Survival in Women with De Novo Metastatic Breast Cancer: A Comparison of Real-World Evidence from a Publicly-Funded Canadian Province and the United States by Insurance Status


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Patient Selection
2.2. Statistical Analysis
3. Results
3.1. US and AB Cohorts
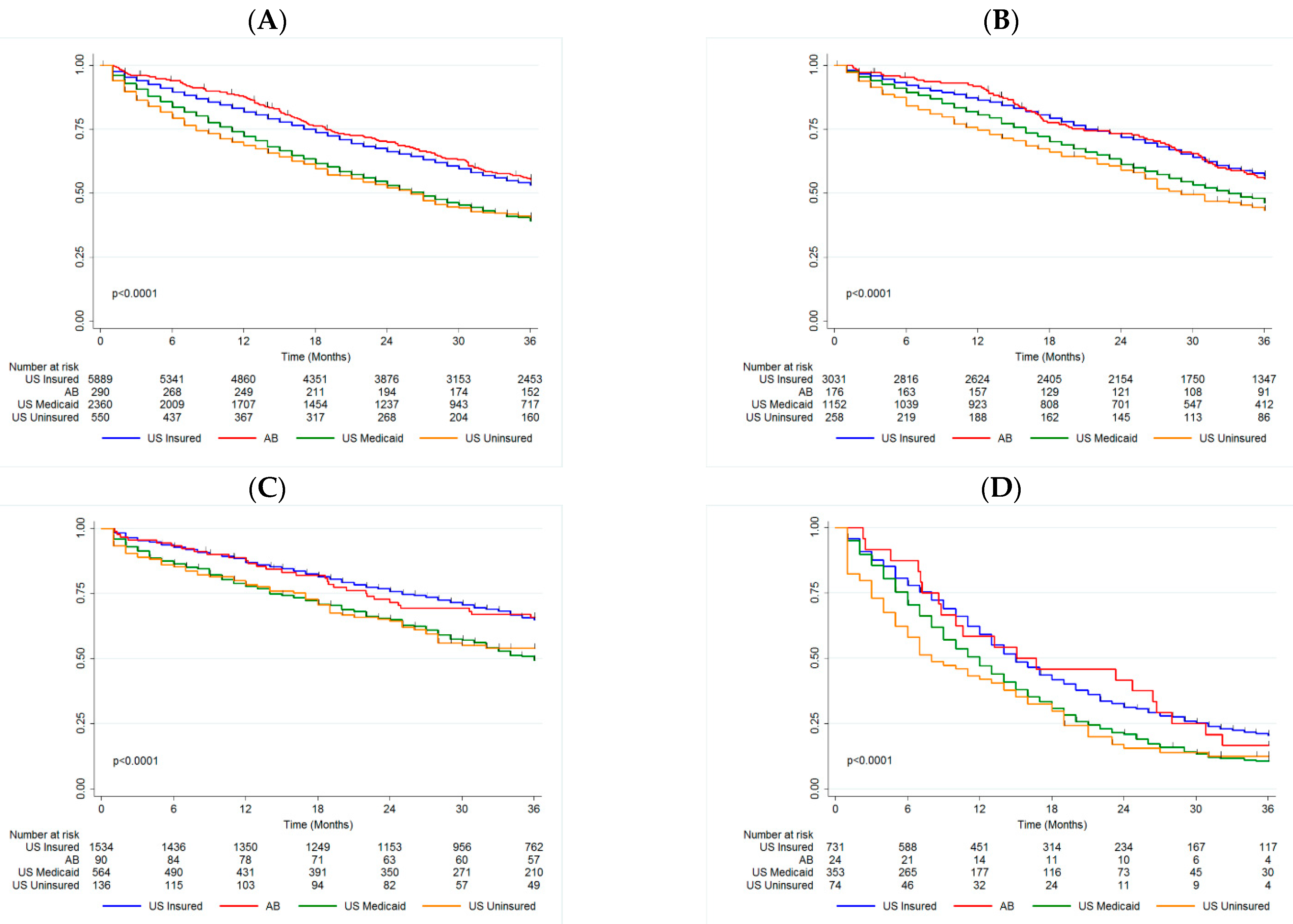
