Abstract
Geranylgeraniol (GG), an ingredient extracted from the South American annatto plant, has been shown to benefit bone and muscle health, is crucial in the biosynthesis of menaquinone-4 and coenzyme Q10, and has pain and inflammation reduction activities. However, no known studies to date have demonstrated the safety and impact of GG supplementation in humans. This 8-week, randomized, placebo-controlled, dose-escalated trial was conducted to determine the effect of GG on blood safety and hormone markers in healthy adults. Sixty-six males and females between 30 and 49 years of age were supplemented with either GG or a placebo (PLA) for 8 weeks, with dose escalation from 150 mg to 300 mg occurring after 4 weeks in the treatment group. Changes in complete blood count and comprehensive metabolic panels were analyzed for whole study groups (males and females) while changes in sex hormone panels were analyzed for males and females independently. There were no significant changes in complete blood count, comprehensive metabolic panel, progesterone, estradiol, sex–hormone binding globulin, or dihydrotestosterone (p > 0.05). An exploratory analysis of testosterone levels in a subgroup of males with baseline (Pre) total testosterone < 700 ng/dL (GG = 15; PLA = 13) demonstrated a significant increase (p < 0.05) from Pre to Week 8 in total-, free-, and bioavailable testosterone (+7.5%, +15.0%, and +14.8%, respectively). This study demonstrates that GG does not significantly change the composition of blood chemistry, hematology, or sex hormone profiles in adult males or females. Given the effects observed in the exploratory analysis in a subgroup of males, GG supplementation may be beneficial for testosterone enhancement in male populations subject to low testosterone (i.e., aging males and those with late-onset hypogonadism), but further research is needed.
1. Introduction
A pigment extract known as annatto is made from the tropical South American plant Bixa orellana (also known as achiote) [1,2]. An important oily component of annatto seeds and food color extracts, geranylgeraniol (GG), makes up about 1% of the dry seeds [3,4,5,6].
While GG can be consumed exogenously, its primary source in humans is endogenous synthesis via the mevalonate pathway, an ancient pathway that has been well-preserved through evolutionary processes in both prokaryotes and eukaryotes. This pathway is responsible for the production of isoprenoids, which constitute some of the earliest known natural products, such as quinones, sterols, carotenoids, and hormones [7,8]. As such, the products of the mevalonate pathway have been long understood to have significant influences on health and vitality in humans [9].
Previous studies have reported the potential health benefits of GG supplementation to include anti-inflammatory and antinociceptive properties as well as functions for bone and muscle health. Moreover, GG acts as an essential building block for vitamin K2 (menaquinone-4) and CoQ10 [10] and, thus, may be associated with the health benefits of each molecule. The annatto plant, with GG as its active ingredient, has been used in ancient medicine as a cardiotonic, hypotensive, antibiotic, and anti-inflammatory aid [11,12], and more contemporary research has suggested GG has positive effects on glucose regulation, bone health, and the gut microbiome [13]. Recent research has also endeavored to explain the relationship between GG and another mevalonate pathway end product: steroid hormones [4].
Previous breakthroughs have been made in understanding the relationship between GG and testosterone [4,14]. The findings revealed that GG can stimulate testosterone production in Leydig cells. These cells play a crucial role in regulating testosterone production, which is essential for male reproductive system development and sexual function in fetuses [15]. Insufficient testosterone levels can lead to infertility and sexual dysfunction, causing late-onset hypogonadism (LOH) in men common in aging populations [16,17,18,19]. Low testosterone levels may also foretell the onset of type 2 diabetes mellitus [20] and increased cardiovascular risk [21,22]. Hence, sufficient testosterone levels are relevant in preserving general health. However, the current treatment for LOH is testosterone replacement therapy and the long-term health effects of testosterone administration are controversial [23]; consequently, alternative natural methods of testosterone enhancement are of considerable interest.
An animal study established the safety and toxicological profiles of GG, deeming it safe for human use at ~400 mg/day for the average person [5]. However, this trial represents the first step in building a safety profile in humans. GG was administered to both males and females at doses of 150 mg and 300 mg for 4 weeks each in a dose escalation manner to evaluate safety via assessment of hematological variables. In addition, given the potential of GG to impact endocrinology, sex hormone profiles were also examined.
2. Materials and Methods
2.1. Study Design and Protocol
This study was carried out at a single study site (Applied Science and Performance Institute; Tampa, FL, USA) in a randomized, double-blind, placebo-controlled, dose-escalation, parallel manner. The protocol was approved by an external Institutional Review Board (IRB) (Advarra; Columbia, MD, USA; Protocol #122102) and was registered with clinicaltrials.gov (ID: NCT05258513) (https://clinicaltrials.gov/study/NCT05258513 (accessed on 4 February 2022)). Before engaging in any study procedures, participants signed an IRB-approved informed consent form for study participation. All the participants visited the laboratory for medical history screening to confirm eligibility based on the criteria described in the following section. The participants were randomly assigned to one of the two possible study conditions using a block design via randomizer.org (accessed on 4 February 2022) (Social Psychology Network, Middletown, CT, USA), with one group supplementing with a soft-gel capsule of geranylgeraniol (GG; trans-Geranylgeraniol GG-Gold®; American River Nutrition LLC, Hadley, MA, USA) and one group supplementing with a visually identical placebo (PLA). Per soft-gel capsule, the GG supplement contained 150 mg of active GG, while the inactive components of the soft-gel capsule consisted of bone gelatin, purified water, glycerin, and carob in glycerin with caramel. The PLA supplement contained olive oil, bone gelatin, purified water, glycerin, and carob in glycerin with caramel.
