Abstract
This scoping review aimed at reporting the outcomes of the bone lid technique in oral surgery in terms of bone healing, ridge preservation, and incidence of complications. Bone-cutting instruments and stabilization methods were also considered. PubMed, Scopus, and the Cochrane Register of Controlled Trials were searched using a combination of terms, including bone lid, bony window, piezosurgery, microsaw, cysts, endodontic surgery, impacted teeth, and maxillary sinus. A hand search was also performed. The last search was conducted on 30 November 2021. No date limitation was set. Searches were restricted to human clinical studies published in English. All types of study design were considered except reviews and case reports. After a two-step evaluation, 20 (2 randomized studies, 2 case-control studies, 3 cohort studies, 13 case series) out of 647 screened studies were included, reporting on 752 bone lid procedures. The bone lid technique was associated with favorable bone healing when compared to other methods, and with a very low incidence of major complications. Clinical indications, surgical procedures, study design, follow-up duration, and outcomes varied among the studies. Overall, favorable outcomes were reported using the bone lid approach, though evidence-based studies were scarce.
Keywords:
bone lid; bone window; bone defect; oral surgery; maxillary sinus; cyst; impacted tooth; apicoectomy 1. Introduction
The bone lid technique consists of the preparation and removal of a bone lid or window that is replaced in its original position at the end of the surgery. The aims of the technique are to achieve a valid exposure of the surgical target, to save bone otherwise lost with other more aggressive methods (ostectomy), and to improve bone healing.
This technique was firstly described for the closure following opening of the maxillary antrum and for endodontic surgical treatment of lower molars, with good results [1].
The indications for this technique were then extended to the enucleation of cysts [2,3,4] and other benign lesions [5,6]. Other applications include the extraction of deeply fractured roots or impacted teeth [7,8], the removal of fracture or failed implants [9,10], the retrieval of implants accidentally displaced into the mandibular bone marrow space [11], and inferior alveolar nerve lateralization [12]. The use of the bone lid technique is indicated for the treatment of pathologies affecting the maxillary sinus, the removal of displaced foreign bodies [13,14], and to seal the antral lateral wall for sinus lift [15]. A combination with the transnasal endoscopic approach has also been reported for the treatment of maxillary sinus pathologies [16,17].
The surgical area is usually accessed via an intraoral approach. Access to deeply impacted lower molars and large mandibular lesions has also been achieved via a submandibular incision [6,18], whose main drawbacks are the risk of facial nerve injury and aesthetic implications due to skin scars.
Precise and thin osteotomies for outlining the bony window can be obtained with both a disc microsaw [9,10] and piezosurgery [2,4,7]. Other instruments, such as traditional rotary burs [1,19], reciprocating saws [20] oscillating saws [21] or lasers [22], have been reported.
An adequate bone lid thickness, together with an optimized design characterized by thin and beveled osteotomies, facilitates the removal of the bony segment, enables its exact fit at the end of the surgery, and increases the contact area at the bone-to-bone interface, thus reducing the need for any additional means of fixation and favoring bone lid revascularization [9]. In case of lack of stability of the repositioned bone lid, various fixation methods have been described, including transcortical screws [9,23], metal [4,8] and resorbable [7,24] mini-plates and screws, sutures [14,19], wires [3], cyanoacrylate-based surgical glue [20], and resorbable pins [25].
Computed tomography (CT) and digital technologies have been applied in surgical planning, as well as in postoperative outcome assessment [4,26]. In recent years, virtual planning has allowed the design of customized surgical templates, produced by milling or through additive manufacturing, which define precise cutting planes [12,27]. The successful application of a computer-assisted intraoperative navigation system for bone lid surgery has also been reported [28].
To the best of our knowledge there is no comprehensive review on this technique, which is deemed to be of great relevance in oral surgery as a bone-saving approach. As the indications for this technique are multiple, and because we expected to find heterogeneous reports, which would be difficult to summarize into a meta-analysis, we decided to perform a scoping review. The latter, in fact, may “examine the extent, range and nature of the evidence on a topic”, and represents the best choice to “summarize findings from a body of knowledge that is heterogeneous in methods or discipline” [29].
The aim of the present scoping review was to summarize the outcomes of the bone lid technique in oral surgery, in terms of bone healing and ridge preservation, based on published evidence.
2. Materials and Methods
The present review was performed and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (http://prisma-statement.org accessed on 30 November 2021). The protocol was registered with the Open Science Framework (OSF).
2.1. Search Strategy
An electronic search was performed in the following databases: PubMed, Scopus, and the Cochrane Central Register of Controlled Trials (CENTRAL). The last search was performed on 30 November 2021. Search details are provided in Table 1. Search terms were used alone or in combination using the Boolean operators OR and AND. Furthermore, a hand search of issues up to the last issue available on 30 November 2021, including the “Early view” (or equivalent) section, was undertaken in the following journals: British Journal of Oral and Maxillofacial Surgery; Clinical Implant Dentistry and Related Research; Clinical Oral Implants Research; Implant Dentistry; International Journal of Oral and Maxillofacial Implants; International Journal of Oral and Maxillofacial Surgery; Journal of Oral and Maxillofacial Surgery; Journal of Oral Implantology; and Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology. The reference list of the retrieved reviews and of the included studies was also searched for possible additional eligible studies not identified by other search methods.

