

Education of Occupational Therapists in Mental Health: A Global Survey of Educators Regarding Perceived Facilitators and Barriers

 , ,
on behalf of the World Federation of Occupational Therapists
, ,
on behalf of the World Federation of Occupational Therapists
Abstract
1. Introduction
2. Method
2.1. Overview
2.2. Survey Design
2.3. Survey Procedures
2.4. Analysis
3. Results
3.1. Participants
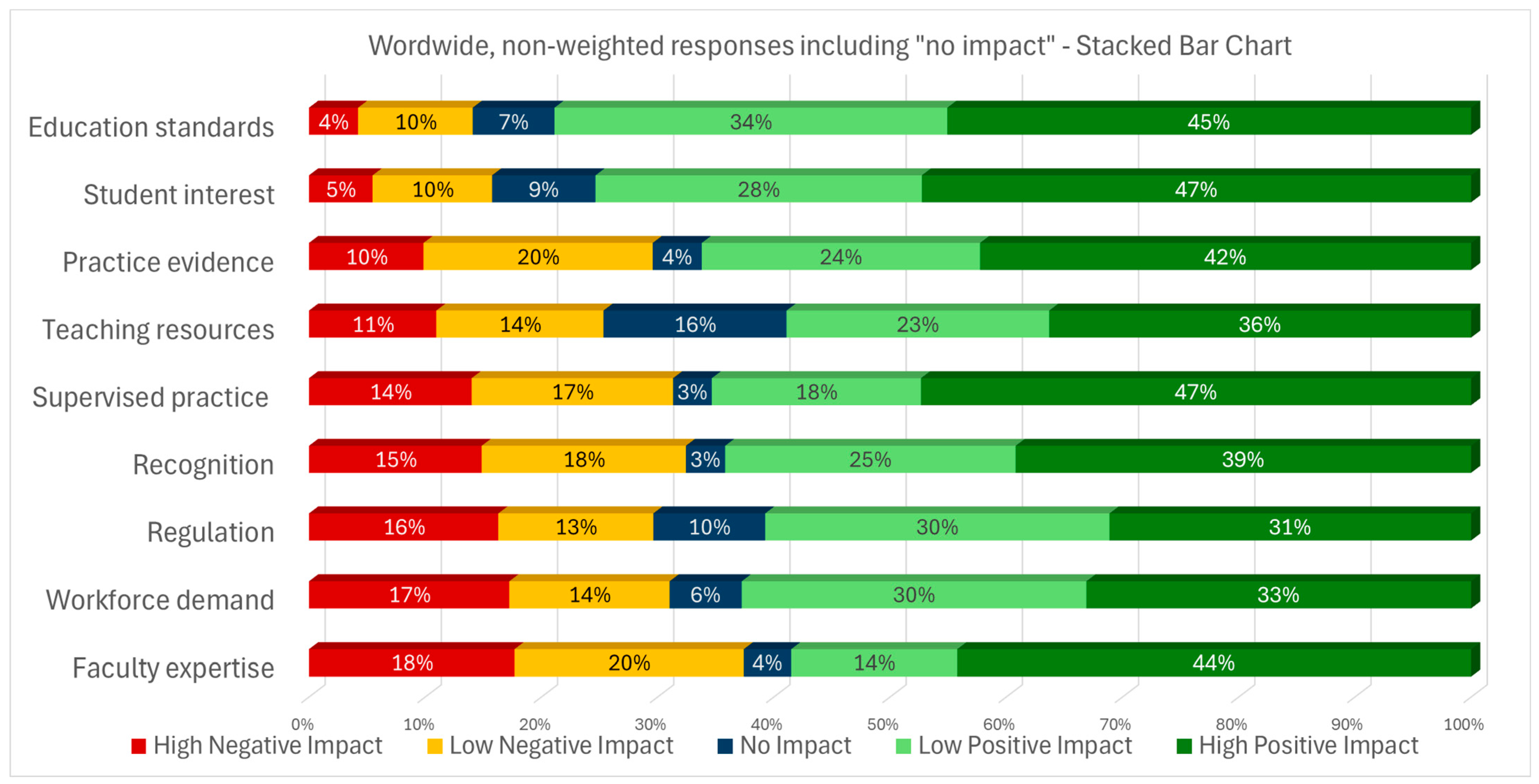
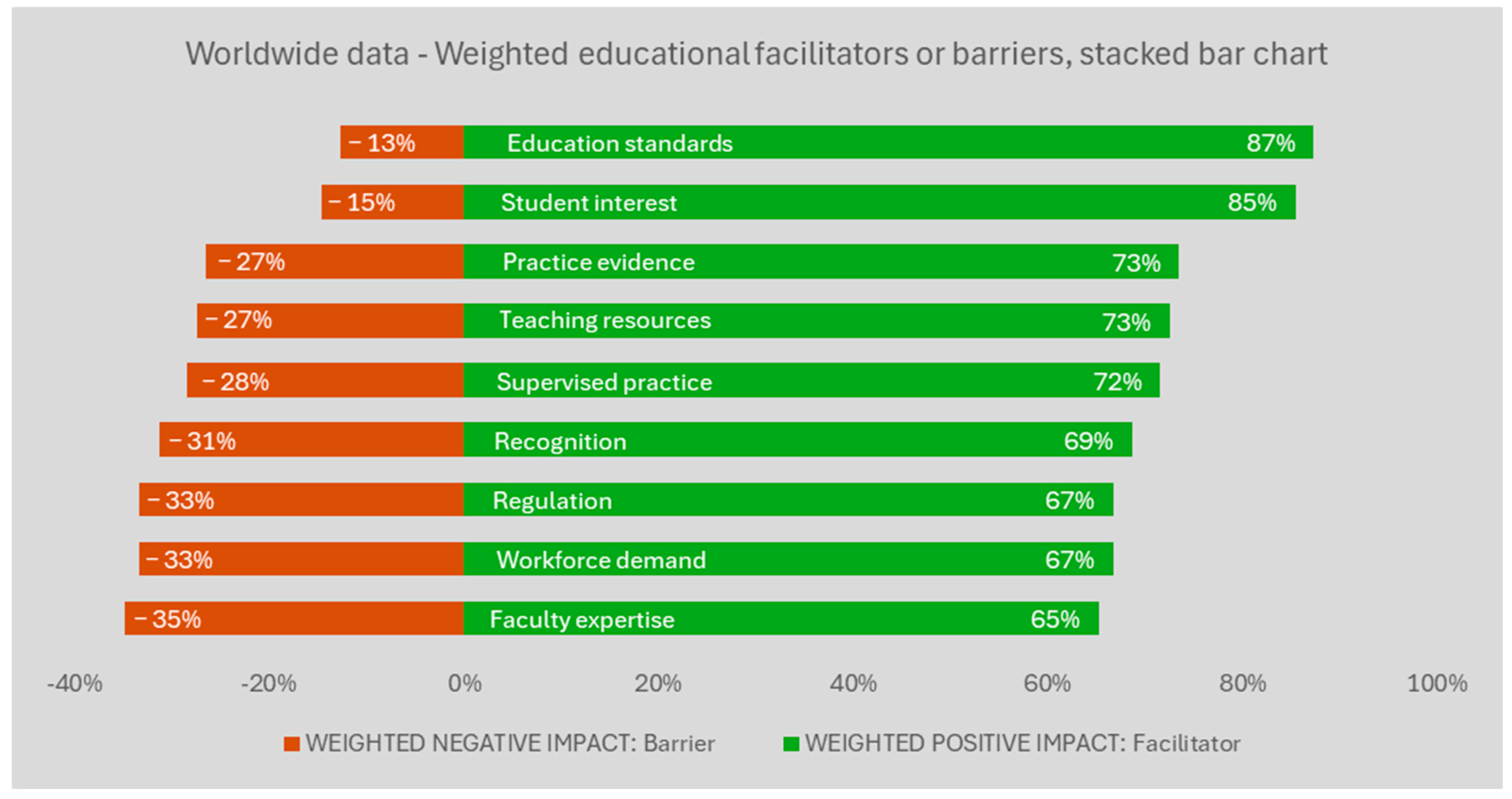
3.2. Results for All Respondents
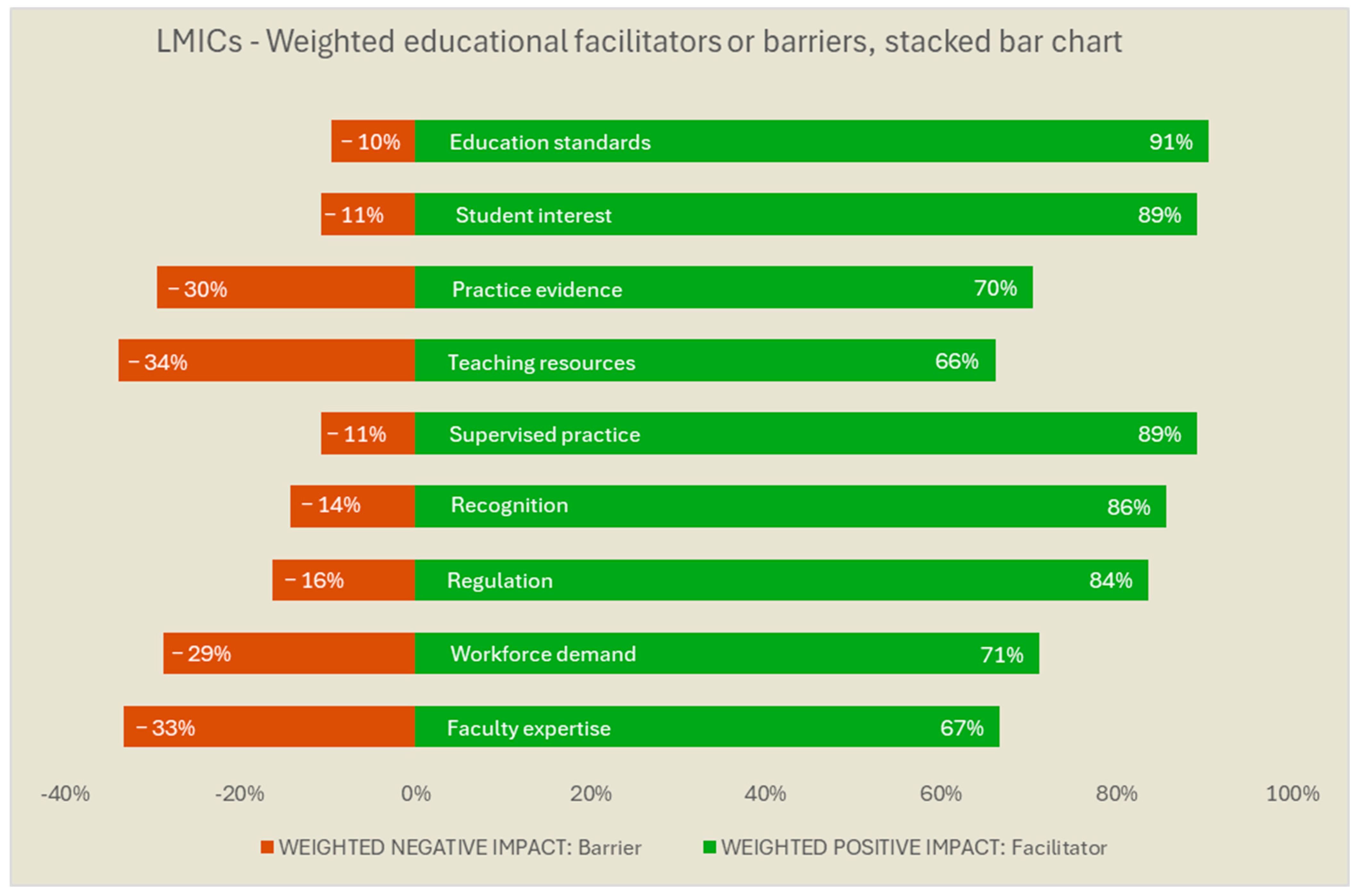
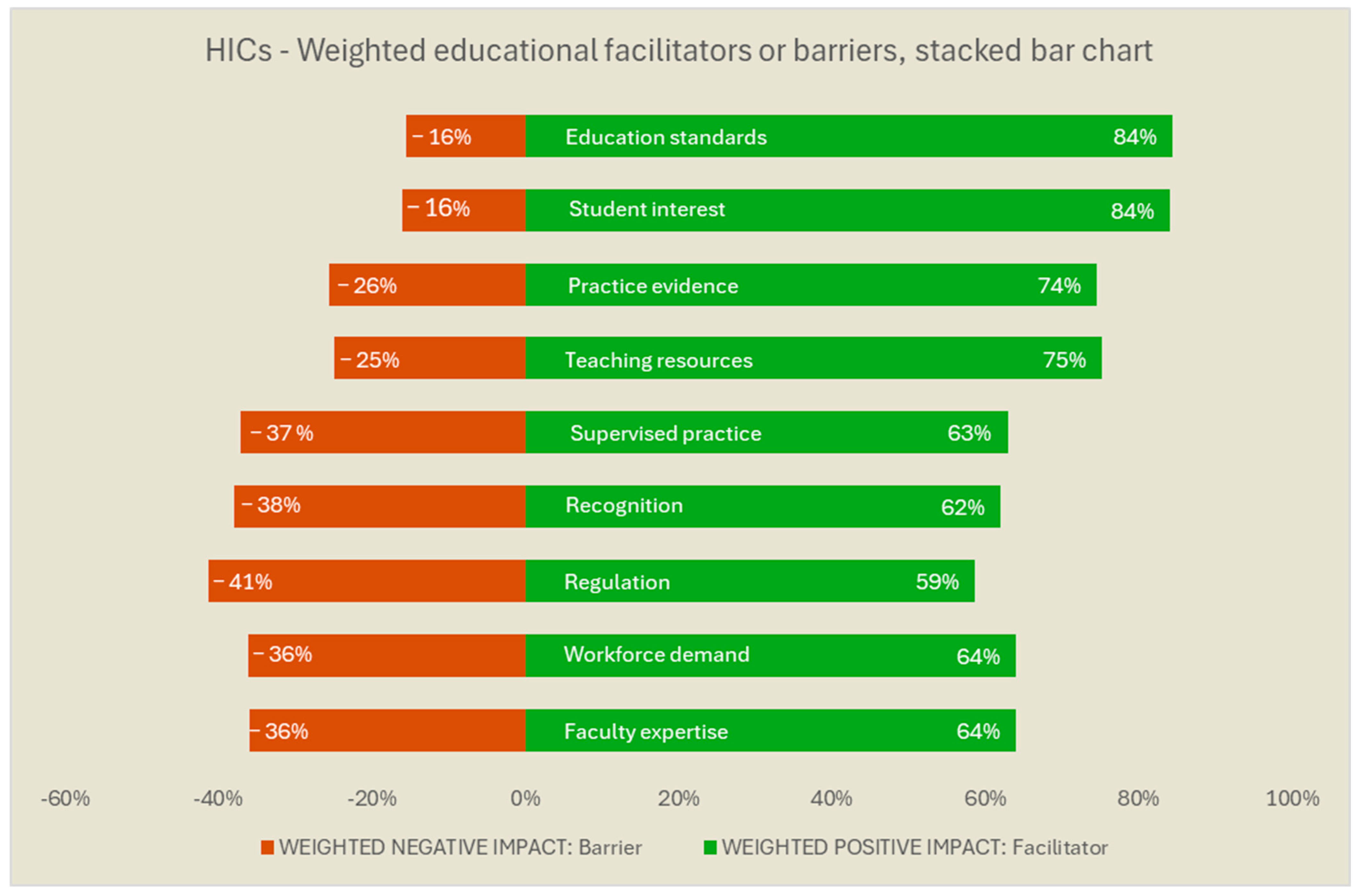
3.3. Stratification by HICs and LMICs
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MH | Mental Health |
| WFOT | World Federation of Occupational Therapists |
References
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- World Health Organization. World Mental Health Report: Transforming Mental Health for All; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Krupa, T.; Fossey, E.; Anthony, W.A.; Brown, C.; Pitts, D.B. Doing daily life: How occupational therapy can inform psychiatric rehabilitation practice. Psychiatr. Rehabil. J. 2009, 32, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Galderisi, S.; Heinz, A.; Kastrup, M.; Beezhold, J.; Sartorius, N. Toward a new definition of mental health. World Psychiatry 2015, 14, 231–233. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- World Federation of Occupational Therapists. Occupational Therapy and Human Rights (Revised); WFOT: London, UK, 2019. [Google Scholar]
- Sedgwick, A.; Cockburn, L.; Trentham, B. Exploring the mental health roots of occupational therapy in Canada: A historical review of primary texts from 1925–1950. Can. J. Occup. Ther. 2007, 74, 407–417. [Google Scholar] [PubMed]
- Shepherd, H.A.; Jesus, T.S.; Nalder, E.; Dabbagh, A.; Colquhoun, H. Occupational Therapy Research Publications From 2001 to 2020 in PubMed: Trends and Comparative Analysis with Physiotherapy and Rehabilitation. OTJR 2024, 15394492241292438. [Google Scholar] [CrossRef] [PubMed]
- García-Gestal, U.; Talavera-Valverde, M.; Souto-Gómez, A.I. Occupational Therapy in Psychiatric Short-Term Hospitalization Units: Scoping Review. Community Ment. Health J. 2024, 60, 1283–1307. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and Process-Fourth Edition. Am. J. Occup. Ther. 2020, 74 (Suppl. S2), 7412410010p1–7412410010p87. [Google Scholar] [CrossRef] [PubMed]
- Read, H.; Zagorac, S.; Neumann, N.; Kramer, I.; Walker, L.; Thomas, E. Occupational Therapy: A Potential Solution to the Behavioral Health Workforce Shortage. Psychiatr. Serv. 2024, 75, 703–705. [Google Scholar] [CrossRef] [PubMed]
