The Impact of Geography in Hepatocellular Carcinoma: A Retrospective Population Based Study


 ,
, 
Abstract
1. Background
2. Methods
2.1. Description of Study Population
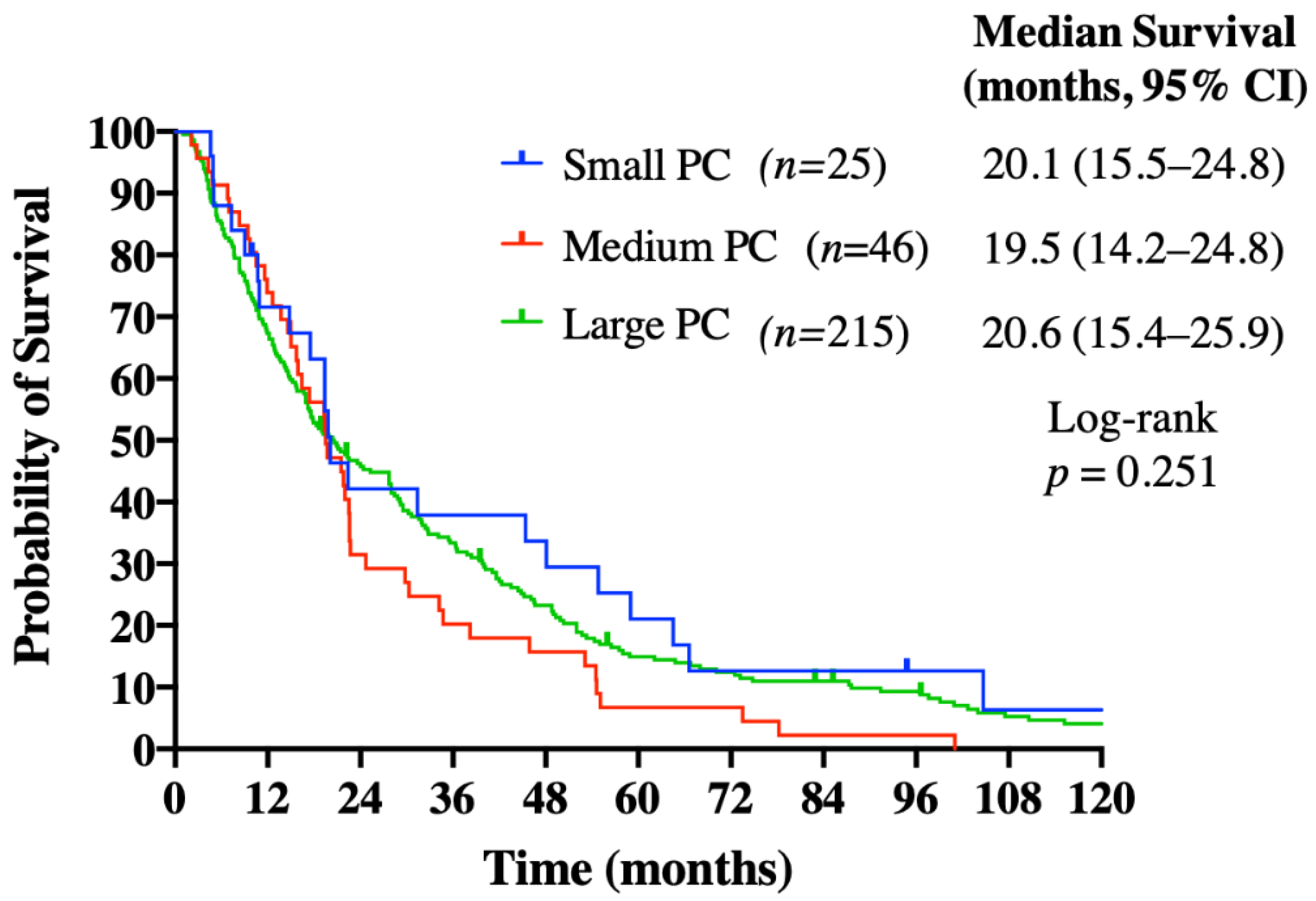
2.2. Definitions of Population Center Size/Geography
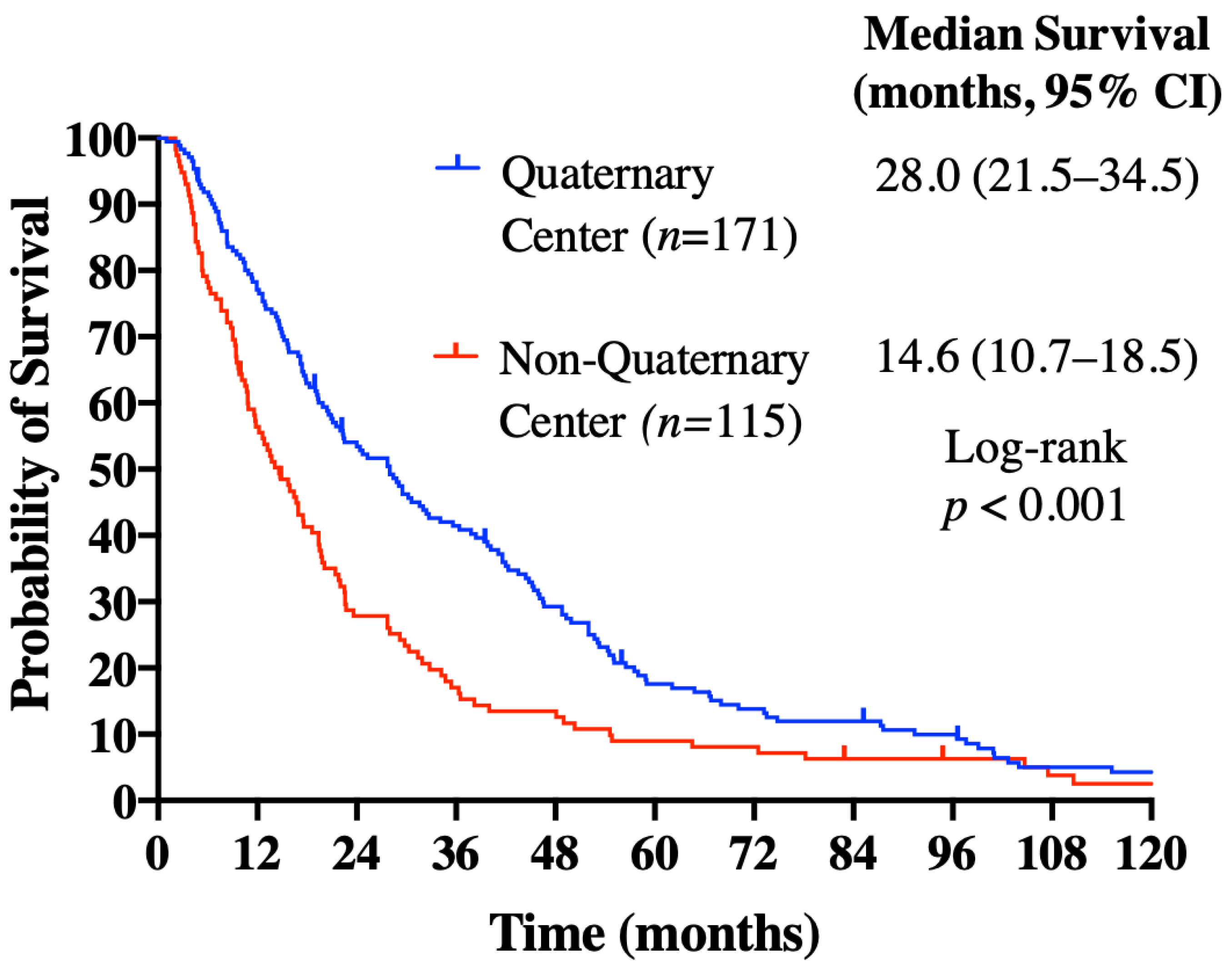
2.3. Description of Treatment Centers
2.4. Data Collection and Statistical Analyses
2.5. Ethics Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2019; Canadian Cancer Society: Toronto, ON, Canada, 2019. [Google Scholar]
- Cancer Stat Facts: Liver and Intrahepatic Bile Duct Cancer. Available online: https://seer.cancer.gov/statfacts/html/livibd.html (accessed on 1 December 2019).
