The Prognostic Effect of Multidisciplinary Team Intervention in Patients with Advanced Gastric Cancer

Abstract
:1. Introduction
2. Materials and Methods
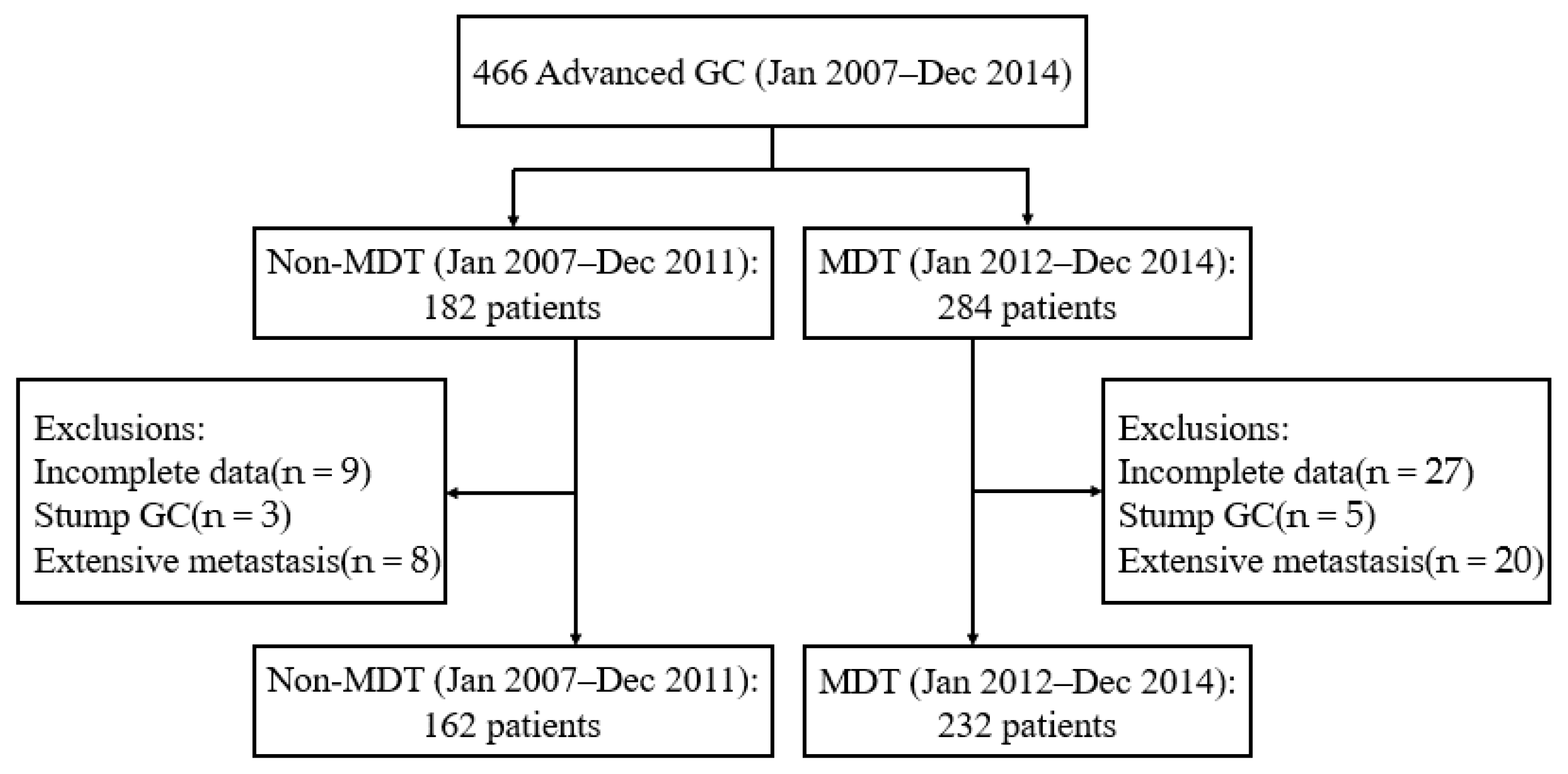
2.1. Basic Characteristics of Patients
2.2. MDT Intervention
2.3. Patients’ Follow-Up Data
2.4. Data Analysis
3. Results
3.1. Clinical Characteristics of Patients
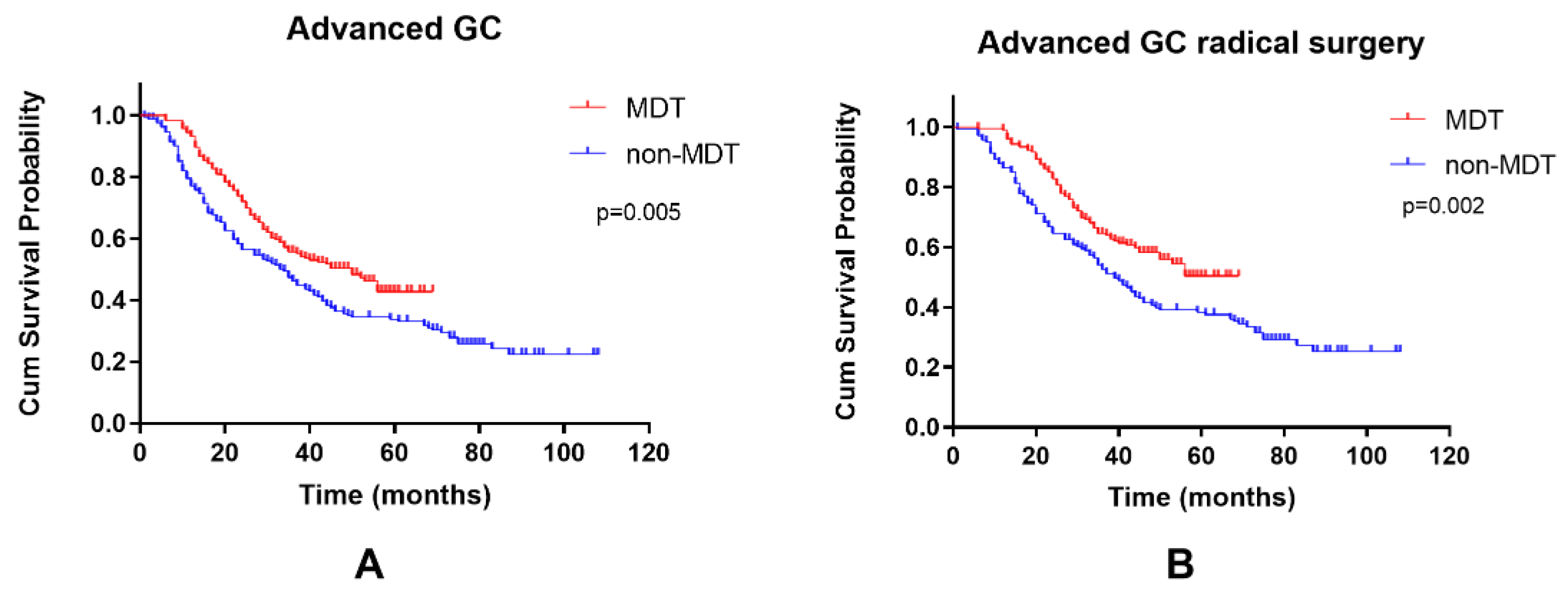
3.2. The Prognosis Effect of MDTs in Advanced GC
3.3. Clinical Characteristics of Stage III Gastric Cancer Patients
3.4. The Prognostic Effect of MDTs in Stage III Gastric Cancer
3.5. Clinical Characteristics of Stage IV Gastric Cancer Patients
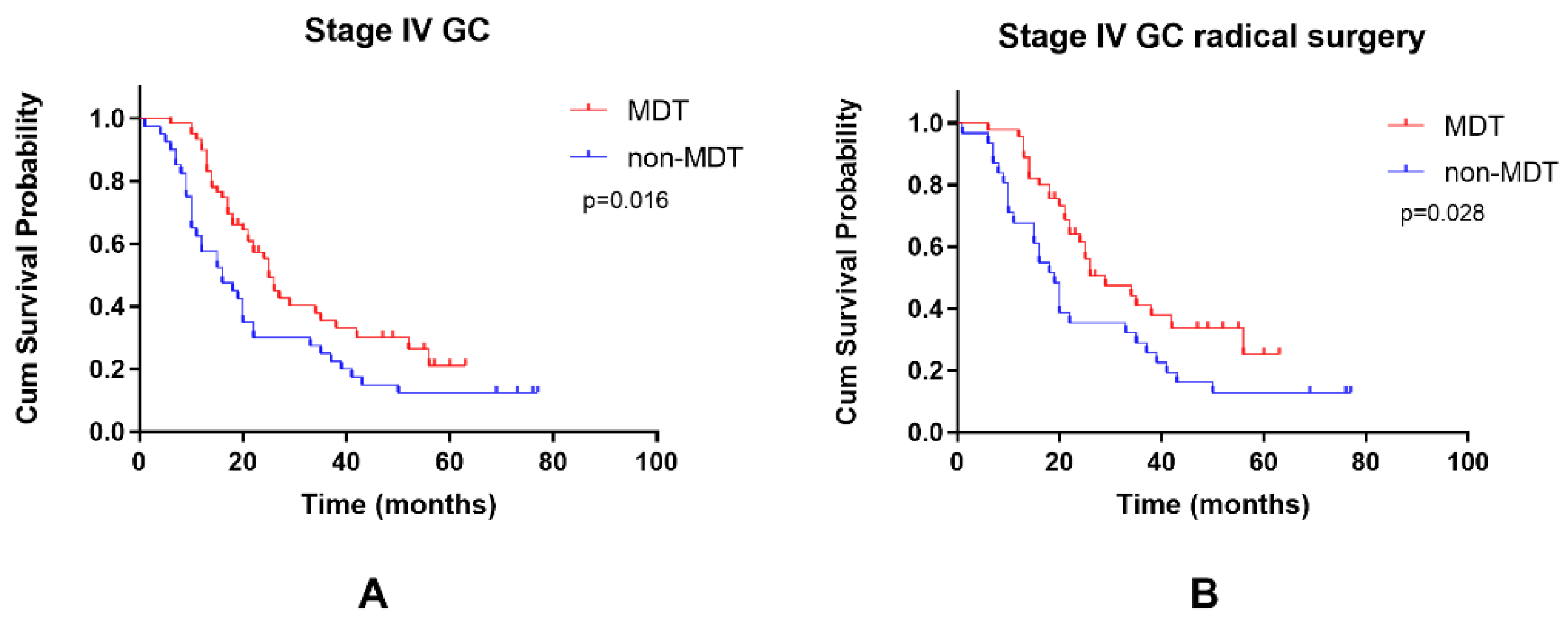
3.6. The Prognostic Effect of MDTs in Stage IV GC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Japanese Gastric Cancer, A. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer 2017, 20, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajani, J.A.; D’Amico, T.A.; Almhanna, K.; Bentrem, D.J.; Chao, J.; Das, P.; Denlinger, C.S.; Fanta, P.; Farjah, F.; Fuchs, C.S.; et al. Gastric Cancer, Version 3.2016, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2016, 14, 1286–1312. [Google Scholar] [CrossRef] [PubMed]
- Tan, Z. Recent Advances in the Surgical Treatment of Advanced Gastric Cancer: A Review. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2019, 25, 3537–3541. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhao, J.; Shen, Z.; Fairweather, M.; Enzinger, P.C.; Sun, Y.; Wang, J. Multidisciplinary Approach in Improving Survival Outcome of Early-Stage Gastric Cancer. J. Surg. Res. 2020, 255, 285–296. [Google Scholar] [CrossRef]
- Di, L.; Wu, H.; Zhu, R.; Li, Y.; Wu, X.; Xie, R.; Li, H.; Wang, H.; Zhang, H.; Xiao, H.; et al. Multi-disciplinary team for early gastric cancer diagnosis improves the detection rate of early gastric cancer. BMC Gastroenterol. 2017, 17, 147. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Chen, L. Chinese consensus on the diagnosis and treatment of gastric cancer with liver metastases. Ther. Adv. Med. Oncol. 