Abstract
Immune-checkpoint inhibitors (ICIs) are the most effective treatments nowadays. Nivolumab was the second ICI used for treating solid tumors with amazing results. Patients treated with Nivolumab may react differently to this treatment. Some people tolerate this treatment very well without experiencing any adverse reactions, whilst some may have mild symptoms and a part of them can present severe reactions. In our research, we sought to identify the answers to four questions: 1. what type of cancer has more severe hypersensitivity reactions to Nivolumab, 2. what is the time frame for developing these severe reactions to Nivolumab, 3. whether it is best to continue or stop the treatment after a severe hypersensitivity reaction to Nivolumab and 4. what severe hypersensitivity reactions are the most frequent reported along Nivolumab treatment. This review also highlights another problem with regard to the usage of concomitant and prior medications or other methods of treatment (e.g., radiation therapy), which can also lead to severe reactions. Treatment with Nivolumab is very well tolerated, but patients should also be warned of the possibility of severe hypersensitivity reactions for which they should urgently see a doctor for a personalized evaluation. There are some options for individuals with severe hypersensitivity reactions, for eg. switching the medication or applying a desensitization protocol.
1. Introduction
In recent years, immunotherapy has become the most used treatment in metastatic cancers besides targeted treatments. Immune-checkpoint inhibitors (ICIs) are molecules that enhance the activity of the immune system by blocking the interaction between programmed cell death 1 (PD-1) and its ligand: programmed cell death ligand 1 (PD-L1) and programmed cell death ligand 2 (PD-L2); or by blocking the costimulatory molecule represented by cytotoxic T lymphocyte-associated protein 4 (CTLA-4) [1,2,3,4,5]. They are divided into 3 classes: PD-1 inhibitors (Nivolumab, Pembrolizumab, Cemiplimab, and Dostarlimab), PD-L1 inhibitors (Avelumab, Atezolizumab, and Durvalumab) and CTLA-4 inhibitors (Ipilimumab).
Nivolumab, a fully human IgG 4 antibody, directed against PD-1, is the first ICI treatment approved for metastatic lung cancer [5,6,7]. It is generally very well tolerated by patients, but can induce immune-related adverse effects (irAEs), which could affect any organ system. The adverse reactions consist of endocrine reactions (e.g., hypothyroidism, hyperthyroidism, thyroiditis), skin reactions (e.g., rash, pruritus, vitiligo, dry skin, erythema, urticaria), metabolic reactions (e.g., decreased appetite, hyperglycemia, hypoglycemia), pulmonary reactions (e.g., dyspnea, cough, pneumonitis, pleural effusion), gastrointestinal reactions (e.g., diarrhea, abdominal pain, constipation, colitis, stomatitis, dry mouth), cardiac reactions (e.g., tachycardia, atrial fibrillation, myocarditis), neurologic reactions (e.g., headache, peripheral neuropathy, dizziness), blood disorders (e.g., lymphopenia, anemia, leucopenia, neutropenia, thrombocytopenia), fatigue, pyrexia, oedema [8]. The hypersensitivity type of reactions to Nivolumab is very rare, between 1% and 3% [9,10], but it is important for them to be recognized early because they need prompt intervention.
A hypersensitivity reaction is an inappropriate or exaggerated immune response to either an antigen or allergen. The hypersensitivity reactions can be divided into two subgroups of immediate reactions (<1 h) or delayed reactions (>1 h) [11]. Immediate reactions are type I and include pruritus, edema, urticaria, and anaphylactic shock [12]. The delayed ones are type IV reactions, mediated by T-cells, and include drug-induced agranulocytosis (DIA), drug-induced skin disorders (DISI), drug-induced liver injury (DILI), and drug-induced renal injury (DIRI) [11]. The DISI group contains contact allergy, fixed drug eruption (FDE), acute, generalized exanthematic pustulosis (AGEP), maculopapular rash (MPR), Stevens–Johnson Syndrome (SJS), toxic epidermal necrolysis (TEN), drug reaction with eosinophilia and systemic symptoms (DRESS) [11,13]. The hypersensitivity reactions may be regarded as a subcategory of irAEs in patients receiving ICIs [14].