Table 1.
Search strategies for the different databases.
2.2. Inclusion Criteria
To be included, studies had to report clinical results of oral surgery procedures in which the bone lid technique was used to cover and protect the healing site in order to improve the clinical and radiographic outcome.
The search was limited to clinical studies reporting on at least 10 cases of the bone lid technique published in the English language involving human subjects. Both prospective and retrospective studies were included. The studies had to provide details on the type of clinical application, the patients’ selection criteria, the procedure for applying the bone lid, the duration of the follow-up, and the number and type of complications. They also had to provide clear definitions of the clinical and/or radiographic outcomes used to assess the success or failure of the procedure.
Publications that did not meet the above inclusion criteria and those that did not deal with original clinical cases (e.g., reviews and technical reports) were excluded. Papers in which the bone lid technique was applied in combination with maxillary sinus augmentation were excluded. Multiple publications of the same pool of patients were also excluded. When papers from the same group of authors with very similar databases of patients, materials, methods, and outcomes were identified, the authors were contacted to clarify whether the pool of patients was indeed the same. In case of multiple publications relative to consecutive phases of the same study or to enlargements of the original sample size, only the most recent data (those with the longer follow-up and the larger sample size) were considered.
2.3. Selection of the Studies
Two reviewers (G.B. and L.S.) independently screened the titles and the abstracts of the articles initially retrieved through the electronic search. The concordance between reviewers was assessed by means of the Cohen’s Kappa coefficient. In case of disagreement, a joint decision was made through discussion, or by consulting a third reviewer (M.D.F.). The full text of all studies of possible relevance were independently assessed by the same two reviewers to check if they met all inclusion criteria. For articles excluded at this stage, the reason for exclusion was recorded. The included studies were divided according to the type of clinical application: endodontic surgery, access to mandibular lesions and impacted teeth, implant explantation, access to the maxillary sinus, and other indications.
2.4. Data Charting
Data were extracted by two reviewers independently (G.B. and L.S.). Cases of disagreement were subject to joint evaluation until an agreement was reached. In case of doubts, a third reviewer was consulted (M.D.F.).
The main variables extracted from each included study were the following: study design, sample size, number of surgeons involved; patients’ genders and ages, proportion of smokers, jaw (maxilla or mandible), bone-cutting devices, fixation method, any outcome variable used to evaluate treatment success, follow-up duration, number and type of complications and time they occurred, and the quality of life of patients as well as their satisfaction, as assessed by means of questionnaires or interviews.
The following methodological parameters were also recorded: selection of participants, sample size (the risk of bias was assumed to be low, medium, or high if >50, 10–50, or <10 patients were treated, respectively), length of follow-up period (it was assumed to be low, medium, or high if the mean follow-up duration was >5 years, 1–5 years, or <1 year, respectively), dropouts (it was assumed to be low, medium, or high if dropouts were <5%, 5–15%, or >15%, respectively), measurement of the outcome, and selection of reported results.
The methodological quality of the selected studies was evaluated independently and in duplicate by two reviewers (M.D.F. and S.P.). The tool reported in the Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0 was used for RCTs [30], and a modified ROBINS-I (“Risk Of Bias In Non-randomised Studies—of Interventions”) tool was used for non-randomized studies [31]. All the criteria were assessed as low, moderate (uncertain), or high. The authors of the included studies were contacted to provide clarifications or missing information as needed. Studies were considered to have a low risk of bias (RoB) (green) if more than 2/3 of the parameters were judged as “low” and none as “high”; they were considered to have a moderate RoB (yellow) with 1 to 4 parameters judged as “low” and the rest as “moderate”, with none at high risk. All papers with at least one score at high risk were classified as having high RoB (red).
2.5. Synthesis of Results
Descriptive statistics of the included studies were recorded by summarizing the total number of patients and cases treated with the bone lid technique, as well as the postsurgical adverse events for each surgery procedure considered.
3. Results
A flowchart summarizing the screening process is presented in Figure 1. The electronic search yielded a total of 610 articles. Thirty-seven additional articles were found by hand-searching. After a first screening of the titles and abstracts, a total of 41 articles reporting results of clinical studies on patients that underwent oral surgery procedures in combination with the use of the bone lid technique were selected. After evaluation of the full-text of these articles, 21 of them were excluded [7,8,13,16,23,24,25,32,33,34,35,36,37,38,39,40,41,42,43,44,45]. The reasons for exclusion are listed in Table 2. A total of 20 studies published in the years 1984–2021 were included. The kappa values for inter-reviewer agreement were 0.95 for both the title/abstract selection and full-text articles, thus indicating an almost perfect agreement between the two independent reviewers. Since a sufficient number of homogeneous studies to be aggregated could not be found, a quantitative analysis was not undertaken.
