A Prognostic Model Generated from an Apparent Diffusion Coefficient Ratio Reliably Predicts the Outcomes of Oral Tongue Squamous Cell Carcinoma

Abstract
1. Introduction
2. Materials and Methods
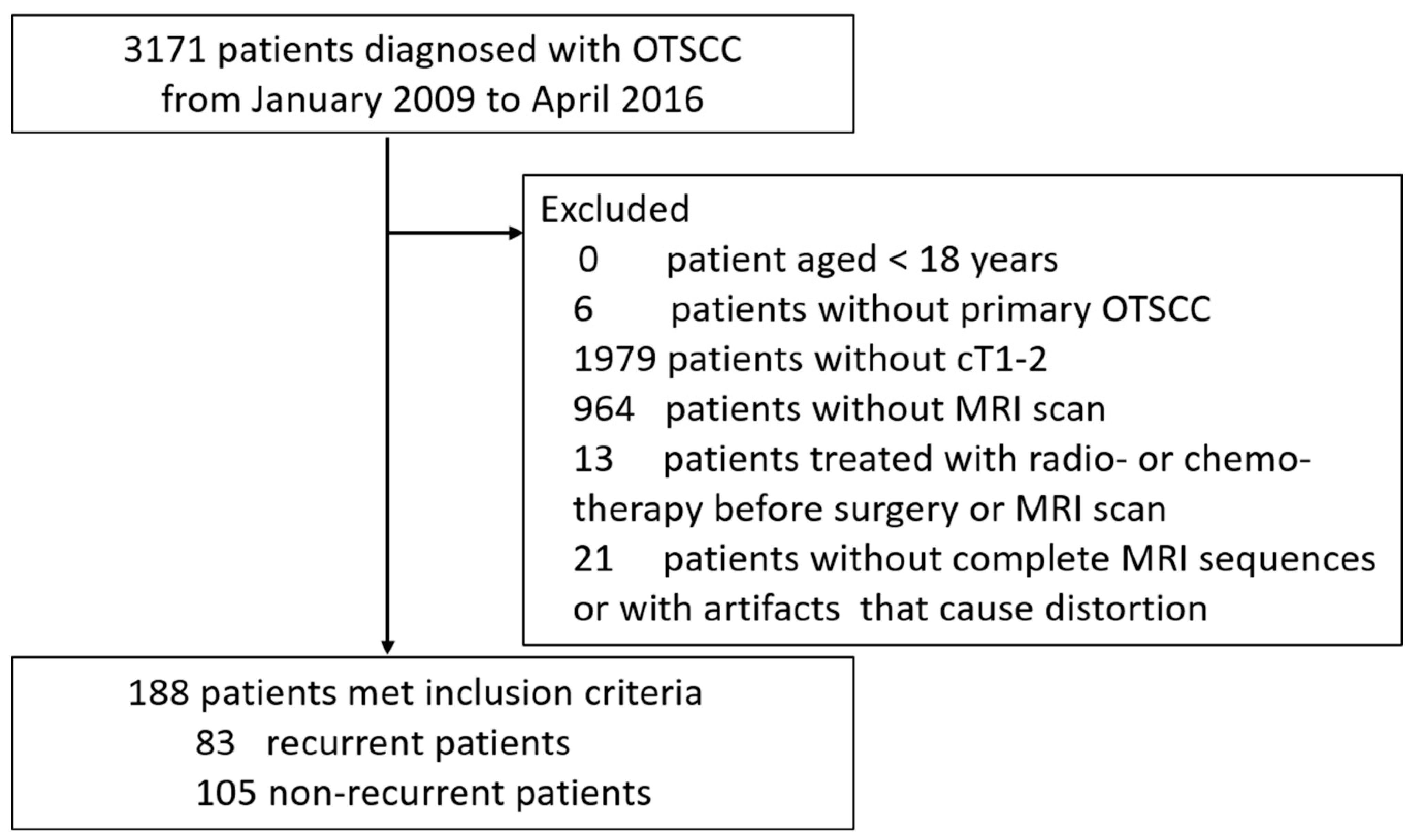
2.1. Study Population and Design
2.2. Inclusion and Exclusion Criteria of Patients
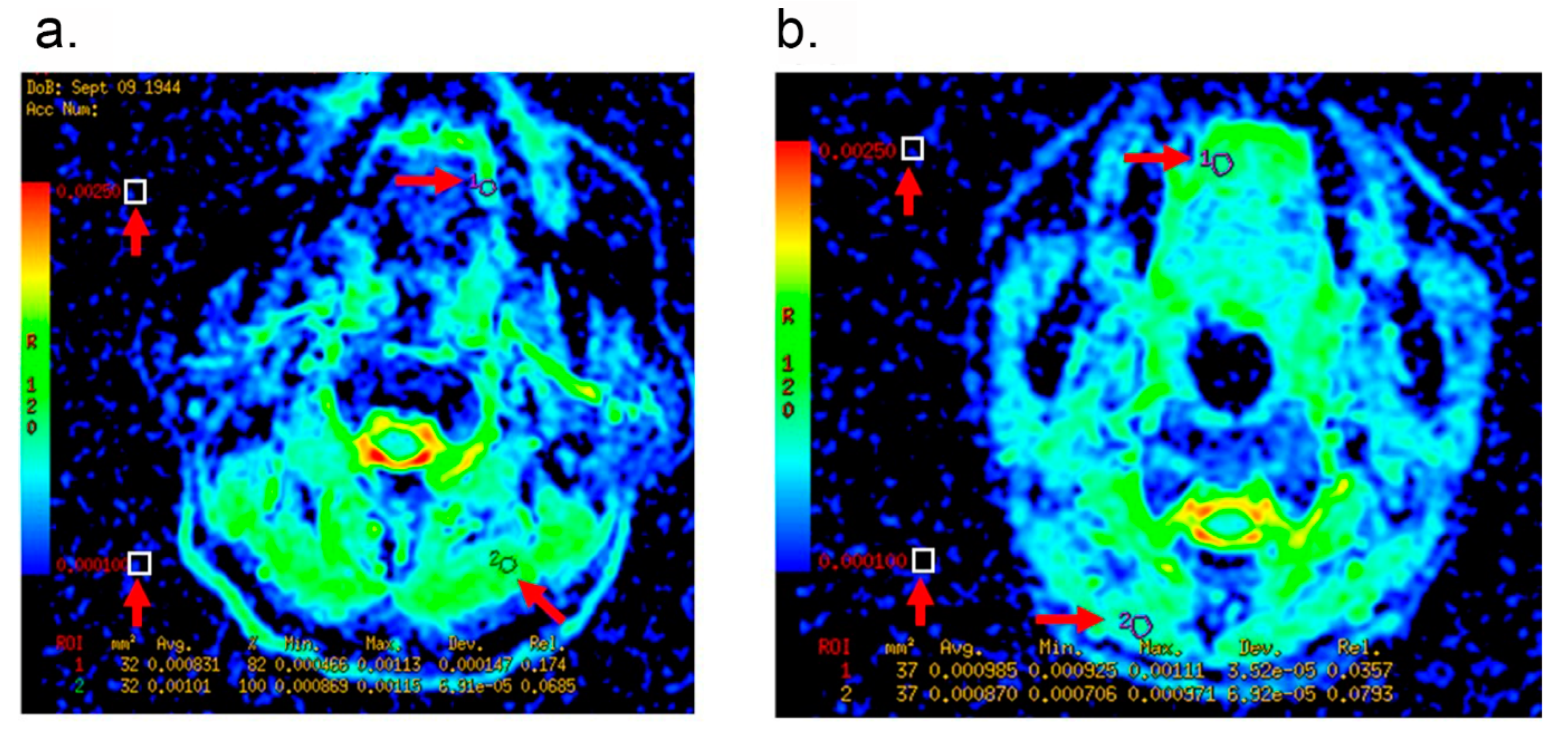
2.3. MR Imaging Verification and Interpretation
2.4. Primary Outcomes and Follow-up
2.5. Candidate Predictors
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics between the Patients with and without Recurrence
3.2. LNR, Tumor Thickness, ADC Value of Tumor and ADC Ratio Are Candidate Predictors for Prognostic Modeling
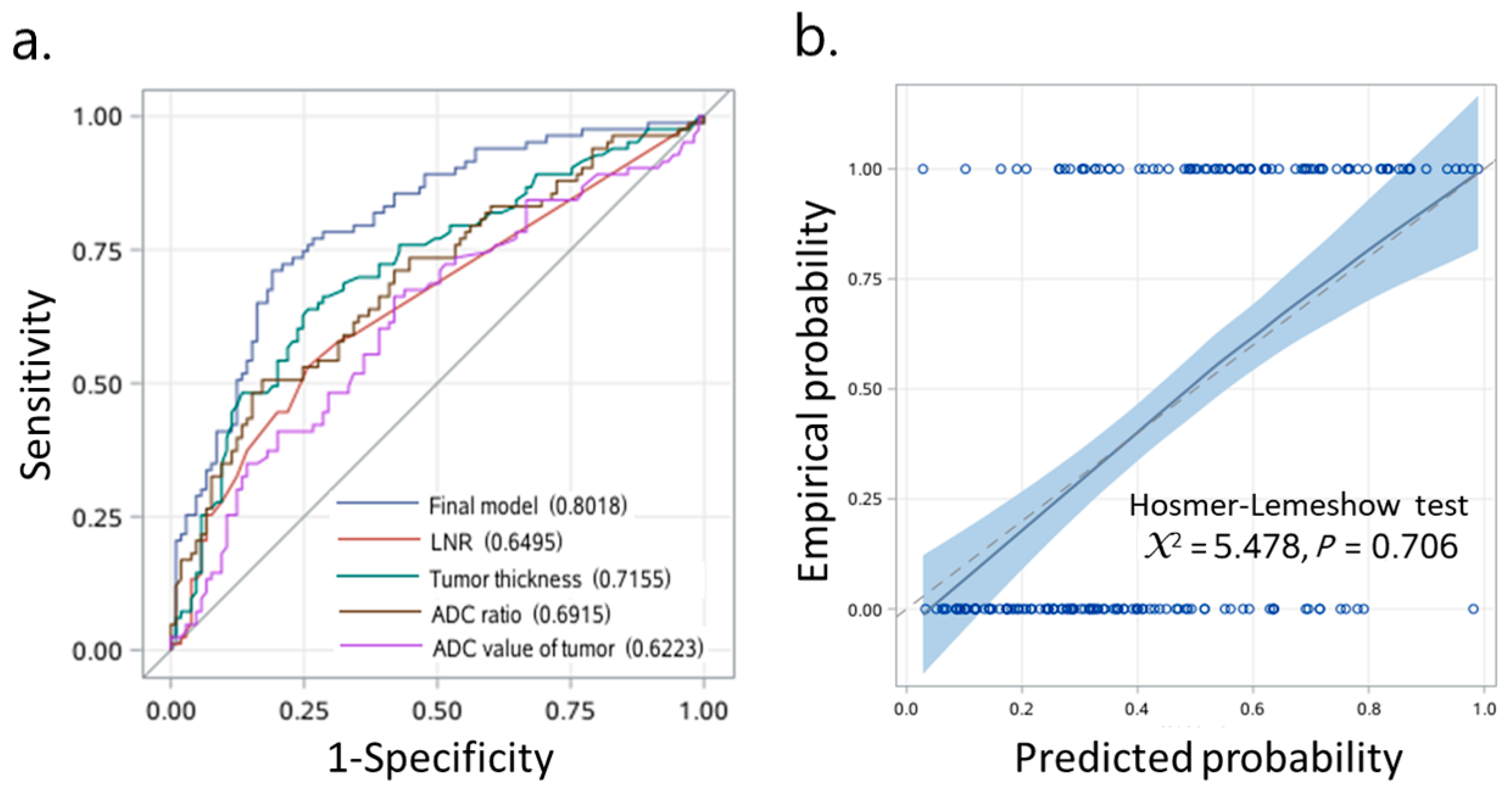
3.3. Prognostic Model Predicts OTSCC with High Sensitivity and Specificity
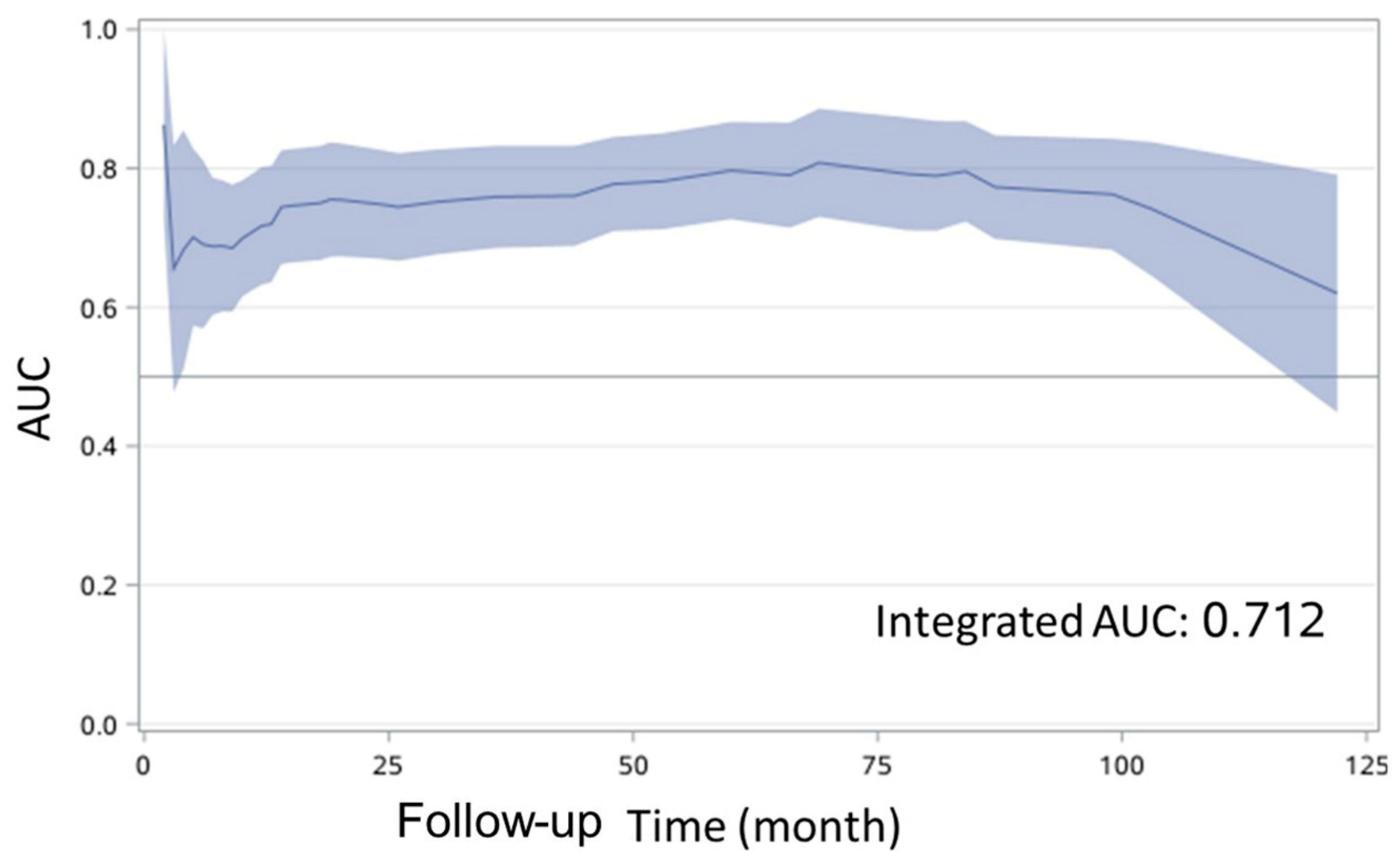
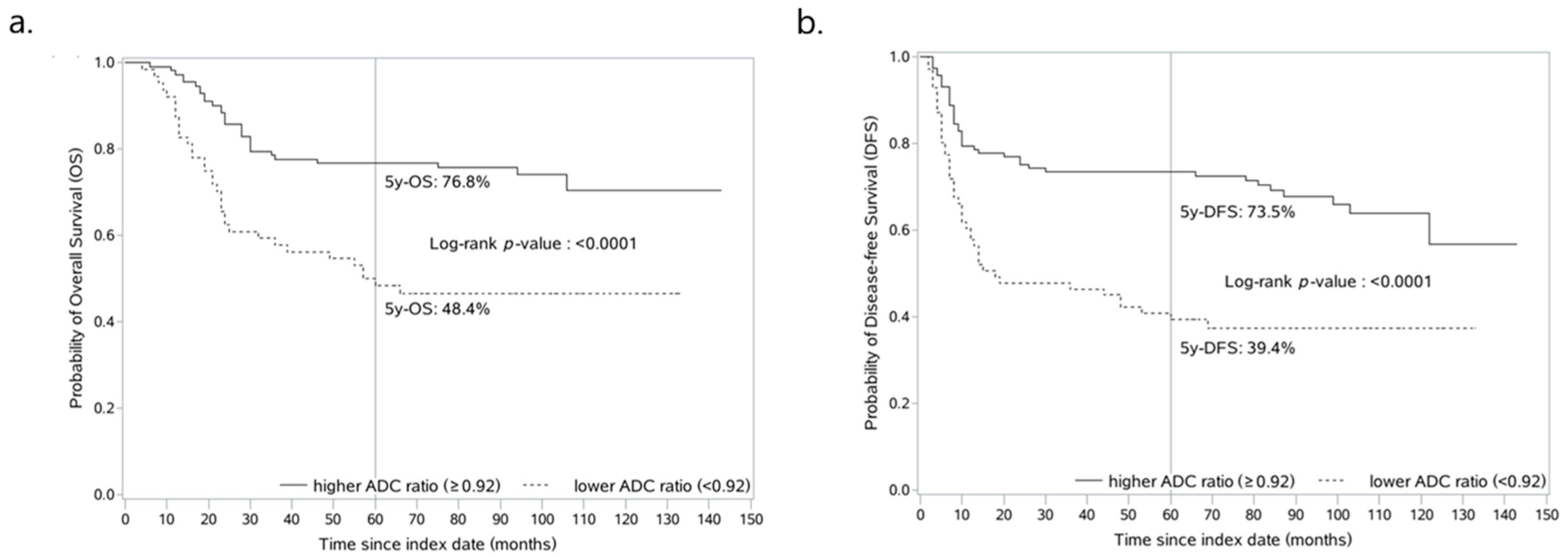
3.4. ADC Ratio-Based Prognostic Model Reliably Predicts OS and DFS of Patients with OTSCC
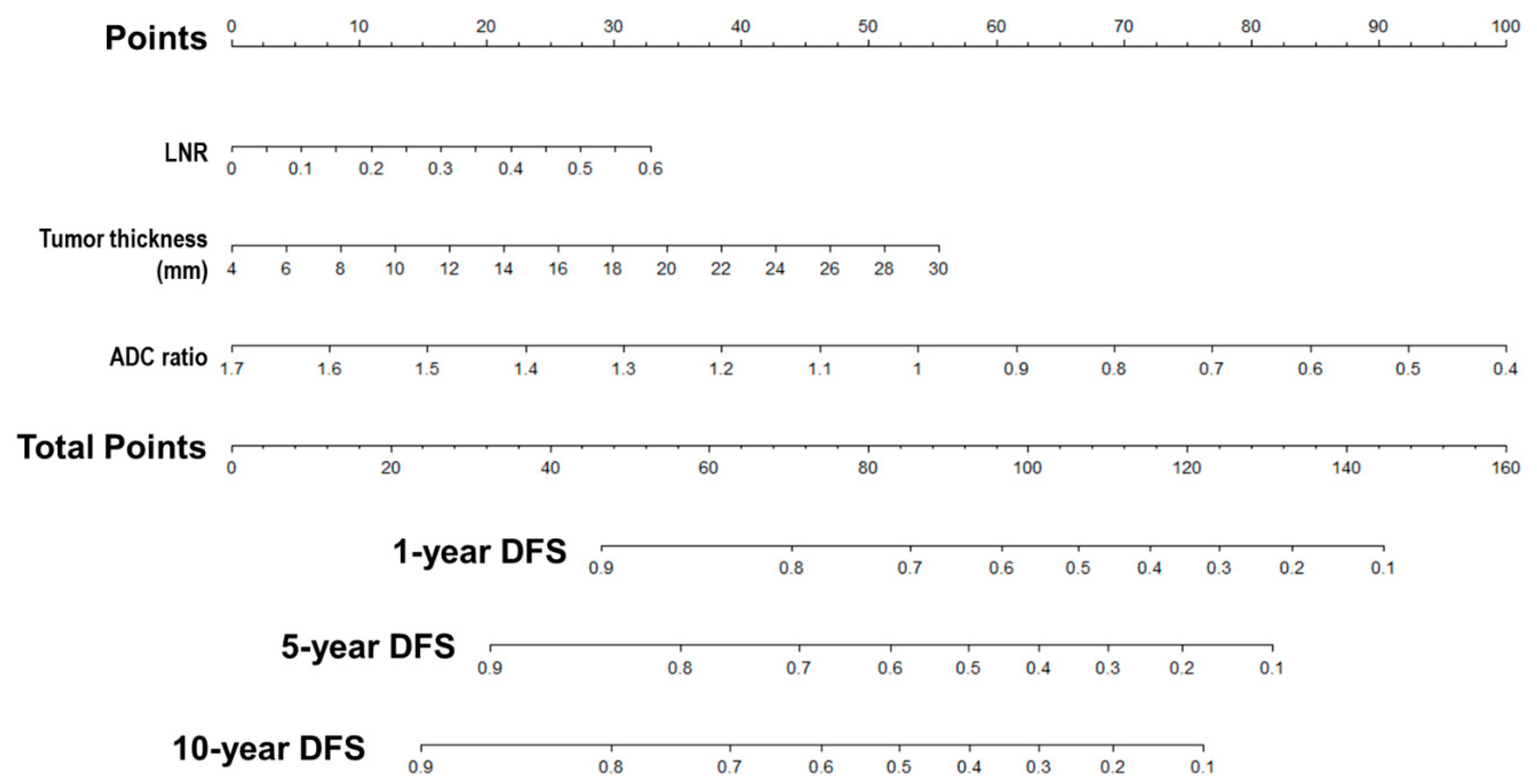
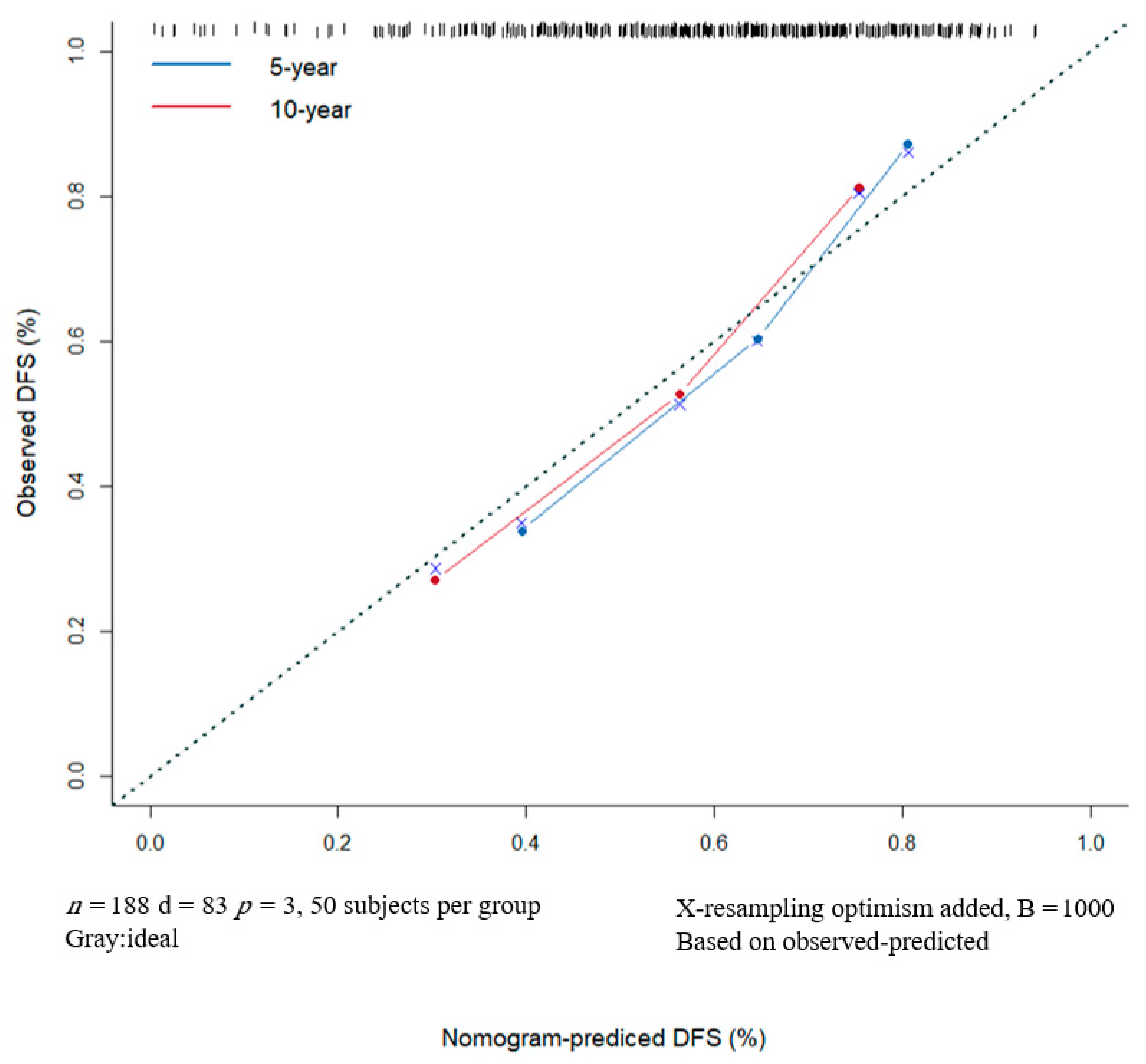
3.5. Nomogram Predicts DFS Reliably and Predictive Accuracy Was Internally Validated
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, L.W.; Li, J.; Cong, X.; Hu, X.S.; Li, D.; Wu, L.L.; Hua, H.; Yu, G.-Y.; Kerr, A.R. Incidence and mortality trends in oral and oropharyngeal cancers in China, 2005–2013. Cancer Epidemiol. 2018, 57, 120–126. [Google Scholar] [CrossRef]
- Almangush, A.; Bello, I.O.; Coletta, R.D.; Makitie, A.A.; Makinen, L.K.; Kauppila, J.H.; Pukkila, M.; Hagström, J.; Laranne, J.; Soini, Y.; et al. For early-stage oral tongue cancer, depth of invasion and worst pattern of invasion are the strongest pathological predictors for locoregional recurrence and mortality. Virchows Arch. 2015, 467, 39–46. [Google Scholar] [CrossRef]
- Rusthoven, K.; Ballonoff, A.; Raben, D.; Chen, C. Poor prognosis in patients with stage I and II oral tongue squamous cell carcinoma. Cancer 2008, 112, 345–351. [Google Scholar] [CrossRef]