2. Materials and Methods
This review has been conducted meeting the guidelines of Preferred Reporting Items for Systematic Reviews (PRISMA 2020). The registration number: no 41482 and the date of approval is 9 August 2022.
2.1. The Review Questions
Are there many severe hypersensitivity reactions to Nivolumab described in the literature? What type of cancer has the most severe hypersensitivity reactions to Nivolumab? What is the time frame for developing severe hypersensitivity reactions to Nivolumab? How are Nivolumab hypersensitivity reactions managed through the literature search? What types of severe hypersensitivity reactions are more frequently reported?
2.2. Literature Search
The literature search was performed in the electronic database of PubMed, and the following combination has been researched: “Nivolumab hypersensitivity reaction”. The search was performed between 2013 and September 2022. The relevant articles related to the questions of this review were identified and only those that met the eligibility criteria were assessed. The inclusion and exclusion criteria are provided in Table 1.

Table 1.
Inclusion and exclusion criteria.
2.3. Data Extraction and Presentation
Using the aforementioned combination of keywords, we searched for the articles published in PubMed. The search yielded a total of 129 articles, of which 104 of them were irrelevant or duplicated. Among the 25 articles relevant to this review, only 18 studies met the eligibility criteria and were included in this systematic review. The flow chart of the research is presented in Figure 1.
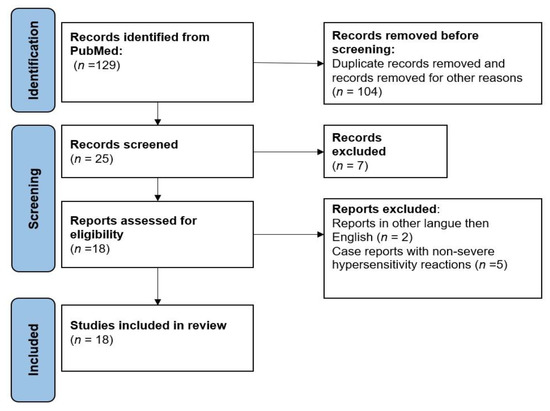
Figure 1.
Flow chart showing the strategy used in this systematic review.
3. Results
This research included only 18 articles. These articles are case reports of severe hypersensitivity reactions to Nivolumab. We excluded from this study the cases with non-severe reactions, grade 1 or 2 according to CTCAE v 5.0, November 2017 [15], and erythema nodosum, lichen planus, morphea, lichen sclerosus et atrophicus. All the included studies are summarized in Table 2.
Table 2.
Cases of Nivolumab hypersensitivity reactions.
4. Discussion
Among the irAEs of ICIs, the most frequently reported are the dermatological ones, which consist of rash and pruritus. They are present in up to 25% of melanoma patients and in 10% or more of non-small-cell lung cancer patients [33,34,35]. Other dermatological irAE (dirAEs) are vitiligo-like depigmentation, morbilliform exanthem, lichenoid dermatitis, bullous pemphigoid, and severe cutaneous irAEs like Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN), acute generalized exanthematous pustulosis (AGEP) and drug reaction with eosinophilia and systemic symptoms (DRESS). Xerosis, alopecia areata, stomatitis, urticaria, photosensitivity reactions [9,17], hyperhidrosis, skin exfoliation [34,36], and hair color changes are rare, but present in daily practice [37].
Most of the dirAEs are low to moderate grades according to the CTCAE v 5.0, November 2017 [15]. In grade 1 and 2 dirAEs, the treatment consists of topical corticosteroids with moderate or high potency and supportive care. Severe dirAEs (grade 3 and grade 4) require the administration of high-dose systemic corticosteroid treatment, intense supportive care management, and wound management. In some cases, it is a must to administer tumor necrosis factor alpha (TNF-α) inhibitors (Infliximab or Etanercept), Mycophenolate mofetil, Cyclosporin, and even plasmapheresis [34,36] These reactions require a definitive interruption of immunotherapy [38,39,40].
