
Coproduction Within Intersectoral Collaboration in the Context of a Neighborhood with Low Socioeconomic Scores in The Netherlands


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.1.1. Background
2.1.2. The Connectors
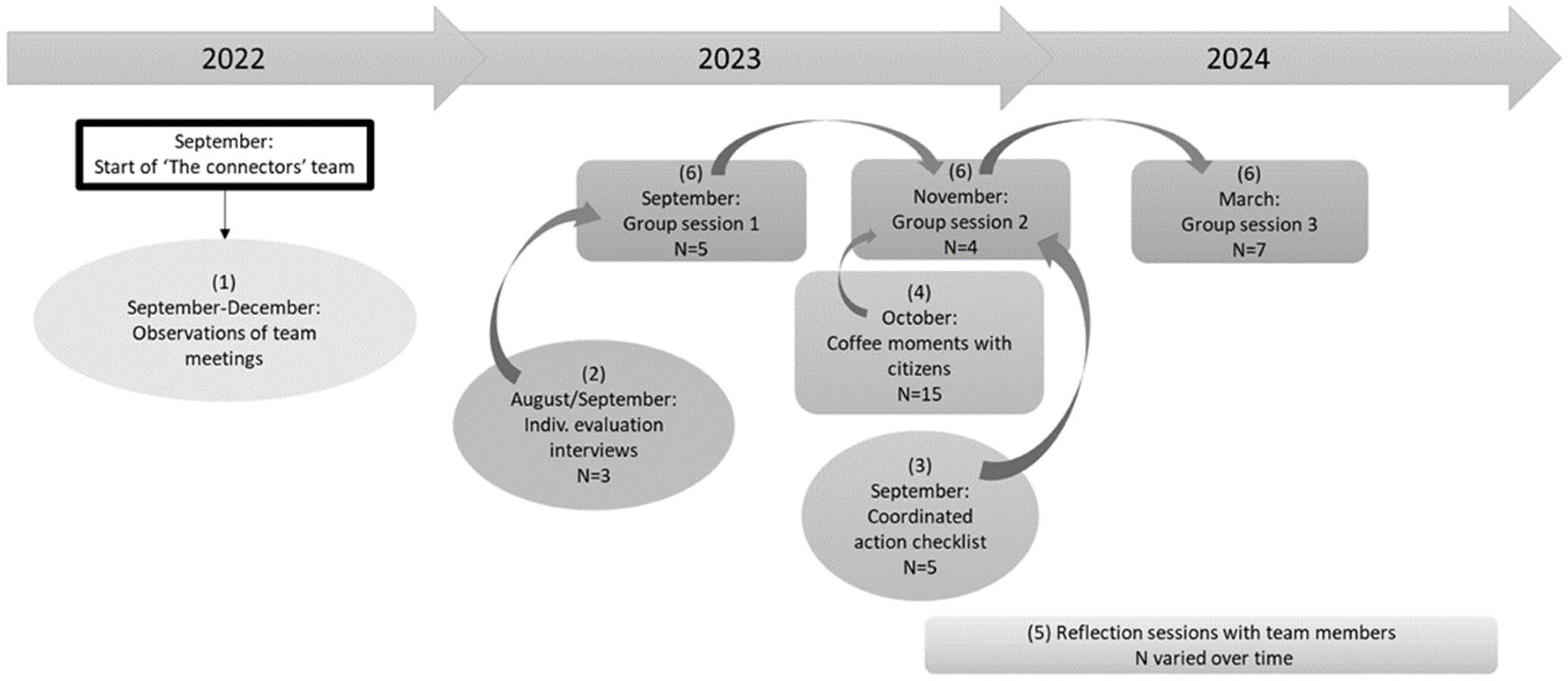
2.2. Study Design
Coordinated Action Checklist (CAC)
2.3. Analytical Strategy
3. Results
3.1. Coproduction Within Intersectoral Collaboration—The Active Contribution of Coproducers
“I now participate much more in all kinds of meetings and networks where it is necessary to introduce the informal voice and the importance of our society. Also to be able to speak about what an informal network needs.”
“They [coproducers] work 36 hours a week as an (informal) caregiver/service provider/community center coordinator in the neighborhood, and in the evenings in the supermarket they are also approached about all kinds of things. That is quite difficult, of course. That will also be the case for the team member of the Connectors, who lives in the neighborhood and has no formal caregiver experience. There is no button to turn off. You are busy for 120 hours a week, or even longer.”