- Alabi, R.O.; Elmusrati, M.; Sawazaki-Calone, I.; Kowalski, L.P.; Haglund, C.; Coletta, R.D.; Mäkitie, A.A.; Salo, T.; Leivo, I.; Almangush, A. Machine learning application for prediction of locoregional recurrences in early oral tongue cancer: A Web-based prognostic tool. Virchows Arch 2019, 475, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Law, B.K.; King, A.D.; Bhatia, K.S.; Ahuja, A.T.; Kam, M.K.; Ma, B.B.; Ai, Q.Y.; Mo, F.K.; Yuan, J.; Yeung, D.K. Diffusion-weighted imaging of nasopharyngeal carcinoma: Can pretreatment dwi predict local failure based on long-term outcome? AJNR Am. J. Neuroradiol. 2016, 37, 1706–1712. [Google Scholar] [CrossRef]
- Arya, S.; Rane, P.; Deshmukh, A. Oral cavity squamous cell carcinoma: Role of pretreatment imaging and its influence on management. Clin Radiol. 2014, 69, 916–930. [Google Scholar] [CrossRef]
- Koh, D.M.; Padhani, A.R. Diffusion-weighted MRI: A new functional clinical technique for tumour imaging. Br. J. Radiol. 2006, 79, 633–635. [Google Scholar] [CrossRef]
- Driessen, J.P.; Caldas-Magalhaes, J.; Janssen, L.M.; Pameijer, F.A.; Kooij, N.; Terhaard, C.H.; Grolman, W.; Philippens, M.E. Diffusion-weighted MR imaging in laryngeal and hypopharyngeal carcinoma: Association between apparent diffusion coefficient and histologic findings. Radiology 2014, 272, 456–463. [Google Scholar] [CrossRef]
- Ohnishi, K.; Shioyama, Y.; Hatakenaka, M.; Nakamura, K.; Abe, K.; Yoshiura, T.; Ohga, S.; Nonoshita, T.; Yoshitake, T.; Nakashima, T.; et al. Prediction of local failures with a combination of pretreatment tumor volume and apparent diffusion coefficient in patients treated with definitive radiotherapy for hypopharyngeal or oropharyngeal squamous cell carcinoma. J. Radiat. Res. 2011, 52, 522–530. [Google Scholar] [CrossRef]
- Kim, S.; Loevner, L.; Quon, H.; Sherman, E.; Weinstein, G.; Kilger, A.; Poptani, H. Diffusion-weighted magnetic resonance imaging for predicting and detecting early response to chemoradiation therapy of squamous cell carcinomas of the head and neck. Clin. Cancer Res. 2009, 15, 986–994. [Google Scholar] [CrossRef]
- Lombardi, M.; Cascone, T.; Guenzi, E.; Stecco, A.; Buemi, F.; Krengli, M.; Carriero, A. Predictive value of pre-treatment apparent diffusion coefficient (ADC) in radio-chemiotherapy treated head and neck squamous cell carcinoma. Radiol. Med. 2017, 122, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Hatakenaka, M.; Nakamura, K.; Yabuuchi, H.; Shioyama, Y.; Matsuo, Y.; Ohnishi, K.; Sunami, S.; Kamitani, T.; Setoguchi, T.; Yoshiura, T.; et al. Pretreatment apparent diffusion coefficient of the primary lesion correlates with local failure in head-and-neck cancer treated with chemoradiotherapy or radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 339–345. [Google Scholar] [CrossRef]
