Laparoscopic vs. Open Gastrectomy for Locally Advanced Gastric Cancer: A Propensity Score-Matched Retrospective Case-Control Study

 ,
, 
Abstract
:1. Introduction
2. Methods
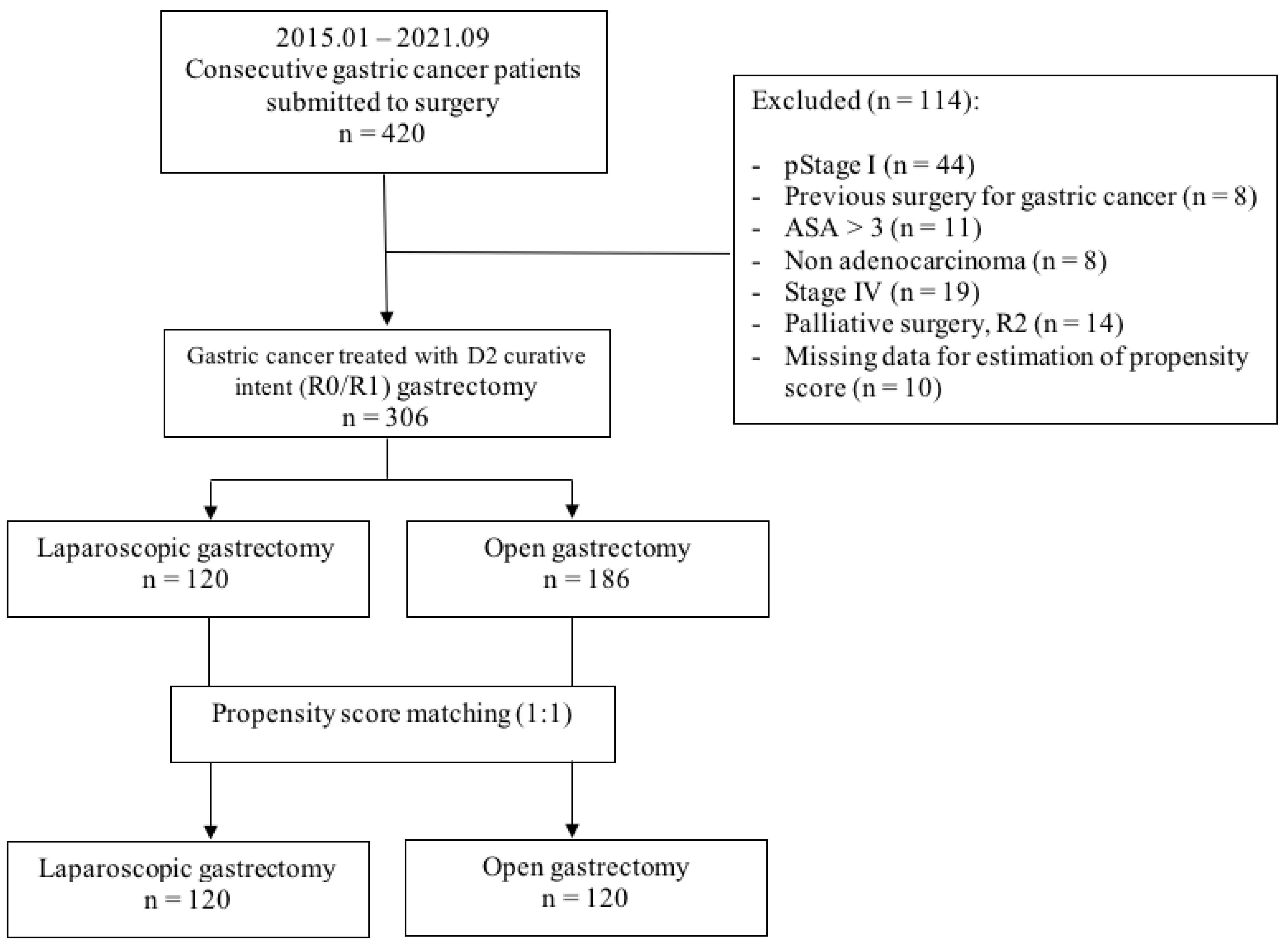
2.1. Study Design
2.2. Patient Population
2.3. Enrollment Process and Definition of Comparative Groups
2.4. Outcome Measures
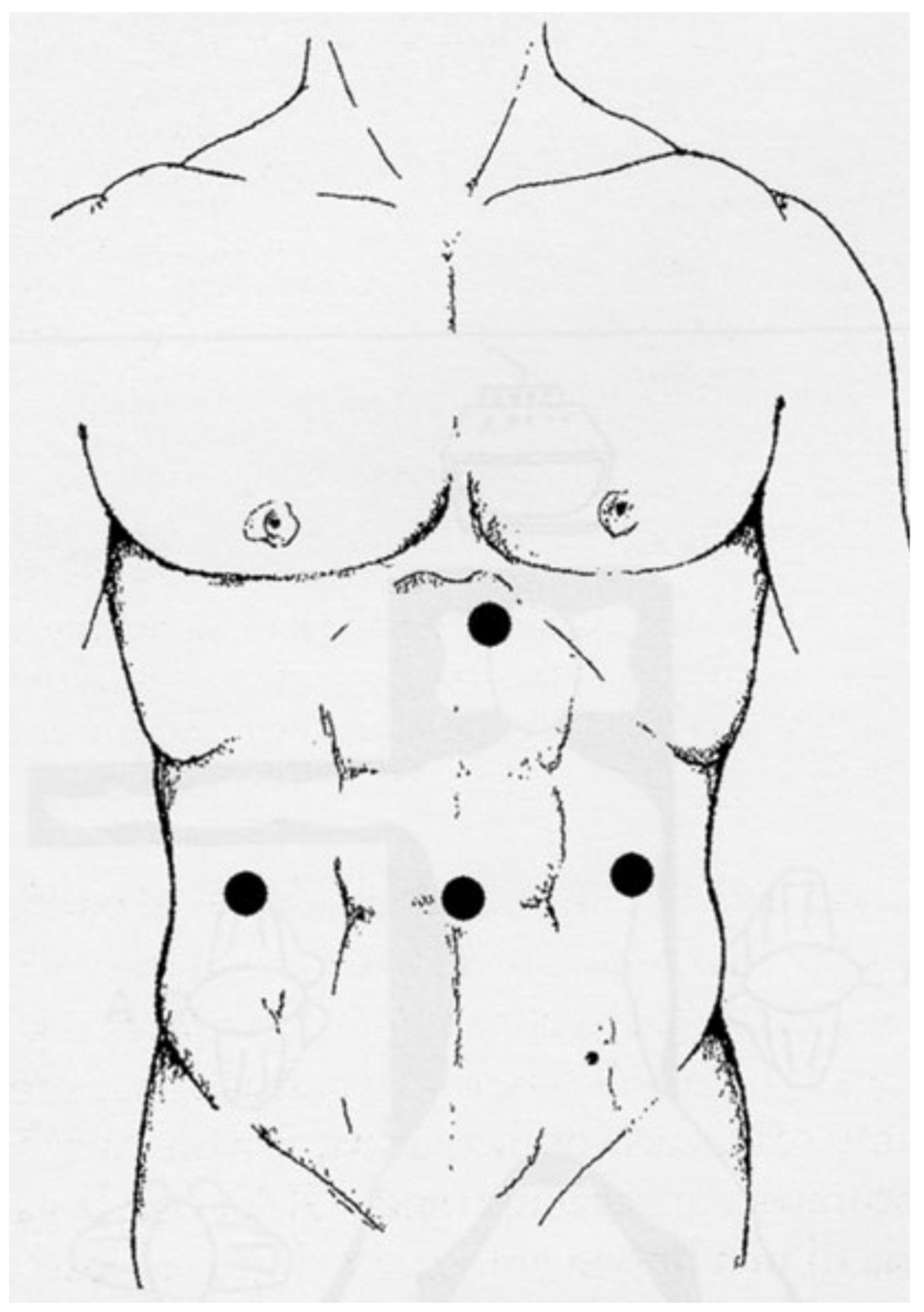
2.5. Surgical Procedure
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Surgical Outcome
3.2. Pathologic Characteristics
3.3. Post-Operative Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Songun, I.; Putter, H.; Kranenbarg, E.M.-K.; Sasako, M.; van de Velde, C.J. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 2010, 11, 439–449. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okines, A.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21 (Suppl. 5), v50–v54. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.W.; Baik, Y.H.; Yun, Y.H.; Nam, B.H.; Kim, D.H.; Choi, I.J.; Bae, J.M. Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: Results of a prospective randomized clinical trial. Ann. Surg. 2008, 248, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Kitano, S.; Shiraishi, N.; Fujii, K.; Yasuda, K.; Inomata, M.; Adachi, Y. A randomized controlled trial comparing open vs laparoscopy-assisted distal gastrectomy for the treatment of early gastric cancer: An interim report. Surgery 2002, 131, S306–S311. [Google Scholar] [CrossRef]
- Fujii, K.; Sonoda, K.; Izumi, K.; Shiraishi, N.; Adachi, Y.; Kitano, S. T lymphocyte subsets and Th1/Th2 balance after laparoscopy-assisted distal gastrectomy. Surg. Endosc. 2003, 17, 1440–1444. [Google Scholar] [CrossRef]
- Hayashi, H.; Ochiai, T.; Shimada, H.; Gunji, Y. Prospective randomized study of open versus laparoscopy-assisted distal gastrectomy with extraperigastric lymph node dissection for early gastric cancer. Surg. Endosc. 2005, 19, 1172–1176. [Google Scholar] [CrossRef]
- Lee, J.-H.; Han, H.-S. A prospective randomized study comparing open vs laparoscopy-assisted distal gastrectomy in early gastric cancer: Early results. Surg. Endosc. 2004, 19, 168–173. [Google Scholar] [CrossRef]
- Sakuramoto, S.; Yamashita, K.; Kikuchi, S.; Futawatari, N.; Katada, N.; Watanabe, M.; Okutomi, T.; Wang, G.; Bax, L. Laparoscopy versus open distal gastrectomy by expert surgeons for early gastric cancer in Japanese patients: Short-term clinical outcomes of a randomized clinical trial. Surg. Endosc. 2012, 27, 1695–1705. [Google Scholar] [CrossRef]
- Takiguchi, S.; Fujiwara, Y.; Yamasaki, M.; Miyata, H.; Nakajima, K.; Sekimoto, M.; Mori, M.; Doki, Y. Laparoscopy-Assisted Distal Gastrectomy Versus Open Distal Gastrectomy. A Prospective Randomized Single-Blind Study. World J. Surg. 2013, 37, 2379–2386. [Google Scholar] [CrossRef]
- Yamashita, K.; Sakuramoto, S.; Kikuchi, S.; Futawatari, N.; Katada, N.; Hosoda, K.; Moriya, H.; Mieno, H.; Watanabe, M. Laparoscopic versus open distal gastrectomy for early gastric cancer in Japan: Long-term clinical outcomes of a randomized clinical trial. Surg. Today 2015, 46, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Kim, H.H.; Han, S.U.; Kim, M.C.; Hyung, W.J.; Ryu, S.W.; Cho, G.S.; Kim, C.Y.; Yang, H.-K.; Park, D.J.; et al. Decreased morbidity of laparoscopic distal gastrectomy compared with open distal gastrectomy for stage I gastric cancer: Short-term outcomes from a multicenter randomized controlled trial (KLASS-01). Ann. Surg. 2016, 263, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Katai, H.; Mizusawa, J.; Katayama, H.; Takagi, M.; Yoshikawa, T.; Fukagawa, T.; Terashima, M.; Misawa, K.; Teshima, S.; Koeda, K.; et al. Short-term surgical outcomes from a phase III study of laparoscopy-assisted versus open distal gastrectomy with nodal dissection for clinical stage IA/IB gastric cancer: Japan Clinical Oncology Group Study JCOG0912. Gastric Cancer 2017, 20, 699–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitano, S.; Shiraishi, N.; Uyama, I.; Sugihara, K.; Tanigawa, N. A Multicenter Study on Oncologic Outcome of Laparoscopic Gastrectomy for Early Cancer in Japan. Ann. Surg. 2007, 245, 68–72. [Google Scholar] [CrossRef]
- Kim, H.H.; Hyung, W.J.; Cho, G.S.; Kim, M.C.; Han, S.U.; Kim, W.; Ryu, S.W.; Lee, H.J.; Song, K.Y. Morbidity and mortality of laparoscopic gastrectomy versus open gastrectomy for gastric cancer: An interim report—A phase III multicenter, prospective, randomized Trial (KLASS Trial). Ann. Surg. 2010, 251, 417–420. [Google Scholar] [CrossRef]
- Kim, H.H.; Han, S.U.; Kim, M.C.; Kim, W.; Lee, H.J.; Ryu, S.W.; Cho, G.S.; Kim, C.Y.; Yang, H.K.; Park, D.J.; et al. Korean Laparoendoscopic Gastrointestinal Surgery Study (KLASS) Group. Effect of Laparoscopic Distal Gastrectomy vs Open Distal Gastrectomy on Long-term Survival Among Patients With Stage I Gastric Cancer: The KLASS-01 Randomized Clinical Trial. JAMA Oncol. 2019, 5, 506–513. [Google Scholar] [CrossRef]