“Support is needed from a citizens’ network that takes on a formal role in the neighborhood. They are all people with certain baggage or a difficult past, who want to participate but need support. They are doing quite well professionally, but when things get difficult, personal problems become visible.”
3.2. Coproduction Within Intersectoral Collaboration—The Relationship Between Professionals and Citizens
3.2.1. Reciprocal Relationship Between Coproducers and Professionals
3.2.2. Obstacles for Professionals to Collaborate
“And in the formal network there you really notice the trauma of having a new organization and they are going to try something new. ‘We have already had ten of you “connectors”, you know… So just tell us exactly what you’re going to do.’ And even if you explain it in the best way, it is still not trusted. ‘Let’s wait and see’ is the attitude of most professionals…”
“Unfortunately, some organizations still reason and act based on the rules first, which means that assistance for citizens has lower priority.”
“It is important that these individuals also transfer this to the rest of the organization so that the ‘oil slick’ can grow. If that does not happen and the individuals leave the organization, a piece of the network disappears and cooperation must be built anew.”
3.2.3. The Team Members as ‘Boundary Spanners’
“So if there were individual problems, the psychotherapist of the team often tackled them. If something was group-oriented and system-oriented, the coproducer team member and I would focus on it. Because that is our background and that is what we are good at. Not that you completely let go of the individual situations, that is not possible, of course.”
3.3. The Context of Neighborhoods with Low Socioeconomic Scores
“So, an emergency fund is also being looked at, but even for that we are now thinking on a large scale. Shouldn’t you have some kind of fund for the neighborhood from which you occasionally take 25 euros to help someone out of problems, without having to be subject to the Financial Supervision Act?”
“You have to understand the DNA of the neighborhood to know what you are talking about.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SES | Socioeconomic Scores |
| HHTH | Healthy and Happy The Hague |
| CAC | Coordinated Action Checklist |
Appendix A. Coordinated Action Checklist

{kind=link}
| Item (Dimension) | Score | |
|---|---|---|
| General | 95 | |
| 1. | The collaboration is an asset to health promotion (including welfare) | 95 |
| Suitability of the partners | 81 | |
| 2. | To realize the goals of the collaboration, the right people are involved | 50 |
| 3. | Equity of the partners is essential for good collaboration | 95 |
| 4. | The contribution of the different members is to everyone’s full satisfaction | 30 |
| 5. | I have a special interest in participating in this collaboration because of my position or organization | 100 |
| 6. | I can contribute to the collaboration in a satisfactory way (time, resources, etc.) | 90 |
| 7. | I feel strongly involved in this partnership | 100 |
| 8. | I can contribute constructively to the collaboration because of my expertise | 100 |
| Task dimension | 56 | |
| 9. | There is agreement on the mission, the goal and the planning within the partnership | 55 |
| 10. | The partnership achieves regular (small) successes | 90 |
| 11. | The partnership functions well (working structure, working methods) | 50 |
| 12. | The partnership evaluates progress at regular intervals and makes adjustments if necessary | 55 |
| 13. | The conditions for the existence of the collaboration are satisfactory | 30 |
| Relation dimension | 57 | |
| 14. | The partnership partners communicate in an open manner | 65 |
| 15. | The partnership partners work together in a constructive manner and know how to involve each other when action is needed | 50 |
| 16. | The partnership partners are willing to compromise | 70 |
| 17. | In the partnership, conflicts are dealt with in a constructive way | 50 |
| 18. | The partnership partners will carry out decisions and actions loyally | 50 |
| Growth dimension | 81 | |
