
Neurodegenerative Disease and Association Football (NDAF): Systematic Review and Meta-Analysis

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Methods
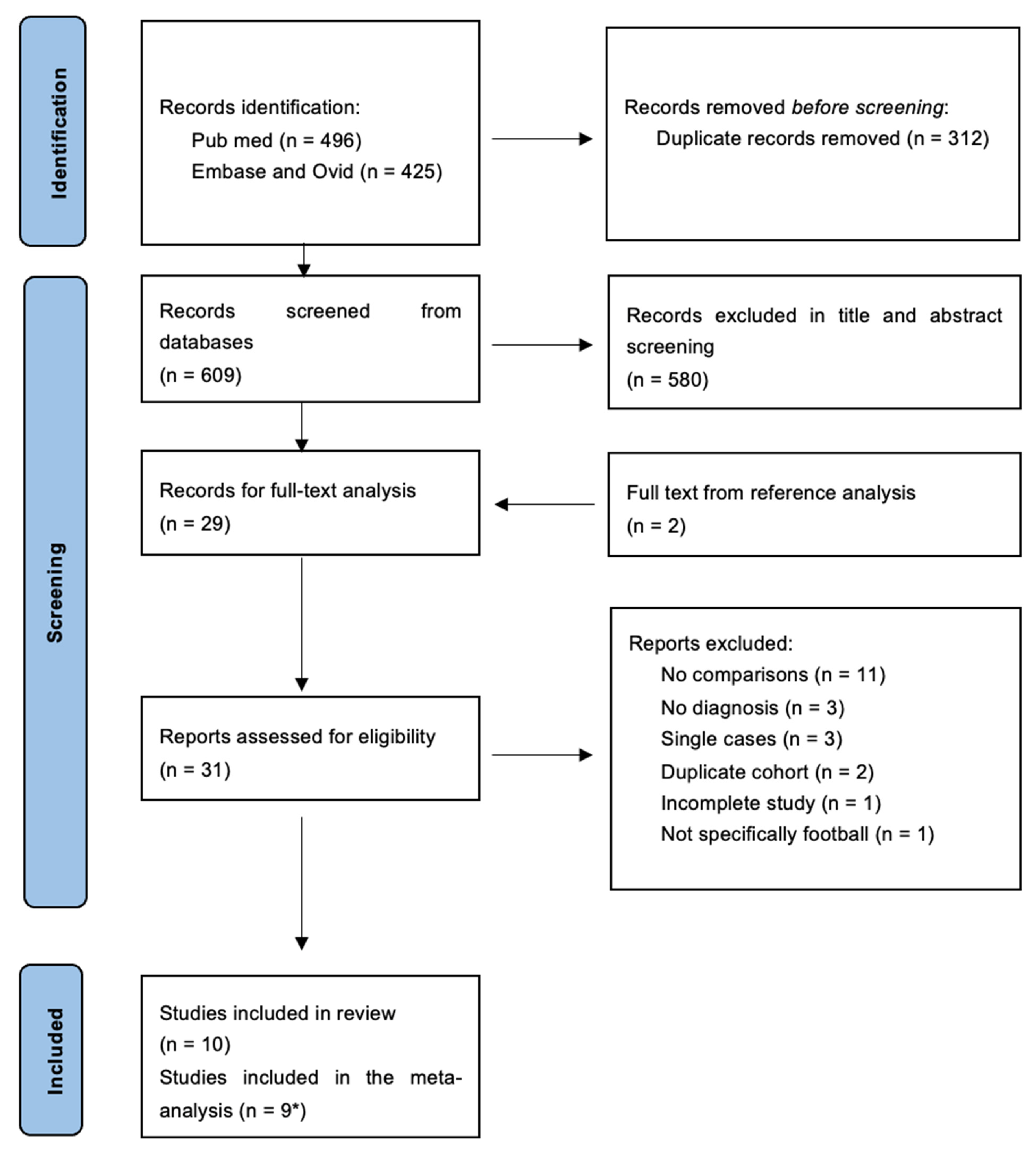
2.1. Search Strategy
2.2. Title and Abstract Analysis
2.3. Inclusion and Exclusion Criteria
2.4. Full-Text Analysis
2.5. Quality Assessment
