Combination of Lenvatinib and Pembrolizumab as Salvage Treatment for Paucicellular Variant of Anaplastic Thyroid Cancer: A Case Report

 , ,
, ,  ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
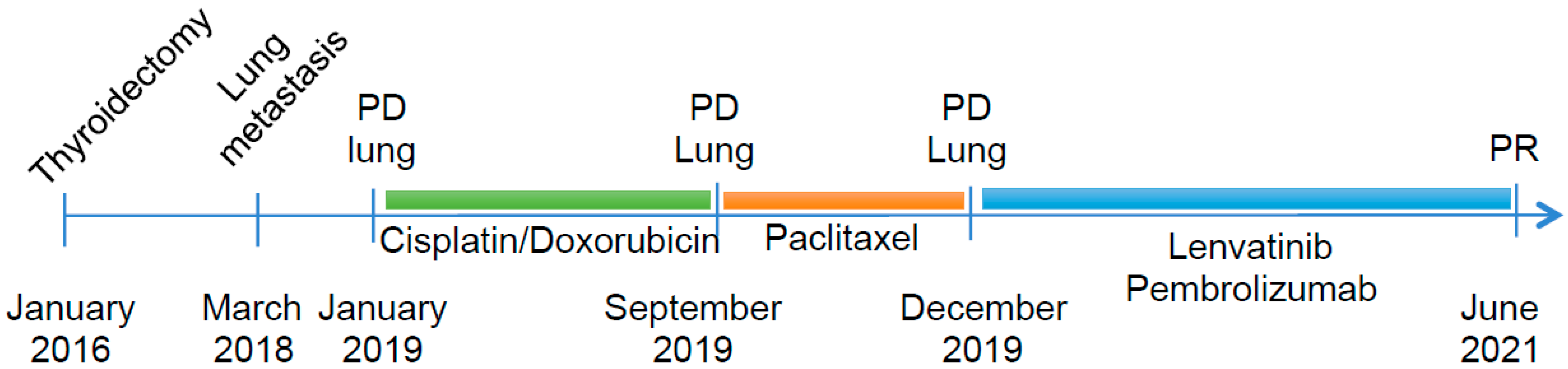
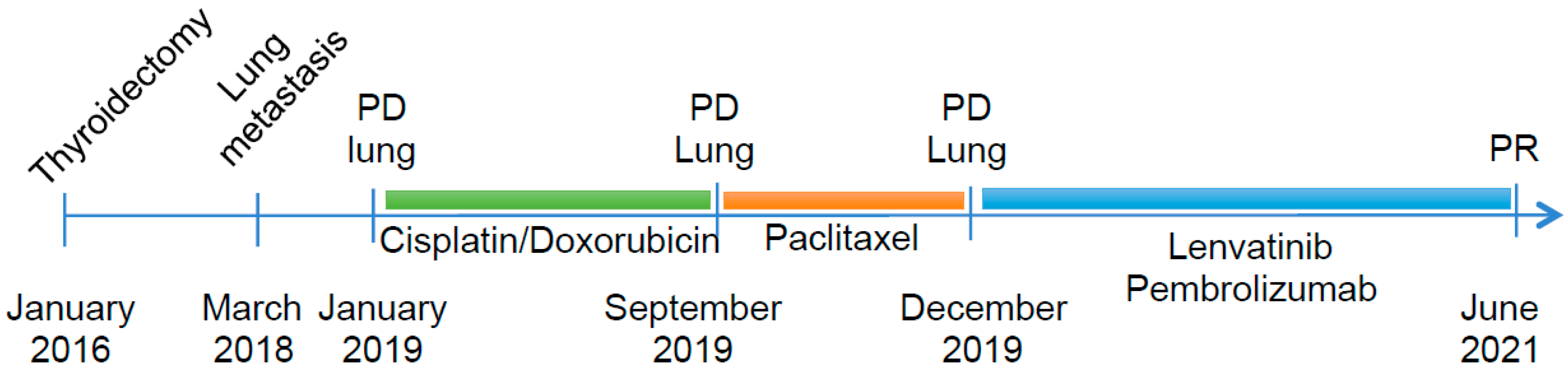
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cabanillas, M.E.; Ahmed, S.; Wang, J.R. Management of Anaplastic and Recurrent Differentiated Thyroid Cancer: Indications for Surgical Resection, Molecular Testing, and Systemic Therapy. Neuroimaging Clin. N. Am. 2021, 31, 359–366. [Google Scholar] [CrossRef]
- Smallridge, R.C.; Copland, J.A. Anaplastic thyroid carcinoma: Pathogenesis and emerging therapies. Clin. Oncol. 2010, 22, 486–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Are, C.; Shaha, A.R. Anaplastic thyroid carcinoma: Biology, pathogenesis, prognostic factors, and treatment approaches. Ann. Surg. Oncol. 2006, 13, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.R.; Zafereo, M.E.; Dadu, R.; Ferrarotto, R.; Busaidy, N.L.; Lu, C.; Ahmed, S.; Gule-Monroe, M.K.; Williams, M.D.; Sturgis, E.M.; et al. Complete Surgical Resection Following Neoadjuvant Dabrafenib Plus Trametinib in BRAF(V600E)-Mutated Anaplastic Thyroid Carcinoma. Thyroid 2019, 29, 1036–1043. [Google Scholar] [CrossRef] [Green Version]
- Bible, K.C.; Kebebew, E.; Brierley, J.; Brito, J.P.; Cabanillas, M.E.; Clark, T.J., Jr.; Di Cristofano, A.; Foote, R.; Giordano, T.; Kasperbauer, J.; et al. 2021 American Thyroid Association Guidelines for Management of Patients with Anaplastic Thyroid Cancer. Thyroid 2021, 31, 337–386. [Google Scholar] [CrossRef]
- Dierks, C.; Seufert, J.; Aumann, K.; Ruf, J.; Klein, C.; Kiefer, S.; Rassner, M.; Boerries, M.; Zielke, A.; la Rosee, P.; et al. Combination of Lenvatinib and Pembrolizumab Is an Effective Treatment Option for Anaplastic and Poorly Differentiated Thyroid Carcinoma. Thyroid 2021, 31, 1076–1085. [Google Scholar] [CrossRef] [PubMed]
- Sparano, C.; Godbert, Y.; Attard, M.; Do Cao, C.; Zerdoud, S.; Roudaut, N.; Joly, C.; Berdelou, A.; Hadoux, J.; Lamartina, L.; et al. Limited efficacy of lenvatinib in heavily pretreated anaplastic thyroid cancer: A French overview. Endocr.-Relat. Cancer 2021, 28, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Canos, J.C.; Serrano, A.; Matias-Guiu, X. Paucicellular variant of anaplastic thyroid carcinoma: Report of two cases. Endocr. Pathol. 2001, 12, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.H.; Munshi, M.M.; Bobhate, S.K. Cytological diagnosis of paucicellular variant of anaplastic carcinoma of thyroid: Report of two cases. Cytopathology 2001, 12, 203–208. [Google Scholar] [CrossRef]
- Chan, J.K.; Tsang, W.Y. Endocrine malignancies that may mimic benign lesions. Sem. Diagn. Pathol. 1995, 12, 45–63. [Google Scholar]
- Wan, S.K.; Chan, J.K.; Tang, S.K. Paucicellular variant of anaplastic thyroid carcinoma. A mimic of Reidel’s thyroiditis. Am. J. Clin. Pathol. 1996, 105, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Bible, K.C. Immunotherapy in Anaplastic Thyroid Cancer: Much Yet to Be Learned. AACE Clin. Case Rep. 2021, 7, 334–335. [Google Scholar] [CrossRef]
