


A Transect Through the Living Environments of Slovakia’s Roma Population: Urban, Sub-Urban, and Rural Settlements, and Exposure to Environmental and Water-Related Health Risks
 ,
,  ,
,  ,
,
Abstract
1. Introduction
- provide deep insights into the living environments of Slovakia’s Roma population;
- compare living conditions in settlements at different levels of centrality, including urban, peri-urban, and rural;
- analyse the occurrence of endoparasite diseases in different Roma settlements across Slovakia, thereby offering a comprehensive view of the overall health of people, animals, and the living environment.
2. Methods
2.1. Conceptual Framing
2.2. Methodological Approach
2.3. Desk Study
2.3.1. Data Collection
- Inside settlements, located within the main village core, including streets, apartment buildings, and yards that host more than 30 Roma inhabitants but remain an integral part of the village’s development area.
- Edge settlements, situated on the outskirts of the village core, where houses in the main part of the village gradually transition to the periphery, forming a Roma concentration immediately adjacent to the village’s development area.
- Outside settlements, located outside the village core, defined as concentrations separated from the main village development area by undeveloped land, railway lines, rivers/streams, or roads.
2.3.2. Data Analysis
2.4. Parasitological Analysis
2.4.1. Data Collection
2.4.2. Data Analysis
3. Results
3.1. Transect Through Roma Living Conditions
3.2. Living Conditions of Roma People in Settlements at Different Levels of Centrality
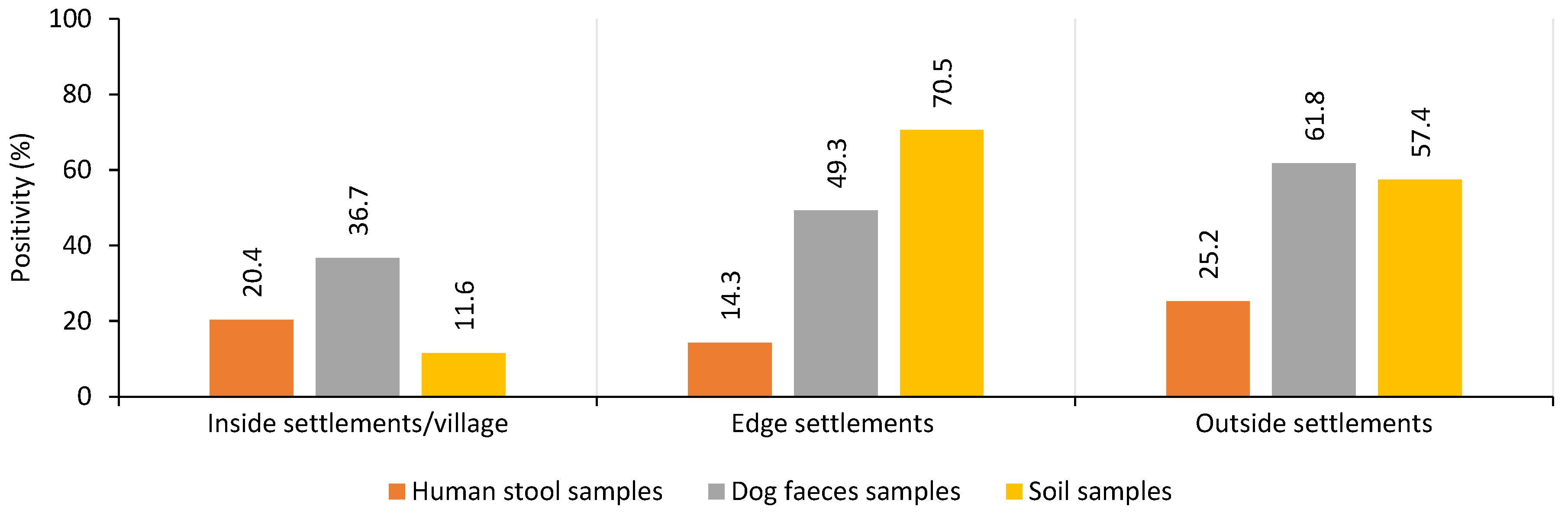
3.3. Parasitological Results
4. Discussion
4.1. Filling Knowledge Gaps on Water and Health Insecurity in Different Roma Living Environments
4.2. Root Causes of Water and Health Insecurity Among These Marginalised Groups
4.3. WASH and Resulting Health Insecurity in Roma Settlements
4.4. Using Evidence for Targeted Interventions and to Improve Health-Promoting Planning
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Greenwood, E.E.; Lauber, T.; van den Hoogen, J.; Donmez, A.; Bain, R.E.S.; Johnston, R.; Crowther, T.W.; Julian, T.R. Mapping safe drinking water use in low- and middle-income countries. Science 2024, 363, 537–543. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Soil-Transmitted Helminth Infections. Available online: https://www.who.int/news-room/fact-sheets/detail/soil-transmitted-helminth-infections (accessed on 1 July 2024).
