
Life Cycle Assessments in Healthcare: Insights and Standardisation Needs

Highlights
- Healthcare delivery contributes substantially to greenhouse gas emissions, linking healthcare operations to population health risks from climate change.
- Life cycle assessment is increasingly used to quantify these impacts, but inconsistent application limits its usefulness for health system decision-making.
- Methodological heterogeneity prevents aggregation and comparison of healthcare LCA results, constraining evidence-based decarbonisation of health systems.
- This study identifies where standardisation is currently most feasible and where healthcare-specific guidance is urgently needed to support public health policy.
- Product-level LCA already provides comparatively consistent evidence and can support sustainable healthcare procurement.
- To inform clinical and system-level decisions, service and organisational assessments require pathway-based functional units and defined hospital sub-unit coverage.
Abstract
1. Introduction
- Which sector-specific standards and frameworks for LCA have been developed for application in healthcare?
- How is LCA currently conceptualised and operationalised across different assessment levels and healthcare contexts?
- To what extent does current practice align with established standards and frameworks, and where do methodological inconsistencies or needs for further standardisation become apparent?
2. Methods
3. Results
3.1. Healthcare-Specific LCA Standards
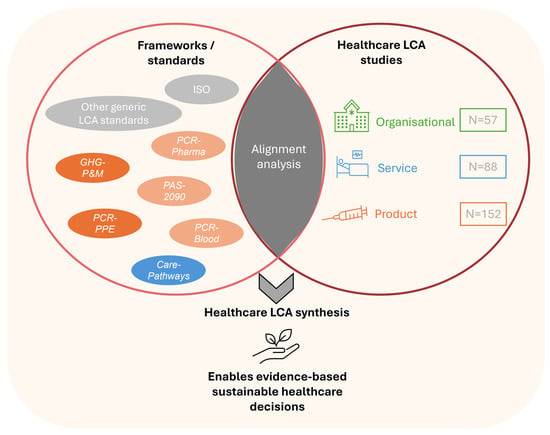
- The second edition of Care Pathways: Guidance on Appraising Sustainability (Care-Pathways) provides service-level guidance for healthcare pathways [29].
- Greenhouse Gas Accounting Sector Guidance for Pharmaceutical Products and Medical Devices (GHG-P&M) offers product-level guidance aligned with the GHG Protocol Product Life Cycle Standard [30]
- Product Category Rules 2016:07 Blood and blood-derived products for therapeutic or prophylactic uses (PCR-Blood) define rules for blood-related products [31].
- Product Category Rules 2017:01 Disposable Surgical Drapes, Gowns, Air Suits and Face Masks (PCR-PPE) define LCA rules for personal protective equipment [32].
- Product Category Rules for pharmaceutical products and processes (PCR-Pharma) is considered an academic, whitepaper-style framework rather than a fully operational PCR [33].
- Publicly Available Specification 2090 Pharmaceutical products—Product category rules for environmental life cycle assessments of pharmaceuticals (PAS-2090) is a recently published British Standard [25].