2020, 12, 1758835920904803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, A.R.; Deans, D.A.; Penman, I.; Plevris, J.N.; Fletcher, J.; Wall, L.; Phillips, H.; Gilmour, H.; Patel, D.; de Beaux, A.; et al. The multidisciplinary team meeting improves staging accuracy and treatment selection for gastro-esophageal cancer. Dis. Esophagus 2006, 19, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Lamb, B.W.; Sevdalis, N.; Mostafid, H.; Vincent, C.; Green, J.S. Quality improvement in multidisciplinary cancer teams: An investigation of teamwork and clinical decision-making and cross-validation of assessments. Ann. Surg. Oncol. 2011, 18, 3535–3543. [Google Scholar] [CrossRef] [PubMed]
- Kurpad, R.; Kim, W.; Rathmell, W.K.; Godley, P.; Whang, Y.; Fielding, J.; Smith, L.; Pettiford, A.; Schultz, H.; Nielsen, M.; et al. A multidisciplinary approach to the management of urologic malignancies: Does it influence diagnostic and treatment decisions? Urol. Oncol. 2011, 29, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; Bentrem, D.J.; Besh, S.; D’Amico, T.A.; Das, P.; Denlinger, C.; Fakih, M.G.; Fuchs, C.S.; Gerdes, H.; Glasgow, R.E.; et al. Gastric cancer, version 2.2013: Featured updates to the NCCN Guidelines. J. Natl. Compr. Cancer Netw. JNCCN 2013, 11, 531–546. [Google Scholar] [CrossRef] [Green Version]
- Ju, M.; Wang, S.C.; Syed, S.; Agrawal, D.; Porembka, M.R. Multidisciplinary Teams Improve Gastric Cancer Treatment Efficiency at a Large Safety Net Hospital. Ann. Surg. Oncol. 2019. [Google Scholar] [CrossRef]
- Pillay, B.; Wootten, A.C.; Crowe, H.; Corcoran, N.; Tran, B.; Bowden, P.; Crowe, J.; Costello, A.J. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat. Rev. 2016, 42, 56–72. [Google Scholar] [CrossRef] [PubMed]
- Basta, Y.L.; Baur, O.L.; van Dieren, S.; Klinkenbijl, J.H.; Fockens, P.; Tytgat, K.M. Is there a Benefit of Multidisciplinary Cancer Team Meetings for Patients with Gastrointestinal Malignancies? Ann. Surg. Oncol. 