Real-World Palbociclib Use in HR+/HER2− Advanced Breast Cancer in Canada: The IRIS Study

Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Study Population
2.3. Data Source and Extraction
2.4. Statistical Analysis
2.5. Role of the Funding Organization
3. Results
3.1. Physician and Patient Demographics
3.2. Palbociclib + Letrozole
3.2.1. Treatment Patterns
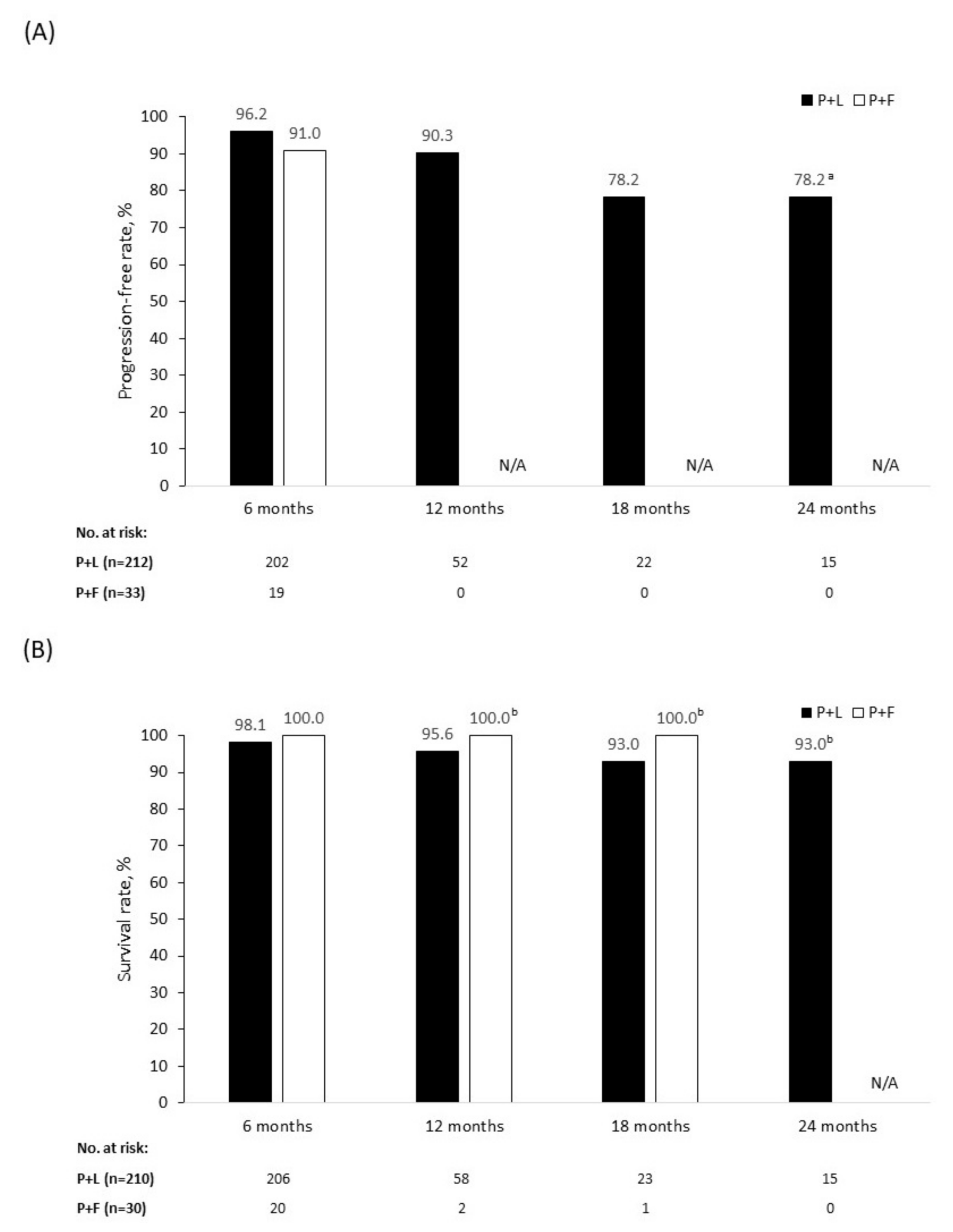
3.2.2. Clinical Outcomes
3.3. Palbociclib + Fulvestrant
3.3.1. Treatment Patterns
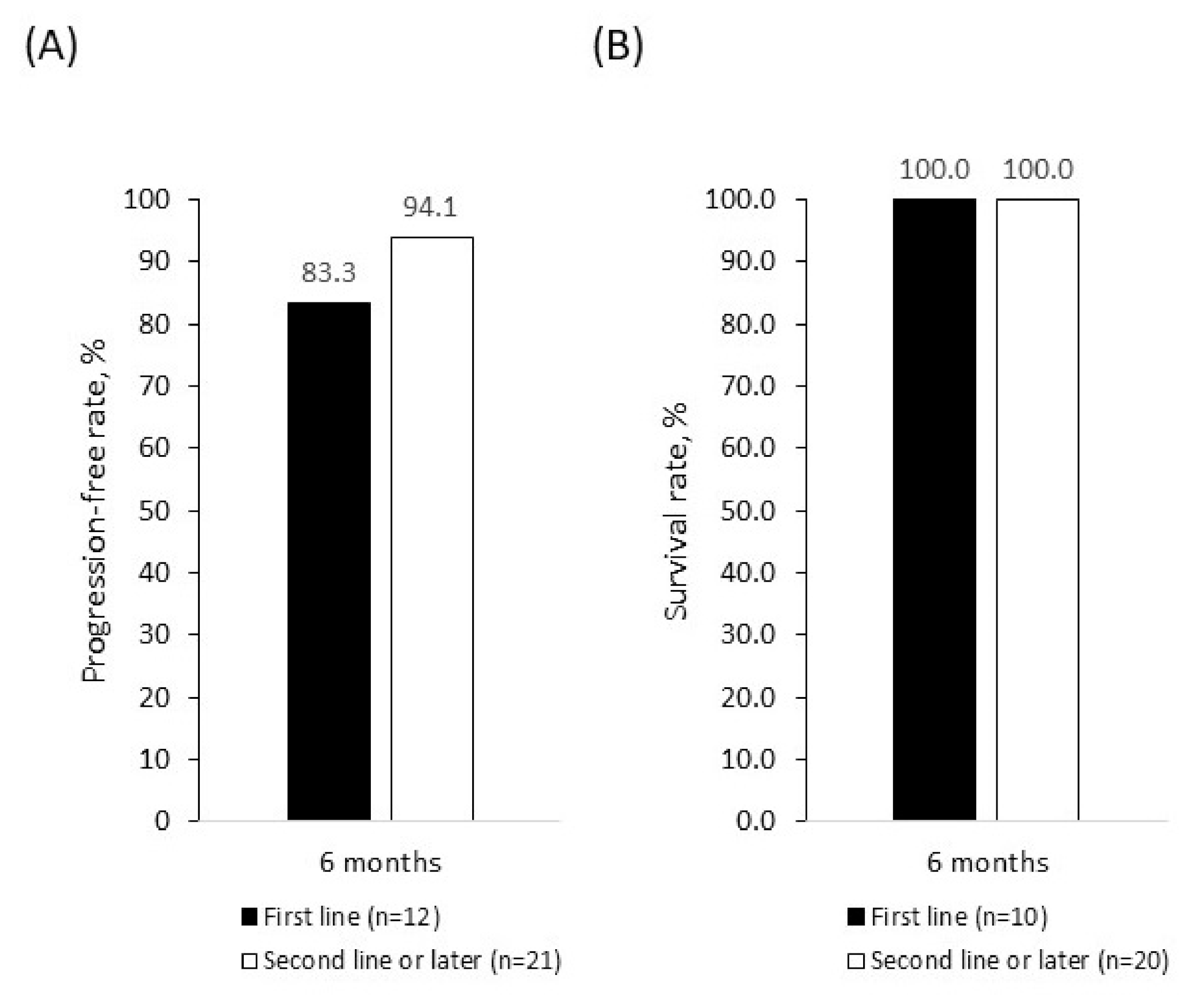
3.3.2. Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brenner, D.R.; Weir, H.K.; Demers, A.A.; Ellison, L.F.; Louzado, C.; Shaw, A.; Turner, D.; Woods, R.R.; Smit, L.M. Projected estimates of cancer in Canada in 2020. CMAJ 2020, 192, E199–E205. [Google Scholar] [CrossRef] [PubMed]
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2019; Canadian Cancer Society: Toronto, ON, Canada, 2019; Available online: https://cancer.ca/Canadian-Cancer-Statistics-2019-EN (accessed on 5 August 2020).
