

Parental Knowledge, Attitudes, and Practices and Their Association with Dental Caries in Children Aged 5–9 Years: A Cross-Sectional Study in Rural Ecuador

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Study Variables
- No obvious decay (codes 0 to 3): Includes healthy teeth or teeth with initial lesions without cavitation.
- Obvious decay (codes 4 to 6): Corresponds to cavitated lesions involving dentin, with direct clinical involvement.
- Knowledge:
- b.
- Attitude:
- c.
- Practices:
2.3. Inclusion and Exclusion Criteria
- Children aged 5–9 years enrolled in school.
- Informed consent signed by caregivers.
- ▪
- Children with severe systemic diseases (e.g., congenital heart disease, immune disorders, uncontrolled diabetes, or ongoing cancer treatment).
- ▪
- Children undergoing specialized or ongoing dental treatment (orthodontics, endodontics, or post-surgical care).
- ▪
- Absence of informed consent.
2.4. Population and Sample
2.5. Calibration of Examiners and Data Collection Protocol
2.6. Data Collection Procedures
2.7. Data Management and Analysis
3. Results
3.1. Sample Distribution by Age and Sex
3.2. Classification of Dental Caries Severity According to ICDAS Grouping
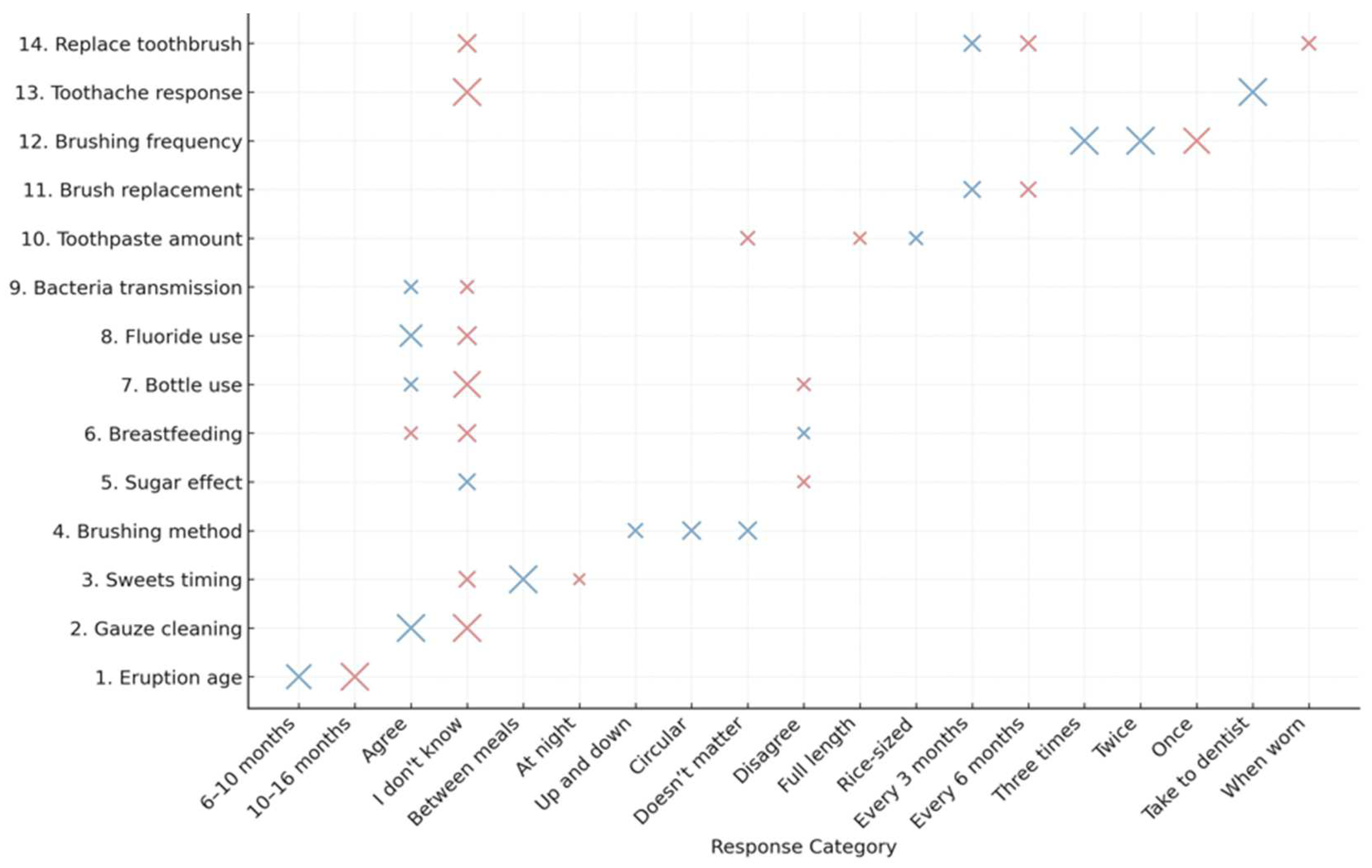
3.3. KAP Survey Instrument (Knowledge, Attitudes, and Practices)
3.4. Bubble Plot of Logistic Regression Coefficients for Caregivers’ Knowledge Items Associated with Obvious Decay in Children (ICDAS 4–6)
3.5. Association Between Caregivers’ Attitude Toward Oral Health and the Presence of Obvious Decay
3.6. Frequency and Association of Children’s Oral Health Practices (N = 229)
3.7. Forest Plot—Multivariate Model (KAPs → Advance)
4. Discussion
4.1. Comparison of Results
4.2. Instruments and Methodology