2.6. Meta-Analysis
2.7. Publication Bias
3. Results
3.1. Population
3.2. Neurodegenerative Diseases, Dementia
3.3. Alzheimer’s Disease (AD)
3.4. Early Onset Dementias
3.5. Motor Neurone Disease (MND)
3.6. Parkinson’s Disease (PD)
3.7. Location
3.8. Study Designs
3.9. Diagnosis
3.10. Quality Assessment
3.11. Meta-Analysis
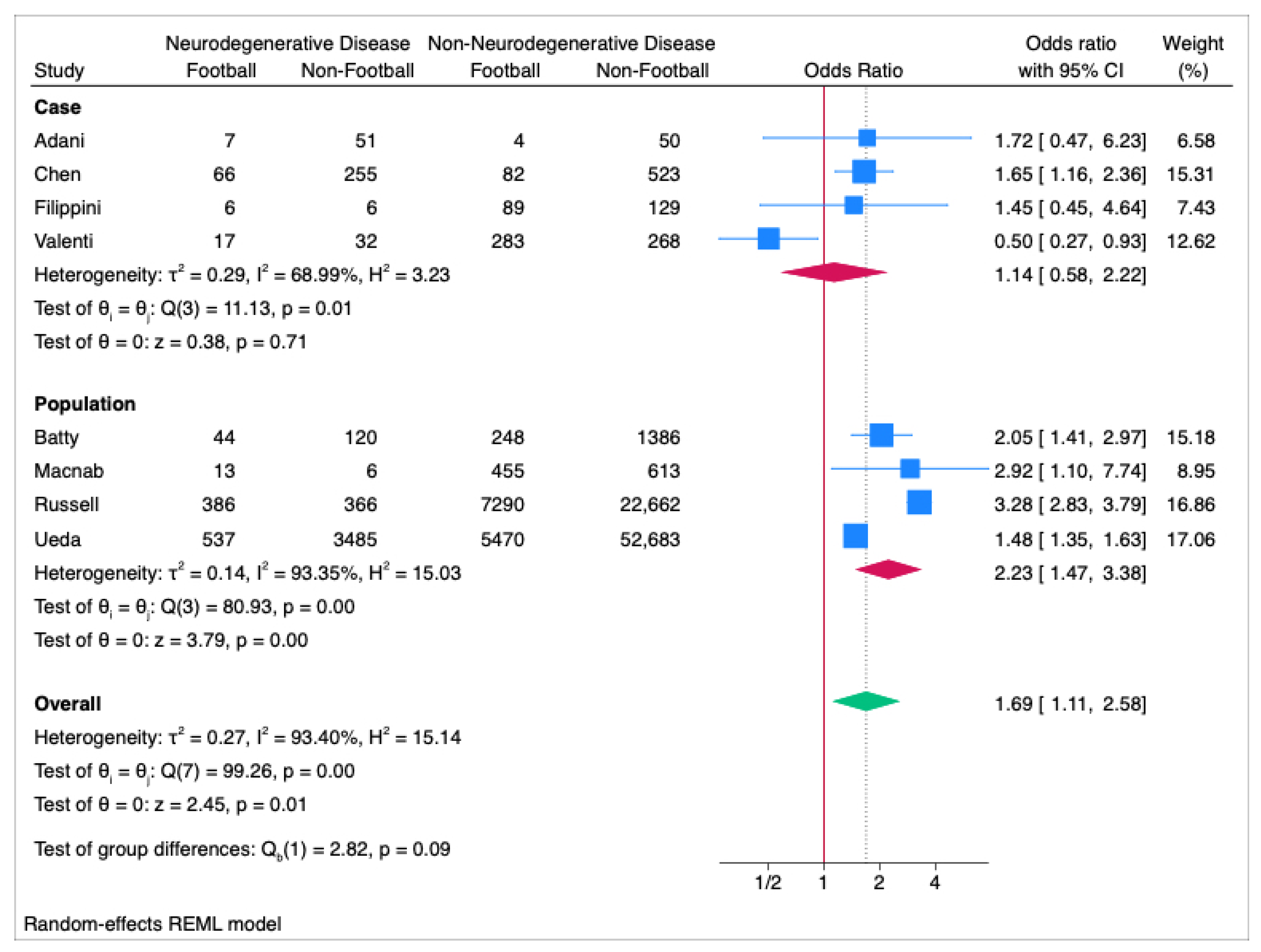