- UN-Water. Summary Progress Update 2021: SDG 6—Water and Sanitation for All. Available online: https://www.unwater.org/sites/default/files/app/uploads/2021/12/SDG-6-Summary-Progress-Update-2021_Version-July-2021a.pdf (accessed on 1 July 2024).
- Joint Monitoring Programme for Water Supply, Sanitation and Hygiene by World Health Organization/UNICEF (JMP). Estimates for Drinking water, Sanitation and Hygiene Services by Country (2000–2022). Available online: https://data.unicef.org/resources/jmp-report-2023 (accessed on 1 July 2024).
- Parekh, N.; Rose, T. Health inequalities of the roma in Europe: A literature review. Cent. Eur. J. Public Health 2011, 19, 139–142. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Roma Integration in the EU. Facts and Figures on EU’s Roma Population and Integration Strategies for Improving the Living Conditions of Roma in EU Countries. 2020. Available online: https://ec.europa.eu/info/policies/justice-and-fundamental-rights/combatting-discrimination/roma-and-eu/roma-integration-eu_en (accessed on 1 July 2024).
- Lecerf, M. Understanding EU Action on Roma Inclusion. EPRS|European Parliamentary Research Service, PE 690.629. Available online: https://www.europarl.europa.eu/RegData/etudes/BRIE/2021/690629/EPRS_BRI(2021)690629_EN.pdf (accessed on 1 July 2024).
- Britannica, The Editors of Encyclopaedia. Roma. Encyclopedia Britannica. Available online: https://www.britannica.com/topic/Rom (accessed on 1 July 2024).
- Popper, M.; Szeghy, P.; Šarkozy, Š. Rómska Populácia a Zdravie: Analýza Situácie na Slovensku [Roma Community and Health: Analysis of the Situation in Slovakia]; FSG: Madrid, Spain, 2009; Available online: http://www.gitanos.org/upload/13/60/Eslovaquia-corrected.pdf (accessed on 1 July 2024).
- Brown, J.; Acey, C.S.; Anthonj, C.; Barrington, D.J.; Beal, C.D.; Capone, D.; Cumming, O.; Pullen Fedinick, K.; MacDonald Gibson, J.; Hicks, B.; et al. Rich countries lack universal safe water and sanitation due to social exclusion, racism, and inaction. Lancet Glob. Health 2023, 11, 76–85. [Google Scholar] [CrossRef]
- Anthonj, C.; Setty, K.E.; Ezbakhe, F.; Manga, M.; Hoeser, C.H. A systematic review of water, sanitation and hygiene among Roma communities in Europe: Situation analysis, cultural context, and obstacles to improvement. Int. J. Hyg. Environ. Health 2020, 226, 113506. [Google Scholar] [CrossRef]
- Ihnacik, L.; Šmigová, J.; Šoltys, J.; Bobíková, D.; Kuzevičová, Ž.; Kuzevič, Š.; Schusterová, I.; Papajová, I. The survey of soil-transmitted helminth species abundance in Slovakia with an emphasis on parameters important for their distribution. Front. Med. 2022, 9, 1043313. [Google Scholar] [CrossRef] [PubMed]
- Wakid, M.H.; Azhar, E.I.; Zafar, T.A. Intestinal parasitic infection among food handlers in holy city Makkah during Hajj season 1428 Hegira. Med. Sci. 2009, 16, 4–8. [Google Scholar]
- Bogitsh, B.J.; Carter, C.E.; Oeltmann, T.N. Chapter 16—Intestinal nematodes. In Human Parasitology, 4th ed.; Bogitsh, B.J., Carter, C.E., Oeltmann, T.N., Eds.; Academic Press: San Diego, CA, USA, 2013; pp. 291–327. [Google Scholar]
- Ravasz, A.; Kovács, Ľ.; Markovič, F. Atlas Rómskych Komunít 2019 [Atlas of Roma Communities 2019]; VEDA: Bratislava, Slovakia, 2020; Available online: https://www.institutmatejabela.sk/atlas (accessed on 10 August 2024).