4.3. Limitations and Biases
4.4. Study Contributions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ICDAS | International Caries Detection and Assessment System. |
| KAPS | Knowledge, Attitudes, and Practices. |
References
- Pozos-Guillén, A.; Molina, G.; Soviero, V.; Arthur, R.A.; Chavarria-Bolaños, D.; Acevedo, A.M. Management of dental caries lesions in Latin American and Caribbean countries. Braz. Oral Res. 2021, 35 (Suppl. S1). [Google Scholar] [CrossRef]
- Cogulu, D.; Saglam, C. Genetic aspects of dental caries. Front. Dent. Med. 2022, 3, 1060177. [Google Scholar] [CrossRef]
- Campus, G.; Niu, J.Y.; Sezer, B.; Yu, O.Y. Prevention and Management of Dental Erosion and Decay. BMC Oral Health 2024, 24, 468. Available online: https://bmcoralhealth.biomedcentral.com/articles/10.1186/s12903-024-04257-y (accessed on 13 May 2025). [CrossRef]
- Monteiro, E.L.O.; Ladeira, L.L.C.; Costa, C.M.; Monteiro, M.C.C.; Rebelo, M.A.B.; Alves, C.M.C.; Costa, C.M.; Monteiro, M.C.C.; Monteiro, E.L.O. Behavior Risk Factors for Noncommunicable Diseases and Caries in Adolescents: A Population Study. Caries Res. 2025. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. (Ed.) Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health By 2030; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240061484 (accessed on 25 May 2025).
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental Caries. Nat. Rev. Dis. Primers 2017, 3, 17030. Available online: https://pubmed.ncbi.nlm.nih.gov/28540937/ (accessed on 13 May 2025).
- Veneri, F.; Vinceti, S.R.; Filippini, T. Fluoride and Caries Prevention: A Scoping Review of Public Health Policies. Ann. Igiene 2024, 36, 270–280. Available online: https://pubmed.ncbi.nlm.nih.gov/38236001/ (accessed on 13 May 2025).
