Artificial Cold Air Increases the Cardiovascular Risks in Spontaneously Hypertensive Rats

Abstract
:1. Introduction
2. Materials and Methods
2.1. Cold Air Data and Cold Air Simulation

{kind=link}
{kind=link}
| Cold air rank | Tmin-s (°C) | Tr (°C) | Tmin-g (°C) | ↓∆T48 (°C) | Tmin (°C) | ↓∆Tmax (°C) | Rewarming duration (h) | Total duration (h) |
|---|---|---|---|---|---|---|---|---|
| Moderate | 20 | 20 | 12.7 | 7.3 | 11.1 | 8.9 | 51 | 55 |
2.2. Animals and Grouping
2.3. Animal Housing for Control Period
2.4. Cold Air Exposure
2.5. Monitoring of Blood Pressure, Heart Rate and Body Weight
2.6. Plasma Collection
2.7. Assessment of Vasoconstrictors, Atherogenesis Risk Factors and Myocardium Injury Indicator
2.8. Statistical Analysis
3. Results
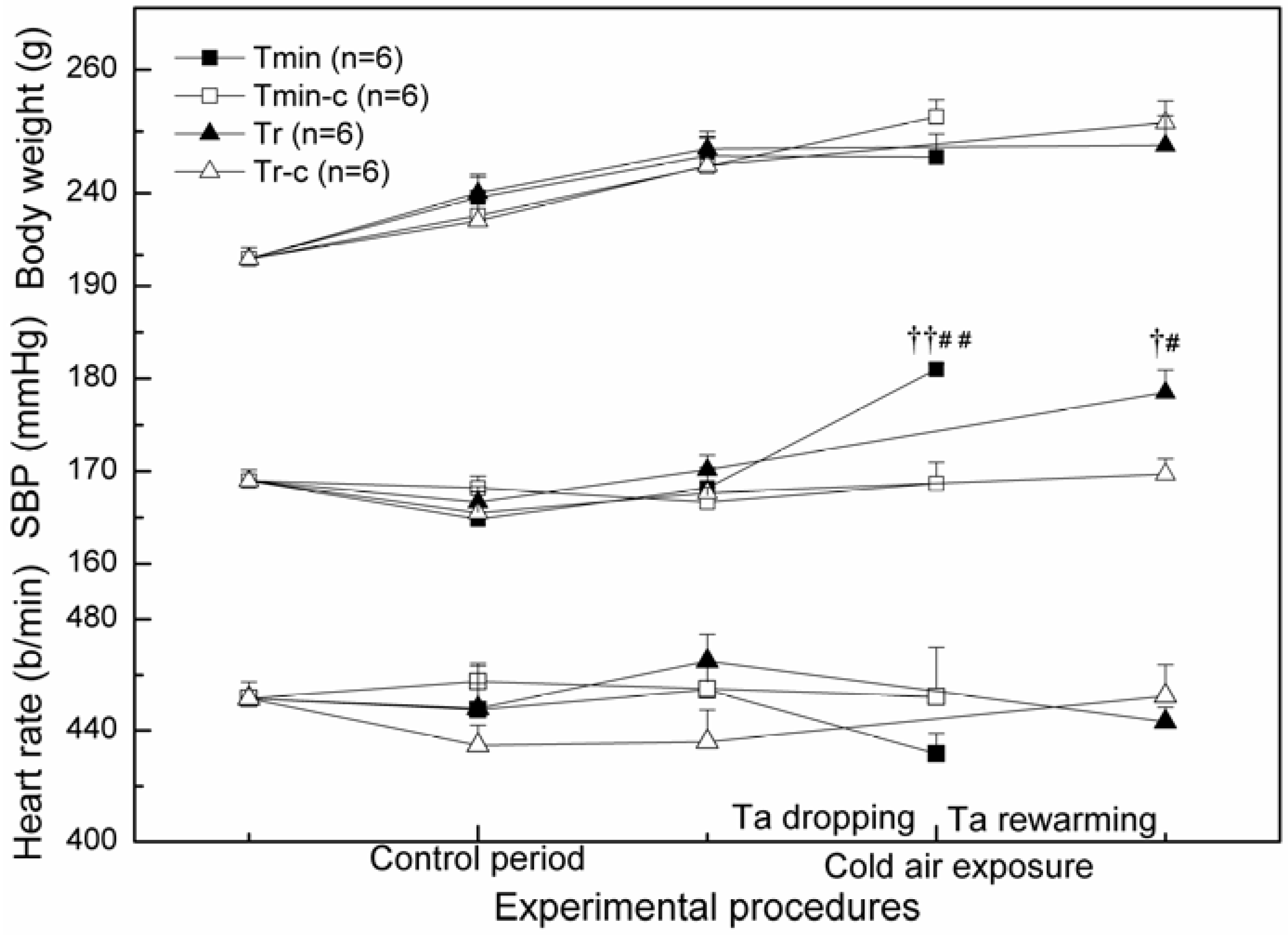
3.1. SBP, Heart Rate and Body Weight

3.2. Vasoconstrictors—EPI, NE, ANGII and ET-1

3.3. CK-MB and Atherogenesis Risk Factors—WBV, Blood Lipids, FG and Uric Acid (Table 2)
| Atherosclerosis risk factors | Tmin-c (n = 6) | Tmin (n = 6) | Tr-c (n = 6) | Tr (n = 6) | |
|---|---|---|---|---|---|
| Whole blood | 10/s | 11.10 (0.58) | 17.31 (0.49) †† | 12.36 (0.76) | 15.97 (2.21) † |
| Viscosity (mPa.s) | 150/s | 4.29 (0.10) | 5.73 (0.14) †† | 4.53 (0.13) | 5.25 (0.39) † |
| Fibrinogen (g/L) | 1.92 (0.04) | 2.06 (0.01) †† | 2.00 (0.04) | 2.30 (0.06) ††,‡‡ | |
| Blood lipids (mmol/L) | TC | 0.89 (0.01) | 1.14 (0.04) †† | 0.93 (0.02) | 1.08 (0.04) † |
| TG | 0.38 (0.04) | 0.27 (0.02) † | 0.39 (0.04) | 0.28 (0.01) † | |
| HDL | 0.5 (0.01) | 0.62 (0.01) †† | 0.56 (0.02) | 0.55 (0.02) ‡ | |
| LDL | 0.48 (0.03) | 0.65 (0.04) † | 0.41 (0.02) | 0.73 (0.10) † | |
| LDL/HDL | 0.97 (0.07) | 1.06 (0.06) | 0.74 (0.01) | 1.33 (0.22) †† | |
| Uric acid (umol/L) | 71.5 (5.67) | 173.67 (17.78) †† | 71.17 (7.01) | 170.67 (18.62) †† | |
| CK-MB (U/L) | 236.17 (20.98) | 362.67 (29.37) †† | 214.5 (9.25) | 378.67 (25.88) †† | |
4. Discussion
Acknowledgements
Conflict of Interest
References
- Hopstock, L.A.; Wilsgaard, T.; Njolstad, I.; Mannsverk, J.; Mathiesen, E.B.; Lochen, M.L.; Bonaa, K.H. Seasonal variation in incidence of acute myocardial infarction in a sub-arctic population: The tromso study 1974–2004. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 18, 320–325. [Google Scholar] [CrossRef]