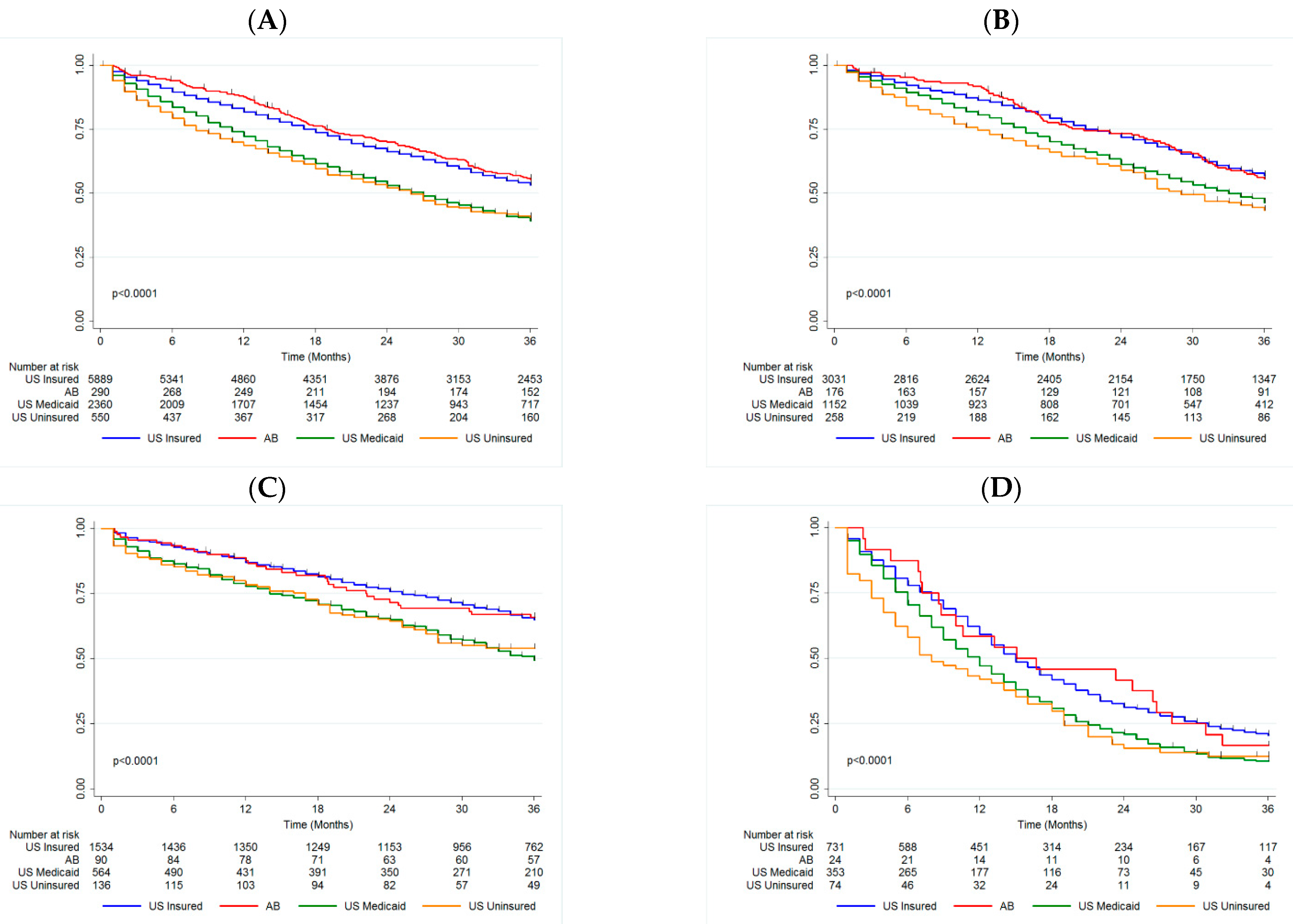
3.2. Insurance Status
3.3. Insurance Status by Biomarker Profile
3.3.1. HR+/HER2−
3.3.2. HER2+
3.3.3. TN
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Canadian Cancer Society. Breast Cancer Statistics. Available online: http://www.cancer.ca/en/cancer-information/cancer-type/breast/statistics/?region=on (accessed on 19 April 2020).