3.12. Meta-Analysis: All Neurodegenerative Disease
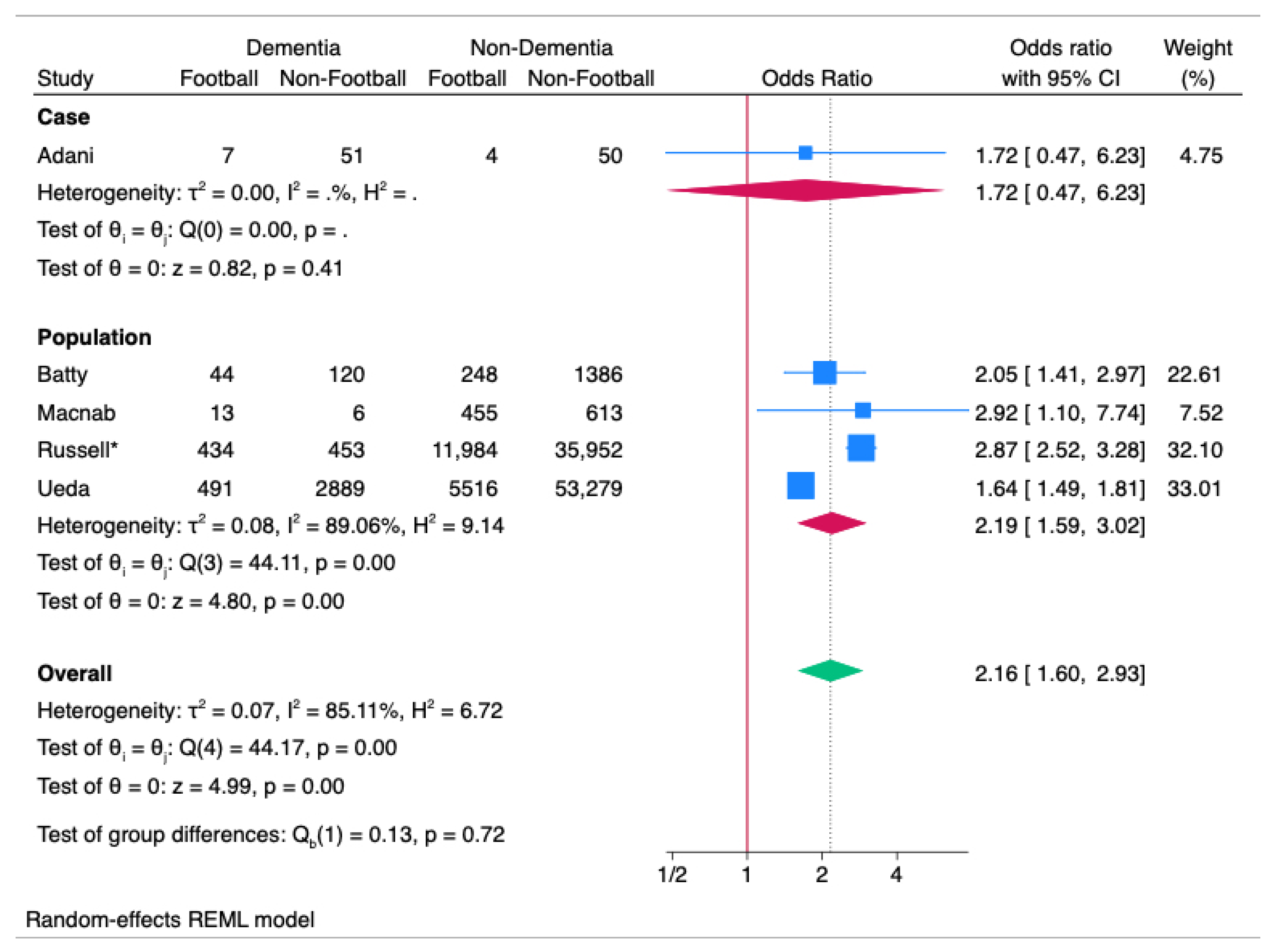
3.13. Meta-Analysis: Dementia
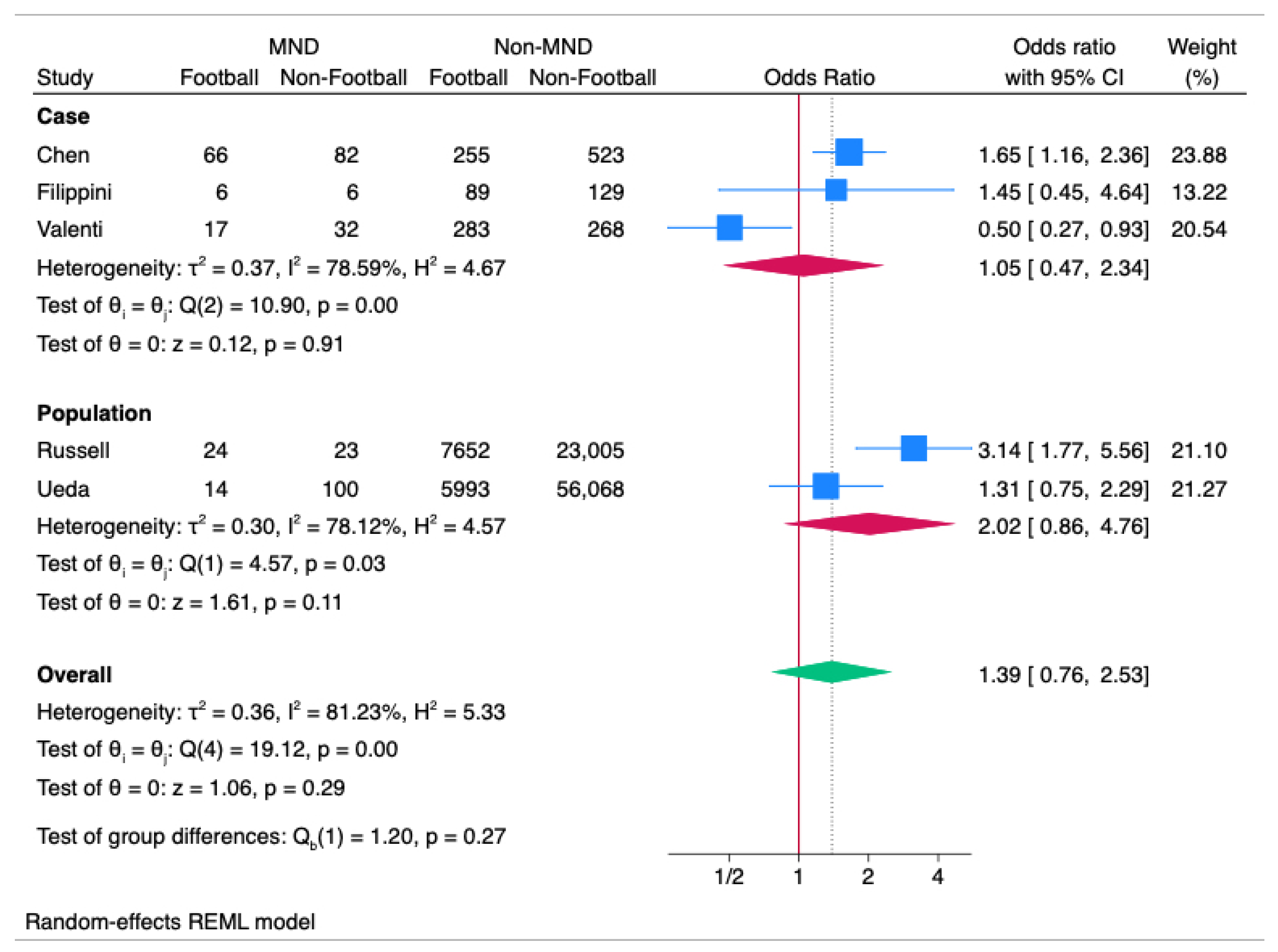
3.14. Meta-Analysis: MND
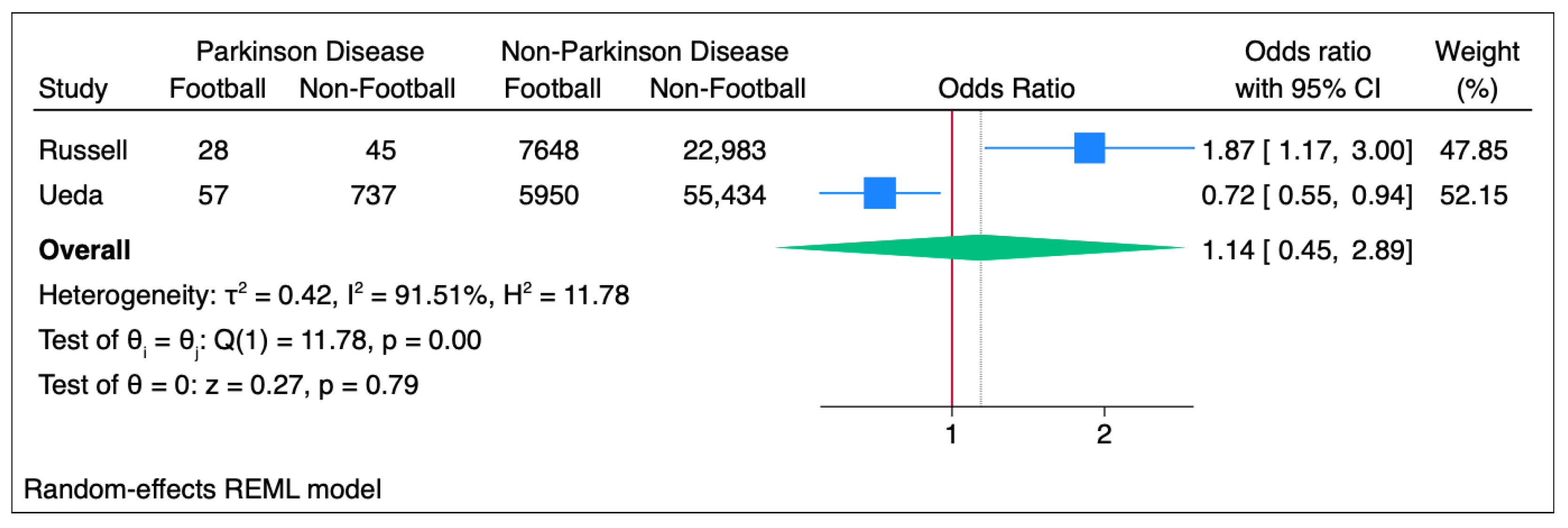
3.15. Meta-Analysis: PD
3.16. Sensitivity Analysis: All Neurodegenerative Disease