3.2. LCA Studies
3.3. Alignment of Healthcare LCA Practice with Existing Standards
4. Discussion and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AHRQ | Agency for Healthcare Research and Quality |
| API | Active Pharmaceutical Ingredient |
| AWARE | Available Water Remaining |
| BMWE | German Federal Ministry for Economic Affairs and Energy (Bundesministerium für Wirtschaft und Energie) |
| CED | Cumulative Energy Demand |
| CF | Carbon Footprint |
| CML | Centrum voor Milieukunde Leiden Impact Assessment Method |
| CO2 | Carbon Dioxide |
| EF method | Environmental Footprint Method (European Commission) |
| EPD | Environmental Product Declaration |
| EU | European Union |
| FU | Functional Unit |
| GHG | Greenhouse Gas |
| GHG-P&M | Greenhouse Gas Accounting Sector Guidance for Pharmaceutical Products and Medical Devices |
| GHG Protocol | Greenhouse Gas Protocol Corporate Accounting and Reporting Standard |
| ICHI | International Classification of Health Interventions |
| ILCD | International Reference Life Cycle Data System |
| IMPACT 2002+ | Impact Assessment Method 2002+ |
| IPCC | Intergovernmental Panel on Climate Change (Global Warming Potential Method) |
| ISO | International Organisation for Standardisation |
| LCA | Life Cycle Assessment |
| LCI | Life Cycle Inventory |
| LCIA | Life Cycle Impact Assessment |
| LCSA | Life Cycle Sustainability Assessment |
| OPS | Operationen- und Prozedurenschlüssel (German Procedure Classification) |
| PAS | Publicly Available Specification |
| PAS 2090 | Pharmaceutical Products—Product Category Rules for Environmental Life Cycle Assessments |
| PCR | Product Category Rules |
| PCR-Blood | Product Category Rules for Blood and Blood-Derived Products |
| PCR-PPE | Product Category Rules for Disposable Surgical Drapes, Gowns, Air Suits and Face Masks |
| PCR-Pharma | Product Category Rules for Pharmaceutical Products and Processes |
| PEF | Product Environmental Footprint |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| ReCiPe | Life Cycle Impact Assessment Method Combining Midpoint And Endpoint Indicators |
| Scope 1–3 | Categories of Greenhouse Gas Emissions According to the GHG Protocol |
| TRACI | Tool for the Reduction and Assessment of Chemical and Other Environmental Impacts |
| USEtox | UNEP-SETAC Toxicity Model for Human Toxicity and Ecotoxicity |
| WHO | World Health Organisation |
References
- Karliner, J.; Slotterback, S.; Boyd, R.; Steele, K.; Ashby, B. Health Cares Climate Footprint. 2019. Available online: https://global.noharm.org/sites/default/files/documents-files/5961/HealthCaresClimateFootprint_092319.pdf (accessed on 18 July 2025).
- Lenzen, M.; Malik, A.; Li, M.; Fry, J.; Weisz, H.; Pichler, P.-P.; Chaves, L.S.M.; Capon, A.; Pencheon, D. The environmental footprint of health care: A global assessment. Lancet Planet. Health 2020, 4, e271–e279. [Google Scholar] [CrossRef] [PubMed]
- Eckelman, M.J.; Sherman, J. Environmental Impacts of the U.S. Health Care System and Effects on Public Health. PLoS ONE 2016, 11, e0157014. [Google Scholar] [CrossRef] [PubMed]
- Chen-Xu, J.; Corda, M.O.; Varga, O.; Viegas, S. Health burden and costs attributable to the carbon footprint of the health sector in the European Union. Environ. Int. 2024, 190, 108828. [Google Scholar] [CrossRef] [PubMed]
- ISO 14040:2006; International Organization for Standardization. Environmental Management—Life Cycle Assessment—Principles and Framework. International Organization for Standardization: Geneva, Switzerland, 2006. Available online: https://www.iso.org/standard/37456.html (accessed on 18 July 2025).
- ISO 14044; Environmental Management—Life Cycle Assessment—Requirements and Guidelines. International Organization for Standardization: Geneva, Switzerland, 2006. Available online: https://www.iso.org/standard/38498.html (accessed on 18 July 2025).
- EU-2024/1781; Regulation (EU) 2024/1781 of the European Parliament and of the Council of 13 June 2024 Establishing a Framework for the Setting of Ecodesign Requirements for Sustainable Products, Amending Directive (EU) 2020/1828 and Regulation (EU) 2023/1542 and Repealing Directive 2009/125/EC (Text with EEA Relevance). European Parliament: Brussels, Belgium; European Council Regulation: Brussels, Belgium, 2024. Available online: https://eur-lex.europa.eu/eli/reg/2024/1781/oj/eng (accessed on 1 September 2025).
- European Comission. EU Taxonomy Navigator. Available online: https://ec.europa.eu/sustainable-finance-taxonomy/ (accessed on 1 September 2025).
- ISO 14046:2014; Environmental Management—Water Footprint—Principles, Requirements and Guidelines. International Organization for Standardization: Geneva, Switzerland, 2014.
- ISO 14067:2018; Greenhouse Gases—Carbon Footprint of Products—Requirements and Guidelines for Quantification. International Organization for Standardization: Geneva, Switzerland, 2018.