- Tao, L.; Chu, L.; Wang, L.I.; Moy, L.; Brammer, M.; Song, C.; Green, M.; Kurian, A.W.; Gomez, S.L.; Clarke, C.A. Occurrence and outcome of de novo metastatic breast cancer by subtype in a large, diverse population. Cancer Causes Control 2016, 27, 1127–1138. [Google Scholar] [CrossRef] [PubMed]
- Caswell-Jin, J.; Plevritis, S.K.; Tian, L.; Cadham, C.; Xu, C.; Stout, N.K.; Sledge, G.W.; Mandelblatt, J.S.; Kurian, A.W. Change in Survival in Metastatic Breast Cancer with Treatment Advances: Meta-Analysis and Systematic Review. JNCI Cancer Spectr. 2018, 2, pky062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariotto, A.B.; Etzioni, R.; Hurlbert, M.; Penberthy, L.; Mayer, M. Estimation of the number of women living with metastatic breast cancer in the United States. Cancer Epidemiol. Biomark. Prev. 2017, 26, 809–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Den Brok, W.D.; Speers, C.H.; Gondara, L.; Baxter, E.; Tyldesley, S.K.; Lohrisch, C.A. Survival with metastatic breast cancer based on initial presentation, de novo versus relapsed. Breast Cancer Res. Treat. 2017, 161, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Berchick, E.R.; Hood, E.; Barnett, J.C. Health Insurance Coverage in the United States: 2017 Current Population Reports (P60-264); United States Census Bureau: Washington, DC, USA, 2018. [Google Scholar]
- Wharam, J.F.; Ross-Degnan, D.; Rosenthal, M.B. The ACA and High-Deductible Insurance—Strategies for Sharpening a Blunt Instrument. N. Engl. J. Med. 2013, 369, 1481–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorey, K.M. Breast cancer survival in Canada and the USA: Meta-analytic evidence of a Canadian advantage in low-income areas. Int. J. Epidemiol. 2009, 38, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Gorey, K.M.; Richter, N.L.; Luginaah, I.; Hamm, C.; Holowaty, E.J.; Zou, G.; Balagurusamy, M.K. Breast Cancer among Women Living in Poverty: Better Care in Canada than in the United States. Soc. Work. Res. 2015, 39, 107–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuel, N.; Verma, S. Cross-comparison of cancer drug approvals at three international regulatory agencies. Curr. Oncol. 2016, 23, 454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niraula, S. Trends of new cancer drug approvals from the perspective of a publicly funded healthcare system: Analyses of the pan-Canadian Oncology Drug Review (pCODR) recommendations. J. Clin. Oncol. 2018, 36, 6516. [Google Scholar] [CrossRef]
- CADTH. About the Pan-Canadian Oncology Drug Review (pCODR). Available online: https://cadth.ca/pcodr/about-pcodr (accessed on 19 April 2020).
- NIH. SEER Incidence Data, 1975–2016. Available online: http://seer.cancer.gov/data (accessed on 19 April 2020).
- Khan, S.A.; Zhao, F.; Solin, L.J.; Goldstein, L.J.; Cella, D.; Basik, M.; Golshan, M.; Julian, T.B.; Pockaj, B.A.; Lee, C.A.; et al. A randomized phase III trial of systemic therapy plus early local therapy versus systemic therapy alone in women with de novo stage IV breast cancer: A trial of the ECOG-ACRIN Research Group (E2108). J. Clin. Oncol. 2020, 38, LBA2. [Google Scholar] [CrossRef]
- Vaz-Luis, I.; Lin, N.U.; Keating, N.L.; Barry, W.T.; Winer, E.P.; Freedman, R.A. Factors Associated with Early Mortality Among Patients with De Novo Metastatic Breast Cancer: A Population—Based Study. Oncologist 2017, 22, 386–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, L.; Canchola, A.J.; Spiegel, D.; Ladabaum, U.; Haile, R.; Gomez, S.L. Trends in cancer survival by health insurance status in California from 1997 to 2014. JAMA Oncol. 2018, 4, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Fallahpour, S.; Navaneelan, T.; De, P.; Borgo, A. Breast cancer survival by molecular subtype: A population-based analysis of cancer registry data. C Open 2017, 5, E734–E739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumachev, A.; Trudeau, M.E.; Chan, K.K.W. Associations among socioeconomic status, patterns of care and outcomes in breast cancer patients in a universal health care system: Ontario’s experience. Cancer 2016, 122, 893–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S Department of Health and Human Services: Office of Minority Health. Profile: Black/African Americans. Available online: https://www.minorityhealth.hhs.gov/omh/browse.aspx?lvl=3&lvlid=61 (accessed on 19 April 2020).