- Zheng, L.; Li, L.; He, Q.; Wang, M.; Ma, Y.; Zhu, J.; Li, Y.; Fu, X.; Zhang, Y. Response to immunotherapy in a patient with anaplastic thyroid cancer: A case report. Medicine 2021, 100, e26138. [Google Scholar] [CrossRef] [PubMed]
- Iyer, P.C.; Dadu, R.; Gule-Monroe, M.; Busaidy, N.L.; Ferrarotto, R.; Habra, M.A.; Zafereo, M.; Williams, M.D.; Gunn, G.B.; Grosu, H.; et al. Salvage pembrolizumab added to kinase inhibitor therapy for the treatment of anaplastic thyroid carcinoma. J. Immunother. Cancer 2018, 6, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bible, K.C.; Suman, V.J.; Menefee, M.E.; Smallridge, R.C.; Molina, J.R.; Maples, W.J.; Karlin, N.J.; Traynor, A.M.; Kumar, P.; Goh, B.C.; et al. A multiinstitutional phase 2 trial of pazopanib monotherapy in advanced anaplastic thyroid cancer. J. Clin. Endocrinol. Metab. 2012, 97, 3179–3184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, E.E.; Rosen, L.S.; Vokes, E.E.; Kies, M.S.; Forastiere, A.A.; Worden, F.P.; Kane, M.A.; Sherman, E.; Kim, S.; Bycott, P.; et al. Axitinib is an active treatment for all histologic subtypes of advanced thyroid cancer: Results from a phase II study. Am. J. Clin. Oncol. 2008, 26, 4708–4713. [Google Scholar] [CrossRef]
- Savvides, P.; Nagaiah, G.; Lavertu, P.; Fu, P.; Wright, J.J.; Chapman, R.; Wasman, J.; Dowlati, A.; Remick, S.C. Phase II trial of sorafenib in patients with advanced anaplastic carcinoma of the thyroid. Thyroid 2013, 23, 600–604. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, S.; Kiyota, N.; Yamazaki, T.; Chayahara, N.; Nakano, K.; Inagaki, L.; Toda, K.; Enokida, T.; Minami, H.; Imamura, Y.; et al. A Phase II study of the safety and efficacy of lenvatinib in patients with advanced thyroid cancer. Fut. Oncol. 2019, 15, 717–726. [Google Scholar] [CrossRef] [Green Version]
- Wirth, L.J.; Brose, M.S.; Sherman, E.J.; Licitra, L.; Schlumberger, M.; Sherman, S.I.; Bible, K.C.; Robinson, B.; Rodien, P.; Godbert, Y.; et al. Open-Label, Single-Arm, Multicenter, Phase II Trial of Lenvatinib for the Treatment of Patients with Anaplastic Thyroid Cancer. Am. J. Clin. Oncol. 2021, 39, 2359–2366. [Google Scholar] [CrossRef] [PubMed]
- Adam, P.; Kircher, S.; Sbiera, I.; Koehler, V.F.; Berg, E.; Knosel, T.; Sandner, B.; Fenske, W.K.; Blaker, H.; Smaxwil, C.; et al. FGF-Receptors and PD-L1 in Anaplastic and Poorly Differentiated Thyroid Cancer: Evaluation of the Preclinical Rationale. Front. Endocrinol. 2021, 12, 712107. [Google Scholar] [CrossRef]
- De Leo, S.; Trevisan, M.; Fugazzola, L. Recent advances in the management of anaplastic thyroid cancer. Thyroid Res. 2020, 13, 17. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, S.M.; Elia, G.; Ragusa, F.; Ruffilli, I.; La Motta, C.; Paparo, S.R.; Patrizio, A.; Vita, R.; Benvenga, S.; Materazzi, G.; et al. Novel treatments for anaplastic thyroid carcinoma. Gland Surg. 2020, 9, S28–S42. [Google Scholar] [CrossRef] [PubMed]