- Danet, S.; Richard, F.; Montaye, M.; Beauchant, S.; Lemaire, B.; Graux, C.; Cottel, D.; Marecaux, N.; Amouyel, P. Unhealthy effects of atmospheric temperature and pressure on the occurrence of myocardial infarction and coronary deaths. A 10-year survey: The lille-world health organization monica project (monitoring trends and determinants in cardiovascular disease). Circulation 1999, 100, E1–E7. [Google Scholar]
- Kriszbacher, I.; Koppan, M.; Bodis, J. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 2005, 353, 429–430. [Google Scholar]
- Neild, P.J.; Syndercombe-Court, D.; Keatinge, W.R.; Donaldson, G.C.; Mattock, M.; Caunce, M. Cold-induced increases in erythrocyte count, plasma cholesterol and plasma fibrinogen of elderly people without a comparable rise in protein C or factor X. Clin. Sci. (Lond.) 1994, 86, 43–48. [Google Scholar]
- Woodhouse, P.R.; Khaw, K.T.; Plummer, M.; Foley, A.; Meade, T.W. Seasonal variations of plasma fibrinogen and factor vii activity in the elderly: Winter infections and death from cardiovascular disease. Lancet 1994, 343, 435–439. [Google Scholar]
- Stout, R.W.; Crawford, V. Seasonal variations in fibrinogen concentrations among elderly people. Lancet 1991, 338, 9–13. [Google Scholar]
- Keatinge, W.R.; Coleshaw, S.R.K.; Cotter, F.; Mattock, M.; Murphy, M.; Chelliah, R. Increases in platelet and red cell counts, blood viscosity, and arterial pressure during mild surface cooling: Factors in mortality from coronary and cerebral thrombosis in winter. Br. Med. J. (Clin. Res. Ed.) 1984, 289, 1405–1408. [Google Scholar]
- Sun, Z. Cardiovascular responses to cold exposure. Front. Biosci. (Elite Ed.) 2010, 2, 495–503. [Google Scholar]
- Watanabe, K.; Takahashi, T.; Miyajima, S.; Hirokawa, Y.; Tanabe, N.; Kato, K.; Kodama, M.; Aizawa, Y.; Tazawa, S.; Inoue, M. Myocardial sympathetic denervation, fatty acid metabolism, and left ventricular wall motion in vasospastic angina. J. Nucl. Med. 2002, 43, 1476–1481. [Google Scholar]
- Luo, B.; Zhang, S.Y.; Ma, S.C.; Zhou, J.; Wang, B.J. Effects of cold air on cardiovascular disease risk factors in rat. Int. J. Environl. Res. Public Health 2012, 9, 2312–2325. [Google Scholar] [CrossRef]
- Qian, Z.M.; Koon, H.W. Area postrema is essential for the maintenance of normal blood pressure under cold stress in rats. Exp. Brain Res. 1998, 121, 186–190. [Google Scholar] [CrossRef]