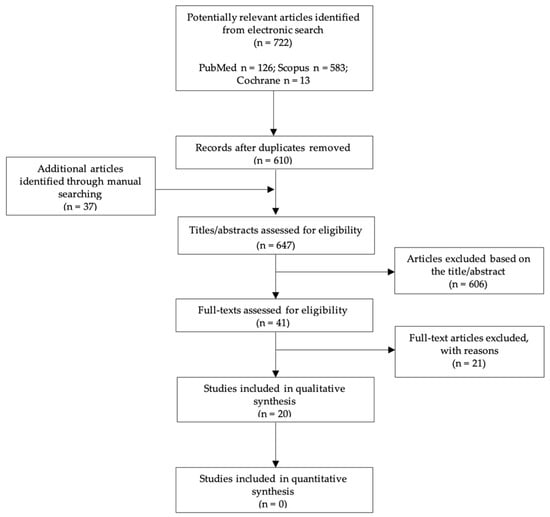
Figure 1.
Flowchart of the article selection procedure.
Table 2.
Main reasons for exclusion after full-text screening.
The main features of the included studies are shown in Table 3 (i.e., study design, clinical indication, sample size, patients’ genders and ages, jaw, number of bone lid cases, follow-up duration, osteotomy technique, and fixation method).
Table 3.
Main features of the included studies.
A total of 2 RCTs (reporting on a total of 60 bone lid patients), 2 longitudinal prospective cohort studies (218 bone lid patients), 1 retrospective cohort study (30 bone lid patients), 2 case-control studies (56 bone lid patients), and 13 case series (371 bone lid patients) were found. The included studies reported on a total of 838 patients, of which 735 were treated with the bone lid approach (752 bone lids performed).
The number of clinicians who performed the surgeries was reported in nine studies. In detail, in six studies the surgeries were carried out by a single clinician [2,9,26,47,49,50], whereas only one study involved two operators [14]. One paper reported that five clinicians performed the surgeries [3], while in another study multiple surgeons provided the treatments [56].
Only 2 out of 20 studies provided detailed information on smokers. In a randomized clinical trial comparing piezoelectric surgery to the conventional surgery (rotatory instruments) in mandibular cyst enucleation, only non-smokers were included [2]. In a retrospective cohort study, approximately one third of the included patients were smokers, and smoking habit was found to be a risk factor for bone lid necrosis (p = 0.005). Indeed, necrosis was observed only in smokers [46].
In half of the included papers, the surgical procedures were performed under local anesthesia, while in the other three articles, they were also completed in combination with conscious sedation [4,46] or general anesthesia [17,46]. In three studies, the surgeries were carried out either under general or local anesthesia [48,52,54]. The remaining four articles reported no information regarding the type of anesthesia [3,51,53,56].
As shown in Table 3, in all the included papers except one [3], details on the bone-cutting tools were provided. Piezosurgery and microsaws were the most frequently reported cutting methods. Rotary instruments, sometimes in combination with chisels, were also used to create the bony windows. The majority of neuronal complications were reported when disks and burs were utilized [1,25,47,48,54,55], whereas only one case of permanent paresthesia occurred with piezosurgery [4].
The stabilization of the bone lid was achieved without the need of rigid fixation in three studies. Bone lids were stabilized with mini-/microplates and screws in four articles, while the use of resorbable sutures was reported for all cases in four studies in the maxilla. Other fixation methods included resorbable miniplates and screws (one study). In the remaining eight articles, multiple fixation methods were reported. Bone lid resorption, necrosis, and removal were rather infrequent, as only 20 cases were found out of 752, of which 5 were in the maxilla [26,51,53] and 12 were in the mandible [1,3,4,46,48], while it was not specified in 3 cases [9]. In 5 cases out of 17, bone lid complications were clearly associated with suture stabilization or no fixation [1,48,53], 2 with rigid fixation methods [4,26], and 3 with resorbable plates [46]; whereas in 10 cases, the fixation method could not be identified [3,9,51]. In Sukegawa et al., different resorbable plates were utilized, and the osteosynthesis material was not found to be related to the bone lid necrosis [46].
The included studies were divided according to the type of surgical procedure: root-end surgery, access to mandibular lesions and impacted teeth, implant explantation, access to the maxillary sinus, and surgery for other indications. The main results of the included studies are reported in Table 4.
Table 4.
Summary of the main results of studies related to different surgical applications.
Two studies [1,55] comprising 99 bone lids reported on the use of this technique to perform root-end surgery (apicoectomy), with successful healing except in two cases (Table 4).
Six papers [2,3,4,46,47,48], including 139 bone lids, described the use of this approach to gain access to lesions, such as cysts and impacted teeth in the mandible (Table 4). An RCT comparing the bone lid with piezosurgery versus bone removal with conventional rotary instruments showed a better postoperative recovery in the bone lid group [2]. In Sivolella et al., no cyst recurrence occurred, and in the 11 cases in which it was possible to compare preoperative and 1-year follow-up CT scans, a mean volume reduction of 93.8% in the radiolucent areas was seen [4]. In a retrospective case-control study, complications were registered in 35.3% of bone lid cases, whereas no undesired effects were observed in the not repositioned group [3]. In one of these six articles, an extensive use of customized surgical guides was reported [47].
In two articles, the bone lid technique was described for the explantation of implants owing to peri-implantitis or implant fracture (see Table 4) [9,10]. Compromised implant removal was achieved in all cases, and good healing of the reimplanted bone was obtained in 153 cases out of 156 [9].