- American Cancer Society. Cancer Stat Facts: Female Breast Cancer. 2019. Available online: https://seer.cancer.gov/statfacts/html/breast.html (accessed on 5 August 2020).
- Seung, S.J.; Traore, A.N.; Pourmirza, B.; Fathers, K.E.; Coombes, M.; Jerzak, K.J. A population-based analysis of breast cancer incidence and survival by subtype in Ontario women. Curr. Oncol. 2020, 27, e191–e198. [Google Scholar] [PubMed]
- Fallahpour, S.; Navaneelan, T.; De, P.; Borgo, A. Breast cancer survival by molecular subtype: A population-based analysis of cancer registry data. CMAJ Open 2017, 5, E734–E739. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology Breast Cancer (version 3.2020). 2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 5 August 2020).
- Ballinger, T.J.; Meier, J.B.; Jansen, V.M. Current landscape of targeted therapies for hormone-receptor positive, HER2 negative metastatic breast cancer. Front. Oncol. 2018, 8, 308. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada. Regulatory Decision Summary—IBRANCE—Health Canada. 2016. Available online: https://hpr-rps.hres.ca/reg-content/regulatory-decision-summary-detail.php?linkID=RDS00082 (accessed on 5 August 2020).
- Government of Canada. Regulatory Decision Summary—IBRANCE—Health Canada. 2017. Available online: https://hpr-rps.hres.ca/reg-content/regulatory-decision-summary-detail.php?linkID=RDS00261 (accessed on 5 August 2020).
- Pfizer Canada ULC. Product Monograph Including Patient Medication Information; IBRANCE; Pfizer: Kirkland, QC, Canada, 2020; Available online: https://www.pfizer.ca/sites/default/files/202001/Ibrance_PM_234582_24_Jan_2020_E.pdf (accessed on 5 August 2020).