- Hatakenaka, M.; Shioyama, Y.; Nakamura, K.; Yabuuchi, H.; Matsuo, Y.; Sunami, S.; Kamitani, T.; Yoshiura, T.; Nakashima, T.; Nishikawa, K.; et al. Apparent diffusion coefficient calculated with relatively high b-values correlates with local failure of head and neck squamous cell carcinoma treated with radiotherapy. AJNR Am. J. Neuroradiol. 2011, 32, 1904–1910. [Google Scholar] [CrossRef]
- Tamada, T.; Prabhu, V.; Li, J.; Babb, J.S.; Taneja, S.S.; Rosenkrantz, A.B. Assessment of prostate cancer aggressiveness using apparent diffusion coefficient values: Impact of patient race and age. Abdom. Radiol. 2017, 42, 1744–1751. [Google Scholar] [CrossRef]
- Woo, S.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. Preoperative evaluation of prostate cancer aggressiveness: Using adc and adc ratio in determining gleason score. AJR Am. J. Roentgenol. 2016, 207, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Siegel, C. Prostate cancer vs. post-biopsy hemorrhage: Diagnosis with T2- and diffusion-weighted imaging. J. Urol. 2011, 185, 1708. [Google Scholar] [CrossRef]
- Harrell, F.E.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Itatani, R.; Namimoto, T.; Yoshimura, A.; Katahira, K.; Noda, S.; Toyonari, N.; Kitani, K.; Hamada, Y.; Kitaoka, M.; Yamashita, Y. Clinical utility of the normalized apparent diffusion coefficient for preoperative evaluation of the aggressiveness of prostate cancer. Jpn. J. Radiol. 2014, 32, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Boesen, L.; Chabanova, E.; Logager, V.; Balslev, I.; Thomsen, H.S. Apparent diffusion coefficient ratio correlates significantly with prostate cancer gleason score at final pathology. J. Magn. Reson. Imaging 2015, 42, 446–453. [Google Scholar] [CrossRef]
- Mourad, M.A.F.; Higazi, M.M. MRI prognostic factors of tongue cancer: Potential predictors of cervical lymph nodes metastases. Radiol. Oncol. 2019, 53, 49–56. [Google Scholar] [CrossRef]
