Musculoskeletal Chronic Graft versus Host Disease—A Rare Complication to Allogeneic Hematopoietic Stem Cell Transplant: A Case-Based Report and Review of the Literature

 ,
, 
Abstract
1. Introduction
2. Case Report
3. Methods
3.1. Strategy of Search and Data Sources
3.2. Selection Criteria
3.3. Data Extraction
4. Results
4.1. Etiology

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Nr. | Diagnostic | Lab | Symptoms | Treatment | Other Organs | Treat Res | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Age | Hem Dis | AI/Au | Bx | Radio | EMG | CK | Weak | Pain | Joint | Swel | Fever | RoM | GC | CyA | Tacro | IG | Other | MM | Az | MA | Skin | Oral | Eyes | GI | Pulm | Liver | CNS | Joints | Heart | Res | IwD | NR | NCT | Ref. | |
| 1 | F | 33 | AML | Allo | <25 | NA | [6] | |||||||||||||||||||||||||||||
| 2 | F | 46 | NHL | Allo | <25 | NA | [6] | |||||||||||||||||||||||||||||
| 3 | F | 55 | AA | Allo | 727 | NA | [6] | |||||||||||||||||||||||||||||
| 4 | F | 64 | NHL | Allo | 35 | NA | [6] | |||||||||||||||||||||||||||||
| 5 | M | 57 | AML | Allo | <25 | NA | [6] | |||||||||||||||||||||||||||||
| 6 | F | 65 | NHL | Auto | 33 | NA | [6] | |||||||||||||||||||||||||||||
| 7 | M | 58 | MDS | Allo | 5200 | NA | [6] | |||||||||||||||||||||||||||||
| 8 | M | 66 | CLL | Allo | 278 | NA | [6] | |||||||||||||||||||||||||||||
| 9 | M | 61 | AML | Allo | 20 | NA | [6] | |||||||||||||||||||||||||||||
| 10 | M | 32 | AML | Allo | 123 | NA | [6] | |||||||||||||||||||||||||||||
| 11 | M | 58 | MDS | Allo | 84 | NA | [6] | |||||||||||||||||||||||||||||
| 12 | M | 65 | AML | Allo | 2422 | NA | [6] | |||||||||||||||||||||||||||||
| 13 | M | 69 | NHL | Auto | NA | NA | NA | [6] | ||||||||||||||||||||||||||||
| 14 | M | 52 | CLL | Allo | 98 | NA | [6] | |||||||||||||||||||||||||||||
| 15 | M | 34 | CML | Allo | 1027 | [3] | ||||||||||||||||||||||||||||||
| 16 | F | 46 | AML | Allo | NA | [4] | ||||||||||||||||||||||||||||||
| 17 | F | 36 | MM | Allo | 1141 | [7] | ||||||||||||||||||||||||||||||
| 18 | F | 53 | AML | Allo | 1643 | [7] | ||||||||||||||||||||||||||||||
| 19 | M | 50 | AML | Allo | 4072 | [7] | ||||||||||||||||||||||||||||||
| 20 | F | 37 | CML | Allo | 3173 | [7] | ||||||||||||||||||||||||||||||
| 21 | M | 39 | CML | Allo | 4864 | [7] | ||||||||||||||||||||||||||||||
| 22 | M | 21 | ALL | Allo | 3930 | [7] | ||||||||||||||||||||||||||||||
| 23 | M | 23 | AML | Allo | 2882 | [7] | ||||||||||||||||||||||||||||||
| 24 | M | 39 | ALL | Allo | 1790 | [7] | ||||||||||||||||||||||||||||||
| 25 | F | 56 | AML | Allo | NA | [7] | ||||||||||||||||||||||||||||||
| 26 | M | 57 | MM | Allo | 25 | [7] | ||||||||||||||||||||||||||||||