- Szczepaniak Sloane, R.A.; Gopalakrishnan, V.; Reddy, S.M.; Zhang, X.; Reuben, A.; Wargo, J.A. Interaction of molecular alterations with immune response in melanoma. Cancer 2017, 123, 2130–2142. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.G.; Gupta, S.; Goel, S. Immunotherapy: Incorporation in the evolving paradigm of renal cancer management and future prospects. Oncotarget 2017, 8, 17313–17327. [Google Scholar] [CrossRef]
- Barsoum, I.B.; Smallwood, C.A.; Siemens, D.R.; Graham, C.H. A mechanism of hypoxia-mediated escape from adaptive immunity in cancer cells. Cancer Res. 2014, 74, 665–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, A.; Sakaguchi, S. Regulatory T cells in cancer immunotherapy. Cell Res. 2017, 27, 109–118. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhang, Z. The history and advances in cancer immunotherapy: Understanding the characteristics of tumor-infiltrating immune cells and their therapeutic implications. Cell. Mol. Immunol. 2020, 17, 807–821. [Google Scholar] [CrossRef]
- Chang, L.; Chang, M.; Chang, H.M.; Chang, F. Microsatellite Instability: A Predictive Biomarker for Cancer Immunotherapy. Appl. Immunohistochem. Mol. Morphol. 2018, 26, e15–e21. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Li, L.; Jiang, X.; Li, Q. Mismatch repair deficiency/microsatellite instability-high as a predictor for anti-PD-1/PD-L1 immunotherapy efficacy. J. Hematol. Oncol. 2019, 12, 54. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luongo, C.; Porcelli, T.; Sessa, F.; De Stefano, M.A.; Scavuzzo, F.; Damiano, V.; Klain, M.; Bellevicine, C.; Matano, E.; Troncone, G.; et al. Combination of Lenvatinib and Pembrolizumab as Salvage Treatment for Paucicellular Variant of Anaplastic Thyroid Cancer: A Case Report. Curr. Oncol. 2021, 28, 5401-5407. https://doi.org/10.3390/curroncol28060450
Luongo C, Porcelli T, Sessa F, De Stefano MA, Scavuzzo F, Damiano V, Klain M, Bellevicine C, Matano E, Troncone G, et al. Combination of Lenvatinib and Pembrolizumab as Salvage Treatment for Paucicellular Variant of Anaplastic Thyroid Cancer: A Case Report. Current Oncology. 2021; 28(6):5401-5407. https://doi.org/10.3390/curroncol28060450
Chicago/Turabian StyleLuongo, Cristina, Tommaso Porcelli, Francesca Sessa, Maria Angela De Stefano, Francesco Scavuzzo, Vincenzo Damiano, Michele Klain, Claudio Bellevicine, Elide Matano, Giancarlo Troncone, and et al. 2021. "Combination of Lenvatinib and Pembrolizumab as Salvage Treatment for Paucicellular Variant of Anaplastic Thyroid Cancer: A Case Report" Current Oncology 28, no. 6: 5401-5407. https://doi.org/10.3390/curroncol28060450
APA StyleLuongo, C., Porcelli, T., Sessa, F., De Stefano, M. A., Scavuzzo, F., Damiano, V., Klain, M., Bellevicine, C., Matano, E., Troncone, G., Schlumberger, M., & Salvatore, D. (2021). Combination of Lenvatinib and Pembrolizumab as Salvage Treatment for Paucicellular Variant of Anaplastic Thyroid Cancer: A Case Report. Current Oncology, 28(6), 5401-5407. https://doi.org/10.3390/curroncol28060450