In our study, we found nineteen cases of severe hypersensitivity reactions to Nivolumab: nine cases of female patients, seven cases of male patients, and three cases without the sex of the patient mentioned in the article. Regarding the solid tumor’s distribution, there were 6/19 patients with gastrointestinal cancers (31.58%), 5/19 lung cancer patients (26.32%), 4/19 melanoma patients (21.05%), 3/19 renal cancer patients (15.79%) and 1/19 patients with head and neck cancer (5.26%) who have developed severe hypersensitivity reactions to Nivolumab. It appears that Nivolumab hypersensitivity reactions are more frequent in patients with gastrointestinal cancers. This may be due to the fact that the gut microbiome is considered responsible for the modulation of immune responses. Lu Y highlighted in his review that the gut microbiome can generate increased responses to ICIs by adjusting the CD8+ T cells, T helper 1, and tumor-associated myeloid cell proportions [41]. In a study of fecal microbial transplantation, the mouse who received the transplant had an increased level of CD8+ T cells [42]. In another review article, Pierrard J. et al. showed that the development of irAEs in mouse models can be influenced by the composition and modifications in the gut microbiome [43]. Patients with Bifidobacterium longum, Collinsella aerofaciens and Enterococcus faecium present in gut microbiome show good responses to anti-PD-1 therapy. In some studies, the Ruminococaceae family of the Firmicutes phylum is responsible for the development of irAEs [44,45].
Most of the hypersensitivity reactions were present in the first week after starting the treatment with Nivolumab and only four of the authors reported different times for the development of the adverse reactions. P. Basu et al. reported the presence of TEN after 2 years [17], Constantin A Dasanu et al. reported the presence of SJS/TEN at 16 weeks [18], Yi-Tsz Lin et al. reported the presence of SJS after 18 cycles [23], while Yuko Watanabe et al. reported them at 7 months [25].
In recent studies, the efficacy of ICIs has been related to the development of irAE in NSCLC patients [45,46]. In NSCLC patients it has been demonstrated by Hussaini et al. that patients with irAE have a better objective response rate (ORR) (41.49% vs. 18.01% without irAEs), a better progression-free survival (PFS) (median 8.97 vs. 3.06 months) and a longer overall survival (OS) (median 19.07 vs. 7.45 months) [47,48]. In melanoma patients, the development of dirAE, especially vitiligo, is associated with the efficacy of ICI treatment in stages III and IV [49,50,51]. Other reports, sustain that the development of irAE was associated with a higher objective response rate (ORR), but not with progression-free survival (PFS) [52].
It is very essential to know the patient previous medications used to treat their cancers or if the patient was exposed to radiation therapy. We should check this information on the hospital networks or hospital records. In our research, five authors reported severe hypersensitivity reactions after Nivolumab was stopped. Yasushige Takeda et al. documented a case of SJS after two cycles of S-1 and Docetaxel for gastric cancer, the author mentioned that the patient received Nivolumab before the start of the first cycle of S-1 and Docetaxel [20]. Takayoshi Komatsu-Fujii et al. reported a case of SJS in a patient receiving tegafur/gimeracil/oteracil (TS-1) who was previously treated with Nivolumab for his disease [53]. Yi-Tsz Lin et al. showed a case of SJS induced by treatment with Esomeprazole in a patient who received Nivolumab for advanced lung cancer [23]. M Arenbergerova et al. related a case of TEN induced by Vemurafenib after discontinuation of Nivolumab [54]. Maximova N et al. presented another patient diagnosed with DRESS induced by Vemurafenib administration after Nivolumab, who responded very well to the administration of Tocilizumab and Infliximab [29]. Also, there are some reports of SJS syndrome induced by radiation in patients receiving Nivolumab [24,55] or anticonvulsant drugs like phenytoin [56], phenobarbital [57], and amifostine [58].