- Finn, R.S.; Crown, J.P.; Ettl, J.; Schmidt, M.; Bondarenko, I.M.; Lang, I.; Pinter, T.; Boer, K.; Patel, R.; Randolph, S.; et al. Efficacy and safety of palbociclib in combination with letrozole as first-line treatment of ER-positive, HER2-negative, advanced breast cancer: Expanded analyses of subgroups from the randomized pivotal trial PALOMA-1/TRIO-18. Breast Cancer Res. 2016, 18, 67. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.C.; Ro, J.; Andre, F.; Sherene, L.; Verma, S.; Iwata, H.; Harbeck, N.; Loibl, S.; Huang Bartlett, C.; Zhang, K.; et al. Palbociclib in hormone-receptor-positive advanced breast cancer. N. Engl. J. Med. 2015, 373, 209–219. [Google Scholar] [CrossRef] [PubMed]
- DeMichele, A.; Cristofanilli, M.; Brufsky, A.; Liu, X.; Mardekian, J.; McRoy, L.; Layman, R.M.; Rugo, H.S.; Finn, R.S. P1-19-02: Overall survival for first-line palbociclib plus letrozole vs letrozole alone for HR+/HER2- metastatic breast cancer patients in US real-world clinical practice. In Proceedings of the San Antonio Breast Cancer Symposium, San Antonio, TX, USA, 10–14 December 2019. [Google Scholar]
- Waller, J.; Mitra, D.; Mycock, K.; Stokes, G.T.; Milligan, G.; Zhan, L.; Iyer, S. Real-world treatment patterns and clinical outcomes in patients receiving palbociclib for hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced or metastatic breast cancer in Argentina: The IRIS study. J. Glob. Oncol. 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Stokes, G.; Mitra, D.; Waller, J.; Gibson, K.; Milligan, G.; Iyer, S. Treatment patterns and clinical outcomes among patients receiving palbociclib in combination with an aromatase inhibitor or fulvestrant for HR+/HER2-negative advanced/metastatic breast cancer in real-world settings in the US: Results from the IRIS study. Breast 2019, 43, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Stokes, G.; Zhan, L.; Mycock, K.L.; Milligan, G.; Ghale, A.; Mitra, D. 177P Real world treatment patterns and clinical outcomes associated with palbociclib combination therapy in Germany: Results from the IRIS study. Ann. Oncol. 2020, 31, S79–S80. [Google Scholar] [CrossRef]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Ah Im, S.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and letrozole in advanced breast cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef] [PubMed]
- Cristofanilli, M.; Turner, N.C.; Bondarenko, I.; Ro, J.; Ah Im, S.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): Final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016, 17, 425–439. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Clinical Outcome | Definition/Variables |
|---|---|
| Clinical response | |
| Complete response | Where “complete response” has been recorded at any time (no 24-week minimum). |
| Partial response | Where “partial response” has been recorded at any time (no 24-week minimum). |
| Stable disease ≥24 weeks | Patient remained on palbociclib for a minimum of 24 weeks, without complete or partial response, death, treatment switch, or progression. |
| Stable disease <24 weeks | Stable disease recorded for initial response, with a subsequent progression recorded within <24 weeks or treatment switch for reason other than progression within <24 weeks or death without recorded progression within <24 weeks. |