- Peltenburg, B.; Driessen, J.P.; Vasmel, J.E.; Pameijer, F.A.; Janssen, L.M.; Terhaard, C.H.J.; de Bree, R.; Philippens, M.E.P. Pretreatment ADC is not a prognostic factor for local recurrences in head and neck squamous cell carcinoma when clinical T-stage is known. Eur. Radiol. 2020, 30, 1228–1231. [Google Scholar] [CrossRef]
- Sistonen, H.J.; Aro, K.; Atula, T.; Jouhi, L.; Linden, R.; Tapiovaara, L.; Loimu, V.; Markkola, A. Prognostic Value of Apparent Diffusion Coefficient in Oropharyngeal Carcinoma. Clin. Neuroradiol. 2021, 31, 1037–1048. [Google Scholar] [CrossRef]
- Ren, J.L.; Yuan, Y.; Li, X.X.; Shi, Y.Q.; Tao, X.F. Histogram analysis of apparent diffusion coefficient maps in the prognosis of patients with locally advanced head and neck squamous cell carcinoma: Comparison of different region of interest selection methods. Eur. J. Radiol. 2018, 106, 7–13. [Google Scholar] [CrossRef]
- Khattab, H.M.; Montasser, M.M.; Eid, M.; Kandil, A.; Desouky, S.E.-D. Diffusion-weighted magnetic resonance imaging (DWMRI) of head and neck squamous cell carcinoma: Could it be an imaging biomarker for prediction of response to chemoradiation therapy. Egypt. J. Radiol. Nucl. Med. 2020, 51, 204. [Google Scholar] [CrossRef]
- Chung, S.R.; Choi, Y.J.; Suh, C.H.; Lee, J.H.; Baek, J.H. Diffusion-weighted magnetic resonance imaging for predicting response to chemoradiation therapy for head and neck squamous cell carcinoma: A systematic review. Korean J. Radiol. 2019, 20, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Braithwaite, A.C.; Dale, B.M.; Boll, D.T.; Merkle, E.M. Short- and midterm reproducibility of apparent diffusion coefficient measurements at 3.0-T diffusion-weighted imaging of the abdomen. Radiology 2009, 250, 459–465. [Google Scholar] [CrossRef]
- Sasaki, M.; Yamada, K.; Watanabe, Y.; Matsui, M.; Ida, M.; Fujiwara, S.; Shibata, E. Variability in absolute apparent diffusion coefficient values across different platforms may be substantial: A multivendor, multi-institutional comparison study. Radiology 2008, 249, 624–630. [Google Scholar] [CrossRef]