- Caruso, S.; Patriti, A.; Roviello, F.; De Franco, L.; Franceschini, F.; Coratti, A.; Ceccarelli, G. Laparoscopic and robot-assisted gastrectomy for gastric cancer: Current considerations. World J. Gastroenterol. 2016, 22, 5694–5717. [Google Scholar] [CrossRef]
- Kim, M.-C.; Kim, H.-H.; Jung, G.-J. Surgical outcome of laparoscopy-assisted gastrectomy with extraperigastric lymph node dissection for gastric cancer. Eur. J. Surg. Oncol. 2005, 31, 401–405. [Google Scholar] [CrossRef]
- Pugliese, R.; Maggioni, D.; Sansonna, F.; Scandroglio, I.; Ferrari, G.C.; Di Lernia, S.; Costanzi, A.; Pauna, J.; De Martini, P. Total and subtotal laparoscopic gastrectomy for adenocarcinoma. Surg. Endosc. 2006, 21, 21–27. [Google Scholar] [CrossRef]
- Tanimura, S.; Higashino, M.; Fukunaga, Y.; Takemura, M.; Tanaka, Y.; Fujiwara, Y.; Osugi, H. Laparoscopic gastrectomy for gastric cancer: Experience with more than 600 cases. Surg. Endosc. 2008, 22, 1161–1164. [Google Scholar] [CrossRef]
- Huang, J.L.; Zheng, Z.H.; Wei, B.; Chen, T.F.; Huang, Y.; Guo, W.P.; Hu, B.; Wei, H.B. Laparoscopy-Assisted D2 Radical Distal Gastrectomy for Advanced Gastric Cancer. Dig. Surg. 2010, 27, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Shimada, M.; Kurita, N.; Iwata, T.; Nishioka, M.; Morimoto, S.; Yoshikawa, K.; Miyatani, T.; Goto, M.; Kashihara, H.; et al. Comparison of long-term prognosis of laparoscopy-assisted gastrectomy and conventional open gastrectomy with special reference to D2 lymph node dissection. Surg. Endosc. 2012, 26, 2240–2246. [Google Scholar] [CrossRef] [PubMed]
- Park, D.J.; Han, S.U.; Hyung, W.J.; Kim, M.C.; Kim, W.; Ryu, S.Y.; Ryu, S.W.; Song, K.Y.; Lee, H.J.; Cho, G.S.; et al. Long-term outcomes after laparoscopy-assisted gastrectomy for advanced gastric cancer: A large-scale multicenter retrospective study. Surg. Endosc. 2012, 26, 1548–1553. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.-H.; Kang, S.H.; Lee, Y.; Min, S.-H.; Park, Y.S.; Park, D.J.; Kim, H.-H. Long-term Survival Outcomes of Laparoscopic Gastrectomy for Advanced Gastric Cancer: Five-year Results of a Phase II Prospective Clinical Trial. J. Gastric Cancer 2019, 19, 102–110. [Google Scholar] [CrossRef]
- Bo, T.; Peiwu, Y.; Feng, Q.; Yongliang, Z.; Yan, S.; Yingxue, H.; Huaxing, L. Laparoscopy-Assisted vs. Open Total Gastrectomy for Advanced Gastric Cancer: Long-Term Outcomes and Technical Aspects of a Case–Control Study. J. Gastrointest. Surg. 2013, 17, 1202–1208. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-H.; Han, S.-U.; Kim, M.-C.; Hyung, W.J.; Kim, W.; Lee, H.-J.; Ryu, S.W.; Cho, G.S.; Song, K.Y.; Ryu, S.Y. Long-Term Results of Laparoscopic Gastrectomy for Gastric Cancer: A Large-Scale Case-Control and Case-Matched Korean Multicenter Study. J. Clin. Oncol. 2014, 32, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.Z.; Wen, L.; Rui, Y.Y.; Liu, C.X.; Zhao, Q.C.; Zhou, Z.G.; Hu, J.K. Long-term survival outcomes of laparoscopic versus open gastrectomy for gastric cancer: A systematic review and meta-analysis. Medicine 2015, 94, e454. [Google Scholar] [CrossRef]
- Yu, J.; Huang, C.; Sun, Y.; Su, X.; Cao, H.; Hu, J.; Wang, K.; Suo, J.; Tao, K.; He, X.; et al. Effect of Laparoscopic vs. Open Distal Gastrectomy on 3-Year Disease-Free Survival in Patients With Locally Advanced Gastric Cancer: The CLASS-01 Randomized Clinical Trial. JAMA 2019, 321, 1983–1992. [Google Scholar] [CrossRef] [Green Version]
- Claassen, Y.H.M.; van Amelsfoort, R.M.; Hartgrink, H.H.; Dikken, J.L.; de Steur, W.O.; van Sandick, J.W.; van Grieken, N.C.T.; Cats, A.; Boot, H.; Trip, A.K.; et al. Effect of Hospital Volume With Respect to Performing Gastric Cancer Resection on Recurrence and Survival: Results From the CRITICS Trial. Ann. Surg. 2019, 270, 1096–1102. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Brierley, J.D. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van De Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative Chemotherapy versus Surgery Alone for Resectable Gastroesophageal Cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scatizzi, M.; Kröning, K.C.; Lenzi, E.; Moraldi, L.; Cantafio, S.; Feroci, F. Laparoscopic versus open distal gastrectomy for locally advanced gastric cancer: A case–control study. Updat. Surg. 2011, 63, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.R.; Rubin, D.B. Constructing a control group using multivariate matched sampling methods that incorporate the propensity score. Am. Stat. 1985, 39, 33–38. [Google Scholar]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Rubin, D.B.T.; Thomas, N. Combining propensity score matching with additional adjustments for prognostic covariates. J. Am. Stat. Assoc. 2000, 95, 573–585. [Google Scholar] [CrossRef]
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. Matching as Nonparametric Preprocessing for Reducing Model Dependence in Parametric Causal Inference. Political Anal. 2007, 15, 199–236. [Google Scholar] [CrossRef] [Green Version]