- Salinas Goodier, C. Factors affecting oral health in children and adolescents in Ecuador. Salud Cienc. Tecnol. Ser. Conf. 2024, 3, 889. [Google Scholar] [CrossRef]
- BaniHani, A.; Deery, C.; Toumba, J.; Munyombwe, T.; Duggal, M. The impact of dental caries and its treatment by conventional or biological approaches on the oral health-related quality of life of children and carers. Int. J. Paediatr. Dent. 2018, 28, 266–276. [Google Scholar] [CrossRef]
- Hugar, S.M.; Gokhale, N.; Soneta, S.P.; Joshi, R.S.; Dialani, P.K.; Saxena, N. Evaluation of the Treatment Protocols in the Management of Pulpally Involved Young Permanent Teeth in Children: A Systematic Review and Meta-analysis. Int. J. Clin. Pediatr. Dent. 2022, 15, S103–S113. [Google Scholar] [CrossRef]
- Casanova-Rosado, J.F.; Vallejos-Sánchez, A.A.; Minaya-Sánchez, M.; Lara-Carrillo, E.; Robles-Bermeo, N.L.; De la Rosa-Santillana, R.; Medina-Solís, C.E. Toothbrushing Frequency and Maternal Schooling Associated with Caries in Primary Dentition in 6- and 7-year-old Children. West Indian Med. J. 2022, 69, 545–549. [Google Scholar]
- Kubota, Y.; San Pech, N.; Durward, C.; Ogawa, H. Early childhood caries status and its associated factors among young children in a rural area of Cambodia. Pediatr. Dent. J. 2020, 30, 17–23. [Google Scholar] [CrossRef]
- Bramhecha, A.; Datta, J.; Balasubramaniam, A. What preventive strategies do dentists prescribe for dental caries prevention?—A KAP survey. Dent. Res. J. 2023, 20, 51. [Google Scholar] [CrossRef]
- Starczewska, M.; Emerich, K. Wiedza stomatologiczna kobiet ciężarnych oraz młodych matek. Pediatr. Pol. 2009, 84, 397–401. [Google Scholar] [CrossRef]
- Brown, U.T.; Spivakovsky, S.; Janal, M. An Epistemic Look at Parental Conceptual Knowledge and Oral Health Outcomes in Children. Glob. Pediatr. Health 2024, 11. [Google Scholar] [CrossRef]
- Pitts, N.B.; Twetman, S.; Fisher, J.; Marsh, P.D. Understanding Dental Caries as a Non-Communicable Disease. Br. Dent. J. 2021, 231, 749–753. Available online: https://www.nature.com/articles/s41415-021-3775-4 (accessed on 13 May 2025). [CrossRef]
- Gresh, A.; Wilson, D.; Fenick, A.; Patil, C.L.; Coker, T.; Rising, S.S.; Glass, N.; Platt, R. A Conceptual Framework for Group Well-Child Care: A Tool to Guide Implementation, Evaluation, and Research. Matern. Child Health J. 2023, 27, 991–1008. [Google Scholar] [CrossRef]
- Donnell, C.C.; Johnston, M.J.; Foley, J.I. The Six-Year-Old ‘Adult’. Prim. Dent. J. 2021, 10, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Singh, H. Plaque Control with Newer Dimension in Children. Indian J. Forensic Med. Toxicol. 2020, 14, 9075–9078. [Google Scholar] [CrossRef]
- Vélez-León, E.; Albaladejo, A.; Cuenca-León, K.; Jiménez-Romero, M.; Armas-Vega, A.; Melo, M. Prevalence of Caries According to the ICDAS II in Children from 6 and 12 Years of Age from Southern Ecuadorian Regions. Int. J. Environ. Res. Public Health 2022, 19, 7266. [Google Scholar] [CrossRef]
- Nepaul, P.; Mahomed, O. Influence of parents’ oral health knowledge and attitudes on oral health practices of children (5–12 years) in a rural school in KwaZulu-Natal, South Africa. J. Int. Soc. Prev. Commun. Dent. 2020, 10, 605. [Google Scholar]