| 19. | I create goodwill and involvement for the partnership within my organization | 90 |
| 20. | Giving feedback to the local officials on behalf of the partnership is satisfactory | 80 |
| 21. | The partnership is willing to recruit new partners in the course of time | 85 |
| 22. | The partnership succeeds in mobilizing others for actions | 70 |
| Visibility dimension | 59 | |
| 23. | The partnership maintains the external relationships in an accurate way | 45 |
| 24. | The partnership is seen as reliable and legitimate by external relations | 50 |
| 25. | The image of my partnership in the outside world is good | 70 |
| 26. | The partnership takes care of continuation after the project period | 70 |
| Mean score of all items | 69 | |
References
- World Health Organization. Health in All Policies: Helsinki Statement—Framework for Country Action; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Such, E.; Smith, K.; Woods, H.B.; Meier, P. Governance of intersectoral collaborations for population health and to reduce health inequalities in high-income countries: A complexity-informed systematic review. Int. J. Health Policy Manag. 2022, 11, 2780. [Google Scholar] [CrossRef] [PubMed]
- Verschuere, B.; Brandsen, T.; Pestoff, V. Co-production: The state of the art in research and the future agenda. Volunt. Int. J. Volunt. Nonprofit Organ. 2012, 23, 1083–1101. [Google Scholar] [CrossRef]
- Brandsen, T.; Honingh, M. Definitions of co-production and co-creation. In Co-Production and Co-Creation; Brandsen, T., Honingh, M., Eds.; Routledge: Cambridge, UK, 2018; pp. 9–17. [Google Scholar]
- Jørgensen, K.; Hansen, M.; Andersen, T.G.; Hansen, M.; Karlsson, B. Healthcare professionals’ experiences with patient participation in a mental healthcare centre: A qualitative study. Int. J. Environ. Res. Public Health 2023, 20, 1965. [Google Scholar] [CrossRef]
- Petiwala, A.; Lanford, D.; Landers, G.; Minyard, K. Community voice in cross-sector alignment: Concepts and strategies from a scoping review of the health collaboration literature. BMC Public Health 2021, 21, 712. [Google Scholar] [CrossRef]
- Milton, B.; Attree, P.; French, B.; Povall, S.; Whitehead, M.; Popay, J. The impact of community engagement on health and social outcomes: A systematic review. Community Dev. J. 2012, 47, 316–334. [Google Scholar] [CrossRef]
- Turnhout, E.; Metze, T.; Wyborn, C.; Klenk, N.; Louder, E. The politics of coproduction: Participation, power, and transformation. Curr. Opin. Environ. Sustain. 2020, 42, 15–21. [Google Scholar] [CrossRef]
- De Weger, E.; Drewes, H.W.; Van Vooren, N.J.; Luijkx, K.G.; Baan, C.A. Engaging citizens in local health policymaking. A realist explorative case-study. PLoS ONE 2022, 17, e0265404. [Google Scholar] [CrossRef] [PubMed]
- McMullin, C.; Needham, C. Coproduction in healthcare. In Co-Production and Co-Creation; Brandsen, T., Honingh, M., Eds.; Routledge: Cambridge, UK, 2018; pp. 151–160. [Google Scholar]
- Caron, R.M. Expansion of coproduction in health care as a population health management approach. Popul. Health Manag. 2019, 22, 286–288. [Google Scholar] [CrossRef]
- Van Eijk, C.; Van der Vlegel-Brouwer, W.; Bussemaker, J. Healthy and happy citizens: The opportunities and challenges of co-producing citizens’ health and well-being in vulnerable neighborhoods. Adm. Sci. 2023, 13, 46. [Google Scholar] [CrossRef]
- Buckwalter, N.D. The potential for public empowerment through government-organized participation. Public Adm. Rev. 2014, 74, 573–584. [Google Scholar] [CrossRef]
- De Graaf, L.; Van Hulst, M.; Michels, A. Enhancing participation in disadvantaged urban neighbourhoods. Local Gov. Stud. 2015, 41, 44–62. [Google Scholar] [CrossRef]
- De Weger, E.; Van Vooren, N.; Luijkx, K.G.; Baan, C.A.; Drewes, H.W. Achieving successful community engagement: A rapid realist review. BMC Health Serv. Res. 2018, 18, 285. [Google Scholar] [CrossRef] [PubMed]
- Vanleene, D.; Voets, J.; Verschuere, B. The co-production of public value in community development: Can street-level professionals make a difference? Int. Rev. Adm. Sci. 2020, 86, 582–598. [Google Scholar] [CrossRef]