| 27 | M | 34 | AML | Allo | 69 | [7] | ||||||||||||||||||||||||||||||
| 28 | F | 50 | AML | Allo | NA | [7] | ||||||||||||||||||||||||||||||
| 29 | F | 39 | MDS | Allo | 27 | [7] | ||||||||||||||||||||||||||||||
| 30 | F | 39 | CML | Allo | 171 | [7] | ||||||||||||||||||||||||||||||
| 31 | F | 40 | AML | Allo | 64 | [7] | ||||||||||||||||||||||||||||||
| 32 | M | 26 | ALL | Allo | 114 | [7] | ||||||||||||||||||||||||||||||
| 33 | M | 20 | CML | Allo | NA | [7] | ||||||||||||||||||||||||||||||
| 34 | M | 49 | NHL | Allo | 73 | [8] | ||||||||||||||||||||||||||||||
| 35 | M | 4 | AA | Allo | 634 | [9] | ||||||||||||||||||||||||||||||
| 36 | F | 26 | CML | Allo | 2350 | [9] | ||||||||||||||||||||||||||||||
| 37 | F | 36 | CML | Allo | 54 | [9] | ||||||||||||||||||||||||||||||
| 38 | M | 28 | CML | Allo | NA | [9] | ||||||||||||||||||||||||||||||
| 39 | M | 46 | AML | Allo | 454 | [9] | ||||||||||||||||||||||||||||||
| 40 | F | 19 | ALL | Allo | NA | [9] | ||||||||||||||||||||||||||||||
| 41 | F | 8 | AA | Allo | 8400 | [9] | ||||||||||||||||||||||||||||||
| 42 | M | 36 | AA | Allo | 2170 | [9] | ||||||||||||||||||||||||||||||
| 43 | M | 28 | CML | Allo | 49 | [9] | ||||||||||||||||||||||||||||||
| 44 | M | 24 | ALL | Allo | 2490 | [9] | ||||||||||||||||||||||||||||||
| 45 | M | 42 | AML | Allo | 1126 | [9] | ||||||||||||||||||||||||||||||
| 46 | F | 35 | AML | Allo | 81 | [9] | ||||||||||||||||||||||||||||||
| 47 | F | 55 | AML | Allo | NA | [10] | ||||||||||||||||||||||||||||||
| 48 | M | 63 | AML | Allo | 257 | [10] | ||||||||||||||||||||||||||||||
| 49 | M | 66 | MDS | Allo | 251 | [10] | ||||||||||||||||||||||||||||||
| 50 | F | 54 | ALL | Allo | 492 | [10] | ||||||||||||||||||||||||||||||
| 51 | M | 45 | CLL | Allo | 1853 | [10] | ||||||||||||||||||||||||||||||
| 52 | M | 62 | AML | Allo | 2195 | [10] | ||||||||||||||||||||||||||||||
| 53 | M | 29 | AML | Allo | N | [11] | ||||||||||||||||||||||||||||||
| 54 | M | 39 | ALL | Allo | 1220 | [12] | ||||||||||||||||||||||||||||||
| 55 | F | 35 | AML | Allo | 664 | [13] | ||||||||||||||||||||||||||||||
| 56 | M | 47 | CML | Allo | 2808 | [13] | ||||||||||||||||||||||||||||||
| 57 | F | 48 | AML | Allo | 2118 | [14] | ||||||||||||||||||||||||||||||
| 58 | F | 31 | AML | Allo | 18 | [14] | ||||||||||||||||||||||||||||||
| 59 | M | 22 | AML | Allo | 650 | [15] | ||||||||||||||||||||||||||||||
| 60 | M | 51 | MM | Allo | 946 | [16] | ||||||||||||||||||||||||||||||
| 61 | M | 66 | AML | Allo | N | [17] | ||||||||||||||||||||||||||||||
| 62 | M | 63 | MDS | Allo | N | [17] | ||||||||||||||||||||||||||||||
| 63 | M | 33 | ALL | Allo | 4× N | [18] | ||||||||||||||||||||||||||||||