- Ortega, F. Prevalencia de caries dental y factores sociodemográficos asociados a su aparición en la población escolar de Mangahuantag, Puembo. OdontoInvestigación 2020, 6, 12–33. [Google Scholar] [CrossRef]
- Vélez León, E.M.; Albaladejo Martínez, A.; Preciado Sarmiento, M.A.; Cordero López, M.A.; Armas Adel, C.; Encalada Verdugo, L.S.; Melo, M. Caries Experience in Preschoolers in Three Ecuadorian Communities. Children 2023, 10, 1123. [Google Scholar] [CrossRef] [PubMed]
- Ladera Castañeda, M.I.; Medina Sotelo, C.G. Oral health in Latin America: A view from public policies. Salud Cienc. Tecnología 2023, 3, 340. [Google Scholar] [CrossRef]
- Du, S.; Cheng, M.; Cui, Z.; Wang, X.; Feng, X.; Tai, B.; Hu, D.; Lin, H.; Wang, B.; Wang, C.; et al. Decomposing Socioeconomic Inequality in Early Childhood Caries Among 3 to 5-Year-Old Children in China. Int. Dent. J. 2024, 74, 968–977. [Google Scholar] [CrossRef]
- Abanto, J.; Cárdenas, S.D.; Duran, A.V.; Garza, M.; Brigato, V.R.; Guinot, F. Association between socioeconomic factors, attitudes and beliefs regarding the primary dentition and caries in children aged 1–5 years of Brazilian and Colombian parents. Eur. J. Paediatr. Dent. 2024, 25, 258–265. [Google Scholar]
- Chinnakotla, B.; Susarla, S.M.; Mohan, D.C.; Turton, B.; Husby, H.M.; Morales, C.P.; Sokal-Gutierrez, K. Associations between Maternal Education and Child Nutrition and Oral Health in an Indigenous Population in Ecuador. Int. J. Environ. Res. Public Health 2023, 20, 473. [Google Scholar] [CrossRef]
- Chen, L.; Hong, J.; Xiong, D.; Zhang, L.; Li, Y.; Huang, S.; Hua, F. Are parents’ education levels associated with either their oral health knowledge or their children’s oral health behaviors? A survey of 8446 families in Wuhan. BMC Oral Health 2020, 20, 203. [Google Scholar] [CrossRef] [PubMed]
- Sabbarwal, B.; Puranik, M.P.; Uma, S.R. Association between parental behavior and child’s oral health among 3–5-year-old children in Bengaluru city. Int. J. Clin. Pediatr. Dent. 2020, 13, 677–681. [Google Scholar]
- Stormon, N.; Ford, P.J.; Lalloo, R. Family-Level Predictors of Australian Children’s Dental Caries and Injuries. Pediatr. Dent. 2020, 42, 28–39. [Google Scholar]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Di Blasio, M.; Ronsivalle, V.; Cicciù, M. Children oral health and parents education status: A cross sectional study. BMC Oral Health 2023, 23, 787. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, K.Y.; Lo, E.C.M.; Wong, M.C.M. Structural equation model for parental influence on children’s oral health practice and status. BMC Oral Health 2020, 20, 56. [Google Scholar] [CrossRef]
- Soares, G.H.; Haag, D.; Bastos, J.L.; Mejia, G.; Jamieson, L. Triple Jeopardy in Oral Health: Additive Effects of Immigrant Status, Education, and Neighborhood. JDR Clin. Transl. Res. 2024, 10, 54–63. [Google Scholar] [CrossRef]
- ICCMS. ICDAS. Available online: https://www.iccms-web.com/content/icdas (accessed on 26 March 2025).