Only two cases in our research of the literature continued desensitization to Nivolumab as an alternative to continuing therapy: a 57 years old female with kidney cancer who developed an infusion reaction to Nivolumab during her third cycle and another patient with kidney cancer [22,31]. In one of the 19 cases Nivolumab was switched with Pembrolizumab and in another one, the combination of Vemurafenib and Cobimetinib was changed to Trametinib and Dabrafenib. The patients stopped showing signs of adverse reactions [16,28]. The combination of chemotherapy, antibiotics and antiretroviral therapy brings more adverse reactions than the treatment with just Nivolumab [45,59,60,61].
Although our research has only a limited number of studies, the distribution of the severe hypersensitivity reactions to Nivolumab was the following: 42.10% of the patients developed SJS (8/19 patients), 26.32% of the patients developed TEN (5/19 patients), 15.79% of the patients developed infusion reactions (3/19 patients), 10.53%of the patients developed DRESS (2/19 patients) and 5.26% of the patients developed CCR grade 3 (1/19 patients). This is the first study reporting the distribution of severe hypersensitivity reactions on Nivolumab in solid tumors.
In our literature research, 10.53% of the patients (2/19 patients) died of the complications of the hypersensitivity reactions and 15.79% of the patients (3/19 patients) presented progression to disease and died afterward [17,19,23,25,26]. Only 5.26% of the patients (1/19 patients) had a complete response to Nivolumab treatment after DRESS and 15.79% of the patients (3/19 patients) had stable disease [9,22,28,31].
Our review has some limitations. We could include in our study only 18 articles on severe hypersensitivity reactions to Nivolumab. We focused our search only on solid tumors and did not include hematological malignancies. Furthermore, our findings need to be extended to include the hematological malignancies treated with Nivolumab.
5. Conclusions
The treatment with Nivolumab is very effective and very well tolerated by most patients without developing any irAE. It is crucial to recognize the prodromal symptoms of severe reactions to the Nivolumab treatment and to promptly intervene. As our research of the literature showed, switching the medication or applying a desensitization protocol are options for severe reactions to Nivolumab.
Author Contributions
Conceptualization, C.-F.P.; methodology, A.I.P.; software, C.O.S.; validation, M.O.; formal analysis, A.M.P.; investigation, C.I.; resources, I.N.; data curation, P.M.; writing—original draft preparation, C.-F.P.; writing—review and editing, C.N.; visualization, C.H.; supervision, L.S.C.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Shiravand, Y.; Khodadadi, F.; Kashani, S.M.A.; Hosseini-Fard, S.R.; Hosseini, S.; Sadeghirad, H.; Ladwa, R.; O’Byrne, K.; Kulasinghe, A. Immune Checkpoint Inhibitors in Cancer Therapy. Curr. Oncol. 2022, 29, 3044–3060. [Google Scholar] [CrossRef] [PubMed]
- Weinmann, S.C.; Pisetsky, D.S. Mechanisms of immune-related adverse events during the treatment of cancer with immune checkpoint inhibitors. Rheumatology 2019, 58 (Suppl. 7), vii59–vii67. [Google Scholar] [CrossRef] [PubMed]
- Westdorp, H.; Sweep, M.W.D.; Gorris, M.A.J.; Hoentjen, F.; Boers-Sonderen, M.J.; van der Post, R.S.; Heuvel, M.M.V.D.; Piet, B.; Boleij, A.; Bloemendal, H.J.; et al. Mechanisms of Immune Checkpoint Inhibitor-Mediated Colitis. Front. Immunol. 2021, 12, 768957. [Google Scholar] [CrossRef] [PubMed]
- Lipson, E.J.; Drake, C.G. Ipilimumab: An Anti-CTLA-4 Antibody for Metastatic Melanoma. Clin. Cancer Res. 2011, 17, 6958–6962. [Google Scholar] [CrossRef]
- Esfahani, K.; Roudaia, L.; Buhlaiga, N.; Del Rincon, S.V.; Papneja, N.; Miller, W.H. A Review of Cancer Immunotherapy: From the Past, to the Present, to the Future. Curr. Oncol. 2020, 27, 87–97. [Google Scholar] [CrossRef]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Opdivo-Epar-Product-Information_En. Available online: https://www.ema.europa.eu/en/documents/product-information/opdivo-epar-product-information_en.pdf (accessed on 15 September 2022).