2016, 23, 2430–2437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basta, Y.L.; Bolle, S.; Fockens, P.; Tytgat, K. The Value of Multidisciplinary Team Meetings for Patients with Gastrointestinal Malignancies: A Systematic Review. Ann. Surg. Oncol. 2017, 24, 2669–2678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pawlik, T.M.; Laheru, D.; Hruban, R.H.; Coleman, J.; Wolfgang, C.L.; Campbell, K.; Ali, S.; Fishman, E.K.; Schulick, R.D.; Herman, J.M.; et al. Evaluating the impact of a single-day multidisciplinary clinic on the management of pancreatic cancer. Ann. Surg. Oncol. 2008, 15, 2081–2088. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Xu, X.; Su, D.; Zhou, T.; Wang, G.; Li, Z.J.B.C. Long-term survival of an elderly patient with advanced gastric cancer after combination therapy: A case report and literature review. BMC Cancer 2019, 19, 459. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Zhang, W.; Yang, L.; Du, C.; Li, N.; Xing, G.; Tian, Y.; Xie, Y.J.W.J.O.G. Role of D2 gastrectomy in gastric cancer with clinical para-aortic lymph node metastasis. World J. Gastroenterol. 2019, 25, 2338–2353. [Google Scholar] [CrossRef]
- Stone, E.; Rankin, N.; Kerr, S.; Fong, K.; Currow, D.; Phillips, J.; Connon, T.; Zhang, L.; Shaw, T.J.L.C. Does presentation at multidisciplinary team meetings improve lung cancer survival? Findings from a consecutive cohort study. Lung Cancer 2018, 124, 199–204. [Google Scholar] [CrossRef]
- Tsai, C.; Hsieh, H.; Lai, T.; Kung, P.; Kuo, W.; Tsai, W.J.B. Effect of multidisciplinary team care on the risk of recurrence in breast cancer patients: A national matched cohort study. Breast 2020, 53, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.; Brown, M.; Niblock, P.; Steele, R.; Carey, F. Do Multidisciplinary Team (MDT) processes influence survival in patients with colorectal cancer? A population-based experience. BMC Cancer 2015, 15, 686. [Google Scholar] [CrossRef] [Green Version]
- Hsu, P.; Chien, L.; Huang, C.; Yeh, Y.; Huang, P.; Chen, M.; Chen, S.; Yen, C.; Hsu, H.J.A.O.S.O. Treatment Patterns and Outcomes in Patients with Esophageal Cancer: An Analysis of a Multidisciplinary Tumor Board Database. Ann. Surg. Oncol. 2021, 28, 5414–5422. [Google Scholar] [CrossRef]