Following the condition allocation, the participants underwent baseline testing (Pre), which included blood sample donation to assess hormone markers and a full blood safety panel in both groups. Following Pre, participants were given their respective conditions to begin supplementation. For the first 4 weeks, participants in GG were given bottles labeled “AM” and “PM” and instructed to orally consume one soft-gel capsule from “AM” in the morning, and one soft-gel capsule from “PM” in the evening, both with food. In the first 4 weeks, the “AM” bottle was the inactive ingredient (mimicking PLA), and the “PM” bottle was active (150 mg of GG from 210 mg trans-Geranylgeraniol GG-Gold®). In the final 4 weeks, following a retest in an identical manner to Pre, participants in GG were given the same labeled bottles and instructed to consume the supplement similarly to the first 4 weeks. However, the active ingredient was in both bottles for a total of 300 mg of active GG per day. The rationale for the study dosing of 150 mg and 300 mg was to assess a dose-response that was based on approximate human equivalent doses from animal studies [13,24,25,26]. The participants in PLA were instructed to orally consume one soft-gel capsule in the morning from the “AM” and one soft-gel capsule in the evening from the “PM”, both with food, for the duration of the 8 weeks. Participants were retested at the end of week 8 for all measures. Figure 1 displays a chevron chart to complement the understanding of the study progression. At the Wk4 and Wk8 time points, participants returned their bottles for measurement of supplement compliance. Supplement compliance was determined to be 96% and 95% for GG and PLA, respectively, and all the participants included in the study analysis had a compliance rate of >80%. Throughout the supplementation period, subjects were instructed to maintain their current nutritional intakes and activity levels to mitigate any covariate effects.

Figure 1.
Study Process.
2.2. Study Participants
Male and female participants, aged 30 to 49 years, were recruited by word of mouth, email contact, and direct contact from the greater Tampa Bay Area. Participants were excluded from the study if they: had any diagnosis of cardiovascular, neurological, metabolic, or endocrine disease; drank heavily (>7 and >14 drinks per week for women and men, respectively); smoked; had any renal, hematological, or hepatic disorder; had any psychiatric disorder, depression; had a peptic ulcer; had any malignancy; had thrombosis; had recently undergone surgery that affects digestion and absorption; were hypo- or hypertensive; were currently undergoing hormone replacement therapy; currently using hormone boosting supplements (herbal or synthetic); currently using drugs that are anti-diabetic, anti-platelet, anti-coagulant, beta blockers, or used to treat erectile dysfunction (ED); were pregnant or trying to conceive, currently breastfeeding, or have breastfeed within the prior 3 months; or have participated in a clinical trial within the past 6 months.
For sample size estimation, an a priori power analysis (G*Power, version 3.0.10) was performed with the given α, power, and effect size values [27]. The test family was set as an F-test, and the statistical test selected was a repeated measures analysis of variance (ANOVA) within-between interaction with the following parameters: α = 0.05, 1 − β = 0.80, effect size f = 0.18, number of groups = 2, number of measurements = 2, correlation among repeated measures 0.5, and nonsphericity correction epsilon = 1. The effect size f value of 0.18 was determined directly in the G*power software (version 3.0.10) from a partial η2 value of 0.03 which was used as a conservative estimate between the small (0.01) and medium (0.06) benchmarks provided by Cohen [28]. The resulting total sample size estimation was 66. To account for potential dropouts, a buffer of +20% was applied to the total sample size estimate. A total of 83 participants were randomly assigned to the two possible study conditions. Following dropouts, a total of 66 participants (GG = 34, PLA = 32) completed the trial and were used for study analysis (Figure 2). The descriptive characteristics of the participants are noted in Table 1.
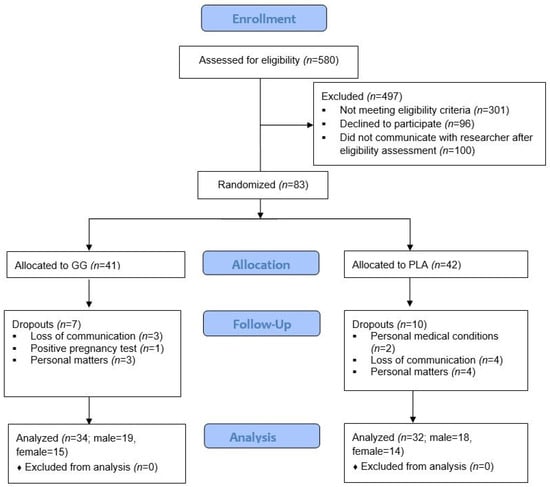
Figure 2.
CONSORT Flow Diagram.

Table 1.
Baseline Descriptive Characteristics.