| 64 | F | 18 | AML | Allo | 14420 | [19] | ||||||||||||||||||||||||||||||
| 65 | F | 37 | AML | Allo | 1445 | [20] | ||||||||||||||||||||||||||||||
| 66 | M | 54 | AML | Allo | 358 | [21] | ||||||||||||||||||||||||||||||
| 67 | M | 31 | CML | Allo | NA | [22] | ||||||||||||||||||||||||||||||
| 68 | M | 11 | ALL | Allo | 3950 | [23] | ||||||||||||||||||||||||||||||
| 69 | M | 39 | AML | Allo | 28 | [24] | ||||||||||||||||||||||||||||||
| 70 | F | 39 | CML | Allo | 67 | [24] | ||||||||||||||||||||||||||||||
| 71 | M | 44 | CLL | Allo | 437 | [24] | ||||||||||||||||||||||||||||||
| 72 | F | 65 | AML | Allo | E | [25] | ||||||||||||||||||||||||||||||
| 73 | F | 59 | AML | Allo | E | [25] | ||||||||||||||||||||||||||||||
| 74 | F | 67 | MDS | Allo | E | [25] | ||||||||||||||||||||||||||||||
| 75 | M | 6 | THA | Allo | 4570 | [26] | ||||||||||||||||||||||||||||||
| 76 | M | 57 | NHL | Allo | N | [27] | ||||||||||||||||||||||||||||||
| 77 | M | 36 | MDS | Allo | E | [28] | ||||||||||||||||||||||||||||||
| 78 | M | 52 | AML | Allo | 923 | [29] | ||||||||||||||||||||||||||||||
| 79 | F | 54 | AML | Allo | 1411 | [30] | ||||||||||||||||||||||||||||||
| 80 | M | 67 | AML | Allo | N | [31] | ||||||||||||||||||||||||||||||
| 81 | M | 33 | CML | Allo | 3113 | [32] | ||||||||||||||||||||||||||||||
| 82 | M | 35 | AML | Allo | 3500 | [32] | ||||||||||||||||||||||||||||||
| 83 | M | 19 | CML | Allo | 2943 | [32] | ||||||||||||||||||||||||||||||
| 84 | M | 62 | CML | Allo | 1291 | PRES | ||||||||||||||||||||||||||||||
| 85 | F | 13 | AA | Allo | 1100 | [33] | ||||||||||||||||||||||||||||||
| Number (n) | Percentage (%) | |
|---|---|---|
| Sex | ||
| Male | 53 | 62 |
| Female | 32 | 38 |
| Hematological Diseases | ||
| Acute myelogenous leukemia (AML) | 33 | 39 |
| Chronic myelogenous leukemia (CML) | 15 | 18 |
| Acute lymphocytic leukemia (ALL) | 11 | 13 |
| Myelodysplastic syndrome (MDS) | 7 | 8 |
| Aplastic anemia (AA) | 5 | 6 |
| Non-Hodgkin lymphoma (NHL) | 5 | 6 |
| Chronic lymphocytic lymphoma (CLL) | 4 | 5 |
| Multiple myeloma (MM) | 3 | 4 |
| Mantle cell lymphoma (ML) | 1 | 1 |
| Thalassemia (Thal) | 1 | 1 |

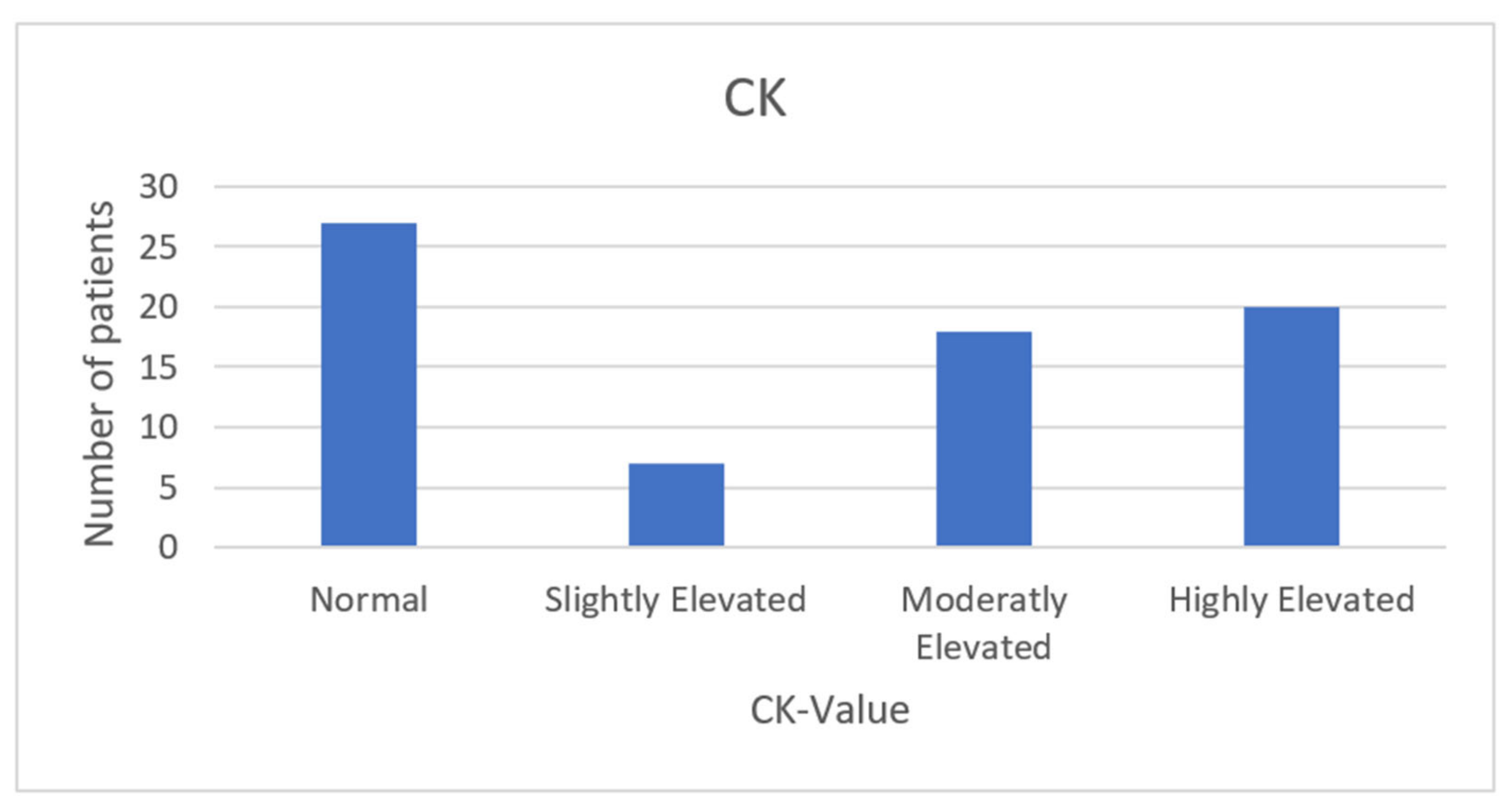
4.2. Symptoms and Clinical Features
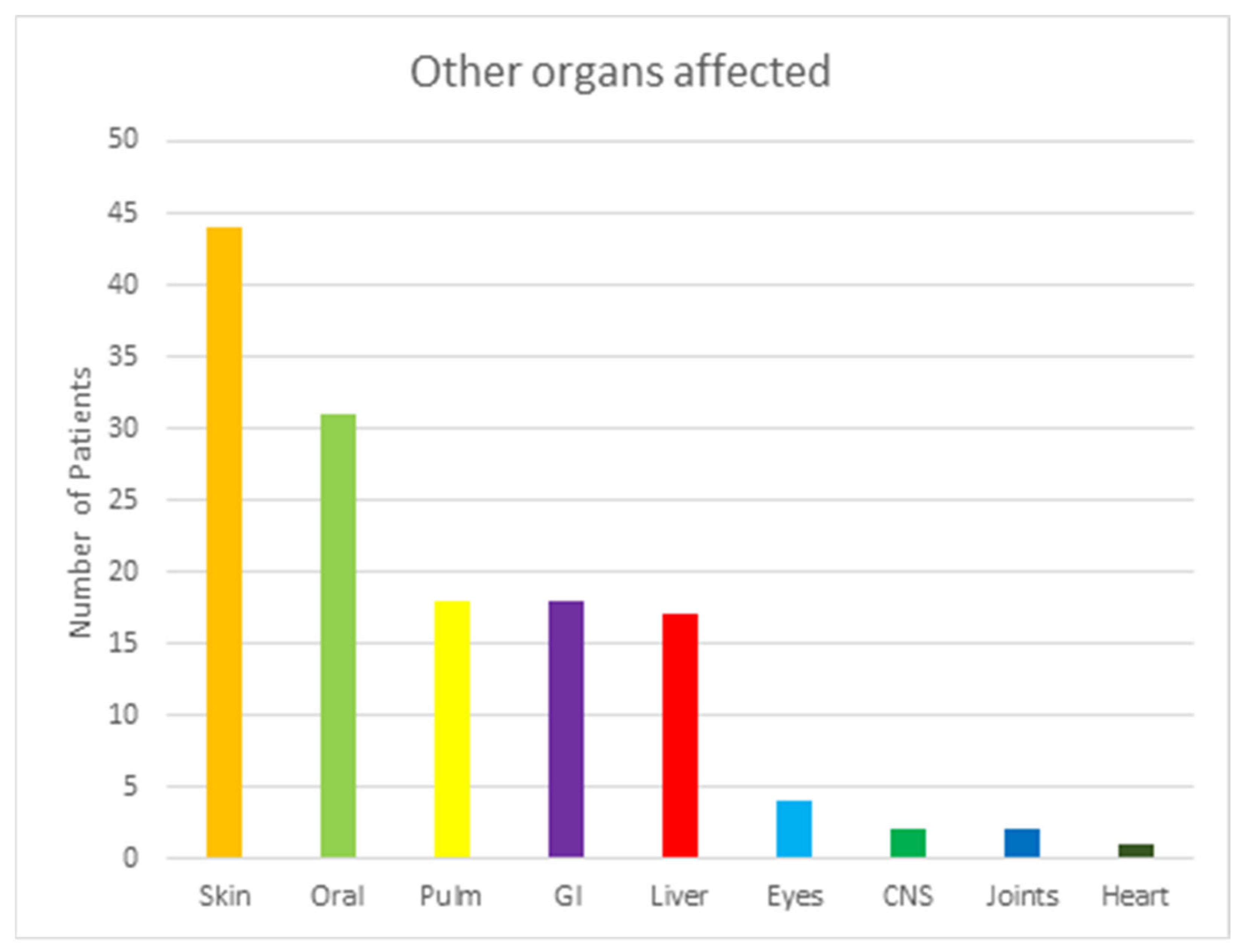
4.3. Affection of Other Organs
4.4. Treatment
4.5. Outcome and Survivability
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ramachandran, V.; Kolli, S.S.; Strowd, L.C. Review of Graft-Versus-Host Disease. Dermatol. Clin. 2019, 37, 569–582. [Google Scholar] [CrossRef]