3.17. Sensitivity Analysis: Dementia
3.18. MND
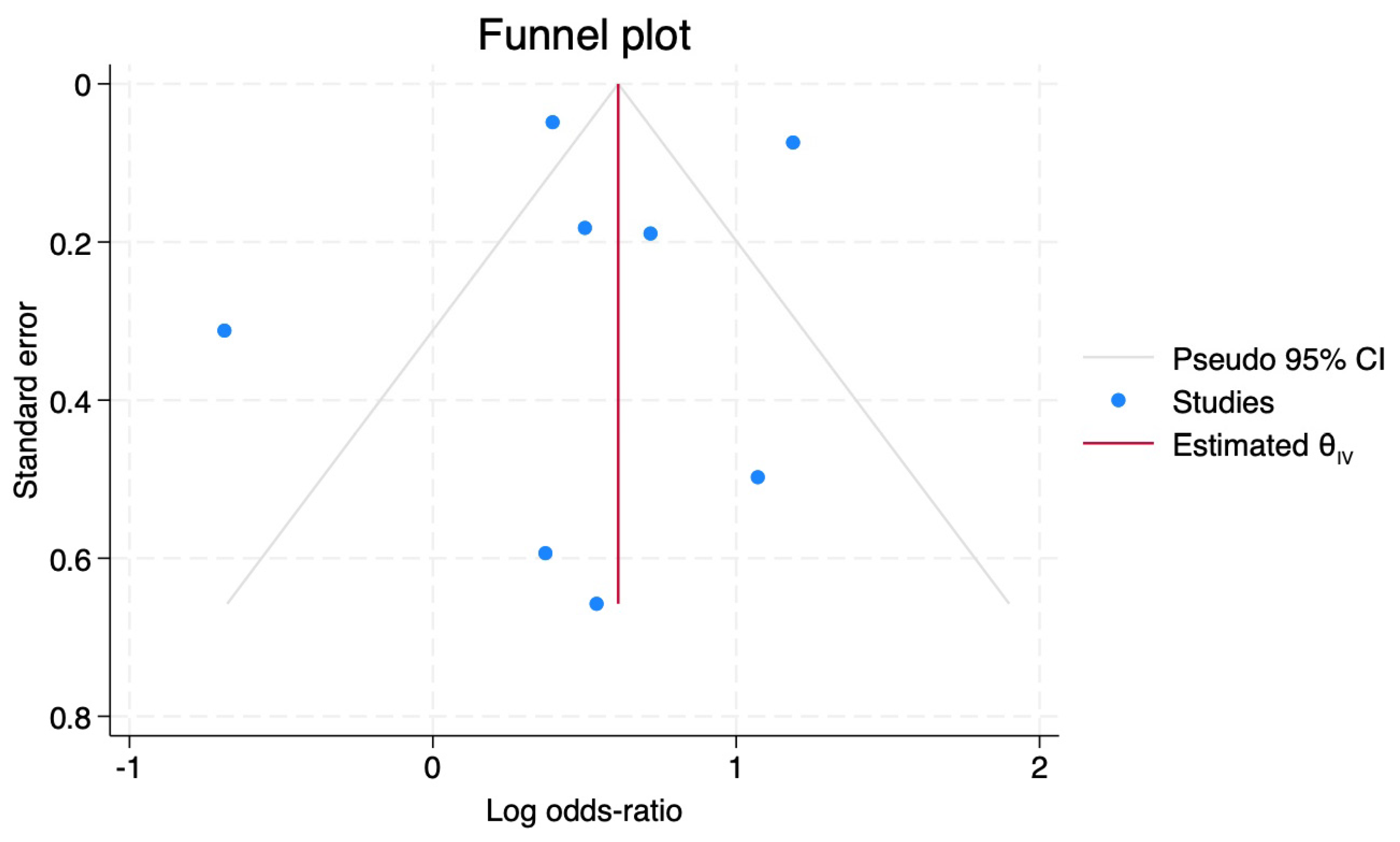
3.19. Publication Bias
4. Discussion
Future Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Berretta, S.; Carri, M.T.; Beghi, E.; Chiò, A.; Ferrarese, C. The sinister side of Italian Soccer. Lancet Neurol. 2003, 2, 656–657. [Google Scholar] [CrossRef] [PubMed]
- Valenti, M.; Pontieri, F.E.; Conti, F.; Altobelli, E.; Manzoni, T.; Frati, L. Amyotrophic lateral sclerosis and sports: A case-control study. Eur. J. Neurol. 2005, 12, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Astle, J. Foundation. Available online: https://thejeffastlefoundation.co.uk/our-story/ (accessed on 4 February 2024).