- Lonjon, G.; Porcher, R.; Ergina, P.; Fouet, M.; Boutron, I. Potential pitfalls of reporting and bias in observational studies with propensity score analysis assessing a surgical procedure: A methodological systematic review. Ann. Surg. 2017, 265, 901–909. [Google Scholar] [CrossRef]
- Yakoub, D.; Athanasiou, T.; Tekkis, P.; Hanna, G.B. Laparoscopic assisted distal gastrectomy for early gastric cancer: Is it an alternative to the open approach? Surg. Oncol. 2009, 18, 322–333. [Google Scholar] [CrossRef]
- Zeng, Y.K.; Yang, Z.L.; Peng, J.S.; Lin, H.S.; Cai, L. Laparoscopy-assisted versus open distal gastrectomy for early gastric cancer: Evidence from randomized and nonrandomized clinical trials. Ann. Surg. 2012, 256, 39–52. [Google Scholar] [CrossRef]
- Ohtani, H.; Tamamori, Y.; Noguchi, K.; Azuma, T.; Fujimoto, S.; Oba, H.; Aoki, T.; Minami, M.; Hirakawa, K. A Meta-Analysis of Randomized Controlled Trials that Compared Laparoscopy-Assisted and Open Distal Gastrectomy for Early Gastric Cancer. J. Gastrointest. Surg. 2010, 14, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Huscher, C.G.; Mingoli, A.; Sgarzini, G.; Sansonetti, A.; Di Paola, M.; Recher, A.; Ponzano, C. Laparoscopic versus open subtotal gastrectomy for distal gastric cancer: Five-year results of a randomized prospective trial. Ann. Surg. 2005, 241, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Uyama, I.; Sugioka, A.; Fujita, J.; Hasumi, A.; Komori, Y.; Matsui, H. Laparoscopic total gastrectomy with distal pancreatosplenectomy and D2 lymphadenectomy for advanced gastric cancer. Gastric Cancer 1999, 2, 230–234. [Google Scholar] [CrossRef]
- Lin, J.-X.; Huang, C.-M.; Zheng, C.-H.; Li, P.; Xie, J.-W.; Wang, J.-B.; Jun, L.; Chen, Q.-Y.; Lin, M.; Tu, R. Evaluation of laparoscopic total gastrectomy for advanced gastric cancer: Results of a comparison with laparoscopic distal gastrectomy. Surg. Endosc. 2015, 30, 1988–1998. [Google Scholar] [CrossRef]
- Noshiro, H.; Nagai, E.; Shimizu, S.; Uchiyama, A.; Tanaka, M. Laparoscopically assisted distal gastrectomy with standard radical lymph node dissection for gastric cancer. Surg. Endosc. 2005, 19, 1592–1596. [Google Scholar] [CrossRef] [PubMed]
- Song, K.Y.; Kim, S.N.; Park, C.H. Laparoscopy-assisted distal gastrectomy with D2 lymph node dissection for gastric cancer: Technical and oncologic aspects. Surg. Endosc. 2007, 22, 655–659. [Google Scholar] [CrossRef]
- Ziqiang, W.; Feng, Q.; Zhimin, C.; Miao, W.; Lian, Q.; Huaxing, L.; Peiwu, Y. Comparison of laparoscopically assisted and open radical distal gastrectomy with extended lymphadenectomy for gastric cancer management. Surg. Endosc. 2006, 20, 1738–1743. [Google Scholar] [CrossRef]
- Hur, H.; Jeon, H.M.; Kim, W. Laparoscopic pancreas- and spleen-preserving D2 lymph node dissection in advanced (cT2) upper-third gastric cancer. J. Surg. Oncol. 2008, 97, 169–172. [Google Scholar] [CrossRef]
- Shinohara, T.; Kanaya, S.; Taniguchi, K.; Fujita, T.; Yanaga, K.; Uyama, I. Laparoscopic Total Gastrectomy With D2 Lymph Node Dissection for Gastric Cancer. Arch. Surg. 2009, 144, 1138–1142. [Google Scholar] [CrossRef] [Green Version]
- Haverkamp, L.; Ruurda, J.; Offerhaus, G.; Weijs, T.; van der Sluis, P.; van Hillegersberg, R. Laparoscopic gastrectomy in Western European patients with advanced gastric cancer. Eur. J. Surg. Oncol. 2015, 42, 110–115. [Google Scholar] [CrossRef]
- Lee, S.-W.; Nomura, E.; Bouras, G.; Tokuhara, T.; Tsunemi, S.; Tanigawa, N. Long-Term Oncologic Outcomes from Laparoscopic Gastrectomy for Gastric Cancer: A Single-Center Experience of 601 Consecutive Resections. J. Am. Coll. Surg. 2010, 211, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.I.; Kim, H.O.; Yoo, C.H.; Shin, J.H.; Son, B.H. Laparoscopic-assisted distal gastrectomy versus open distal gastrectomy for advanced gastric cancer. Surg. Endosc. 2008, 23, 1252–1258. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-T.; Han, X.-P.; Su, L.; Zhu, W.-K.; Xu, W.; Li, K.; Zhao, Q.-C.; Yang, H.; Liu, H.-B. Short-term efficacy of laparoscopy-assisted vs open radical gastrectomy in gastric cancer. World J. Gastrointest. Surg. 2014, 6, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.; Ying, M.; Huang, C.; Wei, H.; Jiang, Z.; Peng, X.; Hu, J.; Du, X.; Wang, B.; Lin, F.; et al. Oncologic outcomes of laparoscopy-assisted gastrectomy for advanced gastric cancer: A large-scale multicenter retrospective cohort study from China. Surg. Endosc. 2014, 28, 2048–2056. [Google Scholar] [CrossRef]
- Park, Y.K.; Yoon, H.M.; Kim, Y.-W.; Park, J.Y.; Ryu, K.W.; Lee, Y.-J.; Jeong, O.; Yoon, K.Y.; Lee, J.H.; Lee, S.E.; et al. Laparoscopy-assisted versus Open D2 Distal Gastrectomy for Advanced Gastric Cancer. Ann. Surg. 2018, 267, 638–645. [Google Scholar] [CrossRef]