2.3. Blood Biochemistry
Participants arrived at the laboratory for Pre, Wk4, and Wk8 blood donation following an overnight fast (~10 h). Venous blood was extracted via standard sterile venipuncture of the antecubital vein by a certified phlebotomist using a 21-gauge syringe and collected into 2 vials (1) an 8.5 mL gel-barrier, marble top tube interiorly coated with silicone (BD Vacutainer®, SST™, Becton, Dickinson, and Company, Franklin Lakes, NJ, USA) and (2) a 5 mL lavender top EDTA vacutainer tube (BD Vacutainer®, Becton, Dickinson and Company, Franklin Lakes, NJ, USA). Afterward, the gel-barrier tubes were inverted 6–8 times and allowed to clot for approximately 30 min at 4 °C. Gel-barrier tubes were then centrifuged at 1665× g for 15 min at 4 °C and the resulting serum samples aliquoted and stored at −80 °C until the further analysis for comprehensive metabolic panel and hormone panel which included progesterone, estradiol, sex hormone binding globulin (SHBG), total testosterone, free testosterone, and bioavailable testosterone. All serum samples were thawed once and analyzed in duplicate in the same assay for each analysis to avoid compounded inter-assay variance. Whole blood samples were collected into the lavender top EDTA vacutainers tubes that were inverted 6–8 times, stored at 4 °C, and analyzed within 3 days of collection for a standard complete blood count analysis. All samples were sent to a local Labcorp (Laboratory Corporation of America Holdings) for analysis.
2.4. Adverse Events
Participants were asked to report any adverse events on each visit in terms of incidences of headache, dizziness, nausea, vomiting, heart palpitations, trouble swallowing pills, lethargy, memory loss, cramps, chest pain, wheezing, ear pain, indigestion, blood in urine, blood in stool, ringing in ears, lethargy, swelling, and itching. In addition, participants were instructed to report any adverse events immediately to the researcher via email to begin the documentation process. Further, in the event that any severe adverse events were to have occurred, such as a life-threatening event, hospitalization, disability, or permanent damage; then, the investigators would have immediately informed the sponsor and stopped the study. The frequency of an adverse event was defined as how many participants reported either, no adverse effects (0), reported an adverse event one time throughout the study (1), or if the adverse event was reported twice by a participant throughout the study (2). Severity was defined as follows: no adverse event (0), the adverse event was mild (1), the adverse event was moderately severe (2), or the adverse event was severe (3).
2.5. Statistical Analysis
Before carrying out inferential statistics, data were screened for outliers and normality. Visual inspection of box plots was used as a graphical method for screening outliers. Quantitatively, outliers were screened by examination of the studentized residuals whereby values ±3 SD were considered outliers. Normality was graphically assessed through visual inspections of Q-Q plots and then confirmed through Shapiro-Wilk testing (p > 0.05). Following outlier and normality testing, dependent variables were scrutinized using a two-way mixed modal analysis of variance (ANOVA) with the group as the “between-group” factor (GG and PLA), time as the “within-group” factor (Pre, Wk4, and Wk8), and participants as the random factor. Whenever a significant F-value was obtained, post hoc testing was performed with a Bonferroni correction for multiple comparison purposes. For ANOVA procedures, homogeneity of variances and covariances were confirmed by Levene’s test and Box’s M test, respectively. Additionally, Mauchly’s test of sphericity was used to test the assumption of sphericity for two-way interactions. If sphericity was violated the Greenhouse-Geisser correction was used. For all analyses, the alpha level was set a priori p < 0.05. Data are presented as a mean ± standard deviation unless otherwise stated.
2.6. Exploratory Analysis
Testosterone treatment is most commonly targeted for men in the lower range of the reference values for testosterone or men who are hypogonadal. Therefore, we sought to investigate in an exploratory analysis if levels of testosterone in participants had any impact on the efficacy of GG treatment. For this male analysis, we used the total testosterone normal reference range values of 280 to 1100 ng/dL to form quartiles. Specifically, the difference in the minimum and maximum values of the reference range is 820 ng/dL, dividing this difference by 4 for quartile separation yields 205 ng/dL. Taking the minimum value of the reference range (280 ng/dL) and adding 205 ng/dL formed the upper limit of the first quartile (485 ng/dL) and 205 ng/dL was added to 485 ng/dL to form the upper limit of the second quartile and so on. Thus, the resulting quartiles are as follows: Q1 = 485 ng/dL and below, Q2 = 486 to 691 ng/dL, Q3 = 692 to 897 ng/dL, Q4 = 898 ng/dL and above. To have a round cutoff males with baseline (Pre) total testosterone levels < 700 ng/dL were excluded from this analysis, to focus on participants in the lower quartile ranges. The sample size was 15 in GG and 13 in PLA. A two-way mixed model ANOVA was carried out to assess significant main effects and interaction effects for total, free-, and bioavailable testosterone assuming group as a between-group factor, time as a within-group factor, and subject as a random factor. This model was applied to all three study time points (Pre, Wk4, Wk8) and repeated only considering Wk4 and Wk8 and again only considering Pre and Wk8. Cohen’s d effect size was calculated and values were interpreted as 0–0.2 (trivial), 0.2–0.5 (small), 0.5–0.8 (moderate), and >0.8 (large) [28]. We also analyzed female testosterone data, applying the same method with the reference range for adult females of 10 to 75 ng/dL [29]. This established a Q2 upper limit of 43 ng/dL, which would only eliminate one female from the sample. Utilizing the median of the female sample (22 ng/dL) as the threshold produced a sample of n = 9 for GG and n = 7 for PLA and no significant statistical effects were observed for testosterone-related markers (Supplementary Tables S1–S3).