- Ai, L.; Gao, J.; Zhao, S.; Li, Q.; Cui, Y.-H.; Liu, Q.; Wu, D.; Wang, Y.; Jin, X.; Ji, Y.; et al. Nivolumab-associated DRESS in a genetic susceptible individual. J. Immunother. Cancer 2021, 9, e002879. [Google Scholar] [CrossRef]
- Rombouts, M.D.; Swart, E.L.; VAN DEN Eertwegh, A.J.M.; Crul, M. Systematic Review on Infusion Reactions to and Infusion Rate of Monoclonal Antibodies Used in Cancer Treatment. Anticancer Res. 2020, 40, 1201–1218. [Google Scholar] [CrossRef]
- Bohm, R.; Proksch, E.; Schwarz, T.; Cascorbi, I. Drug Hypersensitivity. Dtsch Arztebl Int. 2018, 115, 501–512. [Google Scholar]
- Miller, R.L.; Shtessel, M.; Robinson, L.B.; Banerji, A. Advances in drug allergy, urticaria, angioedema, and anaphylaxis in 2018. J. Allergy Clin. Immunol. 2019, 144, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, C.M.; Botto, N. The Role of Patch Testing in Evaluating Delayed Hypersensitivity Reactions to Medications. Clin. Rev. Allergy Immunol. 2022, 62, 548–561. [Google Scholar] [CrossRef] [PubMed]
- Hammond, S.; Olsson-Brown, A.; Grice, S.; Naisbitt, D.J. Does immune checkpoint inhibitor therapy increase the frequency of adverse reactions to concomitant medications? Clin. Exp. Allergy 2022, 52, 600–603. [Google Scholar] [CrossRef] [PubMed]
- CTCAE. CTCfAE. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 15 September 2022).
- Choi, B.; McBride, A.; Scott, A.J. Treatment with pembrolizumab after hypersensitivity reaction to nivolumab in a patient with hepatocellular carcinoma. Am. J. Health Syst. Pharm. 2019, 76, 1749–1752. [Google Scholar] [CrossRef] [PubMed]
- Basu, P.; Tong, Y.; Hinds, B.R.; Schneider, J.A. Nivolumab-induced toxic epidermal necrolysis with retiform purpura. Br. J. Dermatol. 2020, 183, e32. [Google Scholar] [CrossRef] [PubMed]
- Dasanu, C.A. Late-onset Stevens-Johnson syndrome due to nivolumab use for hepatocellular carcinoma. J. Oncol. Pharm. Pract. 2019, 25, 2052–2055. [Google Scholar] [CrossRef]
- Gracia-Cazaña, T.; Padgett, E.; Calderero, V.; Oncins, R. Nivolumab-associated Stevens-Johnson syndrome in a patient with lung cancer. Dermatol. Online J. 2021, 27, 13. [Google Scholar] [CrossRef]
- Takeda, Y.; Kubota, T.; Choda, Y.; Toi, Y.; Ichimura, K.; Ishida, M.; Yano, T.; Sato, D.; Yoshimitsu, M.; Nakano, K.; et al. [Two Cases of Stevens-Johnson Syndrome after Nivolumab Therapy for Gastric Cancer]. Gan Kagaku Ryoho. 2021, 48, 154–156. [Google Scholar]
- Salati, M.; Pifferi, M.; Baldessari, C.; Bertolini, F.; Tomasello, C.; Cascinu, S.; Barbieri, F. Stevens–Johnson syndrome during nivolumab treatment of NSCLC. Ann. Oncol. 2018, 29, 283–284. [Google Scholar] [CrossRef]
- Sanchez Togneri, L.; Duran, I.; Rodriguez Fernandez, F.; de Las Vecillas, L. Refractory cytokine release reaction to Nivolumab: Following desensitization algorithms to optimize the management of drug hypersensitivity. J. Oncol. Pharm. Pract. 2022, 28, 736–739. [Google Scholar] [CrossRef]
- Lin, Y.T.; Yang, J.C.; Chu, C.Y. Esomeprazole-induced Stevens-Johnson syndrome in a patient who underwent nivolumab therapy for advanced lung adenocarcinoma. Lung Cancer 2020, 148, 177–178. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.M.; Rancour, E.A.; Al-Omari, A.; Rahnama-Moghadam, S. Striking enhancement at the site of radiation for nivolumab-induced Stevens-Johnson syndrome. Derm. Online J. 2018, 24, 7. [Google Scholar] [CrossRef]