- Cai, J.; Wei, D.; Gao, C.; Zhang, C.; Zhang, H.; Zhao, T. A Prospective Randomized Study Comparing Open versus Laparoscopy-Assisted D2 Radical Gastrectomy in Advanced Gastric Cancer. Dig. Surg. 2011, 28, 331–337. [Google Scholar] [CrossRef]
- Hu, Y.; Huang, C.; Sun, Y.; Su, X.; Cao, H.; Hu, J.; Xue, Y.; Suo, J.; Tao, K.; He, X.; et al. Morbidity and Mortality of Laparoscopic Versus Open D2 Distal Gastrectomy for Advanced Gastric Cancer: A Randomized Controlled Trial. J. Clin. Oncol. 2016, 34, 1350–1357. [Google Scholar] [CrossRef]
- Shi, Y.; Yingxue, H.; Zhao, Y.; Qian, F.; Tang, B.; Hao, Y.; Luo, H.; Chen, J.; Yu, P. Short-term surgical outcomes of a randomized controlled trial comparing laparoscopic versus open gastrectomy with D2 lymph node dissection for advanced gastric cancer. Surg. Endosc. 2017, 32, 2427–2433. [Google Scholar] [CrossRef]
- Wang, Z.; Xing, J.; Cai, J.; Zhang, Z.; Li, F.; Zhang, N.; Wu, J.; Cui, M.; Liu, Y.; Chen, L.; et al. Short-term surgical outcomes of laparoscopy-assisted versus open D2 distal gastrectomy for locally advanced gastric cancer in North China: A multicenter randomized controlled trial. Surg. Endosc. 2019, 33, 33–45. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-J.; Hyung, W.J.; Yang, H.-K.; Han, S.U.; Park, Y.-K.; An, J.Y.; Kim, W.; Kim, H.-I.; Kim, H.-H.; Ryu, S.W.; et al. Short-term Outcomes of a Multicenter Randomized Controlled Trial Comparing Laparoscopic Distal Gastrectomy with D2 Lymphadenectomy to Open Distal Gastrectomy for Locally Advanced Gastric Cancer (KLASS-02-RCT). Ann. Surg. 2019, 270, 983–991. [Google Scholar] [CrossRef]
- Martínez-Ramos, D.; Miralles-Tena, J.M.; Cuesta, M.A.; Escrig-Sos, J.; van der Peet, D.; Hoashi, J.S.; Salvador-Sanchis, J.L. Laparoscopy versus open surgery for advanced and resectable gastric cancer: A meta-analysis. Rev. Esp. Enferm. Dig. 2011, 103, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, J.; Pankaj, P.; Jiang, H.; Zeng, Y.; Wu, H. Laparoscopy versus open distal gastrectomy for advanced gastric cancer: A systematic review and meta-analysis. Surg. Laparosc. Endosc. Percutan Tech. 2013, 23, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Xu, X.-W.; Mou, Y.-P.; Pan, Y.; Zhou, Y.-C.; Zhang, R.-C.; Wu, D. Systematic review and meta-analysis of laparoscopic and open gastrectomy for advanced gastric cancer. World J. Surg. Oncol. 2013, 11, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, Z.H.; Zhao, L.Y.; Mou, T.Y.; Hu, Y.F.; Yu, J.; Liu, H.; Chen, H.; Wu, J.M.; An, S.L.; Li, G.X. Laparoscopic vs. open D2 gastrectomy for locally advanced gastric cancer: A meta-analysis. World J. Gastroenterol. 2014, 20, 16750–16764. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-L.; Lin, H.-G.; Yang, J.-W.; Jiang, F.-Q.; Zhang, T.; Yang, H.-M.; Li, C.-L.; Cui, Y. Laparoscopy-assisted versus open gastrectomy with D2 lymph node dissection for advanced gastric cancer: A meta-analysis. Int. J. Clin. Exp. Med. 2014, 7, 1490–1499. [Google Scholar] [PubMed]
- Zhou, D.; Quan, Z.; Wang, J.; Zhao, M.; Yang, Y. Laparoscopic-Assisted Versus Open Distal Gastrectomy with D2 Lymph Node Resection for Advanced Gastric Cancer: Effect of Learning Curve on Short-Term Outcomes. A Meta-analysis. J. Laparoendosc. Adv. Surg. Tech. 2014, 24, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Zhou, S.; Peng, Z.; Chen, L. Quality of D2 lymphadenectomy for advanced gastric cancer: Is laparoscopic-assisted distal gastrectomy as effective as open distal gastrectomy? Surg. Endosc. 2014, 29, 1537–1544. [Google Scholar] [CrossRef]
- Quan, Y.; Huang, A.; Ye, M.; Xu, M.; Zhuang, B.; Zhang, P.; Yu, B.; Min, Z. Comparison of laparoscopic versus open gastrectomy for advanced gastric cancer: An updated meta-analysis. Gastric Cancer 2015, 19, 939–950. [Google Scholar] [CrossRef]
- Wei, Y.; Yu, D.; Li, Y.; Fan, C.; Li, G. Laparoscopic versus open gastrectomy for advanced gastric cancer: A meta-analysis based on high-quality retrospective studies and clinical randomized trials. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 577–590. [Google Scholar] [CrossRef]
- Beyer, K.; Baukloh, A.-K.; Kamphues, C.; Seeliger, H.; Heidecke, C.-D.; Kreis, M.E.; Patrzyk, M. Laparoscopic versus open gastrectomy for locally advanced gastric cancer: A systematic review and meta-analysis of randomized controlled studies. World J. Surg. Oncol. 2019, 17, 68. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Feng, X.; Wang, M.; Yao, X. Laparoscopic versus open distal gastrectomy for advanced gastric cancer: A meta-analysis of randomized controlled trials and high-quality nonrandomized comparative studies. Eur. J. Surg. Oncol. 2020, 46, 1998–2010. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Li, L.; Xu, J.; Ye, W.; Zeng, J.; Chen, B.; Huang, Z. Laparoscopic versus open approach in gastrectomy for advanced gastric cancer: A systematic review. World J. Surg. Oncol. 2020, 18, 126. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.Y.; Bae, J.M.; An, J.Y.; Hyung, W.J.; Noh, S.H. Laparoscopic gastrectomy for advanced gastric cancer: Are the long-term results comparable with conventional open gastrectomy? A systematic review and meta-analysis. J. Surg. Oncol. 2013, 108, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhao, Y.; Lian, B.; Liu, Y.; Zhao, Q. Long-term oncological outcomes in laparoscopic versus open gastrectomy for advanced gastric cancer: A meta-analysis of high-quality nonrandomized studies. Am. J. Surg. 2019, 218, 631–638. [Google Scholar] [CrossRef]
