Case Report
A 55-year-old man who presented with a history of atypical angina during the last five years, felt left sided epigastric pain after eating but not during physical or emotional stress. Cardiovascular risk factors included smoking, hypertension, hypercholesterolaemia and a family history for premature coronary artery disease. Physical examination revealed an obese patient (BMI 36 kg/m2) in no acute distress. Blood pressure was 154/80 mm Hg, pulse 72 bpm. Cardiac exam disclosed a 2/6 holosystolic murmur at the lower left sternal border. No signs of congestion were evident. The ECG showed sinus rhythm and no ST/T abnormalities. Chest X-ray was within normal limits. On treadmill exercise test, the patient remained asymptomatic and was able to exercise 160 Watt. However, there was a horizontal ST-segment depression in lead V6. The subsequent coronary angiography demonstrated severe three vessel disease with chronic occlusion of the left anterior descending and the circumflex coronary artery and a 75% stenosis in the right coronary artery. There was evidence of mitral regurgitation. Echocardiography showed normal left and right ventricular dimensions with preserved left ventricular ejection fraction. There was a moderate mitral regurgitation due to a cleft between the second (P2) and the third (P3) posterior mitral valve leaflet (Figure 1). In addition, there was a prolapse of the anterior leaflet. There was no atrial enlargement and right ventricular pressure was within normal limits. The patient was operated with CABG and the cleft in the posterior mitral leaflet was sutured (Figure 2). The rim of the prolapsing A3 leaflet was fixed with artificial chordae and a 30 mm mitral annuloplasty ring was placed.
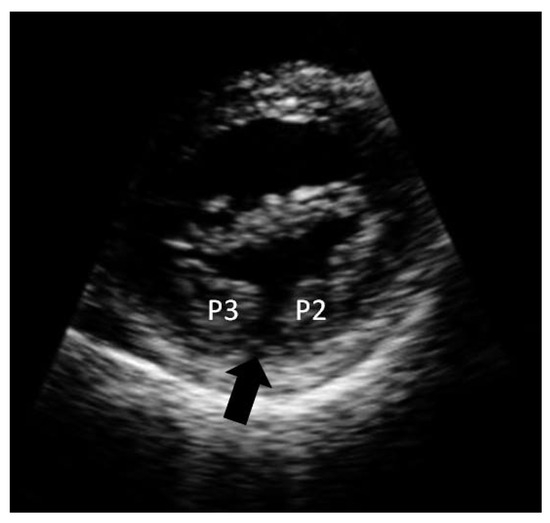
Figure 1.
Short axis view showing the cleft (black arrow) between the second (P2) and the third (P3) posterior mitral valve segment.
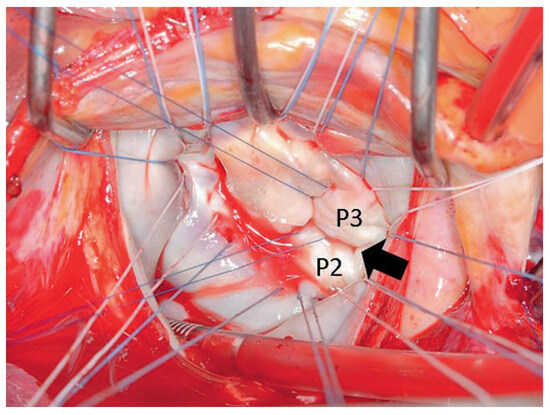
Figure 2.
Surgeons view with the anterior leaflet in the top left corner, below the posterior leaflet with the cleft (black arrow) between segments P2 and P3.
Cleft mitral valve is a relatively uncommon entity and the anterior leaflet is almost always involved [1]. Clefts in the anterior leaflet may occur in patients with otherwise normal hearts as well as in patients with atrioventricular septal defects [2]. Clefts in the posterior mitral valve leaflets are very rare and only a few cases have been reported in literature [3,4]. Treatment options in patients with relevant mitral regurgitation range from surgical reconstruction to mitral valve replacement. In our patient, the cleft was sutured, the prolapsing anterior leaflet was fixed and a 30 mm annuloplasty ring was inserted. Postoperative echocardiography showed mild residual mitral regurgitation. The patient was discharged for rehabilitation seven days after the operation.
Conflicts of Interest
There is no conflict of interest.
References
- Di Segni, E.; Edwards, J.E. Cleft anterior leaflet of the mitral valve with intact septa: a study of 20 cases. Am J Cardiol. 1983, 51, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Sigfússon, G.; Ettedgui, J.A.; Silverman, N.H. , et al. Is a cleft in the anterior leaflet of an otherwise normal mitral valve an atrioventricular canal malformation? J Am Coll Cardiol. 1995, 26, 508–515. [Google Scholar] [CrossRef] [PubMed][Green Version]
- McDonald, R.W.; Ott, G.Y.; Pantely, G.A. Cleft in the anterior and posterior leaflet of the mitral valve: a rare anomaly. J Am Soc Echocardiogr. 1994, 7, 422–424. [Google Scholar] [CrossRef] [PubMed]
- Kent, S.M.; Markwood, T.T.; Vernalis, M.N.; Tighe, J.F., Jr. Cleft posterior mitral valve leaflet associated with counterclockwise papillary muscle malrotation. J Am Soc Echocardiogr. 2001, 14, 303–394. [Google Scholar] [CrossRef] [PubMed]
© 2009 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.