- Armas-Vega, A.; Parise-Vasco, J.M.; Díaz-Segovia, M.C.; Arroyo-Bonilla, D.A.; Cabrera-Dávila, M.J.; Zambrano-Bonilla, M.C.; Ponce-Faula, C.; Viteri-García, A. Prevalence of Dental Caries in Schoolchildren from the Galapagos Islands: ESSO-Gal Cohort Report. Int. J. Dent. 2023, 2023, 6544949. [Google Scholar] [CrossRef]
- Raveendran, N.D.A.P.; Seong, N.C.; Hua, N.S.; Cugati, N.; Ganapathy, S. Parental Knowledge, Practice and Awareness on feeding and Oral hygiene measures for their children: An impact on ICDAS Scores. Res. J. Pharm. Technol. 2024, 17, 4861–4866. [Google Scholar] [CrossRef]
- Bamashmous, N.O.; El Ashiry, E.A.; Alamoudi, N.M.; Qahtan, D.K.; Alamoudi, R.A.; Felemban, O.M. Oral health related knowledge, attitude and behavior among group of mothers in relation to their primary school children’s oral health: A cross-sectional study. J. Clin. Pediatr. Dent. 2024, 48, 152–162. [Google Scholar] [PubMed]
- Mohammed Al-Dahan, H.; Ali Ismael, S. Early Childhood Caries: Parents’ Knowledge, Attitude and Practice Towards Its Prevention in Refugee Camps in Erbil, Iraq. BMC Oral Health 2023, 23, 792. Available online: https://bmcoralhealth.biomedcentral.com/articles/10.1186/s12903-023-03516-8 (accessed on 26 March 2025). [CrossRef] [PubMed]
- Basir, L.; Khanehmasjedi, M.; Khanehmasjedi, S. Knowledge, attitudes, and practices regarding the oral health of children. Braz. J. Oral Sci. 2022, 21, e228274. [Google Scholar] [CrossRef]
- Alsharif, M.K.S.; Mohd Nazan, A.I.N.; Ismail, S. Association of parental knowledge, attitude, and practice of oral health with early childhood caries among preschool children: A systematic review. Malays. J. Med. Health Sci. 2020, 16, 300–307. [Google Scholar]
- Rai, N.K.; Tiwari, T. Parental factors influencing the development of early childhood caries in developing nations: A systematic review. Front. Public Health 2018, 6, 300–307. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Age (Years) | Male N (%) | Female N (%) | Total N (%) |
|---|---|---|---|
| 5 | 3 (1.3%) | 3 (1.3%) | 6 (2.6%) |
| 6 | 14 (6.1%) | 9 (3.9%) | 23 (10.0%) |
| 7 | 38 (16.6%) | 43 (18.8%) | 81 (35.4%) |
| 8 | 37 (16.2%) | 26 (11.4%) | 63 (27.5%) |
| 9 | 28 (12.2%) | 28 (12.2%) | 56 (24.5%) |
| Total | 120 (52.4%) | 109 (47.6%) | 229 (100%) |
| ICDAS Code Range | Decay Classification | N | % |
|---|---|---|---|
| 0–3 | No obvious decay | 61 | 26.6 |
| 4–6 | Obvious decay | 168 | 73.4 |
| Total | 229 | 100 |
| KAP Category | Variable | Response Category | % |
|---|---|---|---|
| Attitude | Attitude toward dental health | Important | 21.0 |
| Less important | 0.4 | ||
| Very important | 73.8 | ||
| Neutral | 4.8 | ||
| Practice | Child’s feeling when brushing teeth | Happy | 90.8 |
| Neutral | 0.4 | ||
| Resistant | 7.9 | ||
| Sad | 0.9 | ||
| Child brushes the tongue | No | 13.5 | |
| I don’t know | 19.2 | ||
| Yes | 67.2 | ||
| Knowledge | Foods that cause cavities | Chocolate | 52.0 |
| Fruits | 4.8 | ||
| Cookies | 29.3 | ||
| Cakes | 14.0 | ||
| Prolonged breastfeeding causes cavities | Agree | 26.6 | |
| Disagree | 21.4 | ||
| I don’t know | 52.0 | ||
| Amount of toothpaste used | Full length of brush | 65.5 | |
| It doesn’t matter | 3.5 | ||
| Pea size | 31.0 | ||
| Excess sugar causes cavities | Agree | 85.6 | |
| Disagree | 2.2 | ||
| I don’t know | 12.2 | ||