- Statistics Canada. Diversity of the Black Population in Canada: An overview. Available online: https://www150.statcan.gc.ca/n1/pub/89-657-x/89-657-x2019002-eng.htm (accessed on 19 April 2020).
- Dietze, E.C.; Sistrunk, C.; Miranda-Carboni, G.; O’Regan, R.; Seewaldt, V.L. Triple-negative breast cancer in African-American women: Disparities versus biology. Nat. Rev. Cancer 2015, 15, 248–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aizer, A.A.; Wilhite Ba, T.J.; Chen, M.-H.; Ahamb, P.L.G.; Choueiri, T.K.; Hoffman, K.E.; Martin, N.E.; Trinh, Q.-D.; Hu, J.C.; Nguyen, P.L. Lack of reduction in racial disparities in cancer-specific mortality over a 20-year period. Cancer 2014, 120, 1532–1539. [Google Scholar] [CrossRef] [PubMed]
- Stark, A.; Kleer, C.G.; Martin, I.; Awuah, B.; Nsiah-Asare, A.; Takyi, V.; Braman, M.; Quayson, S.E.; Zarbo, R.; Wicha, M.; et al. African ancestry and higher prevalence of triple-negative breast cancer. Cancer 2010, 116, 4926–4932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NIH. SEER Program: Population Characteristics. Available online: https://seer.cancer.gov/registries/characteristics.html (accessed on 19 April 2020).
- Brooks, G.A.; Hoverman, J.R.; Colla, C.H. The Affordable Care Act and Cancer Care Delivery. Cancer J. 2017, 23, 163–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wharam, J.F.; Zhang, F.; Lu, C.Y.; Wagner, A.K.; Nekhlyudov, L.; Earle, C.C.; Soumerai, S.B.; Ross-Degnan, D. Breast Cancer Diagnosis and Treatment After High-Deductible Insurance Enrollment. J. Clin. Oncol. 2018, 36, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Magge, H.; Cabral, H.J.; Kazis, L.E.; Sommers, B.D. Prevalence and predictors of underinsurance among low-income adults. J. Gen. Intern. Med. 2013, 28, 1136–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| US Privately Insured | AB | US Medicaid | US Uninsured | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | n | (%) | p-Value | |
| 6124 | 100.0% | 291 | 100.0% | 2493 | 100.0% | 637 | 100.0% | ||
| Age | |||||||||
| Median | 54 | 52 | 53 | 55 | |||||
| Range | (19–64) | (22–64) | (20–64) | (21–64) | |||||
| Age Group | |||||||||
| 18–49 | 1997 | 32.6% | 105 | 36.1% | 884 | 35.5% | 186 | 29.2% | 0.006 |
| 50–64 | 4127 | 67.4% | 186 | 63.9% | 1609 | 64.5% | 451 | 70.8% | |
| Year of Diagnosis | |||||||||
| 2010 | 1200 | 19.6% | 50 | 17.2% | 495 | 19.9% | 114 | 17.9% | 0.014 |
| 2011 | 1220 | 19.9% | 65 | 22.3% | 508 | 20.4% | 136 | 21.4% | |
| 2012 | 1205 | 19.7% | 47 | 16.2% | 481 | 19.3% | 133 | 20.9% | |
| 2013 | 1221 | 19.9% | 64 | 22.0% | 493 | 19.8% | 160 | 25.1% | |
| 2014 | 1278 | 20.9% | 65 | 22.3% | 516 | 20.7% | 94 | 14.8% | |
| Surgical Status | |||||||||
| No Surgery | 3678 | 60.1% | 175 | 60.1% | 1685 | 67.6% | 487 | 76.5% | <0.001 |
| Surgery | 2312 | 37.8% | 116 | 39.9% | 750 | 30.1% | 138 | 21.7% | |
| 134 | 2.2% | 0 | 0.0% | 58 | 2.3% | 12 | 1.9% | ||
| Biomarker Profile | |||||||||
| HR+/HER2− | 3095 | 50.5% | 176 | 60.5% | 1183 | 47.5% | 285 | 44.7% | 0.001 |
| HER2+ | 1589 | 25.9% | 90 | 30.9% | 590 | 23.7% | 150 | 23.5% | |