- Serper, M.; Taddei, T.H.; Mehta, R.; D’Addeo, K.; Dai, F.; Aytaman, A.; Baytarian, M.; Fox, R.; Hunt, K.; Goldberg, D.S.; et al. Association of Provider Specialty and Multidisciplinary Care With Hepatocellular Carcinoma Treatment and Mortality. Gastroenterology 2017, 152, 1954–1964. [Google Scholar] [CrossRef] [PubMed]
- Sibley, L.M.; Weiner, J.P. An evaluation of access to health care services along the rural-urban continuum in Canada. BMC Heal. Serv. Res. 2011, 11, 20. [Google Scholar] [CrossRef] [PubMed]
- Census Profile, 2016 Census. Available online: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/page.cfm?Lang=E&Geo1=PR&Code1=59&Geo2=PR&Code2=01&SearchText=Canada&SearchType=Begins&SearchPR=01&B1=All&type=0 (accessed on 1 December 2019).
- Population Centre (POPCTR). Available online: https://www150.statcan.gc.ca/n1/pub/92-195-x/2011001/geo/pop/pop-eng.htm (accessed on 1 December 2019).
- Canada’s Population Estimates: Subprovincial Areas. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/190328/dq190328b-eng.htm (accessed on 1 December 2019).
- National Comprehensive Cancer Network. Hepatobiliary Cancers Version 2. 2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdf (accessed on 1 May 2020).
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Yopp, A.C.; Mansour, J.C.; Beg, M.S.; Arenas, J.; Trimmer, C.; Reddick, M.; Pedrosa, I.; Khatri, G.; Yakoo, T.; Meyer, J.J.; et al. Establishment of a Multidisciplinary Hepatocellular Carcinoma Clinic is Associated with Improved Clinical Outcome. Ann. Surg. Oncol. 2014, 21, 1287–1295. [Google Scholar] [CrossRef] [PubMed]
- Sinn, D.H.; Choi, G.-S.; Park, H.C.; Kim, J.M.; Kim, H.; Song, K.D.; Kang, T.W.; Lee, M.W.; Rhim, H.; Hyun, D.; et al. Multidisciplinary approach is associated with improved survival of hepatocellular carcinoma patients. PLoS ONE 2019, 14, e0210730. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, P.D.; Phillips, P.; Hillman, L.; Lucey, M.R.; Lee, F.; Mezrich, J.D.; Said, A. Multidisciplinary Management of Hepatocellular Carcinoma Improves Access to Therapy and Patient Survival. J. Clin. Gastroenterol. 2017, 51, 845–849. [Google Scholar] [CrossRef] [PubMed]
- Ohannessian, R.; Duong, T.A.; Odone, A. Global Telemedicine Implementation and Integration Within Health Systems to Fight the COVID-19 Pandemic: A Call to Action. JMIR Public Health Surveill. 2020, 6, e18810. [Google Scholar] [CrossRef] [PubMed]
- Shea, C.M.; Haynes-Maslow, L.; McIntyre, M.; Weiner, B.J.; Wheeler, S.B.; Jacobs, S.R.; Mayer, D.K.; Young, M.; Shea, T.C. Assessing the Feasibility of a Virtual Tumor Board Program: A Case Study. J. Health Manag. 2014, 59, 177–193. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, Y.; Li, M.; Cheng, K.; Zhao, X.; Zheng, Y.; Liu, Y.; Lei, S.; Wang, L. Long-term trends of liver cancer mortality by gender in urban and rural areas in China: An age-period-cohort analysis. BMJ Open 2018, 8, e020490. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Steckle, S.; Lui, A.; Dixon, E.; Ball, C.G.; Sutherland, F.R.; Spratlin, J.; Bathe, O.F. Effect of proximity to specialty care on outcomes for biliary cancers: A population-based retrospective cohort study. CMAJ Open 2019, 7, E131–E139. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.J.; Kim, D.; Ahmed, A.; Singal, A.K. Patients with hepatocellular carcinoma from more rural and lower-income households have more advanced tumor stage at diagnosis and significantly higher mortality. Cancer 2021, 127, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Siddique, O.; Yoo, E.R.; Perumpail, R.B.; Perumpail, B.J.; Liu, A.; Cholankeril, G.; Ahmed, A. The importance of a multidisciplinary approach to hepatocellular carcinoma. J. Multidiscip. Health 2017, 10, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-L.; Lok, A.S.-F.; Wu, P.-C.; Chan, G.C.-B.; Lin, H.-J. Doxorubicin versus no antitumor therapy in inoperable hepatocellular carcinoma. A prospective randomized trial. Cancer 1988, 62, 479–483. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Characteristics 1 | Small Urban Population Center 2 (n = 25), % | Medium Urban Population Center (n = 46), % | Large Urban Population Center (n = 215), % | p-Value | |
|---|---|---|---|---|---|
| Age | <65 | 15 (60.0) | 24 (52.2) | 109 (50.7) | 0.677 |
| ≥65 | 10 (40.0) | 22 (47.8) | 106 (49.3) | ||
| Gender | Male | 20 (80.0) | 37 (80.4) | 177 (82.3) | 0.928 |
| Female | 5 (20.0) | 9 (19.6) | 38 (17.7) | ||
| Race | Non-Asian | 24 (96.0) | 42 (91.3) | 106 (49.3) | <0.001 |
| Asian | 1 (4.0) | 4 (8.7) | 109 (50.7) | ||
| ECOG Performance Status | 0–1 | 21 (84.0) | 37 (82.2) | 176 (82.2) | 0.975 |
| 2–3 | 4 (16.0) | 8 (17.8) | 38 (17.8) | ||
| Child–Pugh Score | A | 20 (80.0) | 3 (82.6) | 200 (93.5) | 0.022 |
| B | 5 (20.0) | 8 (17.4) | 14 (6.5) | ||
| BCLC Staging at initiation of sorafenib 3 | A | 0 (0) | 0 (0) | 2 (0.9) | 0.978 |
| B | 1 (4.0) | 4 (8.7) | 14 (6.5) | ||
| C | 23 (92.0) | 41 (89.1) | 191 (88.8) | ||
| D | 1 (4.0) | 1 (2.2) | 6 (2.8) | ||
| Alpha-fetoprotein (µg/L) | <400 | 11 (47.8) | 22 (51.2) | 106 (52.5) | 0.910 |
| ≥400 | 12 (52.2) | 21 (48.8) | 96 (47.5) | ||
| Liver Disease Etiology | Hepatitis B | 1 (4.0) | 7 (15.2) | 80 (37.2) | <0.001 |
| Hepatitis C | 11 (44.0) | 18 (39.1) | 63 (29.3) | 0.180 | |
| Alcohol-associated | 11 (44.0) | 17 (37.0) | 45 (20.9) | 0.007 | |
| Metastatic Disease at Diagnosis | Yes | 15 (60.0) | 20 (43.5) | 84 (39.1) | 0.128 |
| No | 10 (40.0) | 26 (56.5) | 131 (60.9) |
| Medical or Surgical Specialty Consulted during Course of HCC Treatment | Small Urban Population Center (n = 25), % | Medium Urban Population Center (n = 46), % | Large Urban Population Center (n = 215), % | p-Value | |
|---|---|---|---|---|---|
| Hepatology | Yes | 10 (40.0) | 22 (47.8) | 134 (62.3) | 0.031 |
| No | 15 (60.0) | 24 (52.2) | 81 (37.7) | ||
| Gastroenterology | Yes | 7 (28.0) | 9 (19.6) | 67 (31.2) | 0.288 |
| No | 18 (72.0) | 37 (80.4) | 148 (68.8) | ||
| Internal medicine | Yes | 7 (28.0) | 12 (26.1) | 34 (15.8) | 0.134 |
| No | 18 (72.0) | 34 (73.9) | 181 (84.2) | ||
| Hepatobiliary surgery | Yes | 14 (56.0) | 20 (43.5) | 112 (52.1) | 0.498 |