- Moreno, D.F.; Cid, J. Graft-versus-host disease. Med. Clin. 2019, 152, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Goli, V.B.; Jain, R.; Bhat, G.; Sainani, A.; Advani, S.H. Musculoskeletal chronic graft versus host disease-A rare complication of allogeneic hematopoietic stem cell transplantation: A case report and review of its literature. South Asian J. Cancer 2017, 6, 150. [Google Scholar] [CrossRef] [PubMed]
- Vijaysekharan, K.; Punatar, S.; Bonda, A.; Mohite, A.; Shanmugam, K.; Nayak, L.; Gokarn, A.; Khattry, N. Leflunomide: Is It the Game Changer in Musculoskeletal Chronic Graft Versus Host Disease? Indian J. Hematol. Blood Transfus. 2018, 34, 566–567. [Google Scholar] [CrossRef] [PubMed]
- Blazar, B.R.; Murphy, W.J.; Abedi, M. Advances in graft-versus-host disease biology and therapy. Nat. Rev. Immunol. 2012, 12, 443–458. [Google Scholar] [CrossRef] [PubMed]
- Pestronk, A. Chronic Graft Versus Host Myopathies: Noninflammatory, Multi-Tissue Pathology with Glycosylation Disorders. J. Neuropathol. Exp. Neurol. 2020, 79, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Oda, K.; Nakaseko, C.; Ozawa, S.; Nishimura, M.; Saito, Y.; Yoshiba, F.; Yamashita, T.; Fujita, H.; Takasaki, H.; Kanamori, H.; et al. Fasciitis and myositis: An analysis of muscle-related complications caused by chronic GVHD after allo-SCT. Bone Marrow Transplant. 2009, 43, 159–167. [Google Scholar] [CrossRef]
- Sauter, A.; Bethge, W.; Vogel, U.; Horger, M. Cervical fascial and muscular involvement in chronic GVHD after allo-SCT and radiation therapy. Bone Marrow Transplant. 2009, 44, 451–452. [Google Scholar] [CrossRef]
- Stevens, A.M.; Sullivan, K.M.; Nelson, J.L. Polymyositis as a manifestation of chronic graft-versus-host disease. Rheumatology 2003, 42, 34–39. [Google Scholar] [CrossRef]
- New-Tolley, J.; Smith, C.; Koszyca, B.; Otto, S.; Maundrell, A.; Bardy, P.; Hiwase, D.; Yong, A.S.M.; Lewis, I.; Limaye, V. Inflammatory myopathies after allogeneic stem cell transplantation. Muscle Nerve 2018, 58, 790–795. [Google Scholar] [CrossRef]
- Prussick, R.; Brain, M.C.; Walker, I.R.; Sauder, D.N. Polymyositis: A manifestation of chronic graft-versus-host disease. J. Am. Acad. Dermatol. 1991, 25, 560–562. [Google Scholar] [CrossRef]
- Hanslik, T.; Jaccard, A.; Guillon, J.M.; Vernant, J.P.; Wechsler, B.; Godeau, P. Polymyositis and chronic graft-versus-host disease: Efficacy of intravenous gammaglobulin. J. Am. Acad. Dermatol. 1993, 28, 492–493. [Google Scholar] [CrossRef]
- Couriel, D.R.; Beguelin, G.Z.; Giralt, S.; De Lima, M.; Hosing, C.; Kharfan-Dabaja, M.A.; Anagnostopoulos, A.; Champlin, R. Chronic graft-versus-host disease manifesting as polymyositis: An uncommon presentation. Bone Marrow Transplant. 2002, 30, 543–546. [Google Scholar] [CrossRef]