- Christie, L.; Inman, J.; Davys, D.; Cook, P.A. A systematic review into the effectiveness of occupational therapy for improving function and participation in activities of everyday life in adults with a diagnosis of depression. J. Affect. Disord. 2021, 282, 962–973. [Google Scholar] [CrossRef] [PubMed]
- Ikiugu, M.N.; Nissen, R.M.; Bellar, C.; Maassen, A.; Van Peursem, K. Clinical Effectiveness of Occupational Therapy in Mental Health: A Meta-Analysis. Am. J. Occup. Ther. 2017, 71, 7105100020p1–7105100020p10. [Google Scholar] [CrossRef]
- Noyes, S.; Lannigan, E.G. Occupational Therapy Practice Guidelines for Adults Living with Serious Mental Illness; AOTA Press: Bethesda, MD, USA, 2019. [Google Scholar] [CrossRef]
- Jesus, T.S.; Mani, K.; Bhattacharjya, S.; Kamalakannan, S.; von Zweck, C.; Ledgerd, R. Situational analysis for informing the global strengthening of the occupational therapy workforce. Int. J. Health Plan. Manag. 2023, 38, 527–535. [Google Scholar] [CrossRef] [PubMed]
- World Federation of Occupational Therapists. Top 3 Specific Practice Areas with a Shortage of Occupational Therapists. 2024. Available online: https://hr-project.wfot.org/#top3shortageAreas (accessed on 16 May 2025).
- Jesus, T.S.; Mani, K.; von Zweck, C.; Kamalakannan, S.; Bhattacharjya, S.; Ledgerd, R.; World Federation of Occupational Therapists. Type of Findings Generated by the Occupational Therapy Workforce Research Worldwide: Scoping Review and Content Analysis. Int. J. Environ. Res. Public Health 2022, 19, 5307. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- American Occupational Therapy Association. Workforce and Salary Survey Bethesda; AOTA: North Bethesda, MD, USA, 2019. [Google Scholar]
- US Bureau of Labor Statistics. Occupational Employment and Wage Statistics Washinghton, DC, USA. 2023. Available online: https://www.bls.gov/oes/2022/may/naics5_621330.htm (accessed on 16 May 2025).