- Litjens, G.J.; Hambrock, T.; Hulsbergen-van de Kaa, C.; Barentsz, J.O.; Huisman, H.J. Interpatient variation in normal peripheral zone apparent diffusion coefficient: Effect on the prediction of prostate cancer aggressiveness. Radiology 2012, 265, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Murakami, R.; Shiraishi, S.; Yoshida, R.; Sakata, J.; Yamana, K.; Hirosue, A.; Uchiyama, Y.; Nakayama, H.; Yamashita, Y. Reliability of MRI-derived depth of invasion of oral tongue cancer. Acad. Radiol. 2019, 26, e180–e186. [Google Scholar] [CrossRef] [PubMed]
- Mao, M.H.; Wang, S.; Feng, Z.E.; Li, J.Z.; Li, H.; Qin, L.Z.; Han, Z.-X. Accuracy of magnetic resonance imaging in evaluating the depth of invasion of tongue cancer. A prospective cohort study. Oral Oncol. 2019, 91, 79–84. [Google Scholar] [CrossRef]
- Chen, S.L.; Iddings, D.M.; Scheri, R.P.; Bilchik, A.J. Lymphatic mapping and sentinel node analysis: Current concepts and applications. CA Cancer J. Clin. 2006, 56, 292–309. [Google Scholar] [CrossRef]
- Nseir, S.; Zeineh, N.; Capucha, T.; Israel, Y.; Emodi, O.; Abu El-Naaj, I.; Rachmiel, A. The impact of lymph node density as a predictive factor for survival and recurrence of tongue squamous cell carcinoma. Int. J. Oral Maxillofac. Surg. 2021, 51, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.; Yan, W.; Liang, J.; Yu, M.; Liu, J.; Hao, J.; Wan, Q.; Liu, J.; Luo, C.; Chen, Y. Nomogram based on systemic immune-inflammation index to predict survival of tongue cancer patients who underwent cervical dissection. Front. Oncol. 2020, 10, 341. [Google Scholar] [CrossRef] [PubMed]
- Lieng, H.; Gebski, V.J.; Morgan, G.J.; Veness, M.J. Important prognostic significance of lymph node density in patients with node positive oral tongue cancer. ANZ J. Surg. 2016, 86, 681–686. [Google Scholar] [CrossRef]
- Son, H.J.; Roh, J.L.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Nodal factors predictive of recurrence and survival in patients with oral cavity squamous cell carcinoma. Clin. Otolaryngol. 2018, 43, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Safi, A.F.; Grandoch, A.; Nickenig, H.J.; Zoller, J.E.; Kreppel, M. The importance of lymph node ratio for locoregional recurrence of squamous cell carcinoma of the tongue. J. Craniomaxillofac. Surg. 2017, 45, 1058–1061. [Google Scholar] [CrossRef] [PubMed]