| Progressive disease | Progressive disease recorded for initial response without a subsequent partial or complete response recorded. |
| Derived clinical endpoints | |
| Objective response rate | Proportion of patients achieving a complete or partial response as assessed by the physician and reported in the patient records; radiologic confirmation was not required and no criteria to re-evaluate were provided. |
| Clinical benefit rate | Proportion of patients who achieved a complete or partial response or had stable disease for ≥24 weeks as assessed by the physician. |
| Progression-free rate | Proportion of patients with no evidence of progression or death at 6, 12, 18, and 24 months. |
| Survival rate | Proportion of patients alive at 6, 12, 18, and 24 months. |
| Characteristic | Overall (n = 247) | P+L (n = 214) | P+F (n = 33) |
|---|---|---|---|
| Age at palbociclib initiation, years | |||
| Mean (SD) | 61.9 (10.2) | 61.9 (10.3) | 62.3 (10.1) |
| Median (range) | 62.0 (36.0–88.0) | 63.0 (36.0–88.0) | 60.0 (41.0–85.0) |
| <65, n (%) | 139 (56.3) | 117 (54.7) | 22 (66.7) |
| ≥65, n (%) | 108 (43.7) | 97 (45.3) | 11 (33.3) |
| Ethnicity, n (%) | |||
| White/Caucasian | 178 (72.1) | 153 (71.5) | 25 (75.8) |
| Asian | 34 (13.8) | 29 (13.6) | 5 (15.2) |
| Middle Eastern | 11 (4.5) | 10 (4.7) | 1 (3.0) |
| Other | 24 (9.7) | 22 (10.3) | 2 (6.1) |
| Menopause status, n (%) | |||
| Natural menopause | 224 (90.7) | 193 (90.2) | 31 (93.9) |
| Menopause induced by surgery | 6 (2.4) | 5 (2.3) | 1 (3.0) |
| Menopause induced by LHRH suppression | 17 (6.9) | 16 (7.5) | 1 (3.0) |
| ECOG PS at palbociclib initiation, n (%) | |||
| 0 | 92 (37.2) | 83 (38.8) | 9 (27.3) |
| 1 | 108 (43.7) | 92 (43.0) | 16 (48.5) |
| 2 | 42 (17.0) | 36 (16.8) | 6 (18.2) |
| 3 | 5 (2.0) | 3 (1.4) | 2 (6.1) |
| Stage at ABC/MBC diagnosis, n (%) | |||
| Locoregionally advanced (IIIb, IIIc) | 43 (17.4) | 34 (15.9) | 9 (27.3) |
| Metastatic (stage IV) | 204 (82.6) | 180 (84.1) | 24 (72.7) |
| Occurrence of breast cancer, n (%) | |||
| Recurrent | 89 (36.0) | 61 (28.5) | 28 (84.8) |
| De novo | 158 (64.0) | 153 (71.5) | 5 (15.2) |
| Metastatic sites, n (%) | |||
| No. of patients | 204 | 180 | 24 |
| Bone | 136 (66.7) | 119 (66.1) | 17 (70.8) |
| Lung | 81 (39.7) | 75 (41.7) | 6 (25.0) |
| Lymph nodes | 62 (30.4) | 55 (30.6) | 7 (29.2) |
| Liver | 43 (21.1) | 38 (21.1) | 5 (20.8) |
| Other | 31 (15.2) | 28 (15.6) | 3 (12.5) |
| Visceral disease | 119 (58.3) | 109 (60.6) | 10 (41.7) |
| Non-visceral disease | 85 (41.7) | 71 (39.4) | 14 (58.3) |
| Prior therapy for ABC/MBC, n (%) | |||
| No. of patients | 30 | 9 | 21 |
| Endocrine therapy a | 20 (66.7) | 0 (0.0) | 20 (95.2) |
| Chemotherapy | 11 (36.7) | 9 (100.0) | 2 (9.5) |
| Targeted therapy a | 2 (6.7) | 0 (0.0) | 2 (9.5) |
| Lines of treatment for ABC/MBC, n (%) | |||
| 1 | 204 (82.6) | 193 (90.2) | 11 (33.3) |
| 2 | 34 (13.8) | 15 (7.0) | 19 (57.6) |
| 3 | 8 (3.2) | 5 (2.3) | 3 (9.1) |
| 4 | 1 (0.4) | 1 (0.5) | 0 (0.0) |
| Dose | P+L (n = 214) | P+F (n = 33) |
|---|---|---|
| Starting dose, n (%) | ||
| 125 mg/d | 193 (90.2) | 28 (84.8) |
| 100 mg/d | 17 (7.9) | 4 (12.1) |
| 75 mg/d | 4 (1.9) | 1 (3.0) |