- Yan, W.; Ohlsen, S.; Wood, E. Factors affecting retention of occupational therapists in adult mental health service: A systematic review with narrative synthesis. Br. J. Occup. Ther. 2025, 88, 70–84. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kaiser Family Foundation. Mental Health Care Health Professional Shortage Areas (HPSAs). 2024. Available online: https://www.kff.org/other/state-indicator/mental-health-care-health-professional-shortage-areas-hpsas/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Percent%20of%20Need%20Met%22,%22sort%22:%22asc%22%7D (accessed on 16 May 2025).
- Keptner, K.; Lambdin-Pattavina, C.; Jalaba, T.; Nawotniak, S.; Cozzolino, M. Preparing for and Responding to the Current Mental Health Tsunami: Embracing Mary Reilly’s Call to Action. Am. J. Occup. Ther. 2024, 78, 7801347010. [Google Scholar] [CrossRef] [PubMed]
- The World Federation of Occupational Therapists. Position Statement: Occupational Therapy and Mental Health; The World Federation of Occupational Therapists: London, UK, 2019. [Google Scholar]
- Jesus, T.S.; Landry, M.D.; Dussault, G.; Fronteira, I. Classifying and Measuring Human Resources for Health and Rehabilitation: Concept Design of a Practices- and Competency-Based International Classification. Phys. Ther. 2019, 99, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Jesus, T.; Monteiro, P.; Ledgerd, R.; vom Zweck, C. Barriers and Facilitators for the Practice of Occupational Therapy in Mental Health: Findings from a Global Practitioner Survey of the World Federation of Occupational Therapists. Preprints 2025. [Google Scholar] [CrossRef]
- Scanlan, J.N.; Pépin, G.; Haracz, K.; Ennals, P.; Webster, J.S.; Meredith, P.J.; Batten, R.; Bowman, S.; Bonassi, M.; Bruce, R. Identifying educational priorities for occupational therapy students to prepare for mental health practice in Australia and New Zealand: Opinions of practising occupational therapists. Aust. Occup. Ther. J. 2015, 62, 286–298. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjya, S.; Curtis, S.; Kueakomoldej, S.; von Zweck, C.; Russo, G.; Mani, K.; Kamalakannan, S.; Ledgerd, R.; Jesus, T.S.; World Federation of Occupational Therapists. Developing a Global Strategy for strengthening the occupational therapy workforce: A two-phased mixed-methods consultation of country representatives shows the need for clarifying task-sharing strategies. Hum. Resour. Health 2024, 22, 62. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jesus TSvon Zweck, C.; Bhattacharjya, S.; Mani, K.; Kamalakannan, S.; Ledgerd, R. WFOT Global Strategy for the Occupational Therapy Workforce; WFOT: Geneva, Switzerland, 2024. [Google Scholar]
- Jesus, T.S.; Zweck, C.; Larson, S.; Bhattacharjya, S.; Kamalakannan, S.; Mani, K.; Ledgerd, R. Refining the first global strategy for the occupational therapy workforce: Results from a mixed-methods survey and multimodal expert feedback. Res. Sq. 2024. [Google Scholar] [CrossRef] [PubMed]
- Rodger, S.; Thomas, Y.; Holley, S.; Springfield, E.; Edwards, A.; Broadbridge, J.; Greber, C.; McBryde, C.; Banks, R.; Hawkins, R. Increasing the occupational therapy mental health workforce through innovative practice education: A pilot project. Aust. Occup. Ther. J. 2009, 56, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Morley, E.; Rohlman, D.; Cheyney, M.; Lansing, A. Impact of Training on Addressing Farmer Mental Health in Occupational Therapy Practice. OTJR 2024, 15394492241279781. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nissen, R.M.; Ikiugu, M.N.; Barash, B.; Kathol, M.; Oorlog, A. Perceptions of Occupational Therapy Educators about the Educational Preparation of Occupational Therapists for Designation as Qualified Mental Health Professionals. Occup. Ther. Health Care 2023, 37, 282–295. [Google Scholar] [CrossRef] [PubMed]