- Zhu, S.; Chen, J.; Ni, Y.; Zhang, H.; Liu, Z.; Shen, P.; Sun, G.; Liang, J.; Zhang, X.; Wang, Z.; et al. Dynamic multidisciplinary team discussions can improve the prognosis of metastatic castration-resistant prostate cancer patients. Prostate 2021, 81, 721–727. [Google Scholar] [CrossRef]
- Galan, M.; Farran, L.; Aliste, L.; Hormigo, G.; Aranda, H.; Bettonica, C.; Boladeras, A.M.; Botargues, J.M.; Calvo, M.; Creus, G.; et al. Multidisciplinary cancer care may impact on the postoperative mortality and survival of patients with oesophageal and oesophagogastric junction cancer: A retrospective cohort study. Clin. Transl. Oncol. 2015, 17, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Bouvier, A.M.; Créhange, G.; Azélie, C.; Cheynel, N.; Jouve, J.L.; Bedenne, L.; Faivre, J.; Lepage, C.; Maingon, P. Adjuvant treatments for gastric cancer: From practice guidelines to clinical practice. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2014, 46, 72–75. [Google Scholar] [CrossRef]
- Ychou, M.; Boige, V.; Pignon, J.P.; Conroy, T.; Bouché, O.; Lebreton, G.; Ducourtieux, M.; Bedenne, L.; Fabre, J.M.; Saint-Aubert, B.; et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: An FNCLCC and FFCD multicenter phase III trial. J. Clin. Oncol. 2011, 29, 1715–1721. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v38–v49. [Google Scholar] [CrossRef]
- Du, C.Z.; Li, J.; Cai, Y.; Sun, Y.S.; Xue, W.C.; Gu, J. Effect of multidisciplinary team treatment on outcomes of patients with gastrointestinal malignancy. World J. Gastroenterol. 2011, 17, 2013–2018. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, J.; Fushida, S.; Tsukada, T.; Oyama, K.; Okamoto, K.; Makino, I.; Nakamura, K.; Miyashita, T.; Tajima, H.; Takamura, H.; et al. Efficacy of conversion gastrectomy following docetaxel, cisplatin, and S-1 therapy in potentially resectable stage IV gastric cancer. Eur. J. Surg. Oncol. 2015, 41, 1354–1360. [Google Scholar] [CrossRef] [Green Version]