In 11 articles comprising 290 bone lids, the clinical indication was maxillary sinus access, either for the treatment of pathologies such as cysts, or for the retrieval of displaced roots or foreign bodies [14,17,26,49,50,51,52,53,54,56]. As evidenced in Table 4, a limited number of permanent complications occurred, and in a few cases, revision surgery, such as for recurrence, was needed.
In a randomized prospective study, the bony window healing was radiographically assessed 3 months after surgery in patients treated either with a bone lid as a free bone graft or with a pedicled bone lid [53]. Better results in terms of bone lid consolidation and bone density, as determined by means of CT scans, were observed in patients who received the pedicled one.
In the remaining cases (Table 4), the bone lid was applied for fractured teeth/roots and foreign body removal (29 cases), impacted tooth extraction (14 cases), inferior alveolar nerve lateralization (4 cases) [9], or for the removal of maxillary lesions [46].
Finally, in none of the included studies were patients’ quality of life and satisfaction assessed by means of questionnaires or interviews.
The RoB summary of the two included RCTs is described in Table 5. Regarding the remaining observational studies (Table 6), the majority of the studies (8 out of 18) were judged at moderate risk of bias, while 6 studies were judged to be at high risk of bias and 4 at low risk of bias.
Table 5.
Risk of bias assessment: reviewers’ judgments about each risk of bias item for each included RCT.
Table 6.
Risk of bias assessment: reviewers’ judgments about each risk of bias item for each included observational study.
4. Discussion
The present scoping review set few limitations on the sources of evidence (clinical studies with at least 10 participants and English language) in order to give an overview as inclusive as possible of bone lid applications. Despite the existence of heterogeneity and the lack of comparative studies in this field, the results of the present scoping review, which included 752 cases, showed that the bone lid is a feasible and successful technique in various types of oral surgery procedures, and is accompanied by a low incidence of major complications. Indeed, it seems to be a conservative technique that could reduce the amount of bone removal in particular circumstances, such as deeply impacted wisdom teeth, in which otherwise abundant osteotomy would be required. In addition, the success of this technique might be related to the skills and the experience of the operator, and unfortunately none of the included studies analyzed this crucial aspect.
In the largest prospective cohort study included [9], 200 consecutive patients were followed for at least 4 years. The bone lid approach was applied in conservative pre-implant and implant surgery. As a main result, 98.5% of bone lids healed without any complication, ensuring an adequate volume for the planned implant therapy, and limiting the need for supplementary regenerative procedure and bone donor sites. As also reported in Sivolella et al. [4], one of the most important factors outlined by the authors was the bone lid thickness, which is fundamental for its stabilization and revascularization [9,57,58].
When bone lid approach was reported for root-end surgery of lower molars [1,55], better access and intraoperative visibility to the endodontic lesion, associated with a reduced bone removal, were advocated. The remaining bony defect was reduced, allowing a better environment for complete healing. Overall, short-term results seemed to be as good as those reported historically for root-end surgery without a bone lid [59,60]. However, no comparative study was available.
As regards access to mandibular lesions and impacted teeth, one included RCT aimed to compare the use of the bone lid versus bone removal to gain access to alveolar bone lesions [2]. Short-term data on post-operative swelling, immediate neurological complications, and patients’ subjective response to pain were reported. The results supported the superiority of the bone lid technique. The same technique comparison was presented in a case-control study with a longer follow-up [3]. A tendency to adopt the bone lid technique for large-sized mandibular lesions, which might be considered a selection bias, was described. The critical status of those lesions probably justified the higher rate of complications in the bone lid group. It must be noted that both studies mainly focused on the comparison of piezosurgery vs. rotary instruments, rather than on the bone lid technique [2,3].
Improvements to the technique may derive by the use of computer-designed customized cutting guides, which allow for a pre-planned accurate outline of the osteotomies and, subsequently, better lid realignment and stability [47]. This approach may further improve the outcomes of the bone lid technique [12,27,38,47,61], making it more easily applicable as well. This topic should be further investigated with future RCTs comparing free-hand vs computer-guided bone lid surgery.
Partially osseointegrated failed implants (e.g., fractured or affected by peri-implantitis) are usually surgically removed with a trephine bur, thin Lindemann bur, dedicated piezosurgery inserts, or using a reverse high-torque wrench [62]. These methods may be associated with excessive bone loss or operative difficulties. When thin bone plates or deeply located implant body are present, the bone lid technique allows the surgeon to maintain the bone plate and immediately insert a new implant [9,10,63,64]. In pre-implant cases, at the time of delayed implant placement, complete re-osseointegration of the bony window and filling of the bone defect underlying the bone lid also were frequently observed, with no need for bone grafting [4,9].
The bone lid technique, eventually associated with endoscopic sinus surgery [17,41,44,49,50,65], was developed as a conservative method for the closure of the maxillary antrum [13,14,44,57,65,66,67,68]. In order to enhance its re-integration, pedicled bony windows were proposed [14,16,19,52,53,56,66]. The periosteal attachment seems to be beneficial for nourishing the osteotomized bone, as reported in one of the included RCTs [53]. In the present review, only 5 out of 290 bone lids performed to obtain access to the maxillary sinus were lost due to infection [26,50,51,53].