- Meng, L.; Ji, S.; Wang, Q.; Bu, B. Polymyositis as a manifestation of chronic graft-versus-host disease after allo-HSCT. Clin. Case Rep. 2018, 6, 1723–1726. [Google Scholar]
- Takahashi, K.; Kashihara, K.; Shinagawa, K.; Yoshino, T.; Abe, K.; Harada, M. Myositis as a manifestation of chronic graft-versus-host disease. Intern. Med. 2000, 39, 482–485. [Google Scholar] [CrossRef]
- Stephenson, A.L.; Mackenzie, I.R.; Levy, R.D.; Road, J. Myositis associated graft-versus-host-disease presenting as respiratory muscle weakness. Thorax 2001, 56, 82–84. [Google Scholar] [CrossRef]
- Golec, S.; Rabinovich, E.; Cohen, M.; Baer, L.; Chamoun, K.; Lima, M. Refractory inflammatory myopathy in hematopoietic stem cell transplant patients with chronic graft-versus-host disease: Report of two cases. Hematol. Transfus. Cell Ther. 2019, 41, 268–271. [Google Scholar] [CrossRef]
- Maillard-Lefebvre, H.; Morell-Dubois, S.; Lambert, M.; Charlanne, H.; Launay, D.; Hachulla, E.; Yakoub-Agh, I.; Hatron, P.Y. Graft-versus-host disease-related polymyositis. Clin. Rheumatol. 2010, 29, 431–433. [Google Scholar] [CrossRef]
- George, B.; Danda, D.; Chandy, M.; Srivastava, A.; Mathews, V. Polymyositis--an unusual manifestation of chronic graft-versus-host disease. Rheumatol. Int. 2001, 20, 169–170. [Google Scholar] [CrossRef]
- Leano, A.M.; Miller, K.; White, A.C. Chronic graft-versus-host disease-related polymyositis as a cause of respiratory failure following allogeneic bone marrow transplant. Bone Marrow Transplant. 2000, 26, 1117–1120. [Google Scholar] [CrossRef][Green Version]
- Sharaf, N.; Prayson, R.A. Relapsing polymyositis in chronic graft versus host disease. J. Clin. Neurosci. 2014, 21, 1964–1965. [Google Scholar] [CrossRef] [PubMed]
- Ascensao, J.L.; Mascarenhas, R.B.; Mittelman, A.; Ahmed, T. Case report: Acute polymyositis in a patient with chronic graft vs. host disease. Med. Oncol. Tumor Pharmacother. 1992, 9, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Pier, N.; Dubowitz, V. Chronic graft versus host disease presenting with polymyositis. Br. Med. J. (Clin. Res. Ed.) 1983, 286, 2024. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Allen, J.A.; Greenberg, S.A.; Amato, A.A. Dermatomyositis-like muscle pathology in patients with chronic graft-versus-host disease. Muscle Nerve 2009, 40, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Shahzad, M.; Chaudhary, S.G.; Basit, A.; Thellman, C.; Rodriguez, L.; Abhyankar, S.H.; McGuirk, J.P.; Mushtaq, M.U. Chronic graft-versus-host disease presenting as acute polymyositis: A case series and systematic review. Transpl. Immunol. 2022, 70, 101520. [Google Scholar] [CrossRef]