- Best, L.M.J.; Mughal, M.; Gurusamy, K.S. Laparoscopic versus open gastrectomy for gastric cancer. Cochrane Database Syst. Rev. 2016, 2016, CD011389. [Google Scholar] [CrossRef] [Green Version]
- Hur, H.; Lee, H.Y.; Lee, H.-J.; Kim, M.C.; Hyung, W.J.; Park, Y.K.; Kim, W.; Han, S.-U. Efficacy of laparoscopic subtotal gastrectomy with D2 lymphadenectomy for locally advanced gastric cancer: The protocol of the KLASS-02 multicenter randomized controlled clinical trial. BMC Cancer 2015, 15, 355. [Google Scholar] [CrossRef] [Green Version]
- Hyung, W.J.; Yang, H.-K.; Park, Y.-K.; Lee, H.-J.; An, J.Y.; Kim, W.; Kim, H.-I.; Kim, H.-H.; Ryu, S.W.; Hur, H.; et al. Long-Term Outcomes of Laparoscopic Distal Gastrectomy for Locally Advanced Gastric Cancer: The KLASS-02-RCT Randomized Clinical Trial. J. Clin. Oncol. 2020, 38, 3304–3313. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines (2014) (ver. 4). Gastric Cancer 2017, 20, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.-F.; Jeong, O.; Jung, M.R.; Ryu, S.Y.; Park, Y.K. A propensity score–matched case–control comparative study of laparoscopic and open extended (D2) lymph node dissection for distal gastric carcinoma. Surg. Endosc. 2013, 27, 2792–2800. [Google Scholar] [CrossRef]
- Kim, K.-H.; Kim, M.-C.; Jung, G.-J.; Choi, H.-J.; Jang, J.-S.; Kwon, H.-C. Comparative Analysis of Five-Year Survival Results of Laparoscopy-Assisted Gastrectomy versus Open Gastrectomy for Advanced Gastric Cancer: A Case-Control Study Using a Propensity Score Method. Dig. Surg. 2012, 29, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Inokuchi, M.; Nakagawa, M.; Tanioka, T.; Okuno, K.; Gokita, K.; Kojima, K. Long- and short-term outcomes of laparoscopic gastrectomy versus open gastrectomy in patients with clinically and pathological locally advanced gastric cancer: A propensity-score matching analysis. Surg. Endosc. 2017, 32, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, S.; Kunisaki, C.; Ono, H.; Oshima, T.; Fujii, S.; Taguri, M.; Morita, S.; Sato, T.; Yamada, R.; Yukawa, N.; et al. Omentum-preserving gastrectomy for advanced gastric cancer: A propensity-matched retrospective cohort study. Gastric Cancer 2012, 16, 383–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Liu, Y.; Hao, Y.; Bai, B.; Yu, D.; Zhao, Q. Surgical and long-term oncologic outcomes of laparoscopic and open gastrectomy for serosa-positive (pT4a) gastric cancer: A propensity score-matched analysis. Surg. Oncol. 2019, 28, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Strong, V.E.; Song, K.Y.; Park, C.H.; Jacks, L.M.; Gonen, M.; Shah, M.; Coit, D.G.; Brennan, M. Comparison of Gastric Cancer Survival Following R0 Resection in the United States and Korea Using an Internationally Validated Nomogram. Ann. Surg. 2010, 251, 640–646. [Google Scholar] [CrossRef]
- Russo, A.; Li, P.; Strong, V.E. Differences in the multimodal treatment of gastric cancer: East versus west. J. Surg. Oncol. 2017, 115, 603–614. [Google Scholar] [CrossRef]
- Caruso, S.; Scatizzi, M. Laparoscopic gastrectomy for gastric cancer: Has the time come for considered it a standard procedure? Surg. Oncol. 2022, 40, 101699. [Google Scholar] [CrossRef]
- Dicken, B.J.; Bigam, D.L.; Cass, C.; Mackey, J.R.; Joy, A.A.; Hamilton, S.M. Gastric adenocarcinoma: Review and considerations for future directions. Ann. Surg. 2005, 241, 27–39. [Google Scholar] [CrossRef]
- Sano, T.; Sasako, M.; Yamamoto, S.; Nashimoto, A.; Kurita, A.; Hiratsuka, M.; Tsujinaka, T.; Kinoshita, T.; Arai, K.; Yamamura, Y.; et al. Gastric Cancer Surgery: Morbidity and Mortality Results From a Prospective Randomized Controlled Trial Comparing D2 and Extended Para-Aortic Lymphadenectomy—Japan Clinical Oncology Group Study 9501. J. Clin. Oncol. 2004, 22, 2767–2773. [Google Scholar] [CrossRef]
- Degiuli, M.; Sasako, M.; Ponti, A. Morbidity and mortality in the Italian Gastric Cancer Study Group randomized clinical trial of D1 versus D2 resection for gastric cancer. Br. J. Surg. 2010, 97, 643–649. [Google Scholar] [CrossRef]
- Roukos, D.H.; Lorenz, M.; Encke, A. Evidence of survival benefit of extended (D2) lymphadenectomy in Western patients with gastric cancer based on a new concept: A prospective long-term follow-up study. Surgery 1998, 123, 573–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.W.; Hsieh, M.C.; Lo, S.S.; Wang, L.S.; Hsu, W.H.; Lui, W.Y.; Huang, M.H.; P’Eng, F.K. Morbidity and mortality after radical gastrectomy for patients with carcinoma of the stomach. J. Am. Coll. Surg. 1995, 181, 26–32. [Google Scholar] [PubMed]