- Hauschild, M.Z.; Rosenbaum, R.K.; Olsen, S.I. (Eds.) Life Cycle Assessment: Theory and Practice; Springer International Publishing: Cham, Switzerland, 2018; ISBN 978-3-319-56474-6. Available online: https://link.springer.com/10.1007/978-3-319-56475-3 (accessed on 19 November 2025).
- European Commission. Product Environmental Footprint Category Rules Guidance. 2018. Available online: https://eplca.jrc.ec.europa.eu/permalink/PEFCR_guidance_v6.3-2.pdf (accessed on 1 September 2025).
- EPD International AB. Product Category Rules|EPD International. International EPD System. Available online: https://www.environdec.com/services/what-is-pcr (accessed on 18 December 2025).
- Rizan, C.; Bhutta, M.F. Environmental impact and life cycle financial cost of hybrid (reusable/single-use) instruments versus single-use equivalents in laparoscopic cholecystectomy. Surg. Endosc. 2022, 36, 4067–4078. [Google Scholar] [CrossRef] [PubMed]
- Rizan, C.; Brophy, T.; Lillywhite, R.; Reed, M.; Bhutta, M.F. Life cycle assessment and life cycle cost of repairing surgical scissors. Int. J. Life Cycle Assess. 2022, 27, 780–795. [Google Scholar] [CrossRef]
- Quitmann, C.; Terres, L.; Maun, A.; Sauerborn, R.; Reynolds, E.; Bärnighausen, T.; Herrmann, A.; Franke, B. Assessing greenhouse gas emissions in hospitals: The development of an open-access calculator and its application to a German case-study. Clean. Environ. Syst. 2025, 16, 100262. [Google Scholar] [CrossRef]
- EAHP—European Association of Hospital Pharmacists. EAHP. Available online: https://eahp.eu/ (accessed on 19 November 2025).
- Health Care Without Harm. Sustainable Procurement in Health Care Guide. Available online: https://practicegreenhealth.org/sites/default/files/2020-07/Sustainable%20procurement%20guide%20%28U.S.%20version%29.pdf (accessed on 18 July 2025).
- CBR_Admin. Life Cycle Assessment (LCA) in MedTech. CBR Sustainability Partners. 2024. Available online: https://cbr-partner.de/article/life-cycle-assessment-lca-in-medtech/ (accessed on 19 November 2025).
- Von der Wiege bis zur Bahre: Was ist eine Lebenszyklusanalyse (LCA)? Available online: https://www.oliverhcp.com/news-and-resources/packtalk/from-cradle-to-grave-what-is-a-life-cycle-assessment-lca (accessed on 19 November 2025).
- ISO 14072:2024; Environmental Management—Life Cycle Assessment—Requirements and Guidance for Organizational Life Cycle Assessment. International Organization for Standardization: Geneva, Switzerland, 2024. Available online: https://www.iso.org/standard/86265.html (accessed on 25 August 2025).
- WBCSD; WRI. A Corporate Accounting and Reporting Standard. 2004. Available online: https://ghgprotocol.org/sites/default/files/standards/ghg-protocol-revised.pdf (accessed on 31 July 2025).
- ISO 14064-1:2018; Part 1: Specification with Guidance at the Organization Level for Quantification and Reporting of Greenhouse Gas Emissions and Removals. International Organization for Standardization: Geneva, Switzerland, 2018. Available online: https://www.iso.org/standard/66453.html (accessed on 25 August 2025).
- Normung im Bereich der Ökobilanzen für Medizin- und Pharmaprodukte. Available online: https://www.din.de/de/service-fuer-anwender/normungsportale/gesundheit/aktuelles/oekobilanzen-fuer-medizin-und-pharmaprodukte-1213008 (accessed on 20 August 2025).
- PAS 2090:2025; Pharmaceutical Products–Product Category Rules for Environmental Life Cycle Assessments–Specification. The British Standards Institution: London, UK, 2025.
- Sharma, B.; Swanton, B.; Kuo, J.; Sysawang, K.; Yagyu, S.; Motala, A.; Tolentino, D.; Meshkati, N.; Hempel, S. Use of Life Cycle Assessment in the Healthcare Industry: Environmental Impacts and Emissions Associated With Products, Processes, and Waste; AHRQ Comparative Effectiveness Technical Briefs; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2024. Available online: http://www.ncbi.nlm.nih.gov/books/NBK610172/ (accessed on 2 February 2026).