- Tang, Z.Y.; Zhu, Q.Y.; Xu, L.J.; Deng, L.Y.; Zeng, Y.; Ding, W.J.; Huang, W. Artificial cold wave-induced cerebral infarction in rats with carotid atherosclerosis. J. Mol. Neurosci. 2012, 47, 278–285. [Google Scholar] [CrossRef]
- Clauss, A. Rapid physiological coagulation method in determination of fibrinogen. Acta Haematol. 1957, 17, 237–246. [Google Scholar] [CrossRef]
- Sullivan, D.R.; Kruijswijk, Z.; West, C.E.; Kohlmeier, M.; Katan, M.B. Determination of serum triglycerides by an accurate enzymatic method not affected by free glycerol. Clin. Chem. 1985, 31, 1227–1228. [Google Scholar]
- Nauck, M.; Warnick, G.R.; Rifai, N. Methods for measurement of LDL-cholesterol: A critical assessment of direct measurement by homogeneous assays versus calculation. Clin. Chem. 2002, 48, 236–254. [Google Scholar]
- Warnick, G.R.; Nauck, M.; Rifai, N. Evolution of methods for measurement of HDL-cholesterol: From ultracentrifugation to homogeneous assays. Clin. Chem. 2001, 47, 1579–1596. [Google Scholar]
- Siedel, J.; Hagele, E.O.; Ziegenhorn, J.; Wahlefeld, A.W. Reagent for the enzymatic determination of serum total cholesterol with improved lipolytic efficiency. Clin. Chem. 1983, 29, 1075–1080. [Google Scholar]
- Gochman, N.; Schmitz, J.M. Automated determination of uric acid, with use of a uricase-peroxidase system. Clin. Chem. 1971, 17, 1154–1159. [Google Scholar]
- Lipsitz, L.A.; Hamner, J.M.S.; Gagnon, M.; Babikian, V. Dynamic regulation of middle cerebral artery blood flow velocity in aging and hypertension. Stroke 2000, 31, 1897–1903. [Google Scholar] [CrossRef]
- Heijer, T.; Skoog, I.; Oudkerk, M.; de Leeuw, F.E.; de Groot, J.C.; Hofman, A.; Breteler, M.M. Associationbetween blood pressure levels over time and brain atrophy in the elderly. Neurobiol. Aging 2003, 24, 307–313. [Google Scholar]
- Chobanian, A.V.; Alexander, R.W. Exacerbation of atherosclerosis by hypertension. Potential mechanisms and clinical implications. Arch. Intern. Med. 1996, 156, 1952–1956. [Google Scholar]
- Cohn, J.N.; Quyyumi, A.A.; Hollenberg, N.K.; Jamerson, K.A. Surrogate markers for cardiovascular disease: Functional markers. Circulation 2004, 109, IV31–IV46. [Google Scholar]
- Green, D.; Foiles, N.; Chan, C.; Schreiner, P.J.; Liu, K. Elevated fibrinogen levels and subsequent subclinical atherosclerosis: The cardia study. Atherosclerosis 2009, 202, 623–631. [Google Scholar] [CrossRef]