- Ruzicka, M. Continuity or rupture? Roma/Gypsy communities in rural and urban environments under post-socialism. J. Rural Stud. 2012, 28, 81–88. [Google Scholar] [CrossRef]
- SOBD. Sčítanie Obyvateľov, Domov a Bytov [Census of Inhabitants, Houses and Apartments]; The Statistical Office of the SR (SO SR): Bratislava, Slovakia, 2022; Available online: https://www.scitanie.sk/ (accessed on 18 October 2024).
- Tobler, W. A computer movie simulating urban growth in the Detroit region. Econ. Geogr. 1970, 46, 234–240. [Google Scholar] [CrossRef]
- Mayer, J.D. Relation between two traditions of medical geography: Health systems planning and geographical epidemiology. Prog. Hum. Geogr. 1982, 6, 216–230. [Google Scholar] [CrossRef]
- Bernard, P.; Charafeddine, R.; Frohlich, K.L.; Daniel, M.; Kestens, Y.; Potvin, L. Health inequalities and place: A theoretical conception of neighbourhood. Social Sci. Med. 2007, 65, 1839–1852. [Google Scholar] [CrossRef]
- Curtis, S.; Rees Jones, I. Is There a Place for Geography in the Analysis of Health Inequality? Sociol. Health Illn. 1998, 20, 645–672. [Google Scholar] [CrossRef]
- Kobetz, E.; Daniel, M.; Earp, J.-A. Neighborhood poverty and self-reported health among low-income, rural women, 50 years and older. Health Place 2003, 9, 263–271. [Google Scholar] [CrossRef]
- Lerner, H.; Berg, C.A. Comparison of Three Holistic Approaches to Health: One Health, EcoHealth, and Planetary Health. Front. Vet. Sci. 2017, 4, 163. [Google Scholar] [CrossRef]
- Zinsstag, J.; Schelling, E.; Waltner-Toews, D.; Tanner, M. From “one medicine” to “one health” and systemic approaches to health and well-being. Prev. Vet. Med. 2011, 101, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Dickin, S.; Dagerskog, L.; Dione, M.; Thomas, L.; Arcilla, J. Towards a one health approach to WASH to tackle zoonotic disease and promote health and wellbeing. PLoS Water 2025, 4, e0000376. [Google Scholar] [CrossRef]
- Sivašová, D. Bývanie a Životné Podmienky Rómov na Slovensku [Housing and Living Conditions of Roma in Slovakia]; Economical university in Bratislava: Bratislava, Slovakia, 2017; Volume 15, pp. 91–104. (In Slovak) [Google Scholar]
- Kazacos, K.R. Improved method for recovering ascarid and other helminth eggs from soil associated with epizootics and during survey studies. Am. J. Vet. Res. 1983, 44, 896–900. [Google Scholar] [CrossRef]
- Koupilová, I.; Epstein, H.; Holcík, J.; Hajioff, S.; McKee, M. Health needs of the Roma population in the Czech and Slovak Republics. Soc. Sci. Med. 2001, 53, 119–127. [Google Scholar] [CrossRef]
- ÚVZ SR. Úrad Verejného Zdravotníctva Slovenskej Republiky [Public Health Authority of the Slovak Republic]. Available online: https://www.uvzsr.sk/web/uvz (accessed on 10 June 2025).