- Ong, W.; Zhao, R.; Lui, B.; Tan, W.; Ebrahimi, A.; Clark, J.R.; Soo, K.-C.; Tan, N.-C.; Tan, H.-K.; Iyer, N.G. Prognostic significance of lymph node density in squamous cell carcinoma of the tongue. Head Neck 2016, 38 (Suppl. 1), E859–E866. [Google Scholar] [CrossRef]
- Li, Y.; Jia, H.; Yu, W.; Xu, Y.; Li, X.; Li, Q.; Cai, S. Nomograms for predicting prognostic value of inflammatory biomarkers in colorectal cancer patients after radical resection. Int. J. Cancer 2016, 139, 220–231. [Google Scholar] [CrossRef]
- Guthrie, G.J.; Charles, K.A.; Roxburgh, C.S.; Horgan, P.G.; McMillan, D.C.; Clarke, S.J. The systemic inflammation-based neutrophil-lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol. Hematol. 2013, 88, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Kattan, M.W. Nomograms are superior to staging and risk grouping systems for identifying high-risk patients: Preoperative application in prostate cancer. Curr. Opin. Urol. 2003, 13, 111–116. [Google Scholar] [CrossRef]
- Balasubramanian, D.; Subramaniam, N.; Missale, F.; Marchi, F.; Dokhe, Y.; Vijayan, S.; Nambiar, A.; Mattavelli, D.; Calza, S.; Bresciani, L.; et al. Predictive nomograms for oral tongue squamous cell carcinoma applying the American Joint Committee on Cancer/Union Internationale Contre le Cancer 8th edition staging system. Head Neck 2021, 43, 1043–1055. [Google Scholar] [CrossRef] [PubMed]
- Mascitti, M.; Zhurakivska, K.; Togni, L.; Caponio, V.C.A.; Almangush, A.; Balercia, P.; Balercia, A.; Rubini, C.; Muzio, L.L.; Santarelli, A.; et al. Addition of the tumour-stroma ratio to the 8th edition American Joint Committee on Cancer staging system improves survival prediction for patients with oral tongue squamous cell carcinoma. Histopathology 2020, 77, 810–822. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Without Recurrence (n = 105) | With Recurrence (n = 83) | p-Value |
|---|---|---|---|
| Age, years Male sex | 51.01 ± 12.11 63 (60.00%) | 54.05 ± 13.21 56 (67.47%) | 0.102 0.291 |
| Smoking | 31 (29.52%) | 34 (40.96%) | 0.101 |
| Alcohol drinking | 23 (21.90%) | 24 (28.92%) | 0.270 |
| Lymph node-positive | 36 (34.29%) | 49 (59.04%) | 0.001 |
| Lymph node ratio (LNR) | 0 (0.04) | 0.04 (0.12) | <0.001 |
| Tumor thickness, mm | 10.40 (4.60) | 14.30 (7.60) | <0.001 |
| ADC value of tumor, ×10−3 mm2/s | 0.98 ± 0.21 | 0.90 ± 0.23 | 0.011 |