3. Results
3.1. Complete Blood Count and Comprehensive Metabolic Panel Results for All Participants
There were no significant group-by-time interactions detected among the complete blood count and comprehensive metabolic variables (p > 0.05) as shown in Table 2 and Table 3, respectively.
Table 2.
Complete Blood Count.
Table 3.
Comprehensive Metabolic Panel—All Participants.
3.2. Male Sex Hormone Panel Results
There were no significant group-by-time interactions detected among the male hormone variables (p > 0.05) as shown in Table 4.
Table 4.
Male Hormone Panel.
3.3. Female Sex Hormone Panel Results
There were no significant group by time interactions detected female hormone variables (p > 0.05) as shown in Table 5. There was a significant main time effect (p < 0.001) in which changes were detected in females for dihydrotestosterone from Pre to Wk4 (M = −17.55, 95% CI: −27.26 to −7.83 pg/mL, p < 0.001), from Pre to Wk8 (M = −36.62, 95% CI: −51.83 to −21.41 pg/mL, p < 0.001), and from Wk4 to Wk8 (M = −19.07, 95% CI: −27.63 to −10.51 pg/mL, p < 0.001). There were no other significant changes detected for the remaining hormone variables.
Table 5.
Female Hormone Panel.
3.4. Adverse Events
There were no differences between groups in the shares of participants that reported experiencing at least one adverse event (Chi-square p = 0.826). Eleven participants (GG = 6, PLA = 5) reported 13 adverse events (GG = 7, PLA = 6). No serious adverse events were reported. There were 3 reports of increased acne (GG = 2, PLA = 1), 2 reports of fatigue (GG = 2), 2 reports of nasal bleeding (GG = 2), 2 reports of increased anxiety and emotional irritability (PLA = 2), and 2 reports of a prolonged menstrual cycle (GG = 1, PLA = 1), 1 report of headache (PLA = 1) and 1 report of increased sweating (PLA = 1).
3.5. Exploratory Analysis
In a subgroup of males with a baseline total testosterone < 700 ng/dL, there were no significant main effects or interaction effects detected for models including all three study timepoints and the hormone variables listed in Table 6. No significant main effects or interaction effects were detected when only considering Wk4 and Wk8 in the analysis (all comparisons p > 0.05). When considering Pre and Wk8, the change in total testosterone in the GG group was +33.93 ng/dL (+7.5%) and −38.31 ng/dL (−8.0%) in the PLA group (Table 7); these changes were significantly different between groups (M = +72.24, 95% CI: 3.68 to 140.80 ng/dL, p = 0.040, d = 0.821). The change in free testosterone from Pre to Wk8 in the GG group was +1.41 ng/dL (+15.0%) and −0.68 ng/dL (−6.6%) in the PLA group; these changes were significantly different between groups (M = +2.08, 95% CI: 0.15 to 4.02 ng/dL, p = 0.036, d = 0.838). The change in bioavailable testosterone from Pre to Wk8 in the GG group was +34.09 ng/dL (+14.8%) and −19.151 (−7.6%) ng/dL in the PLA group.; these changes were significantly different between groups (M = +53.24, 95% CI: 4.40 to 102.08 ng/dL, p = 0.034, d = 0.849).
Table 6.
Male Testosterone Exploratory Analysis.
Table 7.
Male Testosterone Exploratory Analysis of Pre to Wk8 Changes.
4. Discussion
The purpose of this study was to determine the safety of GG and its impact on hormone levels in males and females. There were no significant changes in any blood health markers as a complete blood count and comprehensive metabolic panel remained unchanged after 4 weeks of supplementing at 150 mg and after an additional subsequent 4 weeks at 300 mg of GG (8 weeks total). Furthermore, there were no significant changes in male and female hormone panels over the 8 weeks. Testosterone treatment is most commonly targeted for men in the lower range of the reference values for testosterone or men who are hypogonadal. Therefore, we sought to investigate in an exploratory analysis if levels of testosterone in participants had any impact on the efficacy of GG treatment. This exploratory analysis further investigating the impact of GG supplementation in males below the 3rd quartile of total testosterone levels (<700 ng/dL) revealed significant increases at Week 8 relative to baseline levels in testosterone-related hormone measures.
Geranylgeraniol has demonstrated anti-inflammatory and antinociceptive properties and previous research has reported GG to potentially improve bone health, glucose regulation, muscle function, and digestive health [4,10,11,12,13,24]. Despite the extensive research on GG and GG being generally recognized as safe following extensive animal toxicology studies, there have been no known clinical studies to date to investigate the safety of this ingredient. This trial represents the first to investigate and validate GG’s safety in humans. Here we report that the administered dosages of 150 mg and 300 mg of GG yielded no negative effects based on blood panels relating to functions of RBC and WBC stability, primary liver and kidney functions, secondary functions of muscle, lung, and pancreas, and a host of endocrine and hormonal functions.