- Long, J.C.; Cunningham, F.C.; Braithwaite, J. Bridges, brokers and boundary spanners in collaborative networks: A systematic review. BMC Health Serv. Res. 2013, 13, 158. [Google Scholar] [CrossRef]
- Williams, P. The competent boundary spanner. Public Adm. 2002, 80, 103–124. [Google Scholar] [CrossRef]
- Bromley, E.; Figueroa, C.; Castillo, E.G.; Kadkhoda, F.; Chung, B.; Miranda, J.; Menon, K.; Whittington, Y.; Jones, F.; Wells, K.B.; et al. Community partnering for behavioral health equity: Public agency and community leaders’ views of its promise and challenge. Ethn. Dis. 2018, 28 (Suppl. 2), 397. [Google Scholar] [CrossRef]
- Schot, E.; Tummers, L.; Noordegraaf, M. Working on working together. A systematic review on how healthcare professionals contribute to interprofessional collaboration. J. Interprof. Care 2020, 34, 332–342. [Google Scholar] [CrossRef]
- Palumbo, R. Contextualizing co-production of health care: A systematic literature review. Int. J. Public Sect. Manag. 2016, 29, 72–90. [Google Scholar] [CrossRef]
- Algren, M.H.; Bak, C.K.; Berg-Beckhoff, G.; Andersen, P.T. Health-risk behaviour in deprived neighbourhoods compared with non-deprived neighbourhoods: A systematic literature review of quantitative observational studies. PLoS ONE 2015, 10, e0139297. [Google Scholar] [CrossRef]
- Stafford, M.; Marmot, M. Neighbourhood deprivation and health: Does it affect us all equally? Int. J. Epidemiol. 2003, 32, 357–366. [Google Scholar] [CrossRef]
- Dougall, I.; Vasiljevic, M.; Wright, J.D.; Weick, M. How, when, and why is social class linked to mental health and wellbeing? A systematic meta-review. Soc. Sci. Med. 2024, 343, 116542. [Google Scholar] [CrossRef] [PubMed]
- Goodlad, R.; Burton, P.; Croft, J. Effectiveness at what? The processes and impact of community involvement in area-based initiatives. Environ. Plan. C Gov. Policy 2005, 23, 923–938. [Google Scholar] [CrossRef]
- Vanleene, D.; Voets, J.; Verschuere, B. The co-production of a community: Engaging citizens in derelict neighbourhoods. Volunt. Int. J. Volunt. Nonprofit Organ. 2018, 29, 201–221. [Google Scholar] [CrossRef]
- Municipality of The Hague GDH. Staat van de Stad Den Haag. 2022. Available online: https://denhaag.raadsinformatie.nl/document/11408152/1/RIS311788_Bijlage_Staat_van_de_Stad_20222022 (accessed on 24 September 2024).
- Municipality of The Hague. Den Haag in Cijfers—Dutch Native/Minorities 2024—Districts of Municipality the Hague. 2024. Available online: https://denhaag.incijfers.nl (accessed on 1 April 2025).
- Gezond en Gelukkig Den Haag. Hoe Wij Werken. 2020. Available online: https://gezondengelukkigdenhaag.nl/ (accessed on 1 April 2025).
- Fenger, M.; Simonse, R. The implosion of the Dutch surveillance welfare state. Soc. Policy Adm. 2024, 58, 264–276. [Google Scholar] [CrossRef]
- Saunders, P.; Campbell, P.; Webster, M.; Thawe, M. Analysis of small area environmental, socioeconomic and health data in collaboration with local communities to target and evaluate ‘Triple win’ interventions in a deprived community in Birmingham UK. Int. J. Environ. Res. Public Health 2019, 16, 4331. [Google Scholar] [CrossRef]
- Avison, D.E.; Lau, F.; Myers, M.D.; Nielsen, P.A. Action research. Commun. ACM 1999, 42, 94–97. [Google Scholar] [CrossRef]
- De Jong, M.; Tijhuis, Y.; Koelen, M.; Wagemakers, A. Intersectoral collaboration in a Dutch community health promotion programme: Building a coalition and networks. Health Promot. Int. 2023, 38, daab207. [Google Scholar] [CrossRef]
- Jones, J.; Smith, J. Ethnography: Challenges and opportunities. Evid. Based Nurs. 2017, 20, 98–100. [Google Scholar] [CrossRef]
- Akyıldız, S.T.; Ahmed, K.H. An overview of qualitative research and focus group discussion. Int. J. Acad. Res. Educ. 2021, 7, 1–15. [Google Scholar] [CrossRef]
- Wagemakers, A.; Koelen, M.A.; Lezwijn, J.; Vaandrager, L. Coordinated action checklist: A tool for partnerships to facilitate and evaluate community health promotion. Glob. Health Promot. 2010, 17, 17–28. [Google Scholar] [CrossRef]