- Filčák, R.; Szilvasi, M.; Škobla, D. No water for the poor: The Roma ethnic minority and local governance in Slovakia. Ethn. Racial Stud. 2017, 40, 2483–2501. [Google Scholar] [CrossRef]
- Chaudhuri, I.N. Community mobilization for slum upgrading through sanitation in Roma informal settlements in the Paris region. Front. Public Health 2017, 5, 213. [Google Scholar] [CrossRef] [PubMed]
- Chandana, N.; Rao, B. Status of sustainable sanitation chain in rural, semi-urban, and urban regions: A case study of Maharashtra, India. J. Water Sanit. Hyg. Dev. 2021, 11, 112–125. [Google Scholar] [CrossRef]
- Marks, S.J.; Clair-Caliot, G.; Taing, L.; Bamwenda, J.T.; Kanyesigye, C.; Rwendeire, N.E.; Kemerink-Seyoum, J.S.; Kansiime, F.; Batega, D.W.; Ferrero, G. Water supply and sanitation services in small towns in rural–urban transition zones: The case of Bushenyi-Ishaka Municipality, Uganda. NPJ Clean. Water 2020, 3, 21. [Google Scholar] [CrossRef]
- Pullan, R.L.; Freeman, M.C.; Gething, P.W.; Brooker, S. Geographical inequalities in use of improved drinking water supply and sanitation across sub-Saharan Africa: Mapping and spatial analysis of cross-sectional survey data. PLoS Med. 2014, 11, e1001626. [Google Scholar] [CrossRef]
- Pipiková, J.; Papajová, I.; Šoltys, J.; Schusterová, I.; Kočišová, D.; Toháthyová, A. Segregated settlements present an increased risk for the spread of parasite infections in Northeastern Slovakia. Helminthologia 2017, 54, 136–142. [Google Scholar] [CrossRef]
- Mehlhorn, H. Human Parasites; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Pipiková, J.; Papajová, I.; Šoltys, J.; Schusterová, I. Occurrence of the most common helminth infections among children in the Eastern Slovak Republic. Public Health 2017, 146, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Antolová, D.; Reiterová, K.; Miterpáková, M.; Stanko, M.; Dubinský, P. Circulation of Toxocara spp. in suburban and rural ecosystems in the Slovak Republic. Vet. Parasitol. 2004, 123, 91–98. [Google Scholar] [CrossRef]
- Mušinka, A.; Škobla, D.; Hurrle, J.; Matlovičová, K.; Kling, J. Atlas Rómskych Komunít na Slovensku 2013 [Atlas of Roma Communities 2013]; UNDP, Agentúra pre Sociálnu Inklúziu: Banská Bystrica, Slovakia, 2014. [Google Scholar]
- Joint Monitoring Program (JMP). On Progress on Household Drinking Water, Sanitation and Hygiene 2000–2022: Special Focus on Gender; United Nations Children’s Fund (UNICEF): New York, NY, USA; World Health Organization (WHO): Geneva, Switzerland, 2023; Available online: https://washdata.org/reports/jmp-2023-wash-households (accessed on 1 July 2024).
- Anthonj, C.; Stanglow, N.S.; Flacke, J.; Manga, M.; Leinen, A.; Grunwald, N. A question of human dignity: Identifying solutions to improve WASH for people experiencing homelessness. A case study from Germany. Water Secur. 2024, 22, 100176. [Google Scholar] [CrossRef]
- Kluvankova, T.; Nijnik, M.; Spacek, M.; Sarkki, S.; Perlik, M.; Lukesch, R.; Melnykovych, M.; Valero, D.; Brnkalakova, S. Social innovation for sustainability transformation and its diverging development paths in marginalised rural areas. Sociol. Rural. 2021, 61, 554–578. [Google Scholar] [CrossRef]