Another objective of this study was to investigate the changes in the hormone panel measures of progesterone, estradiol, sex–hormone binding globulin (SHBG), and dihydrotestosterone (DHT) over the 8-week supplement period. Potential regulation of these hormone markers could aid in health preservation. For example, lower SHBG values are associated with higher body-mass index values [30,31] while a curvilinear relationship between serum DHT and increased risks of cardiovascular disease has been reported [32]. While hormone regulation clearly has myriad influences on health, no studies have previously investigated the effects of GG on hormone status in humans. In the current study, there were no significant between-group differences detected in progesterone, estradiol, SHBG, and DHT over the 8-week supplement period for both males and females.
Regarding testosterone markers, no significant effects were observed for the male or female cohorts. In males, this could have been due to the above-average values of total testosterone, as men may not respond to testosterone-supporting supplements if they possess normal testosterone levels. Interestingly, when males with above-average total testosterone (>700 ng/dL) were removed from the analysis, the exploratory findings demonstrated a significant increase (p < 0.05) in total-, free-, and bioavailable testosterone (+7.5%, +15.0%, and +14.8%, respectively). These exploratory outcomes agree with Ho et al. [4] who reported an increase in testosterone levels in male rats supplemented with GG for 10 days at a dose of 48.3 mg/kg compared to rats on a control diet. The findings in the exploratory analysis should be further investigated in males with LOH, which tends to occur in the latter part of adulthood, as increases in testosterone could mitigate adipose accumulation [33,34], and enhance skeletal muscle mass [16,33,34,35] and libido [16,36] in this population. However, the body composition results of our current study (Supplementary Tables S4–S6) show no changes in skeletal muscle mass, bone density, or adipose tissue mass following 8 weeks of GG supplementation. Therefore, the effects of GG on body composition are unclear in young-to-middle-age adults. Further research should focus primarily on the aging population to elucidate whether or not this outcome is age-related.
Mechanistically, there is reason to believe GG could influence testosterone metabolism. GG has been shown to stimulate steroidogenesis via the cAMP/PKA pathway by modulating the activity of adenylate cyclases [14]. Endogenously, the 3′,5′-cyclic adenosine monophosphate (cAMP)/protein kinase (PKA) signaling pathway is stimulated after the luteinizing hormone (LH) binds to the LH receptor, and this activation triggers the downstream steroidogenic proteins needed for testosterone synthesis. Furthermore, research has also demonstrated that GG has the ability to increase steroidogenic acute regulatory protein (StAR) expression when these proteins are incubated in the presence of GG in I-10 cells. StAR regulates cholesterol transport in the mitochondria in a rate-limiting step of steroidogenesis in Leydig cells [37] and acts downstream in the cAMP/PKA pathway. Taken together, mechanistically, GG has demonstrated the ability to increase testosterone production through the cAMP/PKA pathway independent of LH stimulation [14]. Since hypogonadism and low testosterone have numerous undesirable health and function effects in aging men [38] a specific focus of this study was to better understand the effects of GG supplementation on testosterone levels in men. While testosterone replacement therapy is a therapeutic option with robust effects [39], some men may face moral and ethical dilemmas with testosterone use [40] which likely influences individuals to seek natural routes of testosterone enhancement. Moreover, the use of exogenous hormone therapy may cause unfavorable side effects such as peripheral edema [41], polycythemia [42], and increased prostate volume [43]. Thus, investigating the testosterone-related effects of GG supplementation in men is important for developing both scientific and consumer knowledge regarding natural testosterone enhancement.
One of the strengths of this investigation was supplement compliance with an average compliance of 96% and 95% for GG and PLA, respectively. Additionally, in an effort to control diurnal variation, the timing of the blood draws was completed at the same time as each study visit (±1 h). A limitation of the study was its duration as participants supplemented for a total of 8 weeks and significant changes in blood chemistry might require a longer duration. In addition, this study was conducted using healthy adult males and females, therefore, these outcomes may not be generalizable to more clinical populations. We would hypothesize that specific populations, which tend to display hypogonadism (aging males), use statins, or have hormonal deficiencies (menopausal women) may exhibit more sensitive or robust responses to GG supplementation. Thus, a limitation of this study is that the results may not apply to the population that could most benefit from GG supplementation. Similarly, the study outcomes cannot be generalized beyond the 150 and 300 mg dosages administered. The occurrence of the female menstrual cycle was not documented, but subsequent study time points were aimed to inherently control the stage of menstruation by standardizing 28 days between testing sessions (average days between testing sessions; GG = 29, PLA = 28). Furthermore, the use of hormonal birth control was not controlled, and the use of such substances may interfere with testosterone production during ovulation. Finally, the plasma metabolites of LH and follicle-stimulating hormone were not examined nor were urinary metabolites of sex hormones, and these metabolites are commonly evaluated by health care practitioners. These data may have subjected additional insight into the effects of GG supplementation deemed useful by practitioners and clinicians.