- Tan, Y.; Lin, J.; Hong, X.; Lu, J.; Lu, Q. Polymyositis in a child with thalassemia after hematopoietic stem cell transplantation: A case report. Medicine 2021, 100, e27388. [Google Scholar] [CrossRef]
- Wilkinson, M.; Yeung, D.; Limaye, V. A case of inflammatory myopathy in graft vs. host disease-A potential role for ibrutinib. Neuromuscul. Disord. 2021, 31, 865–869. [Google Scholar] [CrossRef]
- Koh, S.; Koh, H.; Nakashima, Y.; Katayama, T.; Sakabe, M.; Okamura, H.; Yoshimura, T.; Nanno, S.; Nishimoto, M.; Hayashi, Y.; et al. Plasma Kinetics of Th1, Th2 and Th17 Cytokines in Polymyositis Related to Chronic Graft-versus-Host Disease. Intern. Med. 2016, 55, 2265–2270. [Google Scholar] [CrossRef][Green Version]
- Khan, M.; Ubogu, E.; Alsharabati, M.; Salzman, D.; Mineishi, S.; Saad, A. Acute myofascitis as a manifestation of chronic graft-versus-host disease. Muscle Nerve 2016, 53, 327–329. [Google Scholar] [CrossRef]
- Sato, N.; Okamoto, S.; Mori, T.; Watanabe, R.; Hamano, Y.; Kawamura, J.; Ishihara, D.; Ikeda, Y. Recurrent acute myositis after allogeneic bone marrow transplantation for myelodysplasia. Hematology 2002, 7, 109–112. [Google Scholar] [CrossRef]
- Michelis, F.V.; Bril, V.; Lipton, J.H. A case report and literature review of chronic graft-versus-host disease manifesting as polymyositis. Int. J. Hematol. 2015, 102, 144–146. [Google Scholar] [CrossRef]
- Parker, P.; Chao, N.J.; Ben-Ezra, J.; Slatkin, N.; Openshaw, H.; Niland, J.C.; Linker, C.A.; Greffe, B.S.; Kashyap, A.; Molina, A.; et al. Polymyositis as a manifestation of chronic graft-versus-host disease. Medicine 1996, 75, 279–285. [Google Scholar] [CrossRef]
- Reyes, M.G.; Noronha, P.; Thomas, W., Jr.; Heredia, R. Myositis of chronic graft versus host disease. Neurology 1983, 33, 1222–1224. [Google Scholar] [CrossRef]
- Shulman, H.M.; Kleiner, D.; Lee, S.J.; Morton, T.; Pavletic, S.Z.; Farmer, E.; Moresi, J.M.; Greenson, J.; Janin, A.; Martin, P.J.; et al. Histopathologic diagnosis of chronic graft-versus-host disease: National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: II. Pathology Working Group Report. Biol. Blood Marrow Transplant. 2006, 12, 31–47. [Google Scholar] [CrossRef]
- Min, C.K. The pathophysiology of chronic graft-versus-host disease: The unveiling of an enigma. Korean J. Hematol. 2011, 46, 80–87. [Google Scholar] [CrossRef]
- Hakim, F.T.; Memon, S.A.; Cepeda, R.; Jones, E.C.; Chow, C.K.; Kasten-Sportes, C.; Odom, J.; Vance, B.A.; Christensen, B.L.; Mackall, C.L.; et al. Age-dependent incidence, time course, and consequences of thymic renewal in adults. J. Clin. Investig. 2005, 115, 930–939. [Google Scholar] [CrossRef]