- Watanabe, Y.; Yamaguchi, Y.; Takamura, N.; Takahashi, Y.; Aihara, M. Toxic epidermal necrolysis accompanied by several immune-related adverse events developed after discontinuation of nivolumab. Eur. J. Cancer 2020, 131, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Vivar, K.L.; Deschaine, M.; Messina, J.; Divine, J.M.; Rabionet, A.; Patel, N.; Harrington, M.A.; Seminario-Vidal, L. Epidermal programmed cell death-ligand 1 expression in TEN associated with nivolumab therapy. J. Cutan. Pathol. 2017, 44, 381–384. [Google Scholar] [CrossRef]
- Nayar, N.; Briscoe, K.; Fernandez Penas, P. Toxic Epidermal Necrolysis-like Reaction with Severe Satellite Cell Necrosis Associated with Nivolumab in a Patient with Ipilimumab Refractory Metastatic Melanoma. J. Immunother. 2016, 39, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Kumada, N.; Ito, H.; Teramoto, S.; Nagai, S.; Kubota, Y. [Metastatic Renal Cancer with Stevens-Johnson Syndrome after Nivolumab Treatment: A Case Report]. Hinyokika Kiyo. 2022, 68, 185–190. [Google Scholar]
- Maximova, N.; Maestro, A.; Zanon, D.; Marcuzzi, A. Rapid recovery of postnivolumab vemurafenib-induced Drug Rash with Eosinophilia and Systemic Symptoms (DRESS) syndrome after tocilizumab and infliximab administration. J. Immunother. Cancer. 2019, 8, e000388. [Google Scholar] [CrossRef]
- Kumari, S.; Yun, J.; Soares, J.R.; Ding, P.N. Severe infusion reaction due to nivolumab: A case report. Cancer Rep. 2020, 3, e1246. [Google Scholar] [CrossRef]
- Ramirez-Cruz, S.; Lucena-Campillo, M.A.; Vila-Albelda, C.; Garrido-Arevalo, M.; De Agustin-Sierra, L.; Garcia-Diaz, B. Desensitization protocol to nivolumab without corticosteroid use in a kidney cancer patient. Farm. Hosp. 2020, 44, 182–183. [Google Scholar]
- Ito, J.; Fujimoto, D.; Nakamura, A.; Nagano, T.; Uehara, K.; Imai, Y.; Tomii, K. Aprepitant for refractory nivolumab-induced pruritus. Lung Cancer 2017, 109, 58–61. [Google Scholar] [CrossRef]
- Hasan Ali, O.; Diem, S.; Markert, E.; Jochum, W.; Kerl, K.; French, L.E.; Speiser, D.E.; Früh, M.; Flatz, L. Characterization of nivolumab-associated skin reactions in patients with metastatic non-small cell lung cancer. Oncoimmunology 2016, 5, e1231292. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Yu, H.S.; Yu, S. Cutaneous Adverse Events Associated with Immune Checkpoint Inhibitors: A Review Article. Curr. Oncol. 2022, 29, 2871–2886. [Google Scholar] [CrossRef] [PubMed]
- Kartolo, A.; Sattar, J.; Sahai, V.; Baetz, T.; Lakoff, J.M. Predictors of Immunotherapy-Induced Immune-Related Adverse Events. Curr. Oncol. 2018, 25, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Myers, G. Immune-Related Adverse Events of Immune Checkpoint Inhibitors: A Brief Review. Curr. Oncol. 2018, 25, 342–347. [Google Scholar] [CrossRef]
- Belum, V.; Benhuri, B.; Postow, M.; Hellmann, M.; Lesokhin, A.; Segal, N.; Motzer, R.; Wu, S.; Busam, K.; Wolchok, J.; et al. Characterisation and management of dermatologic adverse events to agents targeting the PD-1 receptor. Eur. J. Cancer 2016, 60, 12–25. [Google Scholar] [CrossRef]