- Mackay, D.F.; Russell, E.R.; Stewart, K.; MacLean, J.A.; Pell, J.P.; Stewart, W. Neurodegenerative Disease Mortality among Former Professional Soccer Players. N. Engl. J. Med. 2019, 381, 1801–1808. [Google Scholar] [CrossRef] [PubMed]
- McKee, A.C.; Daneshvar, D.; Alvarez, V.E.; Stein, T.D. The neuropathology of Sport. Acta Neuropathol. 2014, 127, 29–51. [Google Scholar] [CrossRef] [PubMed]
- McKee, A.C.; Mez, J.; Abdolmohammadi, B.; Butler, M.; Huber, B.R.; Uretsky, M.; Babcock, K.; Cherry, J.D.; Alvarez, V.E.; Martin, B.; et al. Neuropathologic and Clinical Findings in Young Contact Sport Athletes Exposed to Repetitive Head Impacts. JAMA Neurol. 2023, 80, 1037–1050. [Google Scholar] [CrossRef] [PubMed]
- Russell, E.R.; MacKay, D.F.; Stewart, K.; MacLean, J.A.; Pell, J.P.; Stewart, W. Association of Field Position and Career Length With Risk of Neurodegenerative Disease in Male Former Professional Players. JAMA Neurol. 2021, 78, 1057–1063. [Google Scholar] [CrossRef] [PubMed]
- Russell, E.R.; Lyall, D.M.; Mackay, D.F.; Cronin, K.; Stewart, K.; MacLean, J.A.; Pell, J.P.; Stewart, W. Health and Lifestyle Factors and Dementia Risk Among Former Professional Soccer Players. JAMA Netw. Open 2024, 7, e2449742. [Google Scholar] [CrossRef] [PubMed]
- Ueda, P.; Pasternak, B.; Lim, C.-E.; Neovius, M.; Kader, M.; Forssblad, M.; Ludvigsson, J.F.; Svanström, H. Neurodegenerative disease among male elite football (soccer) players in Sweden: A cohort study. Lancet Public Health 2023, 8, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Macnab, T.-M.P.; Espahbodi, S.; Hogervorst, E.; Thanoon, A.; Ferandes, G.S.; Millar, B.; Duncan, A.; Goodwin, M.; Batt, M.; Fuller, C.W.; et al. Cognitive Impairment and Self-Reported Dementia in UK Retired Professional Soccer Players: A Cross Sectional Comparative Study. Sports Med.-Open 2023, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, K.L.; Baker, M.M.; Dalton, S.L.; Dompier, T.P.; Brogilo, S.P.; Kerr, Z.Y. Epidemiology of Sport-Related Concussions in High School Athletes: National Athletic Treatment, Injury and Outcomes Network (NATION), 2011-2012 Through 2013-2014. J. Athl. Train. 2017, 52, 175–185. [Google Scholar] [CrossRef]
- Zetterberg, H.; Blennow, K. Fluid biomarkers for mild traumatic brain injury and related conditions. Nat. Rev. Neurol. 2016, 12, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Chio, A.; Benzi, G.; Dossena, M.; Mutani, R.; Mora, G. Severely increased risk of amyotrophic lateral sclerosis among Italian professional football players. Brain 2005, 128, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Chio, A.; Calvo, A.; Dossena, M.; Ghiglione, P.; Mutani, R.; Mora, G. ALS in Italian professional soccer players: The risk is still present and could be soccer-specific. Amyotroph. Lateral Scler. 2009, 10, 205–209. [Google Scholar] [CrossRef]
- Adani, G.; Filippini, T.; Caterina, G.; Malavolti, M.; Vinceti, G.; Zamboni, G.; Tondelli, M.; Galli, C.; Costa, G.; Vinceti, M.; et al. Environmental Risk Factors for Early-Onset Alzeheimer’s Dementia and Frontotemporal Dementia: A Case-Control Study in Northern Italy. Int. Environ. Res. Public. Health 2020, 17, 7941. [Google Scholar] [CrossRef]
- Batty, G.D.; Frank, P.; Kujala, U.M.; Sarna, S.J.; Valencia-Hernández, C.A.; Kaprio, J. Dementia in former amateur and professional contact sports participants: Population-based cohort study, systematic review, and meta-analysis. eClinicalMedicine 2023, 61, 102056. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.X.; Douwes, J.; van den Berg, L.; Glass, B.; McLean, D.; Mannetje, A.M. Sports and trauma as risk factors for Motor Neurone Disease: New Zealand case-control study. Acta Neurol. Scand. 2022, 145, 770–785. [Google Scholar] [CrossRef] [PubMed]
- Filippini, T.; Fiore, M.; Tesauro, M.; Malagoli, C.; Consonni, M.; Violi, F.; Arcolin, E.; Iacuzio, L.; Conti, G.O.; Cristaldi, A.; et al. Clinical and Lifestyle Factors and Risk of Amyotrophic Lateral Sclerosis: A Population-Based Case-Control Study. Int. J. Environ. Res. Public Health 2020, 17, 857. [Google Scholar] [CrossRef]