- Zango-Martín, I.; Nafai, S.; El Ouazzani, S.; Derkaoui, J.; Stevens-Nafai, E.; Codern-Bové, N. Understanding the role and importance of occupational therapy in mental health services in Morocco: Perspectives from mental health professionals. Work 2022, 72, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Scanlan, J.N.; Meredith, P.J.; Haracz, K.; Ennals, P.; Pépin, G.; Webster, J.S.; Arblaster, K.; Wright, S.; Network, T.A. Mental health education in occupational therapy professional preparation programs: Alignment between clinician priorities and coverage in university curricula. Aust. Occup. Ther. J. 2017, 64, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Mahboub, L.; Milbourn, B.T. Modernising occupational therapy teaching, research and practice in mental Health. Aust. Occup. Ther. J. 2015, 62, 363. [Google Scholar] [CrossRef] [PubMed]
- Kumurenzi, A.; Richardson, J.; Thabane, L.; Kagwiza, J.; Urimubenshi, G.; Hamilton, L.; Bosch, J.; Jesus, T. Effectiveness of interventions by non-professional community-level workers or family caregivers to improve outcomes for physical impairments or disabilities in low resource settings: Systematic review of task-sharing strategies. Hum. Resour. Health 2023, 21, 48. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kumurenzi, A.; Jesus, T.S.; Richardson, J.; Thabane, L.; Kagwiza, J.; Cockburn, L.; Langhorne, P.; DePaul, V.; Melifonwu, R.; Hamilton, L.; et al. A description of functional needs of community-dwelling stroke survivors in Rwanda: A prospective observational cohort study. Disabil. Rehabil. 2025, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Endale, T.; Qureshi, O.; Ryan, G.K.; Esponda, G.M.; Verhey, R.; Eaton, J.; De Silva, M.; Murphy, J. Barriers and drivers to capacity-building in global mental health projects. Int. J. Ment. Health Syst. 2020, 14, 89. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jack, H.E.; Merritt, C.; Medhin, G.; Musesengwa, R.; Mafuta, C.; Gibson, L.J.; Hanlon, C.; Sorsdahl, K.; Chibanda, D.; Abas, M. Developing sustainable capacity-building in mental health research: Implementation outcomes of training of trainers in systematic reviewing. Glob. Health Action 2020, 13, 1715325. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chibanda, D.; Abas, M.; Musesengwa, R.; Merritt, C.; Sorsdahl, K.; Mangezi, W.; Bandawe, C.; Cowan, F.; Araya, R.; Gomo, E.; et al. Mental health research capacity building in sub-Saharan Africa: The African Mental Health Research Initiative. Glob. Ment. Health 2020, 7, e8. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wilburn, V.G.; Hoss, A.; Pudeler, M.; Beukema, E.; Rothenbuhler, C.; Stoll, H.B. Receiving Recognition: A Case for Occupational Therapy Practitioners as Mental and Behavioral Health Providers. Am. J. Occup. Ther. 2021, 75, 7505090010. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Occupational Therapists. Occupational Therapy under Pressure: Workforce Survey Findings 2022–2023; Report; Royal College of Occupational Therapy: London, UK, 2023. [Google Scholar]
- Mertala, S.M.; Kanste, O.; Keskitalo-Leskinen, S.; Juntunen, J.; Kaakinen, P. Job Satisfaction among Occupational Therapy Practitioners: A Systematic Review of Quantitative Studies. Occup. Ther. Health Care 2022, 36, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Scanlan, J.N.; Meredith, P.; Poulsen, A.A. Enhancing retention of occupational therapists working in mental health: Relationships between wellbeing at work and turnover intention. Aust. Occup. Ther. J. 2013, 60, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Foster, F.; Palexas, S.; Hitch, D. Early career programs for mental health occupational therapists: A survey of current practice. Aust. Occup. Ther. J. 2022, 69, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Dillon, M.B.; Dillon, T.H.; King, R.M.; Chamberlin, J.L. Interfacing with Community Mental Health Services: Opportunities for Occupational Therapy and Level II Fieldwork Education. Occup. Ther. Health Care 2007, 21, 91–104. [Google Scholar] [CrossRef] [PubMed]
- World Federation of Occupational Therapists. Countries/Territories Requiring National-Level Registration/Licensing. 2025. Available online: https://hr-project.wfot.org/#data_registration_required_national (accessed on 16 May 2025).