- Grauer, O.; Wolff, D.; Bertz, H.; Greinix, H.; Kühl, J.S.; Lawitschka, A.; Lee, S.J.; Pavletic, S.Z.; Holler, E.; Kleiter, I. Neurological manifestations of chronic graft-versus-host disease after allogeneic haematopoietic stem cell transplantation: Report from the Consensus Conference on Clinical Practice in chronic graft-versus-host disease. Brain 2010, 133, 2852–2865. [Google Scholar] [CrossRef]
- Carreras, E.; Dufour, C.; Mohty, M.; Kröger, N. (Eds.) The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies; Springer: Cham, Switzerland, 2019; Available online: https://link.springer.com/book/10.1007/978-3-030-02278-5#affiliations (accessed on 10 August 2022).
- Filipovich, A.H.; Weisdorf, D.; Pavletic, S.; Socie, G.; Wingard, J.R.; Lee, S.J.; Martin, P.; Chien, J.; Przepiorka, D.; Couriel, D.; et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol. Blood Marrow Transplant. 2005, 11, 945–956. [Google Scholar] [CrossRef]
- Jagasia, M.H.; Greinix, H.T.; Arora, M.; Williams, K.M.; Wolff, D.; Cowen, E.W.; Palmer, J.; Weisdorf, D.; Treister, N.S.; Cheng, G.S.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol. Blood Marrow Transplant. 2015, 21, 389–401.e1. [Google Scholar] [CrossRef]
- Gupta, A.; Gupta, Y. Glucocorticoid-induced myopathy: Pathophysiology, diagnosis, and treatment. Indian J. Endocrinol. Metab. 2013, 17, 913–916. [Google Scholar] [CrossRef]
- Grube, M.; Holler, E.; Weber, D.; Holler, B.; Herr, W.; Wolff, D. Risk Factors and Outcome of Chronic Graft-versus-Host Disease after Allogeneic Stem Cell Transplantation-Results from a Single-Center Observational Study. Biol. Blood Marrow Transplant. 2016, 22, 1781–1791. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.R.; Haig, A.J.; Couriel, D.R. Musculoskeletal, Neurologic, and Cardiopulmonary Aspects of Physical Rehabilitation in Patients with Chronic Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2015, 21, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Sandnes, M.; Ulvik, R.J.; Vorland, M.; Reikvam, H. Hyperferritinemia-A Clinical Overview. J. Clin. Med. 2021, 10, 2008. [Google Scholar] [CrossRef] [PubMed]
- Tvedt, T.H.; Lie, S.A.; Reikvam, H.; Rye, K.P.; Lindås, R.; Gedde-Dahl, T.; Ahmed, A.B.; Bruserud, Ø. Pretransplant Levels of CRP and Interleukin-6 Family Cytokines; Effects on Outcome after Allogeneic Stem Cell Transplantation. Int. J. Mol. Sci. 2016, 17, 1823. [Google Scholar] [CrossRef]
- Bidgoli, A.; DePriest, B.P.; Saatloo, M.V.; Jiang, H.; Fu, D.; Paczesny, S. Current Definitions and Clinical Implications of Biomarkers in Graft-versus-Host Disease. Transplant. Cell Ther. 2022, 28, 657–666. [Google Scholar] [CrossRef]