- Hyun, M.; Lee, C.; Kim, H.; Tong, Y.; Park, S. Systematic review and meta-analysis of robotic surgery compared with conventional laparoscopic and open resections for gastric carcinoma. Br. J. Surg. 2013, 100, 1566–1578. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Wang, J.; Zhang, G.; Wang, J.; Yang, B.; Zhang, Z. Feasibility and safety comparison of laparoscopy-assisted versus open gastrectomy for advanced gastric carcinoma with D2 lymphadenectomy. Jpn. J. Clin. Oncol. 2016, 46, 323–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunisaki, C.; Makino, H.; Kosaka, T.; Oshima, T.; Fujii, S.; Takagawa, R.; Kimura, J.; Ono, H.A.; Akiyama, H.; Taguri, M.; et al. Surgical outcomes of laparoscopy-assisted gastrectomy versus open gastrectomy for gastric cancer: A case-control study. Surg. Endosc. 2011, 26, 804–810. [Google Scholar] [CrossRef]
- Lu, Y.; Jiang, B.; Liu, T. Laparoscopic versus open total gastrectomy for advanced proximal gastric carcinoma: A matched pair analysis. J. BUON 2016, 21, 903–908. [Google Scholar]
- Chen, K.; Xu, X.W.; Zhang, R.C.; Pan, Y.; Wu, D.; Mou, Y.P. Systematic review and meta-analysis of laparoscopy-assisted and open total gastrectomy for gastric cancer. World J. Gastroenterol. 2013, 19, 5365–5376. [Google Scholar] [CrossRef]
- Park, S.H.; Suh, Y.S.; Kim, T.H.; Choi, Y.H.; Choi, J.H.; Kong, S.H.; Park, D.J.; Lee, H.J.; Yang, H.K. Postoperative morbidity and quality of life between totally laparoscopic total gastrectomy and laparoscopy-assisted total gastrectomy: A propensity-score matched analysis. BMC Cancer 2021, 21, 1016. [Google Scholar] [CrossRef]
- Fang, C.; Hua, J.; Li, J.; Zhen, J.; Wang, F.; Zhao, Q.; Shuang, J.; Du, J. Comparison of long-term results between laparoscopy-assisted gastrectomy and open gastrectomy with D2 lymphadenectomy for advanced gastric cancer. Am. J. Surg. 2014, 208, 391–396. [Google Scholar] [CrossRef]
- Li, Z.; Shan, F.; Ying, X.; Zhang, Y.; Jian-Yu, E.; Wang, Y.; Ren, H.; Su, X.; Ji, J. Assessment of Laparoscopic Distal Gastrectomy After Neoadjuvant Chemotherapy for Locally Advanced Gastric Cancer: A Randomized Clinical Trial. JAMA Surg. 2019, 154, 1093–1101. [Google Scholar] [CrossRef] [Green Version]
- Inaki, N.; Etoh, T.; Ohyama, T.; Uchiyama, K.; Katada, N.; Koeda, K.; Yoshida, K.; Takagane, A.; Kojima, K.; Sakuramoto, S.; et al. A Multi-institutional, Prospective, Phase II Feasibility Study of Laparoscopy-Assisted Distal Gastrectomy with D2 Lymph Node Dissection for Locally Advanced Gastric Cancer (JLSSG0901). World J. Surg. 2015, 39, 2734–2741. [Google Scholar] [CrossRef] [PubMed]
- Huscher, C.G.; Mingoli, A.; Sgarzini, G.; Sansonetti, A.; Lirici, M.M.; Napolitano, C.; Piro, F. Videolaparoscopic total and subtotal gastrectomy with extended lymph node dissection for gastric cancer. Am. J. Surg. 2004, 188, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Moisan, F.; Norero, E.; Slako, M.; Varas, J.; Palominos, G.; Crovari, F.; Ibanez, L.; Perez, G.; Pimentel, F.; Guzmán, S.; et al. Completely laparoscopic versus open gastrectomy for early and advanced gastric cancer: A matched cohort study. Surg. Endosc. 2011, 26, 661–672. [Google Scholar] [CrossRef] [PubMed]
- Orsenigo, E.; Di Palo, S.; Tamburini, A.; Staudacher, C. Laparoscopy-assisted gastrectomy versus open gastrectomy for gastric cancer: A monoinstitutional Western center experience. Surg. Endosc. 2011, 25, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Parisi, A.; Reim, D.; Borghi, F.; Nguyen, N.T.; Qi, F.; Coratti, A.; Cianchi, F.; Cesari, M.; Bazzocchi, F.; Alimoglu, O.; et al. Minimally invasive surgery for gastric cancer: A comparison between robotic, laparoscopic and open surgery. World J. Gastroenterol. 2017, 23, 2376–2384. [Google Scholar] [CrossRef]
- van der Veen, A.; Brenkman, H.J.F.; Seesing, M.F.J.; Haverkamp, L.; Luyer, M.D.P.; Nieuwenhuijzen, G.A.P.; Stoot, J.H.M.B.; Tegels, J.J.W.; Wijnhoven, B.P.L.; Lagarde, S.M.; et al. Laparoscopic Versus Open Gastrectomy for Gastric Cancer (LOGICA): A Multicenter Randomized Clinical Trial. J. Clin. Oncol. 2021, 39, 978–989. [Google Scholar] [CrossRef]
- van der Wielen, N.; Straatman, J.; Daams, F.; Rosati, R.; Parise, P.; Weitz, J.; Reissfelder, C.; Diez Del Val, I.; Loureiro, C.; Parada-González, P.; et al. Open versus minimally invasive total gastrectomy after neoadjuvant chemotherapy: Results of a European randomized trial. Gastric Cancer 2021, 24, 258–271. [Google Scholar] [CrossRef]
- Griffin, S.M. Gastric cancer in the East: Same disease, different patient. Br. J. Surg. 2005, 92, 1055–1056. [Google Scholar] [CrossRef]