5. Conclusions
This study demonstrates that GG does not significantly change the composition of blood chemistry, hematology, or sex hormone profiles in adult males or females. However, in an exploratory analysis, GG demonstrated the potential for enhancing testosterone levels among males whose baseline total testosterone value was <700 ng/dL. The potential of GG as a testosterone enhancer in males with low testosterone, such as the aging male population and those with LOH, is a worthy research question to address in future studies.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nutraceuticals3040043/s1, Table S1: Female Testosterone Exploratory Analysis—All Timepoints; Table S2: Female Testosterone Exploratory Analysis—Wk4 and Wk8; Table S3: Female Testosterone Exploratory Analysis—Pre and Wk8; Table S4: Body Composition All Participants; Table S5: Body Composition Male Participants; Table S6: Body Composition Female Participants.
Author Contributions
Conceptualization, J.W. and M.S. (Matthew Sharp); methodology, R.G., M.S. (Matthew Sharp), J.W. and M.S. (Matthew Stefan); formal analysis, M.S. (Matthew Sharp), R.G. and J.W.; investigation, R.G., C.O. and M.S. (Matthew Stefan); data curation, R.G; writing—original draft preparation, R.G., C.O., M.S. (Matthew Sharp) and J.W.; writing—review and editing, R.G., J.W., M.S. (Matthew Sharp), R.L., C.O. and M.S. (Matthew Stefan); visualization, R.G.; supervision, M.S. (Matthew Sharp); project administration, R.G.; funding acquisition, J.W., R.L. and M.S. (Matthew Sharp). All authors have read and agreed to the published version of the manuscript.
Funding
Funding was provided by American River Nutrition LLC. There is no specific funding or grant number to report.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Advarra Inc. (protocol code 122102 and date of approval: 26 January 2022).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
Data is available upon reasonable request to the corresponding author.
Conflicts of Interest
The Applied Science and Performance Institute received funding from American River Nutrition LLC for this study. Funding was not provided to a single author nor does any author have any personal relationship with the funding company. The Applied Science and Performance Institute does not have any financial interest with American River Nutrition LLC nor with the investigational study product used in this study. Associates of the funding company did not interact with study participants, nor was the funding company involved in data collection, data curation, data analysis, data interpretation, or manuscript writing. Thus, the authors declare no conflicts of interest.
References
- Raddatz-Mota, D.; Pérez-Flores, L.J.; Carrari, F.; Mendoza-Espinoza, J.A.; de León-Sánchez, F.D.; Pinzón-López, L.L.; Godoy-Hernández, G.; Rivera-Cabrera, F. Achiote (Bixa orellana L.): A Natural Source of Pigment and Vitamin E. J. Food Sci. Technol. 2017, 54, 1729–1741. [Google Scholar] [CrossRef] [PubMed]
- Medina-Flores, D.; Ulloa-Urizar, G.; Camere-Colarossi, R.; Caballero-García, S.; Mayta-Tovalino, F.; del Valle-Mendoza, J. Antibacterial Activity of Bixa orellana L. (Achiote) against Streptococcus Mutans and Streptococcus Sanguinis. Asian Pac. J. Trop. Biomed. 2016, 6, 400–403. [Google Scholar] [CrossRef]
- Meadows, C.W.; Mingardon, F.; Garabedian, B.M.; Baidoo, E.E.K.; Benites, V.T.; Rodrigues, A.V.; Abourjeily, R.; Chanal, A.; Lee, T.S. Discovery of Novel Geranylgeranyl Reductases and Characterization of Their Substrate Promiscuity. Biotechnol. Biofuels 2018, 11, 340. [Google Scholar] [CrossRef]
- Ho, H.-J.; Shirakawa, H.; Giriwono, P.E.; Ito, A.; Komai, M. A Novel Function of Geranylgeraniol in Regulating Testosterone Production. Biosci. Biotechnol. Biochem. 2018, 82, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Preece, K.; Glávits, R.; Foster, J.R.; Murbach, T.; Endres, J.R.; Hirka, G.; Vértesi, A.; Béres, E.; Szakonyiné, I.P. A Toxicological Evaluation of Geranylgeraniol. Regul. Toxicol. Pharmacol. 2021, 124, 104975. [Google Scholar] [CrossRef] [PubMed]
- Jondiko, I.J.O.; Pattenden, G. Terpenoids and an Apocarotenoid from Seeds of Bixa orellana. Phytochemistry 1989, 28, 3159–3162. [Google Scholar] [CrossRef]