- Guo, F.; Liu, J.; Wang, C.; Liu, N.; Lu, P. Fibrinogen, fibrin, and FDP induce C-reactive protein generation in rat vascular smooth muscle cells: Pro-inflammatory effect on atherosclerosis. Biochem. Biophys. Res. Commun. 2009, 390, 942–946. [Google Scholar] [CrossRef]
- Hansson, G.K. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 2005, 352, 1685–1695. [Google Scholar] [CrossRef]
- Lusis, A.J. Atherosclerosis. Nature 2000, 407, 233–241. [Google Scholar] [CrossRef]
- Mustard, J.F.; Murphy, E.A.; Ogryzlo, M.A.; Smythe, H.A. Blood coagulation and platelet economy in subjects with primary gout. Can. Med. Assoc. J. 1963, 89, 1207–1211. [Google Scholar]
- Kang, D.H.; Nakagawa, T.; Feng, L.; Watanabe, S.; Han, L.; Mazzali, M.; Truong, L.; Harris, R.; Johnson, R.J. A role for uric acid in the progression of renal disease. J. Am. Soc. Nephrol. 2002, 13, 2888–2897. [Google Scholar] [CrossRef]
- Watanabe, S.; Kang, D.H.; Feng, L.; Nakagawa, T.; Kanellis, J.; Lan, H.; Mazzali, M.; Johnson, R.J. Uric acid, hominoid evolution, and the pathogenesis of salt-sensitivity. Hypertension 2002, 40, 355–360. [Google Scholar]
- Zhang, Y.; Hu, N.; Hua, Y.; Richmond, K.L.; Dong, F.; Ren, J. Cardiac overexpression of metallothionein rescues cold exposure-induced myocardial contractile dysfunction through attenuation of cardiac fibrosis despite cardiomyocyte mechanical anomalies. Free Radic. Biol. Med. 2012, 53, 194–207. [Google Scholar]
- Morley, R.M.; Conn, C.A.; Kluger, M.J.; Vander, A.J. Temperature regulation in biotelemetered spontaneously hypertensive rats. Am. J. Physiol. 1990, 258, R1064–R1069. [Google Scholar]
- Kirby, R.F.; Sokoloff, G.; Perdomo, E.; Blumberg, M.S. Thermoregulatory and cardiac responses of infant spontaneously hypertensive and Wistar-Kyoto rats to cold exposure. Hypertension 1999, 33, 1465–1469. [Google Scholar]
- Hadjiisky, P.; Peyri, N. Hypertensive arterial disease and atherogenesis. Part. 1. Intimal changes in the old, spontaneously hypertensive rat (SHR). Atherosclerosis 1982, 44, 181–199. [Google Scholar] [CrossRef]
- Yu, W.; Hu, W.; Mengersen, K.; Guo, Y.; Pan, X.; Connell, D.; Tong, S. Time course of temperature effects on cardiovascular mortality in Brisbane, Australia. Heart 2011, 97, 1089–1093. [Google Scholar] [Green Version]