- Jeong, O.; Ryu, S.Y.; Choi, W.Y.; Piao, Z.; Park, Y.K. Risk Factors and Learning Curve Associated with Postoperative Morbidity of Laparoscopic Total Gastrectomy for Gastric Carcinoma. Ann. Surg. Oncol. 2014, 21, 2994–3001. [Google Scholar] [CrossRef]
- Amato, L.; Fusco, D.; Acampora, A.; Bontempi, K.; Rosa, A.C.; Colais, P.; Cruciani, F.; D’Ovidio, M.; Mataloni, F.; Minozzi, S.; et al. Volume and health outcomes: Evidence from systematic reviews and from evaluation of Italian hospital data. Epidemiol. Prev. 2017, 41 (Suppl. 2), 1–128. [Google Scholar]
- Ding, J.; Liao, G.-Q.; Liu, H.-L.; Liu, S.; Tang, J. Meta-analysis of laparoscopy-assisted distal gastrectomy with D2 lymph node dissection for gastric cancer. J. Surg. Oncol. 2012, 105, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Miura, S.; Kodera, Y.; Fujiwara, M.; Ito, S.; Mochizuki, Y.; Yamamura, Y.; Hibi, K.; Ito, K.; Akiyama, S.; Nakao, A. Laparoscopy-assisted distal gastrectomy with systemic lymph node dissection: A critical reappraisal from the viewpoint of lymph node retrieval. J. Am. Coll. Surg. 2004, 198, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Hamabe, A.; Omori, T.; Tanaka, K.; Nishida, T. Comparison of long-term results between laparoscopy-assisted gastrectomy and open gastrectomy with D2 lymph node dissection for advanced gastric cancer. Surg. Endosc. 2011, 26, 1702–1709. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Zhang, Y.; Guo, T.K. Laparoscopy-assisted versus open distal gastrectomy for early gastric cancer: A meta-analysis based on seven randomized controlled trials. Surg. Oncol. 2015, 24, 71–77. [Google Scholar] [CrossRef]
- Hosono, S.; Arimoto, Y.; Ohtani, H.; Kanamiya, Y. Meta-analysis of short-term outcomes after laparoscopy-assisted distal gastrectomy. World J. Gastroenterol. 2006, 12, 7676–7683. [Google Scholar] [CrossRef]
- Viñuela, E.F.; Gonen, M.; Brennan, M.F.; Coit, D.G.; Strong, V.E. Laparoscopic versus open distal gastrectomy for gastric cancer: A meta-analysis of randomized controlled trials and high-quality nonrandomized studies. Ann. Surg. 2012, 255, 446–456. [Google Scholar] [CrossRef]
- Kodera, Y.; Fujiwara, M.; Ohashi, N.; Nakayama, G.; Koike, M.; Morita, S.; Nakao, A. Laparoscopic Surgery for Gastric Cancer: A Collective Review with Meta-Analysis of Randomized Trials. J. Am. Coll. Surg. 2010, 211, 677–686. [Google Scholar] [CrossRef]
- Chevallay, M.; Jung, M.K.; Berlth, F.; Seung-Hun, C.; Morel, P.; Mönig, S. Laparoscopic Surgery for Gastric Cancer: The European Point of View. J. Oncol. 2019, 2019, 8738502. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | LG (n = 120) | OG (n = 120) | p Value |
|---|---|---|---|
| Age, Mean ± SD (range, year) | 70.5 ± 11.4 (40–90) | 70.9 ± 8.5 (44–89) | 1.000 |
| Sex, n (%) | 1.000 | ||
| Male | 77 (64.1%) | 75 (62.5%) | |
| Female | 43 (35.9%) | 45 (37.5%) | |
| BMI, mean ± SD (range, kg/m2) | 20.7 ± 1.2 | 21.0 ± 1.5 | 0.560 |
| (17.5–35.4) | (18.1–36.1) | ||
| Previous abdominal surgery, n (%) | 13 (10.8%) | 15 (12.5%) | 0.481 |
| Co-morbility, n pts (%) | 41 (34.1%) | 42 (35.0%) | 1.000 |
| Cardiovascular | 3 | 4 | |
| Hypertension | 20 | 17 | |
| Diabetes | 5 | 10 | |
| Pulmonary | 4 | 2 | |
| Hepatic | 2 | 2 | |
| Renal | 4 | 2 | |
| Other | 3 | 5 | |
| ASA score, n (%) | 1.000 | ||
| 1 | 18 (15.0%) | 18 (15.0%) | |
| 2 | 46 (38.3%) | 48 (40.0%) | |
| 3 | 56 (46.7%) | 54 (45.0%) | |
| Tumour location | 1.000 | ||
| upper | 17 (14.2%) | 19 (15.8%) | |
| mid | 46 (38.3%) | 48 (40.0%) | |
| lower | 57 (47.5%) | 53 (44.2%) | |
| Neoadjuvant Chemotherapy (%) | 0.650 | ||
| Yes | 5 (4.2%) | 6 (5.0%) | |
| No | 115 (95.8%) | 114 (95.5%) |
| Characteristics | LG (n = 120) | OG (n = 120) | p Value |
|---|---|---|---|
| Type of gastrectomy | 0.121 | ||
| Total gastrectomy | 34 (28.3%) | 42 (35.0%) | |
| Subtotal distal gastrectomy | 86 (71.7%) | 78 (65.0%) | |
| Type of reconstruction | 0.140 | ||
| Billroth 2, gastrojejunostomy | 21 (17.5%) | 29 (24.2%) | |
| Roux-en-Y (either gastric or esophagel) | 99 (82.5%) | 91 (75.8%) | |
| Combined resection | 4 (3.3%) | 6 (5.0%) | 0.093 |
| Gallbladder | 6 | 4 | |
| Spleen | 0 | 2 | |
| Distal pancreas | 0 | 1 | |
| Transverse colon | 1 | 2 | |
| Operative time (min.), Mean ± SD (Range) | |||
| Overall | 212.3 ± 46.6 (120–400) | 192.4 ± 42.6 (120–320) | 0.012 |
| Subtotal gastrectomy | 180.9 ± 43.6 (120–360) | 180.2 ± 39.9 (180–290) | 0.560 |
| Total gastrectomy | 235.4 ± 45.7 (160–400) | 213.7 ± 38.8 (140–320) | <0.001 |
| Radicality, n (%) | 0.432 | ||
| R0 | 117 (97.5) | 115 (95.8) | |
| R1 | 3 (2.5) | 5 (4.2) | |
| Conversion to open, n (%) | 3 (2.5) | - | |
| Lauren classification (%) | 0.347 | ||
| Intestinal | 55 (45.8) | 59 (49.2) | |
| Diffuse | 46 (38.3) | 40 (33.3) | |
| Mixed | 15 (12.5) | 16 (13.3) | |
| Unknown | 4 (3.4) | 5 (4.2) | |
| Tumour differentiation (%) | 0.420 | ||
| Good | 23 (19.2) | 24 (20.0) | |
| Moderate | 45 (37.5) | 43 (35.8) | |
| Poor | 48 (40.0) | 50 (41.7) | |
| Undifferentiated or Signet ring cell carcinoma | 4 (3.3) | 3 (2.5) | |