- Orhant, E.; Carling, C.; Chapellier, J.-F.; Marchand, J.-L.; Pradat, P.-F.; Elbaz, A.; Maniez, S.; Moisan, F.; Rochcongar, P. A retrospective analysis of all-cause and cause specific mortality rates in French male professional footballers. Scand. J. Med. Sci. Sports 2022, 32, 1389–1399. [Google Scholar] [CrossRef] [PubMed]
- Celtic, F.C. Past Seasons. Available online: https://www.celticfc.com/history/results-archive/ (accessed on 8 June 2024).
- BESOCCER. Website. Available online: https://www.besoccer.com/team/matches/olympique-marsella (accessed on 8 June 2024).
- GSA (Global Sports Achieve). Website. Available online: https://globalsportsarchive.com/team/soccer/malmo-ff/1293/ (accessed on 8 June 2024).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Characteristics | Population |
|---|---|---|
| Adani [15] | Italian study specifically looking at Early Onset Dementia (EOD). Mixture of former amateurs and professional footballers. The matched controls to EOD were the caregivers irrespective of age. | Total 112 Football Dementia 7, Non-Football Dementia 51, Football Non-Dementia 4, Non-Football Non-Dementia 50 |
| Batty [16] | Finnish study with surveillance ending in 2015. Mixture of former amateurs and professional footballers. Controls from military and civil servants were age-, gender-, and socio-economically matched. | Total 1798 Football Dementia 44, Non-Football Dementia 120, Football Non-Dementia 248, Non-Football Non-Dementia 1386 |
| Chen [17] | New Zealand MND nationwide surveillance 2013–2016. Mixture of former amateurs and professional footballers. Controls from general population, which were socio-economically matched. The general population had an over-representation of individuals in their 70s. | Total 926 Football MND 66, Non-Football MND 255, Football Non-MND 82, Non-Football Non-MND 523 |
| Chio * [14] | Italian study focused on MND cases in former professional footballers. Controls are athletic populations, cyclists and basketballers. Between 1970 and 2006. | Total 10,999 Football MND 8, Non-Football MND 0, Football Non-MND 7317, Non-Football Non-MND 3674 |
| Filippini [18] | Italian study on MND 2008 to 2011 in two regions and 2002–2012 to a third. Cases of competitive football were recruited through discharge letters or death certificates. Controls were recruited from the general population who was age-, sex-, and socio-economically matched. | Total 230 Football MND 6, Non-Football MND 6, Football Non-MND 89, Non-Football Non-MND 129 |
| Macnab [10] | Cross-sectional study into Dementia in Nottinghamshire, UK. Self-disclosed diagnosis in both the former professional footballers and age- and sex-matched general population controls. | Total 1087 Football Dementia 13, Non-Football Dementia 6, Non-Football Non-Dementia 455, Non-Football Non-Dementia 613 |
| Russell ** [7] Included for Neurodegenerative Disease, Parkinson’s Disease, and MND analysis. | Scottish cohort study following former professional footballers with age- and gender-matched general population controls for Alzheimer’s, MND, and Parkinson’s Disease. Based upon clinical records through prescriptions and death certificates. Collection ended December 2018. | Total 30,704 Football Neurodegeneration 386, Non-Football Neurodegeneration 366, Football Non-Neurodegeneration 7290, Non-Football Non-Neurodegeneration 22,662 |
| Russell ** [8] Included for Dementia analysis. | Scottish cohort study following former professionals with age- and gender-matched general population controls for Alzheimer’s, MND, and Parkinson’s Disease. Based upon clinical records through prescriptions and death certificates. Collection ended in December 2021. | Total 47,936 Football Dementia 434, Non-Football Dementia 453, Football Non-Dementia 11,550, Non-Football Non-Dementia 35,499 |
| Ueda [9] | Swedish cohort study of amateur and professional based upon prescription data and death certificates. Controls were matched based on year of birth, locality, and sex. | Total 62,175 Football Neurodegeneration 537, Non-Football Neurodegeneration 3485, Football Non-Neurodegeneration 5470, Non-Football Non-Neurodegeneration 52,683 |
