https://doi.org/10.3390/curroncol29030153