- Beom, S.H.; Choi, Y.Y.; Baek, S.E.; Li, S.X.; Lim, J.S.; Son, T.; Kim, H.I.; Cheong, J.H.; Hyung, W.J.; Choi, S.H.; et al. Multidisciplinary treatment for patients with stage IV gastric cancer: The role of conversion surgery following chemotherapy. BMC Cancer 2018, 18, 1116. [Google Scholar] [CrossRef] [PubMed]
- Fukuchi, M.; Ishiguro, T.; Ogata, K.; Suzuki, O.; Kumagai, Y.; Ishibashi, K.; Ishida, H.; Kuwano, H.; Mochiki, E. Prognostic Role of Conversion Surgery for Unresectable Gastric Cancer. Ann. Surg. Oncol. 2015, 22, 3618–3624. [Google Scholar] [CrossRef]
- Schildberg, C.W.; Weidinger, T.; Hohenberger, W.; Wein, A.; Langheinrich, M.; Neurath, M.; Boxberger, F. Metastatic adenocarcinomas of the stomach or esophagogastric junction (UICC stage IV) are not always a palliative situation: A retrospective analysis. World J. Surg. 2014, 38, 419–425. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Non-MDT (n = 162) | MDT (n = 232) | p |
|---|---|---|---|
| Age (years) | |||
| <60 | 93 (57.4) | 143 (61.6) | 0.399 |
| ≥60 | 69 (42.6) | 89 (38.4) | |
| Sex | |||
| Male | 108 (66.7) | 146 (62.9) | 0.446 |
| Female | 54 (33.3) | 86 (37.1) | |
| Primary tumor site | |||
| Upper | 47 (29.0) | 85 (36.6) | 0.284 |
| Middle | 41 (25.3) | 62 (26.7) | |
| Lower | 62 (38.3) | 73 (31.5) | |
| Whole | 12 (7.4) | 12 (5.2) | |
| Radical resection | |||
| No | 23 (14.2) | 37 (15.9) | 0.634 |
| Yes | 139 (85.8) | 195 (84.1) | |
| cT stage | |||
| T1 + T2 | 4 (2.5) | 5 (2.2) | 0.000 *** |
| T3 | 106 (65.4) | 90 (38.8) | |
| T4 | 52 (32.1) | 137 (59.1) | |
| cN stage | |||
| N0 | 5 (3.1) | 32 (13.8) | 0.000 *** |
| N1 | 23 (14.2) | 30 (12.9) | |
| N2 | 84 (51.9) | 65 (28.0) | |
| N3 | 50 (30.9) | 105 (45.3) | |
| cTNM stage | |||
| III | 122 (75.3) | 172 (74.1) | 0.793 |
| IV | 40 (24.7) | 60 (25.9) | |
| Differentiation | |||
| Moderate | 30 (18.5) | 59 (25.4) | 0.106 |
| Poor | 132 (81.5) | 173 (74.6) | |
| Borrmann type | |||
| I + II | 25 (15.4) | 41 (17.7) | 0.558 |
| III + IV | 137 (84.6) | 191 (82.3) | |
| CEA (ug/L) | |||
| ≤5 | 111 (68.5) | 173 (74.6) | 0.188 |
| >5 | 51 (31.5) | 59 (25.4) |