| TN | 760 | 12.4% | 25 | 8.6% | 369 | 14.8% | 83 | 13.0% | |
| Missing | 680 | 11.1% | 0 | 0.0% | 351 | 14.1% | 119 | 18.7% | |
| Overall Cohort | Multivariate | ||
|---|---|---|---|
| HR | 95%CI | p-Value | |
| US Privately Insured | Reference | ||
| AB | 1.04 | (0.87–1.25) | 0.703 |
| US Medicaid | 1.41 | (1.32–1.52) | <0.001 |
| US Uninsured | 1.44 | (1.26–1.63) | <0.001 |
| No Surgery | Reference | ||
| Surgery | 0.51 | (0.47–0.55) | <0.001 |
| Age | |||
| (continuous) | 1.01 | (1.01–1.02) | <0.001 |
| HR+/HER2− | Reference | ||
| HER2+ | 0.87 | (0.81–0.94) | 0.001 |
| TN | 3.48 | (3.21–3.76) | <0.001 |
| HR+/HER2− | Multivariate | ||
| HR | 95%CI | p-Value | |
| US Privately Insured | Reference | ||
| AB | 1.06 | (0.84–1.35) | 0.603 |
| US Medicaid | 1.36 | (1.23–1.51) | <0.001 |
| US Uninsured | 1.42 | (1.19–1.70) | <0.001 |
| No Surgery | Reference | ||
| Surgery | 0.52 | (0.47–0.57) | <0.001 |
| Age | |||
| (continuous) | 1.01 | (1.01–1.02) | <0.001 |
| HER2+ | Multivariate | ||
| HR | 95%CI | p-Value | |
| US Privately Insured | Reference | ||
| AB | 0.93 | (0.64–1.35) | 0.701 |
| US Medicaid | 1.61 | (1.39–1.87) | <0.001 |
| US Uninsured | 1.37 | (1.04–1.81) | 0.023 |
| No Surgery | Reference | ||
| Surgery | 0.49 | (0.42–0.56) | <0.001 |
| Age | |||
| (continuous) | 1.03 | (1.02–1.04) | <0.001 |
| TN | Multivariate | ||
| HR | 95%CI | p-Value | |
| US Privately Insured | Reference | ||
| AB | 1.06 | (0.67–1.65) | 0.814 |
| US Medicaid | 1.34 | (1.16–1.54) | <0.001 |
| US Uninsured | 1.50 | (1.15–1.95) | 0.003 |
| No Surgery | Reference | ||
| Surgery | 0.51 | (0.45–0.58) | <0.001 |
| Age | |||
| (continuous) | 1.00 | (1.00–1.01) | 0.220 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savard, M.-F.; Kornaga, E.N.; Kahn, A.M.; Lupichuk, S. Survival in Women with De Novo Metastatic Breast Cancer: A Comparison of Real-World Evidence from a Publicly-Funded Canadian Province and the United States by Insurance Status. Curr. Oncol. 2022, 29, 383-391. https://doi.org/10.3390/curroncol29010034
Savard M-F, Kornaga EN, Kahn AM, Lupichuk S. Survival in Women with De Novo Metastatic Breast Cancer: A Comparison of Real-World Evidence from a Publicly-Funded Canadian Province and the United States by Insurance Status. Current Oncology. 2022; 29(1):383-391. https://doi.org/10.3390/curroncol29010034
Chicago/Turabian StyleSavard, Marie-France, Elizabeth N. Kornaga, Adriana Matutino Kahn, and Sasha Lupichuk. 2022. "Survival in Women with De Novo Metastatic Breast Cancer: A Comparison of Real-World Evidence from a Publicly-Funded Canadian Province and the United States by Insurance Status" Current Oncology 29, no. 1: 383-391. https://doi.org/10.3390/curroncol29010034
APA StyleSavard, M.-F., Kornaga, E. N., Kahn, A. M., & Lupichuk, S. (2022). Survival in Women with De Novo Metastatic Breast Cancer: A Comparison of Real-World Evidence from a Publicly-Funded Canadian Province and the United States by Insurance Status. Current Oncology, 29(1), 383-391. https://doi.org/10.3390/curroncol29010034