| Valenti [2] | Italian MND study from January 2002 to May 2003 with competitive and amateur football practice in Neurology clinics and control populations from general population locally, age- and sex-matched. | Total 600 Football MND 17, Non-Football MND 32, Football Non-MND 283, Non-Football Non-MND 268 |
| JBI Case-Control Studies | Adani [15] | Chen [17] | Filippini [18] | Valenti [2] | JBI Cohort Studies | Batty [16] | Chio [14] | Russell [7] | Russell [8] | Ueda [9] | JBI Cross-Sectional Studies | Macnab [10] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Were the groups comparable other than the presence of disease in cases or the absence of disease in controls? | n | y | Y | y | 1. Were the two groups similar and recruited from the same population? | n | n | n | n | y | 1. Were the criteria for inclusion in the sample clearly defined? | y |
| 2. Were cases and controls matched appropriately? | n | n | Y | y | 2. Were the exposures measured similarly to assign people to both exposed and unexposed groups? | y | y | y | y | y | 2. Were the study subjects and the setting described in detail? | y |
| 3. Were the same criteria used for identification of cases and controls? | n | y | y | y | 3. Was the exposure measured in a valid and reliable way? | y | y | y | y | y | 3. Was the exposure measured in a valid and reliable way? | n |
| 4. Was exposure measured in a standard, valid, and reliable way? | u | y | y | y | 4. Were confounding factors identified? | y | n | y | y | y | 4. Were objective, standard criteria used for measurement of the condition? | n |
| 5. Was exposure measured in the same way for cases and controls? | y | y | y | u | 5. Were strategies to deal with confounding factors stated? | u | u | y | y | y | 5. Were confounding factors identified? | y |
| 6. Were confounding factors identified? | y | y | y | y | 6. Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)? | u | u | u | u | u | 6. Were strategies to deal with confounding factors stated? | y |
| 7. Were strategies to deal with confounding factors stated? | u | y | y | y | 7. Were the outcomes measured in a valid and reliable way? | y | y | y | y | y | 7. Were the outcomes measured in a valid and reliable way? | y |
| 8. Were outcomes assessed in a standard, valid, and reliable way for cases and controls? | y | y | y | u | 8. Was the follow-up time reported and sufficient to be long enough for outcomes to occur? | y | y | y | y | y | 8. Was appropriate statistical analysis used? | y |
| 9. Was the exposure period of interest long enough to be meaningful? | u | u | u | u | 9. Was follow up complete, and if not, were the reasons for loss to follow up described and explored? | y | n | y | y | y | ||
| 10. Was appropriate statistical analysis used? | u | y | y | y | 10. Were strategies to address incomplete follow up utilized? | na | y | na | na | na | ||
| 11. Was appropriate statistical analysis used? | y | y | y | y | y |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Howarth, N.E.; Ji, C.; Batten, J.; Pearce, A.J.; Dawes, H.; White, A.J.; DeLuca, G.; Bureau, S.; Nowinski, C.J.; Miller, M.A. Neurodegenerative Disease and Association Football (NDAF): Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2025, 22, 806. https://doi.org/10.3390/ijerph22050806
Howarth NE, Ji C, Batten J, Pearce AJ, Dawes H, White AJ, DeLuca G, Bureau S, Nowinski CJ, Miller MA. Neurodegenerative Disease and Association Football (NDAF): Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2025; 22(5):806. https://doi.org/10.3390/ijerph22050806
Chicago/Turabian StyleHowarth, Nathan E., Chen Ji, John Batten, Alan J. Pearce, Helen Dawes, Adam J. White, Gabriele DeLuca, Samantha Bureau, Christopher J. Nowinski, and Michelle A. Miller. 2025. "Neurodegenerative Disease and Association Football (NDAF): Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 22, no. 5: 806. https://doi.org/10.3390/ijerph22050806
APA StyleHowarth, N. E., Ji, C., Batten, J., Pearce, A. J., Dawes, H., White, A. J., DeLuca, G., Bureau, S., Nowinski, C. J., & Miller, M. A. (2025). Neurodegenerative Disease and Association Football (NDAF): Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 22(5), 806. https://doi.org/10.3390/ijerph22050806