- Verbeke, L.; Snyers, K.; Kwanten, L.; Hasevoets, G. Netwerken en Lokaal Welzijnsbeleid: Model, Meetinstrument en Praktijk; Ministerie van de Vlaamse Gemeenschap: Brussels, Belgium, 2004. [Google Scholar]
- Pearse, N. An illustration of a deductive pattern matching procedure in qualitative leadership research. Electron. J. Bus. Res. Methods 2019, 17, 143–154. [Google Scholar] [CrossRef]
- Ansell, C.; Gash, A. Collaborative governance in theory and practice. J. Public Adm. Res. Theory 2008, 18, 543–571. [Google Scholar] [CrossRef]
- Alderwick, H.; Hutchings, A.; Briggs, A.; Mays, N. The impacts of collaboration between local health care and non-health care organizations and factors shaping how they work: A systematic review of reviews. BMC Public Health 2021, 21, 753. [Google Scholar] [CrossRef]
- Harting, J.; Kunst, A.E.; Kwan, A.; Stronks, K. A ‘health broker’ role as a catalyst of change to promote health: An experiment in deprived Dutch neighbourhoods. Health Promot. Int. 2011, 26, 65–81. [Google Scholar] [CrossRef]
- Stephens, W.; van Steden, R.; Schoonmade, L. Boundary spanning in local governance: A scoping review. Adm. Soc. 2024, 56, 99–144. [Google Scholar] [CrossRef]
- Thijssen, P.; Van Dooren, W. Who you are/where you live: Do neighbourhood characteristics explain co-production? Int. Rev. Adm. Sci. 2016, 82, 88–109. [Google Scholar] [CrossRef]
- Pollitt, R.A.; Kaufman, J.S.; Rose, K.M.; Diez-Roux, A.V.; Zeng, D.; Heiss, G. Cumulative life course and adult socioeconomic status and markers of inflammation in adulthood. J. Epidemiol. Community Health 2008, 62, 484–491. [Google Scholar] [CrossRef]
- Jakobsen, M.; Andersen, S.C. Coproduction and equity in public service delivery. Public Adm. Rev. 2013, 73, 704–713. [Google Scholar] [CrossRef]
| Composition of the Connectors Team Starting in 2022: | Composition of the Connectors Team from 2024 and Onwards: |
|---|---|
| Psychotherapist | Psychotherapist |
| Social worker | Mental health nurse |
| Active citizen as coproducer | Outpatient supervisor (social work background) |
| Community worker | |
| Project employee |
| Variety of Citizens in the Neighborhood Where the Connectors Collaborate with the Following: | Main Services in the Network of the Connectors: |
|---|---|
| Citizen coproducers, among others: | Mental health care |
| - Community center coordinators and volunteers. | Primary health care |
| - Food bank volunteers. | Welfare |
| - Grouped citizens organizing activities. | Social care |
| (potential) Service users. | Police |
| Citizens. | Housing corporation |
| Topics Derived from the CAC (Top Down): | New Topics that Emerged from the Data (Bottom Up): |
|---|---|
| Suitability of partners | Learning network |
| Task dimension | Professional–coproducer collaboration |
| Relation dimension | Experiences in practice |
| Growth dimension | |
| Visibility dimension |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Lammeren, R.; Schalk, J.; van der Pas, S.; Bussemaker, J. Coproduction Within Intersectoral Collaboration in the Context of a Neighborhood with Low Socioeconomic Scores in The Netherlands. Int. J. Environ. Res. Public Health 2025, 22, 954. https://doi.org/10.3390/ijerph22060954
van Lammeren R, Schalk J, van der Pas S, Bussemaker J. Coproduction Within Intersectoral Collaboration in the Context of a Neighborhood with Low Socioeconomic Scores in The Netherlands. International Journal of Environmental Research and Public Health. 2025; 22(6):954. https://doi.org/10.3390/ijerph22060954
Chicago/Turabian Stylevan Lammeren, Roos, Jelmer Schalk, Suzan van der Pas, and Jet Bussemaker. 2025. "Coproduction Within Intersectoral Collaboration in the Context of a Neighborhood with Low Socioeconomic Scores in The Netherlands" International Journal of Environmental Research and Public Health 22, no. 6: 954. https://doi.org/10.3390/ijerph22060954
APA Stylevan Lammeren, R., Schalk, J., van der Pas, S., & Bussemaker, J. (2025). Coproduction Within Intersectoral Collaboration in the Context of a Neighborhood with Low Socioeconomic Scores in The Netherlands. International Journal of Environmental Research and Public Health, 22(6), 954. https://doi.org/10.3390/ijerph22060954