Thin and beveled osteotomy, which can be obtained with both a microsaw and piezosurgery, can provide an ideal self-retentive morphology of the lid, thus reducing the need for rigid fixation [4,9,10,47,53]. Piezosurgery might present potential advantages, including ease of handling and less danger in case of accidental contact with soft tissue [69]. Fixation devices such as microplates, screws, or metallic ligatures represent a stable fixation method, but may have some drawbacks, such as undesired tension on the lid, screw or plate superficialization, and patient complaints [3,4,26,50]. As a consequence, a second surgery for their removal may be necessary.
The recurrence rate was rarely described as a clear outcome [3,4,17,46,48,50]. No recurrence was reported after cyst removal bone lid surgeries. One recurrence was recorded in a study on bone lids associated with functional endoscopic sinus surgery for the treatment of a fungus ball of the maxillary sinus [17].
The results of this scoping review confirmed that the bone lid technique is associated with good outcomes, resulting in a bone-saving approach. However, the results of this review must be interpreted with caution. Among the limitations of the present review, it is worth mentioning the design of the included studies, the variety of instruments utilized, the advancements of the technologies available for both treatment planning and post-op assessment, the different surgical applications, and the short follow-up period of the majority of the studies. Despite that this technique is deemed to be influenced by the experience of the surgeon, its role has not been evaluated. In conclusion, considering the limited number of controlled trials on this topic, the low-quality evidence, and the heterogeneity of the examined clinical studies, randomized clinical trials are needed to assess the effectiveness of the bone lid technique over other approaches. Moreover, which is the most appropriate cutting tool for bone lid fashioning has not been determined so far. Similarly, the usefulness of further fixation methods in cases of well-fitted and stable bone lids is not clear. Virtual planning and the application of customized computer-designed guides might help to improve the outcomes of the technique and its reproducibility.
Author Contributions
Conceptualization, S.S., G.B., F.K., and M.D.F.; data curation, G.B., S.P., L.S., and M.D.F.; supervision, S.S., M.D.F., and F.K.; writing—original draft, S.S., G.B., and L.S.; writing—review and editing, all authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Data will be provided upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Khoury, F.; Hensher, R. The bony lid approach for the apical root resection of lower molars. Int. J. Oral Maxillofac. Surg. 1987, 16, 166–170. [Google Scholar] [CrossRef]
- Pappalardo, S.; Guarnieri, R. Randomized clinical study comparing piezosurgery and conventional rotatory surgery in mandibular cyst enucleation. J. Craniomaxillofac. Surg. 2014, 42, e80–e85. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Park, J.-H.; Paeng, J.-Y.; Kim, C.-S.; Hong, J. Comparison of surgical approach and outcome for the treatment of cystic lesion on lower jaw. J. Korean Assoc. Oral Maxillofac. Surg. 2012, 38, 276–283. [Google Scholar] [CrossRef]
- Sivolella, S.; Brunello, G.; Fistarol, F.; Stellini, E.; Bacci, C. The bone lid technique in oral surgery: A case series study. Int. J. Oral Maxillofac. Surg. 2017, 46, 1490–1496. [Google Scholar] [CrossRef]
- Savitha, K.; Cariappa, K.M. An effective extraoral approach to the mandible. A technical note. Int. J. Oral Maxillofac. Surg. 1998, 27, 61–62. [Google Scholar] [CrossRef]
- Rattan, V.; Sethi, A. Arteriovenous malformation of the mandible: Successful management by buccal window approach. Br. J. Oral Maxillofac. Surg. 2010, 48, e31–e33. [Google Scholar] [CrossRef]
- Degerliyurt, K.; Akar, V.; Denizci, S.; Yucel, E. Bone lid technique with piezosurgery to preserve inferior alveolar nerve. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, e1–e5. [Google Scholar] [CrossRef]
- Sivolella, S.; Brunello, G.; Berengo, M.; De Biagi, M.; Bacci, C. Rehabilitation with Implants after Bone Lid Surgery in the Posterior Mandible. J. Oral Maxillofac. Surg. 2015, 73, 1485–1492. [Google Scholar] [CrossRef]
- Khoury, F. The bony lid approach in pre-implant and implant surgery: A prospective study. Eur. J. Oral Implantol. 2013, 6, 375–384. [Google Scholar]