| ADC values of normal tissue, ×10−3 mm2/s | 0.96 (0.41) | 1.01 (0.40) | 0.107 |
| ADC ratio | 1.03 ± 0.21 | 0.88 ± 0.23 | <0.001 |
| Preoperative pain | 80 (76.19%) | 70 (84.34%) | 0.167 |
| Preoperative anemia | 0.193 | ||
| No | 100 (95.24%) | 74 (89.16%) | |
| Mild | 5 (4.76%) | 8 (9.64%) | |
| Moderate | 0 | 1 (1.20%) | |
| Postoperative anemia | 0.198 | ||
| No | 66 (62.86%) | 43 (51.81%) | |
| Mild | 38 (36.19%) | 37 (44.58%) | |
| Moderate | 1 (0.95%) | 3 (3.61%) | |
| Midline crossing | 13 (12.38%) | 20 (24.10%) | 0.036 |
| Time intensity curve (TIC) shape | 0.414 | ||
| Type I | 15 (14.29%) | 14 (16.87%) | |
| Type II | 85 (80.95%) | 68 (81.93%) | |
| Type III | 5 (4.76%) | 1 (1.20%) | |
| Preoperative T status | 0.313 | ||
| cT1 | 39 (37.14%) | 25 (30.12%) | |
| cT2 | 66 (62.86%) | 58 (69.88%) | |
| Histologic grade | 0.182 | ||
| I | 14 (13.33%) | 5 (6.02%) | |
| I-II | 57 (54.29%) | 38 (45.78%) | |
| II | 29 (27.62%) | 33 (39.76%) | |
| II-III | 4 (3.81%) | 6 (7.23%) | |
| III | 1 (0.95%) | 1 (1.20%) | |
| Treatment characteristics | |||
| Type of surgery | 0.053 | ||
| Supra-omohyoid | 69 (65.71%) | 40 (48.19%) | |
| Functional | 30 (28.57%) | 35 (42.17%) | |
| Radical | 6 (5.71%) | 8 (9.64%) | |
| Postoperative adjuvant treatment | 0.350 | ||
| No Radiotherapy (RT) | 37 (35.24%) 44 (41.90%) | 20 (24.10%) 42 (50.60%) | |
| Chemotherapy Chemotherapy plus RT | 4 (3.81%) 20 (19.05%) | 2 (2.41%) 19 (22.89%) |
| Variables | Crude HR (95% CI) | p-Value | Adjusted HR a (95% CI) | p-Value |
| Age, years | 1.01 (0.99–1.03) | 0.173 | ||
| Male sex | 1.18 (0.75-1.88) | 0.463 | ||
| Smoking | 1.34 (0.86–2.07) | 0.195 | ||
| Alcohol drinking | 1.22 (0.76–1.97) | 0.412 | ||
| Lymph node-positive | 2.03 (1.31–3.15) | 0.001 | ||
| Lymph node ratio (LNR) | 20.44 (3.31–126.43) | 0.001 | 5.57 (0.72–42.79) | 0.099 |
| Tumor thickness, mm | 1.09 (1.05–1.13) | <0.001 | 1.07 (1.03–1.11) | <0.001 |
| ADC value of tumor, ×10−3 mm2/s | 0.30 (0.11–0.79) | 0.015 | ||
| ADC values of normal tissue, ×10−3 mm2/s | 2.45 (1.08–5.53) | 0.032 | ||
| ADC ratio | 0.07 (0.02–0.21) | <0.001 | 0.09 (0.03–0.26) | <0.001 |
| Preoperative pain | 1.49 (0.83–2.71) | 0.182 | ||
| Preoperative anemia | ||||
| Mild (vs. No) | 1.64 (0.78–3.39) | 0.186 | ||
| Moderate (vs. No) | 3.58 (0.49–26.02) | 0.206 | ||