- Teimouri, A.; Minard, L.V.; Scott, S.N.; Daniels, A.; Snow, S. Real-World Adherence to Toxicity Management Guidelines for Immune-Related Adverse Events. Curr. Oncol. 2022, 29, 3104–3117. [Google Scholar] [CrossRef]
- Frantz, R.; Huang, S.; Are, A.; Motaparthi, K. Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis: A Review of Diagnosis and Management. Medicina 2021, 57, 895. [Google Scholar] [CrossRef]
- Charlton, O.A.; Harris, V.; Phan, K.; Mewton, E.; Jackson, C.; Cooper, A. Toxic Epidermal Necrolysis and Steven-Johnson Syndrome: A Comprehensive Review. Adv. Wound Care 2020, 9, 426–439. [Google Scholar] [CrossRef]
- Lu, Y.; Yuan, X.; Wang, M.; He, Z.; Li, H.; Wang, J.; Li, Q. Gut microbiota influence immunotherapy responses: Mechanisms and therapeutic strategies. J. Hematol. Oncol. 2022, 15, 47. [Google Scholar] [CrossRef]
- Wan, X.; Song, M.; Wang, A.; Zhao, Y.; Wei, Z.; Lu, Y. Microbiome Crosstalk in Immunotherapy and Antiangiogenesis Therapy. Front. Immunol. 2021, 12, 747914. [Google Scholar] [CrossRef]
- Pierrard, J.; Seront, E. Impact of the gut microbiome on immune checkpoint inhibitor efficacy-a systematic review. Curr. Oncol. 2019, 26, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Deng, Y.; Chu, Q.; Zhang, P. Gut microbiome and cancer immunotherapy. Cancer Lett. 2019, 447, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Dragomirescu, C.C.; Lixandru, B.E.; Coldea, I.L.; Palade, A.M.; Baltoiu, M.; Dinu, S.; Cristea, V.C.; Manolescu, L.; Popa, M.I. Comparative analysis of different phenotypic and molecular methods used for the taxonomic identification of Corynebacterium spp. isolated from clinical samples in Romania. Rom. Biotechnol. Lett. 2017, 22, 12926–12933. [Google Scholar]
- Haratani, K.; Hayashi, H.; Chiba, Y.; Kudo, K.; Yonesaka, K.; Kato, R.; Kaneda, H.; Hasegawa, Y.; Tanaka, K.; Takeda, M.; et al. Association of Immune-Related Adverse Events with Nivolumab Efficacy in Non–Small-Cell Lung Cancer. JAMA Oncol. 2018, 4, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Grangeon, M.; Tomasini, P.; Chaleat, S.; Jeanson, A.; Souquet-Bressand, M.; Khobta, N.; Bermudez, J.; Trigui, Y.; Greillier, L.; Blanchon, M.; et al. Association Between Immune-related Adverse Events and Efficacy of Immune Checkpoint Inhibitors in Non-small-cell Lung Cancer. Clin. Lung Cancer 2019, 20, 201–207. [Google Scholar] [CrossRef]
- Hussaini, S.; Chehade, R.; Boldt, R.G.; Raphael, J.; Blanchette, P.; Maleki Vareki, S.; Fernandes, R. Association between immune-related side effects and efficacy and benefit of immune checkpoint inhibitors—A systematic review and meta-analysis. Cancer Treat Rev. 2021, 92, 102134. [Google Scholar] [CrossRef]
- Indini, A.; Di Guardo, L.; Cimminiello, C.; Prisciandaro, M.; Randon, G.; De Braud, F.; Del Vecchio, M. Immune-related adverse events correlate with improved survival in patients undergoing anti-PD1 immunotherapy for metastatic melanoma. J. Cancer Res. Clin. Oncol. 2019, 145, 511–521. [Google Scholar] [CrossRef]