- Jung, S.R.; Bashutski, J.D.; Linebaugh, M.L. Application of modified bony lid technique to remove or replace compromised implants: Case series. Implant Dent. 2013, 22, 206–211. [Google Scholar] [CrossRef]
- Kwon, Y.D.; Pae, A. Piezoelectric Trapezoidal Osteotomy for the Retrieval of a Displaced Dental Implant in the Osteoporotic Mandibular Body. Implant Dent. 2016, 25, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Atef, M.; Mounir, M. Computer-Guided Inferior Alveolar Nerve Lateralization with Simultaneous Implant Placement: A Preliminary Report. J. Oral Implantol. 2018, 44, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Bacci, C.; Sivolella, S.; Brunello, G.; Stellini, E. Maxillary sinus bone lid with pedicled bone flap for foreign body removal: The piezoelectric device. Br. J. Oral Maxillofac. Surg. 2014, 52, 987–989. [Google Scholar] [CrossRef] [PubMed]
- Biglioli, F.; Chiapasco, M. An easy access to retrieve dental implants displaced into the maxillary sinus: The bony window technique. Clin. Oral Implants Res. 2014, 25, 1344–1351. [Google Scholar] [CrossRef]
- Sohn, D.S.; Heo, J.U.; Kwak, D.H.; Kim, D.E.; Kim, J.M.; Moon, J.W.; Lee, J.H.; Park, I.S. Bone regeneration in the maxillary sinus using an autologous fibrin-rich block with concentrated growth factors alone. Implant Dent. 2011, 20, 389–395. [Google Scholar] [CrossRef]
- Chiapasco, M.; Felisati, G.; Maccari, A.; Borloni, R.; Gatti, F.; Di Leo, F. The management of complications following displacement of oral implants in the paranasal sinuses: A multicenter clinical report and proposed treatment protocols. Int. J. Oral Maxillofac. Surg. 2009, 38, 1273–1278. [Google Scholar] [CrossRef]
- Naros, A.; Peters, J.P.; Biegner, T.; Weise, H.; Krimmel, M.; Reinert, S. Fungus Ball of the Maxillary Sinus-Modern Treatment by Osteoplastic Approach and Functional Endoscopic Sinus Surgery. J. Oral Maxillofac. Surg. 2019, 77, 546–554. [Google Scholar] [CrossRef]
- Göçmen, G.; Varol, A.; Selçuk, B.; Göker, K. Extraoral Extraction of an Impacted Molar Using Bone Lid Technique. Marmara Dent. J. 2013, 1, 42–43. [Google Scholar] [CrossRef]
- Lazaridis, N.; Tilaveridis, I.; Venetis, G.; Lazaridou, M. Maxillary sinus osteoplasty with vascularized pedicled bone flap. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 106, 828–832. [Google Scholar] [CrossRef]
- Balleri, P.; Veltri, M.; Nuti, N.; Ferrari, M. Implant placement in combination with sinus membrane elevation without biomaterials: A 1-year study on 15 patients. Clin. Implant Dent. Relat. Res. 2012, 14, 682–689. [Google Scholar] [CrossRef]
- Bayram, B.; Alaaddinoglu, E. Implant-box mandible: Dislocation of an implant into the mandible. J. Oral Maxillofac. Surg. 2011, 69, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Sohn, D.S.; Heo, J.U.; Moon, J.W.; Lee, J.H.; Park, I.S. Benefit of the replaceable bony window in lateral maxillary sinus augmentation: Clinical and histologic study. Implant Dent. 2014, 23, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco, M.; Flora, A.; Serioli, L.; Zaniboni, M. The removal of a deeply impacted lower third molar by means of the bone lid technique with piezoelectric instruments. Ital. J. Dent. Med. 2017, 2, 13–17. [Google Scholar]
- Sukegawa, S.; Kanno, T.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Masui, M.; Furuki, Y. Complications of a poly-L-lactic acid and polyglycolic acid osteosynthesis device for internal fixation in maxillofacial surgery. Odontology 2018, 106, 360–368. [Google Scholar] [CrossRef]
- Katauczek, F.; Nkenke, E.; Wagner, F.; Seemann, R. A modified bone lid for osteoplastic surgery of the maxillary sinus. Int. J. Oral Maxillofac. Surg. 2015, 44, 889–891. [Google Scholar] [CrossRef]
- Hu, Y.K.; Yang, C.; Xu, G.Z.; Xie, Q.Y. Digital design of functional surgery for odontogenic cyst intruding into maxillary sinus. Braz. J. Otorhinolaryngol. 2018, 84, 212–219. [Google Scholar] [CrossRef]
- Sivolella, S.; Brunello, G.; Fincato, A.; De Stavola, L. Computer-guided bone lid osteotomy with piezosurgery. Ann. Stomatol. 2018, 9, 84–90. [Google Scholar]