- Lombardi, M.; Lopolito, A.; Andriano, A.M.; Prosperi, M.; Stasi, A.; Iannuzzi, E. Network impact of social innovation initiatives in marginalised rural communities. Soc. Netw. 2020, 63, 11–20. [Google Scholar] [CrossRef]
- Winston, N. Sustainable community development: Integrating social and environmental sustainability for sustainable housing and communities. Sustain. Dev. 2022, 30, 191–202. [Google Scholar] [CrossRef]
- Masseria, C.; Mladovsky, P.; Hernández-Quevedo, C. The socio-economic determinants of the health status of Roma in comparison with non-Roma in Bulgaria, Hungary and Romania. Eur. J. Public. Health 2010, 20, 549–554. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Category | Factors | Type of Data |
|---|---|---|
| Population | Number of inhabitants per settlement | Average number of people calculated from an interval of the estimate of inhabitants living in settlements |
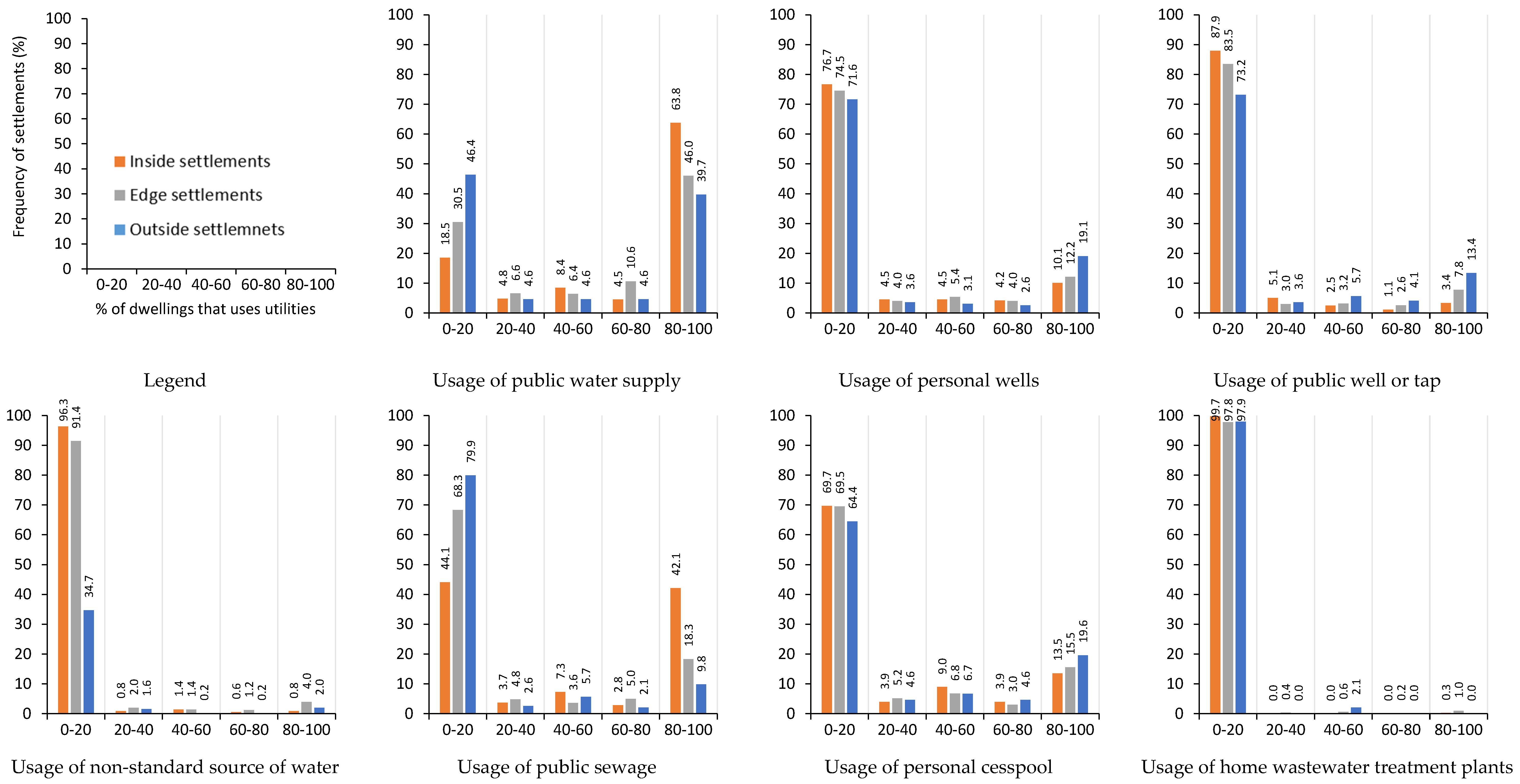
| Water sources | Usage of public water supply | Percentage of dwellings that rely on each type of water source |
| Usage of personal wells | ||
| Usage of public wells or taps | ||
| Usage of non-standard water source (nearby streams, rivers) | ||
| Waste disposal | Usage of public sewage | Percentage of dwellings that rely on each type of waste and wastewater disposal |
| Usage of a personal cesspool | ||
| Usage of home wastewater treatment plants | ||
| Ownership of waste receptacle | ||
| Flooding | Floods | Percentage of settlements having previously experienced natural disaster |
| Other natural disasters | ||
| Distance to health care | Distance to general practitioners | Distance from settlement to facility in kilometers |
| Distance to paediatricians | ||
| Infrastructure | Distance to bus stop | Distance from settlement to facility in kilometers |
| Distance to train stop | ||
| Housing | Dwelling ownership | Number of houses with different ownership and house type |
| House types | ||
| Density in dwellings | Average number of people per dwelling calculated from average number of people and number of dwellings | |
| Energy | Household connectivity to the electricity grid | Percentage of dwellings in each settlements which relies on them |
| Household connectivity to the gas distribution system |
| Level of Centrality | Urban | Sub-Urban | Natural/Rural |
|---|---|---|---|
| Location of Settlements | Settlement Located Inside Village | Settlements Located at the Edge of Villages | Settlements Located Outside the Main Village |
| Map * |  |  |  |
| Images * |  |  |  |
| Water source | The majority of dwellings have access to safe and reliable water sources (>70% public supply). | 60% of dwellings connected to public supply, around 20% use personal wells. | 47% of dwellings are connected to public supply. 24% use personal wells, 21% public wells, 8% non-standard source. |
| Wastewater, waste disposal | Half of the dwellings are connected to public sewerage systems, 73% have safe wastewater removal. 84% have their own waste containers. | About 53% of dwellings have safe wastewater disposal. 72% of dwellings have waste containers. | 44% of the dwellings have safe wastewater disposal. 57% of dwellings have their own waste containers. |