| Postoperative anemia | ||||
| Mild (vs. No) | 1.24 (0.79–1.92) | 0.343 | ||
| Moderate (vs. No) | 3.24 (1.00–10.51) | 0.050 | ||
| Midline crossing | 1.64 (0.99–2.71) | 0.054 | ||
| Time intensity curve (TIC) shape | ||||
| Type II (vs. Type I) | 0.86 (0.48–1.53) | 0.622 | ||
| Type III (vs. Type I) | 0.27 (0.04–2.09) | 0.211 | ||
| Preoperative T status | ||||
| cT2 (vs. cT1) | 1.15 (0.71–1.83) | 0.560 | ||
| Histologic grade | ||||
| I-II (vs. I) | 1.53 (0.60–3.89) | 0.372 | ||
| II (vs. I) | 2.30 (0.89–5.90) | 0.082 | ||
| II-III (vs. I) | 2.53 (0.77–8.28) | 0.126 | ||
| III (vs. I) | 2.94 (0.34–25.15) | 0.325 | ||
| Treatment characteristics | ||||
| Type of surgery | ||||
| Functional (vs. Supra-omohyoid) | 1.60 (1.02–2.52) | 0.042 | ||
| Radical (vs. Supra-omohyoid) | 1.72 (0.80–3.67) | 0.165 | ||
| Postoperative adjuvant treatment Radiotherapy (RT) (vs. No) | 1.38 (0.81–2.35) | 0.232 | ||
| Chemotherapy (vs. No) Chemotherapy plus RT (vs. No) | 0.95 (0.22–4.08) 1.46 (0.78–2.74) | 0.950 0.235 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, L.; Li, X.; Wu, L.; Wang, B.; Si, M.; Tao, X. A Prognostic Model Generated from an Apparent Diffusion Coefficient Ratio Reliably Predicts the Outcomes of Oral Tongue Squamous Cell Carcinoma. Curr. Oncol. 2022, 29, 9031-9045. https://doi.org/10.3390/curroncol29120708
Cai L, Li X, Wu L, Wang B, Si M, Tao X. A Prognostic Model Generated from an Apparent Diffusion Coefficient Ratio Reliably Predicts the Outcomes of Oral Tongue Squamous Cell Carcinoma. Current Oncology. 2022; 29(12):9031-9045. https://doi.org/10.3390/curroncol29120708
Chicago/Turabian StyleCai, Lingling, Xiaoguang Li, Lizhong Wu, Bocheng Wang, Mingjue Si, and Xiaofeng Tao. 2022. "A Prognostic Model Generated from an Apparent Diffusion Coefficient Ratio Reliably Predicts the Outcomes of Oral Tongue Squamous Cell Carcinoma" Current Oncology 29, no. 12: 9031-9045. https://doi.org/10.3390/curroncol29120708
APA StyleCai, L., Li, X., Wu, L., Wang, B., Si, M., & Tao, X. (2022). A Prognostic Model Generated from an Apparent Diffusion Coefficient Ratio Reliably Predicts the Outcomes of Oral Tongue Squamous Cell Carcinoma. Current Oncology, 29(12), 9031-9045. https://doi.org/10.3390/curroncol29120708