- Sukegawa, S.; Kanno, T.; Shibata, A.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Sakaida, K.; Furuki, Y. Intraoperative navigation-assisted accurate bone lid surgery to remove a mandibular lesion: A case report. Oral Maxillofac. Surg. Cases 2017, 3, 15–19. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Shuster, J.J. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. In The Cochrane Collaboration; Higgins, J.P.T., Green, S., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2011. [Google Scholar]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Aliyev, T.; Efeoglu, B.F.; Rizaj, X.; Sahin, O. Removal of the residual root and implant therapy simultaneously via bone lid approach. Niger. J. Clin. Pract. 2019, 22, 739–741. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, A.; Badiali, G.; Piersanti, L.; Marchetti, C. Computer-assisted piezoelectric surgery: A navigated approach toward performance of craniomaxillofacial osteotomies. J. Craniofac. Surg. 2015, 26, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Bovi, M.; Manni, A.; Mavriqi, L.; Bianco, G.; Celletti, R. The use of piezosurgery to mobilize the mandibular alveolar nerve followed immediately by implant insertion: A case series evaluating neurosensory disturbance. Int. J. Periodontics Restor. Dent. 2010, 30, 73–81. [Google Scholar]
- Choi, H.; Cho, G.J.; Jung, K.H.; Jeon, J.Y.; Lim, S.W.; Park, C.J.; Hwang, K.G. The dual-port endoscope-assisted cyst enucleation on the maxillofacial region. Maxillofac. Plast. Reconstr. Surg. 2021, 43, 40. [Google Scholar] [CrossRef]
- Hamdoon, Z.; Mahmood, N.; Talaat, W.; Sattar, A.A.; Naeim, K.; Qais, A.; Kheder, W.; Jerjes, W. Evaluation of different surgical approaches to remove dental implants from the maxillary sinus. Sci. Rep. 2021, 11, 4440. [Google Scholar] [CrossRef]
- Lee, S.M.; Yu, Y.H.; Wang, Y.; Kim, E.; Kim, S. The Application of “Bone Window” Technique in Endodontic Microsurgery. J. Endod. 2020, 46, 872–880. [Google Scholar] [CrossRef]
- Liu, Z.; Huang, D.; Li, K.; Li, H.; Liu, L. Precise locating and cutting of the bone lid with a digital template during the treatment of large mandibular cysts: A case series study. J. Craniomaxillofac. Surg. 2021, 49, 358–361. [Google Scholar] [CrossRef] [PubMed]
- Nordera, P.; Spanio di Spilimbergo, S.; Stenico, A.; Fornezza, U.; Volpin, L.; Padula, E. The cutting-edge technique for safe osteotomies in craniofacial surgery: The piezosurgery bone scalpel. Plast. Reconstr. Surg. 2007, 120, 1989–1995. [Google Scholar] [CrossRef] [PubMed]
- Saibene, A.M.; Collurà, F.; Pipolo, C.; Bulfamante, A.M.; Lozza, P.; Maccari, A.; Arnone, F.; Ghelma, F.; Allevi, F.; Biglioli, F.; et al. Odontogenic rhinosinusitis and sinonasal complications of dental disease or treatment: Prospective validation of a classification and treatment protocol. Eur. Arch. Otorhinolaryngol. 2019, 276, 401–406. [Google Scholar] [CrossRef]
- Scolozzi, P.; Martinez, A.; Lombardi, T.; Jaques, B. Lateral antrotomy as a surgical approach for maxillary sinus: A modified technique with free bone flap repositioning and fixation with a titanium plate. J. Oral Maxillofac. Surg. 2009, 67, 689–692. [Google Scholar] [CrossRef]
- Seo, M.-H.; Lee, J.-Y.; Frimpong, P.; Eo, M.-Y.; Kim, S.-M. Modified Endoscopic-Assisted Approach for Removal of Ectopic Third Molar in the Maxillary Sinus. Appl. Sci. 2021, 11, 8446. [Google Scholar] [CrossRef]
- Wang, Y.J.; He, Y.Y.; Zhao, S.F.; Bacci, C.; Sivolella, S.; Brunello, G.; Stellini, E. Maxillary sinus bone lid with pedicled bone flap for foreign body removal: The piezoelectric device. Br. J. Oral Maxillofac. Surg. 2015, 53, 404–405. [Google Scholar] [CrossRef] [PubMed]
- Yura, S.; Kato, T.; Ooi, K.; Izumiyama, Y. Access to the maxillary sinus using a bone flap with sinus mucosal and mucoperiosteal pedicles. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e8–e12. [Google Scholar] [CrossRef]
- Sohn, D.S.; Jung, H.S.; Kim, K.H.; Song, K.J.; An, H.W.; Min, K.H. Removal of displaced foreign body from the maxillary sinus using replaceable bony windows and saline irrigation, followed by suctioning of the foreign body. Implant Dent. 2011, 20, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Yamamoto, N.; Matsuyama, T.; Takabatake, K.; Kawai, H.; Nagatsuka, H.; Furuki, Y. Factors of successful treatment using the bone lid technique in maxillofacial surgery: A pilot study. J. Hard Tissue Biol. 2021, 30, 193–198. [Google Scholar] [CrossRef]
- Ahmed, M.; Salah, M.K.; Khairy, N. Computer-Aided Design/Computer-Aided Manufacturing Cutting Guides for Odontectomy of Deeply Impacted Mandibular Third Molars. Open Access Maced. J. Med. Sci. 2018, 6, 2395–2401. [Google Scholar] [CrossRef] [PubMed]
- Kablan, F.; Yaffe, V.; El-Naaj, I.A. The Buccal Lid Approach for Removal of Impacted Mandibular Molars—When, How and Why? Open J. Stomatol. 2017, 7, 81. [Google Scholar] [CrossRef][Green Version]