| No | 11 (44.0) | 26 (56.5) | 103 (47.9) | ||
| General surgery | Yes | 5 (20.0) | 10 (21.7) | 28 (13.0) | 0.271 |
| No | 20 (80.0) | 36 (78.3) | 187 (87.0) | ||
| Interventional radiology | Yes | 5 (20.0) | 8 (17.4) | 56 (26.0) | 0.405 |
| No | 20 (80.0) | 38 (82.6) | 159 (74.0) |
| Liver-Directed Therapies during Course of HCC Treatment | Small Urban Population Center (n = 25), % | Medium Urban Population Center (n = 46), % | Large Urban Population Center (n = 215), % | p-Value | |
|---|---|---|---|---|---|
| Liver resection | Yes | 8 (32.0) | 11 (23.9) | 59 (27.4) | 0.761 |
| No | 17 (68.0) | 35 (76.1) | 156 (72.6) | ||
| Liver transplant | Yes | 2 (8.0) | 0 (0.0) | 7 (3.3) | 0.115 |
| No | 23 (92.0) | 46 (100.0) | 208 (96.7) | ||
| Liver ablation | Yes | 3 (12.0) | 6 (13.0) | 34 (15.8) | 0.802 |
| No | 22 (88.0) | 40 (87.0) | 181 (84.2) | ||
| Alcohol injection | Yes | 0 (0.0) | 3 (6.5) | 10 (4.7) | 0.259 |
| No | 25 (100.0) | 43 (93.5) | 205 (95.3) | ||
| Transarterial embolization | Yes | 0 (0.0) | 1 (2.2) | 10 (4.7) | 0.256 |
| No | 25 (100.0) | 45 (97.8) | 205 (95.3) | ||
| Transarterial chemoembolization | Yes | 6 (24.0) | 11 (23.9) | 92 (42.8) | 0.018 |
| No | 19 (76.0) | 35 (76.1) | 123 (57.2) | ||
| Radioembolization | Yes | 1 (4.0) | 0 (0.0) | 10 (4.7) | 0.138 |
| No | 24 (96.0) | 46 (100.0) | 205 (95.3) | ||
| Stereotactic radiation | Yes | 0 (0.0) | 0 (0.0) | 3 (1.4) | 0.423 |
| No | 25 (100.0) | 46 (100.0) | 212 (98.6) | ||
| Any liver-directed therapy | Yes | 12 (48.0) | 20 (43.5) | 137 (63.7) | 0.020 |
| No | 13 (52.0) | 26 (56.5) | 78 (36.3) |
| Hazard Ratio | 95% CI | p-Value | ||
|---|---|---|---|---|
| ECOG performance status | 0–1 | 0.417 | 0.300–0.579 | <0.001 |
| ≥2 | 1 | REF | ||
| Alpha-fetoprotein (µg/L) | <400 | 0.679 | 0.527–0.873 | 0.003 |
| ≥400 | 1 | REF | ||
| Quaternary versus non-quaternary treatment center | Quaternary | 0.652 | 0.503–0.844 | 0.001 |
| Non-quaternary | 1 | REF |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, I.S.; Liu, S.L.; Zaborska, V.; Raycraft, T.; Gill, S.; Lim, H.; Davies, J.M. The Impact of Geography in Hepatocellular Carcinoma: A Retrospective Population Based Study. Curr. Oncol. 2021, 28, 396-404. https://doi.org/10.3390/curroncol28010042
Yu IS, Liu SL, Zaborska V, Raycraft T, Gill S, Lim H, Davies JM. The Impact of Geography in Hepatocellular Carcinoma: A Retrospective Population Based Study. Current Oncology. 2021; 28(1):396-404. https://doi.org/10.3390/curroncol28010042
Chicago/Turabian StyleYu, Irene S., Shiru L. Liu, Valeriya Zaborska, Tyler Raycraft, Sharlene Gill, Howard Lim, and Janine M. Davies. 2021. "The Impact of Geography in Hepatocellular Carcinoma: A Retrospective Population Based Study" Current Oncology 28, no. 1: 396-404. https://doi.org/10.3390/curroncol28010042
APA StyleYu, I. S., Liu, S. L., Zaborska, V., Raycraft, T., Gill, S., Lim, H., & Davies, J. M. (2021). The Impact of Geography in Hepatocellular Carcinoma: A Retrospective Population Based Study. Current Oncology, 28(1), 396-404. https://doi.org/10.3390/curroncol28010042