- EFPIA. Advancing Environmental Sustainability Assessment of Pharmaceuticals Through Standardisation and Harmonisation of Product Carbon Footprint Assessment. 2025. Available online: https://www.efpia.eu/media/mdsb0efi/advancing-environmental-sustainability-assessment-of-pharmaceuticals-through-standardisation-and-harmonisation-of-product-carbon-footprint-assessment.pdf (accessed on 27 May 2026).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.; Aumônier, S.; Galley, S.; Calnan, A. Care Pathways: Guidance on Appraising Sustainability Main Document; Sustainable Healthcare Coalition (SHC): Newton Abbot, UK, 2023. [Google Scholar]
- Penny, T.; Fisher, K.; Collins, M.; Allison, C. Greenhouse Gas Accounting Sector Guidance for Pharmaceutical Products and Medical Devices GHG Protocol Product Life Cycle Accounting and Reporting Standard 2012. Available online: https://ghgprotocol.org/sites/default/files/tools/Summary-Document_Pharmaceutical-Product-and-Medical-Device-GHG-Accounting_November-2012.pdf (accessed on 16 June 2026).
- EPD International AB. Product Cetegory Rules: Blood and Blood Derived Products for Therapeutic or Prophylactic Uses UN CPC 35270. 2022. Available online: https://environdec.com/pcr-library/with-documents (accessed on 18 July 2025).
- EPD International AB. PCR 2017:01 Version 2.0.0 Disposable Surgical Drapes, Gowns, Air Suits and Face Masks Product Category Classification: UN CPC 35290. 2024. Available online: https://environdec.com/pcr-library/pcr2017-01 (accessed on 18 July 2025).
- Siegert, M.-W.; Finkbeiner, M.; Emara, Y.; Lehmann, A. Product Category Rules (PCR) for Pharmaceutical Products and Processes. 2019. Available online: https://depositonce.tu-berlin.de/handle/11303/10154 (accessed on 18 July 2025).
- HealthcareLCA Database. Available online: https://healthcarelca.com/database (accessed on 5 May 2025).
- Keil, M.; Viere, T.; Helms, K.; Rogowski, W. The impact of switching from single-use to reusable healthcare products: A transparency checklist and systematic review of life-cycle assessments. Eur. J. Public Health 2023, 33, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Rizan, C.; Steinbach, I.; Nicholson, R.; Lillywhite, R.; Reed, M.; Bhutta, M.F. The Carbon Footprint of Surgical Operations: A Systematic Review. Ann. Surg. 2020, 272, 986–995. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Jiménez, L.; Romero-Martín, M.; Spruell, T.; Steley, Z.; Gómez-Salgado, J. The carbon footprint of healthcare settings: A systematic review. J. Adv. Nurs. 2023, 79, 2830–2844. [Google Scholar] [CrossRef] [PubMed]
- Ortsäter, G.; Borgström, F.; Baldwin, M.; Miltenburger, C. Incorporating the Environmental Impact into a Budget Impact Analysis: The Example of Adopting RESPIMAT® Re-usable Inhaler. Appl. Health Econ. Health Policy 2020, 18, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Ortsäter, G.; Borgström, F.; Soulard, S.; Miltenburger, C. A Budget Impact Model to Estimate the Environmental Impact of Adopting RESPIMAT® Re-usable in the Nordics and Benelux. Adv. Ther. 2019, 36, 3435–3445. [Google Scholar] [CrossRef] [PubMed]
- Bundesinstitut für Arnzeimittel und Medizinprodukte. BfArM-OPS, ICHI. Available online: https://www.bfarm.de/DE/Kodiersysteme/Klassifikationen/OPS-ICHI/_node.html (accessed on 16 February 2026).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LCA-Phase | Subcategories | Care-Pathways | Service LCA Studies | Interpretation of Alignment |
|---|---|---|---|---|
| Goal and Scope | Functional/declared unit | Defined by care pathway characteristics (illness, severity, patient, location, duration). | Defined predominantly as number of practices, with strong preference for one procedure, occasionally provision over time period (one year) | Practice operationalises procedure-based rather than pathway-based |
| System boundary | Flexible: cradle-to-gate or cradle-to-grave. | Cadle-to-grave and door-to-door. | Partial alignment; practice reflects both life cycle-based and spatial-based boundary interpretation | |