- Fernandez, M.L.; Webb, D. The LDL to HDL cholesterol ratio as a valuable tool to evaluate coronary heart disease risk. J. Am. Coll. Nutr. 2008, 27, 1–5. [Google Scholar]
- Huynen, M.M.; Martens, P.; Schram, D.; Weijenberg, M.P.; Kunst, A.E. The impact of heat waves and cold spells on mortality rates in the Dutch population. Environ. Health Perspect. 2001, 109, 463–470. [Google Scholar] [CrossRef]
- Sun, Z.; Cade, J.R.; Fregly, M.J.; Rowland, N.E. Effect of chronic treatment with propranolol on the cardiovascular responses to chronic cold exposure. Physiol. Behav. 1997, 62, 379–384. [Google Scholar] [CrossRef]
- Sun, Z.; Cade, R.; Morales, C. Role of central angiotensin II receptors in cold-induced hypertension. Am. J. Hypertens. 2002, 15, 85–92. [Google Scholar] [CrossRef]
- Fujiwara, T.; Kawamura, M.; Nakajima, J.; Adachi, T.; Hiramori, K. Seasonal differences in diurnal blood pressure of hypertensive patients living in a stable environmental temperature. J. Hypertens. 1995, 13, 1747–1752. [Google Scholar]
- Manfredini, R.; Gallerani, M.; Portaluppi, F.; Salmi, R.; Fersini, C. Chronobiological patterns of onset of acute cerebrovascular diseases. Thromb. Res. 1997, 88, 451–463. [Google Scholar] [CrossRef]
- Sun, Z.; Cade, R.; Katovich, M.J.; Fregly, M.J. Body fluid distribution in rats with cold-induced hypertension. Physiol. Behav. 1999, 65, 879–884. [Google Scholar]
- Barney, C.C.; Katovich, M.J.; Fregly, M.J.; Tyler, P.E. Changes in beta-adrenergic responsiveness of rats during chronic cold exposure. J. Appl. Physiol. 1980, 49, 923–929. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Luo, B.; Zhang, S.; Ma, S.; Zhou, J.; Wang, B. Artificial Cold Air Increases the Cardiovascular Risks in Spontaneously Hypertensive Rats. Int. J. Environ. Res. Public Health 2012, 9, 3197-3208. https://doi.org/10.3390/ijerph9093197
Luo B, Zhang S, Ma S, Zhou J, Wang B. Artificial Cold Air Increases the Cardiovascular Risks in Spontaneously Hypertensive Rats. International Journal of Environmental Research and Public Health. 2012; 9(9):3197-3208. https://doi.org/10.3390/ijerph9093197
Chicago/Turabian StyleLuo, Bin, Shuyu Zhang, Shoucun Ma, Ji Zhou, and Baojian Wang. 2012. "Artificial Cold Air Increases the Cardiovascular Risks in Spontaneously Hypertensive Rats" International Journal of Environmental Research and Public Health 9, no. 9: 3197-3208. https://doi.org/10.3390/ijerph9093197