| Characteristics | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age (years) | ||||||
| <60 | 1.000 | 1.000 | ||||
| ≥60 | 1.056 | 0.813–1.371 | 0.684 | 1.204 | 0.912–1.590 | 0.191 |
| Sex | ||||||
| Male | 1.000 | 1.000 | ||||
| Female | 1.138 | 0.872–1.475 | 0.341 | 1.156 | 0.868–1.540 | 0.320 |
| Primary tumor site | ||||||
| Upper | 1.000 | 1.000 | ||||
| Middle | 0.920 | 0.648–1.305 | 0.639 | 0.623 | 0.425–0.912 | 0.015 * |
| Lower | 1.035 | 0.756–1.417 | 0.829 | 0.828 | 0.595–1.153 | 0.263 |
| Whole | 2.039 | 1.243–3.346 | 0.005 ** | 1.192 | 0.706–2.010 | 0.511 |
| Radical resection | ||||||
| No | 1.000 | 1.000 | ||||
| Yes | 0.147 | 0.106–0.203 | 0.000 *** | 0.127 | 0.087–0.185 | 0.000 *** |
| cT stage | ||||||
| T1 + T2 | 1.000 | 1.000 | ||||
| T3 | 1.814 | 0.688–5.046 | 0.221 | 2.116 | 0.758–5.907 | 0.152 |
| T4 | 1.616 | 0.595–4.393 | 0.346 | 2.433 | 0.862–6.866 | 0.093 |
| cN stage | ||||||
| N0 | 1.000 | 1.000 | ||||
| N1 | 1.391 | 0.698–2.769 | 0.348 | 1.408 | 0.687–2.886 | 0.349 |
| N2 | 1.645 | 0.894–3.025 | 0.110 | 1.883 | 0.959–3.698 | 0.066 |
| N3 | 3.326 | 1.833–6.033 | 0.000 *** | 3.760 | 1.938–7.295 | 0.000 *** |
| cTNM stage | ||||||
| III | 1.000 | 1.000 | ||||
| IV | 2.917 | 1.660–2.907 | 0.000 | 1.320 | 0.960–1.814 | 0.088 |
| Differentiation | ||||||
| Moderate | 1.000 | 1.000 | ||||
| Poor | 1.976 | 1.379–2.832 | 0.000 *** | 1.597 | 1.086–2.349 | 0.017 * |
| Borrmann type | ||||||
| I + II | 1.000 | 1.000 | ||||
| III + IV | 1.651 | 1.125–2.424 | 0.010 * | 1.174 | 0.777–1.773 | 0.446 |
| CEA (μg/L) | ||||||
| ≤5 | 1.000 | 1.000 | ||||
| >5 | 1.360 | 1.032–1.791 | 0.029 * | 1.420 | 1.058–1.907 | 0.020 * |
| Group | ||||||
| Non-MDT | 1.000 | 1.000 | ||||
| MDT | 0.689 | 0.528–0.899 | 0.006 ** | 0.493 | 0.365–0.667 | 0.000 *** |
| Characteristics | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age (years) | ||||||
| <60 | 1.000 | 1.000 | ||||
| ≥60 | 1.088 | 0.794–1.492 | 0.598 | 1.254 | 0.894–1.759 | 0.190 |
| Sex | ||||||
| Male | 1.000 | 1.000 | ||||
| Female | 1.704 | 0.775–1.489 | 0.666 | 1.096 | 0.782–1.537 | 0.594 |