| Flooding | 16% had experienced flooding events, and nearly 9% of settlements had faced other natural disasters. | 33% had experienced flooding events, and 23% had faced other natural disasters. | 25% of settlements had experienced flooding events, and 16% had faced other natural disasters. |
| Distance to healthcare | The average distance to the nearest GP is 1.8 km. The average distance to a paediatrician is 3.6 km. | The average distance to the nearest GP is 4 km. The average distance to a paediatrician is 5.6 km. | The average distance to a GP is 5 km. The average distance to a paediatrician is 6.5 km. |
| Infrastructure | The closest bus stop is only a few 100 m away. The closest train stop is about 6 km away. | The closest bus stop is only a few 100 m away. The closest train stop is about 9 km away. | The closest bust stop is within 1 km of the settlement. The closest train station is about 8 km away. |
| Housing | Average of 1–2 unapproved brick houses, 0–1 unapproved wood houses, 0–1 unapproved huts. | Average of 7–8 unapproved brick houses, 0–1 unapproved wood houses, 5–6 unapproved huts. | Average of 7 unapproved brick houses, 2–3 unapproved wood houses, 10–11 unapproved huts. |
| Energy | 93% of dwellings are connected to electricity grid, 30% with access to gas distribution system. | 85% of dwellings are connected to the electricity grid, 16% connected to the gas distribution system. | 80% of dwellings connected to electricity grid, 4% connected to gas distribution system. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ihnacik, L.; Papajová, I.; Šmigová, J.; Brussel, M.; Manga, M.; Papaj, J.; Schusterová, I.; Anthonj, C. A Transect Through the Living Environments of Slovakia’s Roma Population: Urban, Sub-Urban, and Rural Settlements, and Exposure to Environmental and Water-Related Health Risks. Int. J. Environ. Res. Public Health 2025, 22, 988. https://doi.org/10.3390/ijerph22070988
Ihnacik L, Papajová I, Šmigová J, Brussel M, Manga M, Papaj J, Schusterová I, Anthonj C. A Transect Through the Living Environments of Slovakia’s Roma Population: Urban, Sub-Urban, and Rural Settlements, and Exposure to Environmental and Water-Related Health Risks. International Journal of Environmental Research and Public Health. 2025; 22(7):988. https://doi.org/10.3390/ijerph22070988
Chicago/Turabian StyleIhnacik, Lukáš, Ingrid Papajová, Júlia Šmigová, Mark Brussel, Musa Manga, Ján Papaj, Ingrid Schusterová, and Carmen Anthonj. 2025. "A Transect Through the Living Environments of Slovakia’s Roma Population: Urban, Sub-Urban, and Rural Settlements, and Exposure to Environmental and Water-Related Health Risks" International Journal of Environmental Research and Public Health 22, no. 7: 988. https://doi.org/10.3390/ijerph22070988
APA StyleIhnacik, L., Papajová, I., Šmigová, J., Brussel, M., Manga, M., Papaj, J., Schusterová, I., & Anthonj, C. (2025). A Transect Through the Living Environments of Slovakia’s Roma Population: Urban, Sub-Urban, and Rural Settlements, and Exposure to Environmental and Water-Related Health Risks. International Journal of Environmental Research and Public Health, 22(7), 988. https://doi.org/10.3390/ijerph22070988