- Lange, B.M.; Rujan, T.; Martin, W.; Croteau, R. Isoprenoid Biosynthesis: The Evolution of Two Ancient and Distinct Pathways across Genomes. Proc. Natl. Acad. Sci. USA 2000, 97, 13172–13177. [Google Scholar] [CrossRef]
- Holstein, S.A.; Hohl, R.J. Isoprenoids: Remarkable Diversity of Form and Function. Lipids 2004, 39, 293–309. [Google Scholar] [CrossRef]
- Buhaescu, I.; Izzedine, H. Mevalonate Pathway: A Review of Clinical and Therapeutical Implications. Clin. Biochem. 2007, 40, 575–584. [Google Scholar] [CrossRef]
- Stoffel, W.; Martius, C. Zur Synthese Der K-Vitamine Und Ubichinone. Angew. Chem. 1960, 72, 627. [Google Scholar] [CrossRef]
- Vilar, D.d.A.; Vilar, M.S.d.A.; Moura, T.F.A.d.L.e; Raffin, F.N.; de Oliveira, M.R.; Franco, C.F.d.O.; de Athayde-Filho, P.F.; Diniz, M.d.F.F.M.; Barbosa-Filho, J.M. Traditional Uses, Chemical Constituents, and Biological Activities of Bixa orellana L.: A Review. Sci. World J. 2014, 2014, 857292. [Google Scholar] [CrossRef]
- Giriwono, P.E.; Shirakawa, H.; Ohsaki, Y.; Sato, S.; Aoyama, Y.; Ho, H.-J.; Goto, T.; Komai, M. Geranylgeraniol Suppresses the Expression of IRAK1 and TRAF6 to Inhibit NFκB Activation in Lipopolysaccharide-Induced Inflammatory Responses in Human Macrophage-Like Cells. Int. J. Mol. Sci. 2019, 20, 2320. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.; Elmassry, M.M.; Cao, J.J.; Kaur, G.; Dufour, J.M.; Hamood, A.N.; Shen, C.-L. Beneficial Effect of Dietary Geranylgeraniol on Glucose Homeostasis and Bone Microstructure in Obese Mice Is Associated with Suppression of Proinflammation and Modification of Gut Microbiome. Nutr. Res. 2021, 93, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.-J.; Shirakawa, H.; Yoshida, R.; Ito, A.; Maeda, M.; Goto, T.; Komai, M. Geranylgeraniol Enhances Testosterone Production via the cAMP/Protein Kinase A Pathway in Testis-Derived I-10 Tumor Cells. Biosci. Biotechnol. Biochem. 2016, 80, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Zirkin, B.R.; Papadopoulos, V. Leydig Cells: Formation, Function, and Regulation†. Biol. Reprod. 2018, 99, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Rastrelli, G.; Vignozzi, L.; Mannucci, E.; Maggi, M. How to Recognize Late-Onset Hypogonadism in Men with Sexual Dysfunction. Asian J. Androl. 2012, 14, 251–259. [Google Scholar] [CrossRef]
- Dudek, P.; Kozakowski, J.; Zgliczyński, W. Late-Onset Hypogonadism. Prz. Menopauzalny 2017, 16, 66–69. [Google Scholar] [CrossRef]
- Giagulli, V.A.; Castellana, M.; Lisco, G.; Triggiani, V. Critical Evaluation of Different Available Guidelines for Late-Onset Hypogonadism. Andrology 2020, 8, 1628–1641. [Google Scholar] [CrossRef]
- Wylie, K.; Froggatt, N. Late Onset Hypogonadism, Sexuality and Fertility. Hum. Fertil. 2010, 13, 126–133. [Google Scholar] [CrossRef]
- Yao, Q.; Wang, B.; An, X.; Zhang, J.; Ding, L. Testosterone Level and Risk of Type 2 Diabetes in Men: A Systematic Review and Meta-Analysis. Endocr. Connect. 2017, 7, 220–231. [Google Scholar] [CrossRef]
- Morgentaler, A.; Miner, M.M.; Caliber, M.; Guay, A.T.; Khera, M.; Traish, A.M. Testosterone Therapy and Cardiovascular Risk: Advances and Controversies. Mayo Clin. Proc. 2015, 90, 224–251. [Google Scholar] [CrossRef]
- Ohlsson, C.; Barrett-Connor, E.; Bhasin, S.; Orwoll, E.; Labrie, F.; Karlsson, M.K.; Ljunggren, O.; Vandenput, L.; Mellström, D.; Tivesten, A. High Serum Testosterone Is Associated with Reduced Risk of Cardiovascular Events in Elderly Men. The MrOS (Osteoporotic Fractures in Men) Study in Sweden. J. Am. Coll. Cardiol. 2011, 58, 1674–1681. [Google Scholar] [CrossRef]
- Bassil, N.; Alkaade, S.; Morley, J.E. The Benefits and Risks of Testosterone Replacement Therapy: A Review. Ther. Clin. Risk Manag. 2009, 5, 427–448. [Google Scholar]
- Jiwan, N.C.; Appell, C.R.; Wang, R.; Shen, C.-L.; Luk, H.-Y. Geranylgeraniol Supplementation Mitigates Soleus Muscle Atrophy via Changes in Mitochondrial Quality in Diabetic Rats. In Vivo 2022, 36, 2638–2649. [Google Scholar] [CrossRef]
- Shen, C.-L.; Dufour, J.M.; Miranda, J.M.; Kaur, G.; Chung, E.; Ramalingam, L.; Moustaid-Moussa, N.; Cao, J.J. Effect of Dietary Geranylgeraniol and Green Tea Polyphenols on Glucose Homeostasis, Bone Turnover Biomarkers, and Bone Microstructure in Obese Mice. Int. J. Mol. Sci. 2023, 24, 979. [Google Scholar] [CrossRef]