- Reikvam, H.; Vo, A.K.; Johansen, S.; Hemsing, A.L.; Solheim, M.H.; Mosevoll, K.A.; Tvedt, T.H.A.; Hatfield, K.J. MicroRNA serum profiles and chronic graft-versus-host disease. Blood Adv. 2022, 6, 5295–5306. [Google Scholar] [CrossRef]




| Analysis | Before Treatment | Six Months after Treatment | Reference Area |
|---|---|---|---|
| Hemoglobin (g/dL) | 14.0 | 13.6 | 13–18 |
| WBC (×109/L) | 15.3 | 7.5 | 3.5–10.0 |
| Neutrophils (×109/L) | 11.9 | 2.6 | 1.5–7.3 |
| Lymphocytes (×109/L) | 2.4 | 4 | 1.1–3.3 |
| Thrombocytes (×109/L) | 291 | 250 | 150–400 |
| Ferritin (ng/mL) | 658 | 786 | 7–75 |
| CRP (mg/L) | 52 | <1 | <5 |
| Sodium (mmol/L) | 138 | 141 | 136–146 |
| Potassium (mmol/L) | 4.7 | 4.1 | 3.5–5.0 |
| ALAT (U/L) | 107 | 40 | <70 |
| ALP (U/L) | 155 | 39 | 35–105 |
| GT (U/L) | 425 | 91 | <115 |
| Bilirubin (µmol/dL) | 9 | 5 | <26 |
| LDH (U/L) | 268 | 197 | 300–600 |
| Albumin (g/L) | 38 | 42 | 36–47 |
| CK (U/L) | 1291 | 173 | <280 |
| Organ or Site | Diagnostic (Sufficient to Establish the Diagnosis of cGVHD) | Distinctive (Seen in cGVHD, but Insufficient Alone to Establish a Diagnosis of cGVHD) | Other Features * |
|---|---|---|---|
| Muscles, fascia, joints | Fasciitis, joint stiffness, or contractures secondary to sclerosis | Myositis or polymyositis ** | Edema, muscle cramps, arthralgia, or arthritis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kvinge, A.D.; Kvammen, T.; Miletic, H.; Bindoff, L.A.; Reikvam, H. Musculoskeletal Chronic Graft versus Host Disease—A Rare Complication to Allogeneic Hematopoietic Stem Cell Transplant: A Case-Based Report and Review of the Literature. Curr. Oncol. 2022, 29, 8415-8430. https://doi.org/10.3390/curroncol29110663
Kvinge AD, Kvammen T, Miletic H, Bindoff LA, Reikvam H. Musculoskeletal Chronic Graft versus Host Disease—A Rare Complication to Allogeneic Hematopoietic Stem Cell Transplant: A Case-Based Report and Review of the Literature. Current Oncology. 2022; 29(11):8415-8430. https://doi.org/10.3390/curroncol29110663
Chicago/Turabian StyleKvinge, Alexander Dåtland, Tobias Kvammen, Hrvoje Miletic, Laurence Albert Bindoff, and Håkon Reikvam. 2022. "Musculoskeletal Chronic Graft versus Host Disease—A Rare Complication to Allogeneic Hematopoietic Stem Cell Transplant: A Case-Based Report and Review of the Literature" Current Oncology 29, no. 11: 8415-8430. https://doi.org/10.3390/curroncol29110663
APA StyleKvinge, A. D., Kvammen, T., Miletic, H., Bindoff, L. A., & Reikvam, H. (2022). Musculoskeletal Chronic Graft versus Host Disease—A Rare Complication to Allogeneic Hematopoietic Stem Cell Transplant: A Case-Based Report and Review of the Literature. Current Oncology, 29(11), 8415-8430. https://doi.org/10.3390/curroncol29110663