- Hu, Y.K.; Yang, C.; Zhou Xu, G.; Wang, Y.; Abdelrehem, A. Retrieval of root fragment in maxillary sinus via anterolateral wall of the sinus to preserve alveolar bone. J. Craniofac. Surg. 2015, 26, e81–e84. [Google Scholar] [CrossRef]
- Xu, G.Z.; Yang, C.; Fan, X.D.; Hu, Y.K.; Yu, C.Q. Functional surgery for the treatment of dentigerous cyst in the maxillary sinus. J. Craniofac. Surg. 2015, 26, e84–e86. [Google Scholar] [CrossRef]
- Kurokawa, H.; Takeda, S.; Yamashita, Y.; Nakamura, T.; Takahashi, T. Evaluation of a modified method for maxillary sinus surgery—Reimplantation of the anterior bony wall of the maxillary sinus. Asian J. Oral Maxillofac. Surg. 2002, 14, 144–147. [Google Scholar] [CrossRef]
- Choung, P.H.; Choung, Y.H. Vascularized bone flap for access to the maxillary sinus. J. Oral Maxillofac. Surg. 1997, 55, 832–835. [Google Scholar] [CrossRef]
- Choi, B.H.; Yoo, J.H.; Sung, K.J. Radiographic comparison of osseous healing after maxillary sinusotomy performed with and without a periosteal pedicle. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 82, 375–378. [Google Scholar] [CrossRef]
- Widmark, G.; Ekholm, S.; Borrman, H.; Grangård, U.; Holmberg, K. The use of a bone lid to close the anterior wall defect after surgery in the maxillary sinus. Swed. Dent. J. 1992, 16, 173–182. [Google Scholar] [PubMed]
- Lasaridis, N.; Zouloumis, L.; Antoniadis, K. Bony lid approach for apicoectomy of mandibular molars. Aust. Dent. J. 1991, 36, 366–368. [Google Scholar] [CrossRef]
- Lindorf, H.H. Osteoplastic surgery of the sinus maxillaris--the “bone lid”-method. J. Maxillofac. Surg. 1984, 12, 271–276. [Google Scholar] [CrossRef]
- Lindorf, H. Knochendeckelverschluss nach oraler Kieferhoehleneroffnung. Dtsch. Zhanaertl. Z. 1974, 29, 587–590. [Google Scholar]
- Lindorf, H. Tierexperimentelle Untersuchungen zur osteo plastischen Kieferhöhlenoperation (Knochendeckelmethode). Dtsch. Z. Mund Kiefer Gesichtschir. 1983, 7, 378–383. [Google Scholar]
- Lieblich, S.E. Endodontic surgery. Dent. Clin. N. Am. 2012, 56, 121–132. [Google Scholar] [CrossRef]
- Setzer, F.C.; Shah, S.B.; Kohli, M.R.; Karabucak, B.; Kim, S. Outcome of endodontic surgery: A meta-analysis of the literature--part 1: Comparison of traditional root-end surgery and endodontic microsurgery. J. Endod. 2010, 36, 1757–1765. [Google Scholar] [CrossRef]
- Hu, Y.K.; Xie, Q.Y.; Yang, C.; Xu, G.Z. Computer-designed surgical guide template compared with free-hand operation for mesiodens extraction in premaxilla using “trapdoor” method. Medicine 2017, 96, e7310. [Google Scholar] [CrossRef]
- Stajčić, Z.; Stojčev Stajčić, L.J.; Kalanović, M.; Đinić, A.; Divekar, N.; Rodić, M. Removal of dental implants: Review of five different techniques. Int. J. Oral Maxillofac. Surg. 2016, 45, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Khoury, F.; Antoun, H.; Missika, P. Bone Augmentation in Oral Implantology; Quintessence Publishing: Hanover Park, IL, USA, 2007. [Google Scholar]
- Lee, S.C.; Jeong, C.H.; Im, H.Y.; Kim, S.Y.; Ryu, J.Y.; Yeom, H.Y.; Kim, H.M. Displacement of dental implants into the focal osteoporotic bone marrow defect: A report of three cases. J. Korean Assoc. Oral Maxillofac. Surg. 2013, 39, 94–99. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nogami, S.; Yamauchi, K.; Tanuma, Y.; Odashima, K.; Matsui, A.; Tanaka, K.; Takahashi, T. Removal of dental implant displaced into maxillary sinus by combination of endoscopically assisted and bone repositioning techniques: A case report. J. Med. Case Rep. 2016, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Biglioli, F.; Goisis, M. Access to the maxillary sinus using a bone flap on a mucosal pedicle: Preliminary report. J. Craniomaxillofac. Surg. 2002, 30, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Tilaveridis, I.; Lazaridou, M.; Dimitrakopoulos, I.; Lazaridis, N.; Charis, C. Displacement of three dental implants into the maxillary sinus in two patients. Report of two cases. Oral Maxillofac. Surg. 2012, 16, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Tsodoulos, S.; Karabouta, I.; Voulgaropoulou, M.; Georgiou, C. Atraumatic removal of an asymptomatic migrated dental implant into the maxillary sinus: A case report. J. Oral Implantol. 2012, 38, 189–193. [Google Scholar] [CrossRef]
- Vercellotti, T.; De Paoli, S.; Nevins, M. The piezoelectric bony window osteotomy and sinus membrane elevation: Introduction of a new technique for simplification of the sinus augmentation procedure. Int. J. Periodontics Restor. Dent. 2001, 21, 561–567. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).