| Reason for starting dose <125 mg/d, n (%) a | ||
| No. of patients | 21 | 5 |
| To avoid toxicity | 13 (61.9) | 5 (100.0) |
| Age | 7 (33.3) | 3 (60.0) |
| ECOG PS | 5 (23.8) | 2 (40.0) |
| Presence of comorbidities | 4 (19.0) | 0 (0.0) |
| Dose adjustment, n (%) | ||
| Dose reduction | 33 (15.4) | 4 (12.1) |
| Dose increase | 3 (1.4) | 0 (0.0) |
| Dose interruption | 2 (0.9) | 1 (3.0) |
| Cycle delay | 5 (2.3) | 0 (0.0) |
| Treatment status | ||
| Treatment ongoing | 186 (86.9) | 30 (90.9) |
| Treatment discontinued | 28 (13.1) | 3 (9.1) |
| Reason for discontinuation, n (%)b | ||
| No. of patients | 27 | 3 |
| PD following initial control/response | 12 (44.4) | 2 (66.7) |
| PD without initial control/response | 8 (29.6) | 1 (33.3) |
| Patient request | 3 (11.1) | 0 (0.0) |
| P+F | |||||
|---|---|---|---|---|---|
| Outcome | Overall (n = 247) | P+L a (n = 214) | All (n = 33) | First Line (n = 12) | Second Line or Line (n = 21) |
| Best response, n (%) | |||||
| No. of patients | 246 | 214 | 32 | 11 | 21 |
| Complete response | 26 (10.6) | 22 (10.3) | 4 (12.5) | 1 (9.1) | 3 (14.3) |
| Partial response | 171 (69.5) | 151 (70.6) | 20 (62.5) | 6 (54.5) | 14 (66.7) |
| Stable disease ≥24 weeks | 30 (12.2) | 28 (13.1) | 2 (6.3) | 1 (9.1) | 1 (4.8) |
| Stable disease <24 weeks | 3 (1.2) | 1 (0.5) | 2 (6.3) | 1 (9.1) | 1 (4.8) |
| Progressive disease | 12 (4.9) | 12 (5.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Objective response rate, n (%) | 197 (80.1) | 173 (80.8) | 24 (75.0) | 7 (63.6) | 17 (81.0) |
| Clinical benefit rate, n (%) b | |||||
| Upper bound | 231 (93.9) | 201 (93.9) | 30 (93.8) | 10 (90.9) | 20 (95.2) |
| Lower bound | 227 (92.3) | 201 (93.9) | 26 (81.3) | 8 (72.7) | 18 (85.7) |
| Progression-free rate, % c | |||||
| No. of patients | 245 | 212 | 33 | 12 | 21 |
| 6 months | 95.8 | 96.2 | 91.0 | 83.3 | 94.1 |
| 12 months | 88.7 | 90.3 | – | – | – |
| 18 months | 76.9 | 78.2 | – | – | – |
| 24 months | 76.9 | 78.2 | – | – | – |
| Survival rate, % d | |||||
| No. of patients | 240 | 210 | 30 | 10 | 20 |
| 6 months | 98.3 | 98.1 | 100.0 | 100.0 | 100.0 |
| 12 months | 95.9 | 95.6 | 100.0 | 100.0 | – |
| 18 months | 93.4 | 93.0 | 100.0 | 100.0 | – |
| 24 months | 93.4 | 93.0 | – | – | – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mycock, K.; Zhan, L.; Taylor-Stokes, G.; Milligan, G.; Mitra, D. Real-World Palbociclib Use in HR+/HER2− Advanced Breast Cancer in Canada: The IRIS Study. Curr. Oncol. 2021, 28, 678-688. https://doi.org/10.3390/curroncol28010066
Mycock K, Zhan L, Taylor-Stokes G, Milligan G, Mitra D. Real-World Palbociclib Use in HR+/HER2− Advanced Breast Cancer in Canada: The IRIS Study. Current Oncology. 2021; 28(1):678-688. https://doi.org/10.3390/curroncol28010066
Chicago/Turabian StyleMycock, Katie, Lin Zhan, Gavin Taylor-Stokes, Gary Milligan, and Debanjali Mitra. 2021. "Real-World Palbociclib Use in HR+/HER2− Advanced Breast Cancer in Canada: The IRIS Study" Current Oncology 28, no. 1: 678-688. https://doi.org/10.3390/curroncol28010066
APA StyleMycock, K., Zhan, L., Taylor-Stokes, G., Milligan, G., & Mitra, D. (2021). Real-World Palbociclib Use in HR+/HER2− Advanced Breast Cancer in Canada: The IRIS Study. Current Oncology, 28(1), 678-688. https://doi.org/10.3390/curroncol28010066