| Primary tumor site | ||||||
| Upper | 1.000 | 1.000 | ||||
| Middle | 0.711 | 0.463–1.094 | 0.121 | 0.464 | 0.293–0.736 | 0.001 ** |
| Lower | 0.931 | 0.646–1.343 | 0.703 | 0.829 | 0.553–1.243 | 0.364 |
| Whole | 1.499 | 0.743–3.025 | 0.258 | 0.864 | 0.416–1.794 | 0.695 |
| Radical resection | ||||||
| No | 1.000 | 1.000 | ||||
| Yes | 0.044 | 0.026–0.072 | 0.000 *** | 0.044 | 0.025–0.077 | 0.000 *** |
| cT stage | ||||||
| T1 + T2 | 1.000 | 1.000 | ||||
| T3 | 1.309 | 0.414–4.138 | 0.646 | 1.97 | 0.581–6.676 | 0.276 |
| T4 | 0.990 | 0.311–3.156 | 0.986 | 2.836 | 0.798–10.08 | 0.107 |
| cN stage | ||||||
| N0 | 1.000 | 1.000 | ||||
| N1 | 1.145 | 0.514–2.55 | 0.74 | 0.721 | 0.317–1.639 | 0.435 |
| N2 | 1.387 | 0.708–2.718 | 0.34 | 0.957 | 0.457–2.005 | 0.908 |
| N3 | 3.173 | 1.635–6.16 | 0.001 ** | 2.203 | 1.038–4.677 | 0.040 * |
| Differentiation | ||||||
| Moderate | 1.000 | 1.000 | ||||
| Poor | 2.392 | 1.510–3.788 | 0.000 *** | 2.206 | 1.336–3.643 | 0.002 ** |
| Borrmann type | ||||||
| I + II | 1.000 | 1.000 | ||||
| III + IV | 1.542 | 1.005–2.365 | 0.047 | 1.426 | 0.895–2.271 | 0.135 |
| CEA (μg/L) | ||||||
| ≤5 | 1.000 | 1.000 | ||||
| >5 | 1.358 | 0.970–1.901 | 0.074 | 1.544 | 1.061–2.247 | 0.023 * |
| Group | ||||||
| Non-MDT | 1.000 | 1.000 | ||||
| MDT | 0.709 | 0.511–0.982 | 0.039 * | 0.504 | 0.347–0.731 | 0.000 *** |
| Characteristics | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age (years) | ||||||
| <60 | 1.000 | 1.000 | ||||
| ≥60 | 1.113 | 0.695–1.781 | 0.656 | 1.413 | 0.834–2.393 | 0.198 |
| Sex | ||||||
| Male | 1.000 | 1.000 | ||||
| Female | 1.240 | 0.781–1.969 | 0.361 | 1.048 | 0.585–1.878 | 0.874 |
| Primary tumor site | ||||||
| Upper | 1.000 | 1.000 | ||||
| Middle | 1.452 | 0.752–2.804 | 0.267 | 1.476 | 0.665–3.275 | 0.338 |
| Lower | 1.137 | 0.601–2.150 | 0.693 | 1.173 | 0.584–2.354 | 0.654 |
| Whole | 2.202 | 1.001–4.844 | 0.050 | 1.920 | 0.783–4.713 | 0.154 |
| Radical resection | ||||||
| No | 1.000 | 1.000 | ||||
| Yes | 0.529 | 0.315–0.888 | 0.016 * | 0.323 | 0.167–0.624 | 0.001 ** |