- World Federation of Occupational Therapists. Total WFOT-Approved Education Programmes. 2025. Available online: https://hr-project.wfot.org/#data_ep_wfot_approved_total (accessed on 16 May 2025).
- Al Imam, M.H.; Jahan, I.; Das, M.C.; Muhit, M.; Akbar, D.; Badawi, N.; Khandaker, G. Situation analysis of rehabilitation services for persons with disabilities in Bangladesh: Identifying service gaps and scopes for improvement. Disabil. Rehabil. 2022, 44, 5571–5584. [Google Scholar] [CrossRef] [PubMed]
- Jesus, T.S.; Hoenig, H. Crossing the Global Quality Chasm in Health Care: Where Does Rehabilitation Stand? Arch. Phys. Med. Rehabil. 2019, 100, 2215–2217. [Google Scholar] [CrossRef] [PubMed]
- Jesus, T.S.; von Zweck, C.; Mani, K.; Kamalakannan, S.; Bhattacharjya, S.; Ledgerd, R. Mapping the occupational therapy workforce research worldwide: Study protocol for a scoping review. Work 2021, 70, 677–686. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Introductory Question | Factors to be Rated as Either Facilitators or Barriers | Likert Rating Scale |
|---|---|---|
| Please rate the degree to which the following issues impact occupational therapy education for people with mental health needs | Regulation: Legislation/regulation regarding the role of occupational therapy in mental health | (1) “High Negative Impact” (2) “Low Negative Impact” (3) “No impact” (4) “Low Positive Impact” (5) “High Positive Impact” OR - “Unknown” - “Not applicable” |
| Education standards: Education standards for occupational therapy (e.g., accreditation requirements) | ||
| Faculty expertise: Availability of faculty with required knowledge and experience in mental health | ||
| Supervised practice: Availability of fieldwork/supervised practice opportunities for occupational therapy students for working with people with mental health needs | ||
| Teaching resources: Availability of required teaching resources (funding, equipment, supplies) | ||
| Practice evidence: Availability of best practice evidence in occupational therapy mental health | ||
| Recognition: Recognition of the role of occupational therapy in working with people with mental health needs | ||
| Workforce demand: Workforce demand for occupational therapists to work with people with mental health needs | ||
| Student interest: Student interest in working with people with mental health needs |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jesus, T.S.; Monteiro, P.C.; Ledgerd, R.; von Zweck, C., on behalf of the World Federation of Occupational Therapists. Education of Occupational Therapists in Mental Health: A Global Survey of Educators Regarding Perceived Facilitators and Barriers. Int. J. Environ. Res. Public Health 2025, 22, 1009. https://doi.org/10.3390/ijerph22071009
Jesus TS, Monteiro PC, Ledgerd R, von Zweck C on behalf of the World Federation of Occupational Therapists. Education of Occupational Therapists in Mental Health: A Global Survey of Educators Regarding Perceived Facilitators and Barriers. International Journal of Environmental Research and Public Health. 2025; 22(7):1009. https://doi.org/10.3390/ijerph22071009
Chicago/Turabian StyleJesus, Tiago S., Pedro C. Monteiro, Ritchard Ledgerd, and Claudia von Zweck on behalf of the World Federation of Occupational Therapists. 2025. "Education of Occupational Therapists in Mental Health: A Global Survey of Educators Regarding Perceived Facilitators and Barriers" International Journal of Environmental Research and Public Health 22, no. 7: 1009. https://doi.org/10.3390/ijerph22071009
APA StyleJesus, T. S., Monteiro, P. C., Ledgerd, R., & von Zweck, C., on behalf of the World Federation of Occupational Therapists. (2025). Education of Occupational Therapists in Mental Health: A Global Survey of Educators Regarding Perceived Facilitators and Barriers. International Journal of Environmental Research and Public Health, 22(7), 1009. https://doi.org/10.3390/ijerph22071009