| pT-stage, n (%) (UICC 8th ed.) | 1.000 | ||
| pT1 | 0 | 0 | |
| pT2 | 29 (24.1) | 29 (24.1) | |
| pT3 | 47 (39.2) | 47 (39.2) | |
| pT4a | 41 (34.2) | 41 (34.2) | |
| pT4b | 3 (2.5) | 3 (2.5) | |
| pN-stage, n (%) (UICC 8th ed.) | 0.987 | ||
| pN0 | 22 (18.3) | 20 (16.7) | |
| pN1 | 48 (40) | 41 (34.2) | |
| pN2 | 16 (13.4) | 11 (9.2) | |
| pN3a | 12 (10) | 29 (24.1) | |
| pN3b | 22 (18.3) | 19 (15.8) | |
| pStage, n (%) (UICC 8th ed.) | 0.798 | ||
| IIA | 42 (35.0) | 45 (37.5) | |
| IIB | 22 (18.3) | 10 (8.3) | |
| IIIA | 20 (16.7) | 21 (17.5) | |
| IIIB | 14 (11.7) | 26 (21.7) | |
| IIIC | 22 (18.3) | 18 (15.0) | |
| Clearance of surgical margin (negative) | |||
| Overall | 117 (97.5%) | 115 (95.8%) | 0.432 |
| Proximal margin | 118 (98.3%) | 118 (98.3%) | 1.000 |
| Distal margin | 119 (99.2%) | 117 (97.5%) | 0.295 |
| Retrieved number of LNs, n | 31.4 ± 11.4 | 33.3 ± 15.4 | 0.134 |
| Mean ± SD (range) | (16–79) | (16–97) | |
| Number of positive lymph nodes, n (%) | 76 (63.3) | 80 (66.7) | 0.760 |
| Variables | LG (n = 120) | OG (n = 120) | Odds Ratio (RR 95% CI) | p Value |
|---|---|---|---|---|
| Postoperative complications, n (%) | ||||
| Overall | 20 (16.7) | 25 (20.8) | 1.3 (−1.9 to 6.6) | 0.210 |
| Anastomotic leakage (1) | 4 (3.3) | 3 (2.5) | 2.3 (−1.1 to 3.9) | 0.500 |
| Duodenal stump leakage (2) | 3 (2.5) | 1 (0.8) | 0.4 (−1.2 to 2.1) | 0.142 |
| Leakages (1) + (2) | 7 (5.8) | 4 (3.3) | 1.6 (−1.1 to 4.2) | 0.072 |
| Anastomotic bleeding | 1 (0.8) | 1 (0.8) | 0.2 (−1.1 to 1.1) | 1.000 |
| Pancreatitis/Pancreatic fistula | 1 (0.8) | 2 (1.7) | 1.3 (−0.1to 2.0) | 0.681 |
| Intra-abdominal collection | 2 (1.7) | 2 (1.7) | 0.4 (−1.4 to 1.4) | 1.000 |
| Intra-abdominal bleeding | 2 (1.7) | 2 (1.7) | 0.4 (−1.4 to 1.4) | 1.000 |
| Bleeding wound complication | 0 | 1 (0.8) | −0.2 (−0.6 to 1.2) | 0.446 |
| Wound infection | 1 (0.8) | 5 (4.2) | 0.8 (−1.1 to 4.3) | <0.01 |
| Pulmonary effusion | 1 (0.8) | 1 (0.8) | −0.2 (−1.1 to 1.1) | 1.000 |
| Pulmonary infection | 1 (0.8) | 5 (4.2) | −0.8 (−2.2 to 0.3) | <0.01 |
| Intestinal obstruction/ileus | 2 (1.7) | 2 (1.7) | −1.1 (−1.4 to 1.4) | 0.475 |
| Cardiac | 1 (0.8) | 0 | 0.2 (−0.6 to 1.2) | 0.695 |
| Hepatic | 1 (0.8) | 0 | 0.2 (−0.6 to 1.2) | 0.744 |
| Reoperation, n (%) | 4 (3.3) | 3 (2.5) | 0.714 | |
| Clavien–Dindo classification | ||||
| Grade II (%) | 7 (5.8) | 11 (9.2) | 0.281 | |
| Wound infection | 1 | 2 | 0.740 | |
| Pulmonary infection | 1 | 4 | <0.05 | |
| Anastomosis bleeding | 1 | 1 | 1.000 | |
| Pancreatitis | 1 | 0 | 1.000 | |
| Bleeding wound complication | 0 | 1 | 1.000 | |
| Intra-abdominal collection | 1 | 1 | 1.000 | |
| Pulmonary effusion | 1 | 1 | 1.000 | |
| Intestinal obstruction/ileus | 1 | 1 | 1.000 | |
| Grade III (%) | 7 (5.8) | 10 (8.3) | 0.628 | |
| Wound infection | 0 | 3 | <0.05 | |
| Pulmonary infection | 0 | 1 | 1.000 | |
| Intra-abdominal collection | 1 | 1 | 1.000 | |
| Anastomotic leakage | 2 | 1 | 1.000 | |
| Duodenal stump leakage | 1 | 1 | 1.000 | |
| Intestinal obstruction/ileus | 1 | 1 | 1.000 | |
| Intra-abdominal bleeding | 2 | 2 | 1.000 | |
| Grade IV (%) | 1 (0.8) | 0 | 1.000 | |
| Anastomotic leakage | 1 | 0 | ||
| Grade V (%) | 5 (4.2) | 4 (3.3) | 0.453 | |
| Anastomotic leakage | 2 | 2 | 1.000 | |
| Heart failure | 1 | 0 | 1.000 | |
| Pancreatitis/Pancreatic fistula | 0 | 2 | 1.000 | |
| Duodenal stump leakage | 2 | 0 | 1.000 | |
| Clavien–Dindo grade ≥III (%) | 13 (10.8) | 14 (11.7) | 0.625 | |
| Mortality, n (%) | 5 (4.2) | 4 (3.3) | 0.987 | |
| Postoperative hospital stay (days; mean ± SD) | 9.1 ± 4.7 | 11.6 ± 4.8 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caruso, S.; Giudicissi, R.; Mariatti, M.; Cantafio, S.; Paroli, G.M.; Scatizzi, M. Laparoscopic vs. Open Gastrectomy for Locally Advanced Gastric Cancer: A Propensity Score-Matched Retrospective Case-Control Study. Curr. Oncol. 2022, 29, 1840-1865. https://doi.org/10.3390/curroncol29030151
Caruso S, Giudicissi R, Mariatti M, Cantafio S, Paroli GM, Scatizzi M. Laparoscopic vs. Open Gastrectomy for Locally Advanced Gastric Cancer: A Propensity Score-Matched Retrospective Case-Control Study. Current Oncology. 2022; 29(3):1840-1865. https://doi.org/10.3390/curroncol29030151
Chicago/Turabian StyleCaruso, Stefano, Rosina Giudicissi, Martina Mariatti, Stefano Cantafio, Gian Matteo Paroli, and Marco Scatizzi. 2022. "Laparoscopic vs. Open Gastrectomy for Locally Advanced Gastric Cancer: A Propensity Score-Matched Retrospective Case-Control Study" Current Oncology 29, no. 3: 1840-1865. https://doi.org/10.3390/curroncol29030151
APA StyleCaruso, S., Giudicissi, R., Mariatti, M., Cantafio, S., Paroli, G. M., & Scatizzi, M. (2022). Laparoscopic vs. Open Gastrectomy for Locally Advanced Gastric Cancer: A Propensity Score-Matched Retrospective Case-Control Study. Current Oncology, 29(3), 1840-1865. https://doi.org/10.3390/curroncol29030151