- Eggermont, A.M.M.; Kicinski, M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.; Dalle, S.; Haydon, A.; Khattak, A.; Carlino, M.S.; et al. Association Between Immune-Related Adverse Events and Recurrence-Free Survival among Patients with Stage III Melanoma Randomized to Receive Pembrolizumab or Placebo: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2020, 6, 519–527. [Google Scholar] [CrossRef]
- Ralli, M.; Botticelli, A.; Visconti, I.C.; Angeletti, D.; Fiore, M.; Marchetti, P.; Lambiase, A.; De Vincentiis, M.; Greco, A. Immunotherapy in the Treatment of Metastatic Melanoma: Current Knowledge and Future Directions. J. Immunol. Res. 2020, 2020, 9235638. [Google Scholar] [CrossRef]
- Holstead, R.G.; Kartolo, B.A.; Hopman, W.M.; Baetz, T.D. Impact of the development of immune related adverse events in metastatic melanoma treated with PD-1 inhibitors. Melanoma Res. 2021, 31, 258–263. [Google Scholar] [CrossRef]
- Komatsu-Fujii, T.; Ogawa, M.; Nonoyama, S.; Fukumoto, T.; Tanabe, H. Recurrence of nivolumab-induced Stevens-Johnson syndrome due to tegafur/gimeracil/oteracil (TS-1(R)) after nivolumab discontinuation. Eur. J. Dermatol. 2021, 31, 98–99. [Google Scholar] [CrossRef] [PubMed]
- Arenbergerova, M.; Mrazova, I.; Horazdovsky, J.; Sticova, E.; Fialova, A.; Arenberger, P. Toxic epidermal necrolysis induced by vemurafenib after nivolumab failure. J. Eur. Acad. Dermatol. Venereol. 2017, 31, e253–e254. [Google Scholar] [CrossRef] [PubMed]
- Rouyer, L.; Bursztejn, A.C.; Charbit, L.; Schmutz, J.L.; Moawad, S. Stevens-Johnson syndrome associated with radiation recall dermatitis in a patient treated with nivolumab. Eur. J. Dermatol. 2018, 28, 380–381. [Google Scholar] [CrossRef] [PubMed]
- Kandil, A.O.; Dvorak, T.; Mignano, J.; Wu, J.K.; Zhu, J.J. Multifocal Stevens-Johnson syndrome after concurrent phenytoin and cranial and thoracic radiation treatment, a case report. Radiat. Oncol. 2010, 5, 49. [Google Scholar] [CrossRef]
- Duncan, K.O.; Tigelaar, R.E.; Bolognia, J.L. Stevens-Johnson syndrome limited to multiple sites of radiation therapy in a patient receiving phenobarbital. J. Am. Acad. Dermatol. 1999, 40, 493–496. [Google Scholar] [CrossRef]
- Vern-Gross, T.Z.; Kowal-Vern, A. Erythema multiforme, Stevens Johnson syndrome, and toxic epidermal necrolysis syndrome in patients undergoing radiation therapy: A literature review. Am. J. Clin. Oncol. 2014, 37, 506–513. [Google Scholar] [CrossRef]
- Radu, M.C.; Boeru, C.; Marin, M.; Manolescu, L.S. SARS-CoV-2 Infection in Seven Childbearing Women at the Moment of Delivery, a Romanian Experience. Cureus 2021, 13, e12811. [Google Scholar]
- Manolescu, L.; Temereanca, A.; Diaconu, C.C.; Ruta, S. Correlation between resistance profile and immunosuppression in heavily treated HIV-1 infected Romanian patients. Rom. Biotechnol. Lett. 2011, 16, 6439–6449. [Google Scholar]
- Nita, I.; Nitipir, C.; Toma, S.A.; Limbău, A.M.; Pîrvu, E.; Bădărău, I.A.; Suciu, I.; Suciu, G.; Manolescu, L.S.C. Histological Aspects and Quantitative Assessment of Ki67 as Prognostic Factors in Breast Cancer Patients: Result from a Single-Center, Cross Sectional Study. Medicina 2020, 56, 600. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).