- Irwin, J.C.; Fenning, A.S.; Vella, R.K. Geranylgeraniol Prevents Statin-Induced Skeletal Muscle Fatigue without Causing Adverse Effects in Cardiac or Vascular Smooth Muscle Performance. Transl. Res. 2020, 215, 17–30. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Haring, R.; Hannemann, A.; John, U.; Radke, D.; Nauck, M.; Wallaschofski, H.; Owen, L.; Adaway, J.; Keevil, B.G.; Brabant, G. Age-Specific Reference Ranges for Serum Testosterone and Androstenedione Concentrations in Women Measured by Liquid Chromatography-Tandem Mass Spectrometry. J. Clin. Endocrinol. Metab. 2012, 97, 408–415. [Google Scholar] [CrossRef]
- O’Reilly, M.W.; Glisic, M.; Kumarendran, B.; Subramanian, A.; Manolopoulos, K.N.; Tahrani, A.A.; Keerthy, D.; Muka, T.; Toulis, K.A.; Hanif, W.; et al. Serum Testosterone, Sex Hormone-Binding Globulin and Sex-Specific Risk of Incident Type 2 Diabetes in a Retrospective Primary Care Cohort. Clin. Endocrinol. 2019, 90, 145–154. [Google Scholar] [CrossRef]
- Yeap, B.B.; Marriott, R.J.; Antonio, L.; Raj, S.; Dwivedi, G.; Reid, C.M.; Anawalt, B.D.; Bhasin, S.; Dobs, A.S.; Handelsman, D.J.; et al. Associations of Serum Testosterone and Sex Hormone-Binding Globulin with Incident Cardiovascular Events in Middle-Aged to Older Men. Ann. Intern. Med. 2021, 175, 159–170. [Google Scholar] [CrossRef]
- Shores, M.M.; Biggs, M.L.; Arnold, A.M.; Smith, N.L.; Longstreth, W.T.; Kizer, J.R.; Hirsch, C.H.; Cappola, A.R.; Matsumoto, A.M. Testosterone, Dihydrotestosterone, and Incident Cardiovascular Disease and Mortality in the Cardiovascular Health Study. J. Clin. Endocrinol. Metab. 2014, 99, 2061–2068. [Google Scholar] [CrossRef]
- Isidori, A.M.; Giannetta, E.; Greco, E.A.; Gianfrilli, D.; Bonifacio, V.; Isidori, A.; Lenzi, A.; Fabbri, A. Effects of Testosterone on Body Composition, Bone Metabolism and Serum Lipid Profile in Middle-Aged Men: A Meta-Analysis. Clin. Endocrinol. 2005, 63, 280–293. [Google Scholar] [CrossRef]
- Allan, C.A.; Strauss, B.J.G.; Burger, H.G.; Forbes, E.A.; McLachlan, R.I. Testosterone Therapy Prevents Gain in Visceral Adipose Tissue and Loss of Skeletal Muscle in Nonobese Aging Men. J. Clin. Endocrinol. Metab. 2008, 93, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Eyre, D.R.; Clark, R.; Kleinberg, D.; Newman, C.; Iranmanesh, A.; Veldhuis, J.; Dudley, R.E.; Berman, N.; Davidson, T.; et al. Sublingual Testosterone Replacement Improves Muscle Mass and Strength, Decreases Bone Resorption, and Increases Bone Formation Markers in Hypogonadal Men—A Clinical Research Center Study. J. Clin. Endocrinol. Metab. 1996, 81, 3654–3662. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rizk, P.J.; Kohn, T.P.; Pastuszak, A.W.; Khera, M. Testosterone Therapy Improves Erectile Function and Libido in Hypogonadal Men. Curr. Opin. Urol. 2017, 27, 511–515. [Google Scholar] [CrossRef]
- Stocco, D.M.; Wang, X.; Jo, Y.; Manna, P.R. Multiple Signaling Pathways Regulating Steroidogenesis and Steroidogenic Acute Regulatory Protein Expression: More Complicated than We Thought. Mol. Endocrinol. 2005, 19, 2647–2659. [Google Scholar] [CrossRef]
- Surampudi, P.N.; Wang, C.; Swerdloff, R. Hypogonadism in the Aging Male Diagnosis, Potential Benefits, and Risks of Testosterone Replacement Therapy. Int. J. Endocrinol. 2012, 2012, 625434. [Google Scholar] [CrossRef]
- Corona, G.; Sforza, A.; Maggi, M. Testosterone Replacement Therapy: Long-Term Safety and Efficacy. World J. Mens Health 2017, 35, 65–76. [Google Scholar] [CrossRef]
- Leone, J.E.; Fetro, J.V. Perceptions and Attitudes toward Androgenic-Anabolic Steroid Use among Two Age Categories: A Qualitative Inquiry. J. Strength Cond. Res. 2007, 21, 532–537. [Google Scholar] [CrossRef]
- Osterberg, E.C.; Bernie, A.M.; Ramasamy, R. Risks of Testosterone Replacement Therapy in Men. Indian J. Urol. 2014, 30, 2–7. [Google Scholar] [CrossRef]
- Drinka, P.J.; Jochen, A.L.; Cuisinier, M.; Bloom, R.; Rudman, I.; Rudman, D. Polycythemia as a Complication of Testosterone Replacement Therapy in Nursing Home Men with Low Testosterone Levels. J. Am. Geriatr. Soc. 1995, 43, 899–901. [Google Scholar] [CrossRef]
- Guo, C.; Gu, W.; Liu, M.; Peng, B.O.; Yao, X.; Yang, B.; Zheng, J. Efficacy and Safety of Testosterone Replacement Therapy in Men with Hypogonadism: A Meta-Analysis Study of Placebo-Controlled Trials. Exp. Ther. Med. 2016, 11, 853–863. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).