| Sleeping with bottle causes cavities | Agree | 45.0 | |
| Disagree | 5.7 | ||
| I don’t know | 49.3 | ||
| Age of first tooth eruption | 10–16 months | 18.8 | |
| 6–10 months | 71.6 | ||
| I don’t know | 9.6 | ||
| Cleaning baby teeth with gauze | Agree | 68.1 | |
| Disagree | 6.6 | ||
| I don’t know | 25.3 | ||
| Best time to give sweets/cold drinks | After meals | 53.3 | |
| Between meals | 12.7 | ||
| None | 0.4 | ||
| I don’t know | 33.2 | ||
| Evening | 0.4 | ||
| Brushing method | Forward/backward | 16.6 | |
| Up/down | 39.7 | ||
| Circulars | 37.6 | ||
| It doesn’t matter | 6.1 | ||
| Transmission of bacteria from mother to child | Agree | 58.1 | |
| Disagree | 9.6 | ||
| I don’t know | 32.3 | ||
| Use of fluoride toothpaste | Agree | 54.1 | |
| Disagree | 5.2 | ||
| I don’t know | 40.6 | ||
| Toothbrush replacement frequency | Every 3 months | 77.3 | |
| Every 6 months | 16.6 | ||
| When they open | 3.9 | ||
| I don’t know | 2.2 | ||
| Brushing frequency | After every meal | 17.9 | |
| Twice | 16.2 | ||
| Thrice | 63.3 | ||
| Once | 2.6 | ||
| What to do if child has toothache | Analgesic | 10.0 | |
| Salt water | 9.6 | ||
| Take to the dentist | 76.4 | ||
| I don’t know | 1.7 | ||
| Eat elsewhere | 2.2 |
| Attitude Toward Oral Health | Frequency | Percentage (%) | OR | p-Value |
|---|---|---|---|---|
| Very Important | 169 | 73.8 | 1.32 | 0.363 |
| Important | 48 | 21.0 | ||
| Neutral | 11 | 4.8 | ||
| Less Important | 1 | 0.4 |
| Variable | Response | Frequency | Percentage (%) | OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Child’s feeling when brushing teeth | Happy | 209 | 91.3% | 0.30 (0.07–1.35) | 0.117 |
| Neutral | 0 | 0.0% | |||
| Resistant | 18 | 7.9% | |||
| Sad | 2 | 0.9% | |||
| Child brushes the tongue | Yes | 154 | 67.2% | 0.81 (0.42–1.54) | 0.519 |
| I don’t know | 44 | 19.2% | |||
| No | 31 | 13.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saquicela-Pulla, M.; Dávila-Arcentales, M.; Vélez-León, E.; Armas-Vega, A.; Melo, M. Parental Knowledge, Attitudes, and Practices and Their Association with Dental Caries in Children Aged 5–9 Years: A Cross-Sectional Study in Rural Ecuador. Int. J. Environ. Res. Public Health 2025, 22, 953. https://doi.org/10.3390/ijerph22060953
Saquicela-Pulla M, Dávila-Arcentales M, Vélez-León E, Armas-Vega A, Melo M. Parental Knowledge, Attitudes, and Practices and Their Association with Dental Caries in Children Aged 5–9 Years: A Cross-Sectional Study in Rural Ecuador. International Journal of Environmental Research and Public Health. 2025; 22(6):953. https://doi.org/10.3390/ijerph22060953
Chicago/Turabian StyleSaquicela-Pulla, María, Mónica Dávila-Arcentales, Eleonor Vélez-León, Ana Armas-Vega, and María Melo. 2025. "Parental Knowledge, Attitudes, and Practices and Their Association with Dental Caries in Children Aged 5–9 Years: A Cross-Sectional Study in Rural Ecuador" International Journal of Environmental Research and Public Health 22, no. 6: 953. https://doi.org/10.3390/ijerph22060953
APA StyleSaquicela-Pulla, M., Dávila-Arcentales, M., Vélez-León, E., Armas-Vega, A., & Melo, M. (2025). Parental Knowledge, Attitudes, and Practices and Their Association with Dental Caries in Children Aged 5–9 Years: A Cross-Sectional Study in Rural Ecuador. International Journal of Environmental Research and Public Health, 22(6), 953. https://doi.org/10.3390/ijerph22060953