| Life cycle stages | Modular pathway structure (e.g., consultation, inpatient stay, surgery) incl. consumables, equipment, direct emissions, facilities data, staff travel, support services/admin. If applicable: pharmaceuticals, patient food. | Includes raw materials, production, transport, electricity use, pharmaceuticals, patient/staff transport, disposal. | Structural modelling mismatch between modular healthcare processes and patient flows rather than conventional upstream and downstream processes | |
| Life Cycle Inventory | Data collection | Primary data for processes under control; secondary data otherwise. | Combination of hybrid and process-based data. | Broad methodological alignment |
| Life Cycle Impact Assessment | Selection of impact categories and models | Limited set: IPCC GWP 100, Global Water Footprint Standard, waste indicator. | Broad use: IPCC, TRACI, ReCiPe. | Guidance prescribes limited indicators, practice applies generic LCA methods |
| Interpret-ation | Assessment | Parameter, scenario, and model uncertainty; qualitative statements required, quantitative recommended. | Contribution, comparative, and sensitivity analyses frequently used. | Partial methodological convergence but no standardised reporting structure |
| LCA-Phase | Subcategories | GHG-P&M | Product LCA Studies | Interpretation of Alignment |
|---|---|---|---|---|
| Goal and Scope | Functional/declared unit | Flexible; defined per product or per use. Guiding questions on nature, quantity, duration, and context of use. | Typically amount-based or use-based, followed by practice-based FU (predominantly one item/use/procedure). Pharmaceuticals also Mass of Item. | Practice shows greater heterogeneity and occasional practice-oriented framing |
| System boundary | Cradle-to-grave, pharmaceuticals also cradle-to-gate. | Mostly cradle-to-grave; pharmaceuticals also cradle-to-gate | Broad alignment (cradle-to-grave approaches dominate both guidance and practice) | |
| Life cycle stages | Excludes: research and development, capital goods, overhead operations, corporate activities. | Staff transport, building energy use, and infrastructure were each included in only a single study. | Not all guidance-defined stages in practice included | |
| Life Cycle Inventory | Data collection | Primary data for processes under control; secondary for external processes; focus on major contributors (>10%). | Predominantly process-based data; hybrid models occasionally used. | Broad alignment |
| Life Cycle Impact Assessment | Selection of impact categories and models | Limited to IPCC (carbon footprint). | Broader use (ReCiPe, IPCC, CML, others). | Standard limited to carbon, while studies apply multi-impact assessment |
| Interpret-ation | Assessment | Qualitative assessment of parameter, scenario, and model uncertainty; quantitative analysis encouraged; reporting required but no standardised format. | Sensitivity, comparative, and contribution analyses; heterogeneous reporting formats. | Similar methods but no harmonised reporting |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Zecha, F.; Hupperich, L.-M.; Viere, T. Life Cycle Assessments in Healthcare: Insights and Standardisation Needs. Int. J. Environ. Res. Public Health 2026, 23, 828. https://doi.org/10.3390/ijerph23070828
Zecha F, Hupperich L-M, Viere T. Life Cycle Assessments in Healthcare: Insights and Standardisation Needs. International Journal of Environmental Research and Public Health. 2026; 23(7):828. https://doi.org/10.3390/ijerph23070828
Chicago/Turabian StyleZecha, Franziska, Lena-Marie Hupperich, and Tobias Viere. 2026. "Life Cycle Assessments in Healthcare: Insights and Standardisation Needs" International Journal of Environmental Research and Public Health 23, no. 7: 828. https://doi.org/10.3390/ijerph23070828
APA StyleZecha, F., Hupperich, L.-M., & Viere, T. (2026). Life Cycle Assessments in Healthcare: Insights and Standardisation Needs. International Journal of Environmental Research and Public Health, 23(7), 828. https://doi.org/10.3390/ijerph23070828