| cT stage | ||||||
| T1 + T2 | 1.000 | 1.000 | ||||
| T3 | 4.57 | 0.624–33.482 | 0.135 | 2.966 | 0.362–24.283 | 0.311 |
| T4 | 4.628 | 0.632–33.869 | 0.131 | 4.051 | 0.479–34.256 | 0.199 |
| cN stage | ||||||
| N0 | 1.000 | 1.000 | ||||
| N1 | 1.806 | 0.395–8.253 | 0.446 | 3.938 | 0.709–21.86 | 0.117 |
| N2 | 4.119 | 0.952–17.816 | 0.058 | 11.408 | 2.189–59.466 | 0.004 ** |
| N3 | 2.887 | 0.699–11.918 | 0.143 | 10.398 | 1.906–56.724 | 0.007 ** |
| Differentiation | ||||||
| Moderate | 1.000 | 1.000 | ||||
| Poor | 1.219 | 0.680–2.185 | 0.505 | 1.314 | 0.699–2.469 | 0.397 |
| Borrmann type | ||||||
| I + II | 1.000 | 1.000 | ||||
| III + IV | 1.389 | 0.729–2.645 | 0.317 | 1.300 | 0.576–2.931 | 0.528 |
| CEA (μg/L) | ||||||
| ≤5 | 1.000 | 1.000 | ||||
| >5 | 1.300 | 0.801–2.109 | 0.288 | 1.405 | 0.792–2.493 | 0.245 |
| Group | ||||||
| Non-MDT | 1.000 | 1.000 | ||||
| MDT | 0.578 | 0.366–0.915 | 0.019 * | 0.368 | 0.203–0.667 | 0.001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiang, Y.-Y.; Deng, C.-C.; Liu, H.-Y.; Kuo, Z.-C.; Zhang, C.-H.; He, Y.-L. The Prognostic Effect of Multidisciplinary Team Intervention in Patients with Advanced Gastric Cancer. Curr. Oncol. 2022, 29, 1201-1212. https://doi.org/10.3390/curroncol29020102
Xiang Y-Y, Deng C-C, Liu H-Y, Kuo Z-C, Zhang C-H, He Y-L. The Prognostic Effect of Multidisciplinary Team Intervention in Patients with Advanced Gastric Cancer. Current Oncology. 2022; 29(2):1201-1212. https://doi.org/10.3390/curroncol29020102
Chicago/Turabian StyleXiang, Yuan-Yuan, Cun-Can Deng, Han-Yuan Liu, Zi-Chong Kuo, Chang-Hua Zhang, and Yu-Long He. 2022. "The Prognostic Effect of Multidisciplinary Team Intervention in Patients with Advanced Gastric Cancer" Current Oncology 29, no. 2: 1201-1212. https://doi.org/10.3390/curroncol29020102
APA StyleXiang, Y.-Y., Deng, C.-C., Liu, H.-Y., Kuo, Z.-C., Zhang, C.-H., & He, Y.-L. (2022). The Prognostic Effect of Multidisciplinary Team Intervention in Patients with Advanced Gastric Cancer. Current Oncology, 29(2), 1201-1212. https://doi.org/10.3390/curroncol29020102