
Leveraging Stakeholder Engagement for Adolescent School Journeys in Malawi: An Exploration of Road Safety and Air Pollution Interventions

 , , and
, , and
Abstract
1. Introduction
- To identify and seek consensus on potential interventions for the prevention of road crashes and air pollution on school children’s journeys to school in urban Blantyre, Malawi.
- To explore contextual barriers and facilitators to implementation of preventative interventions in urban Blantyre.
2. Materials and Methods
- Identification and recruitment of local and international stakeholders.
- Successive consensus rounds.
- (a)
- First-round identification of potential interventions from experts.
- Feeding these interventions to community members (teachers and parents from urban schools in Blantyre) to understand barriers and facilitators.
- (b)
- Second-round ranking of interventions by experts.
- Focus group discussions among experts.
- (c)
- Third-round ranking of interventions by experts.
- Mapping of interventions onto relevant evidence-based frameworks.
- Reduction of intervention list based on evidence and response analysis.
2.1. Identification and Recruitment
2.2. Successive Consensus Rounds
2.3. Reduction of Intervention List
2.4. Statistical Analysis
- fi = frequency of responses at rank position i,wi = weight assigned to rank position i,n = total number of rank positions (number of interventions in the domain),N = number of interventions in the domain.
2.5. Ethics
3. Results
3.1. Identification and Ranking of Interventions
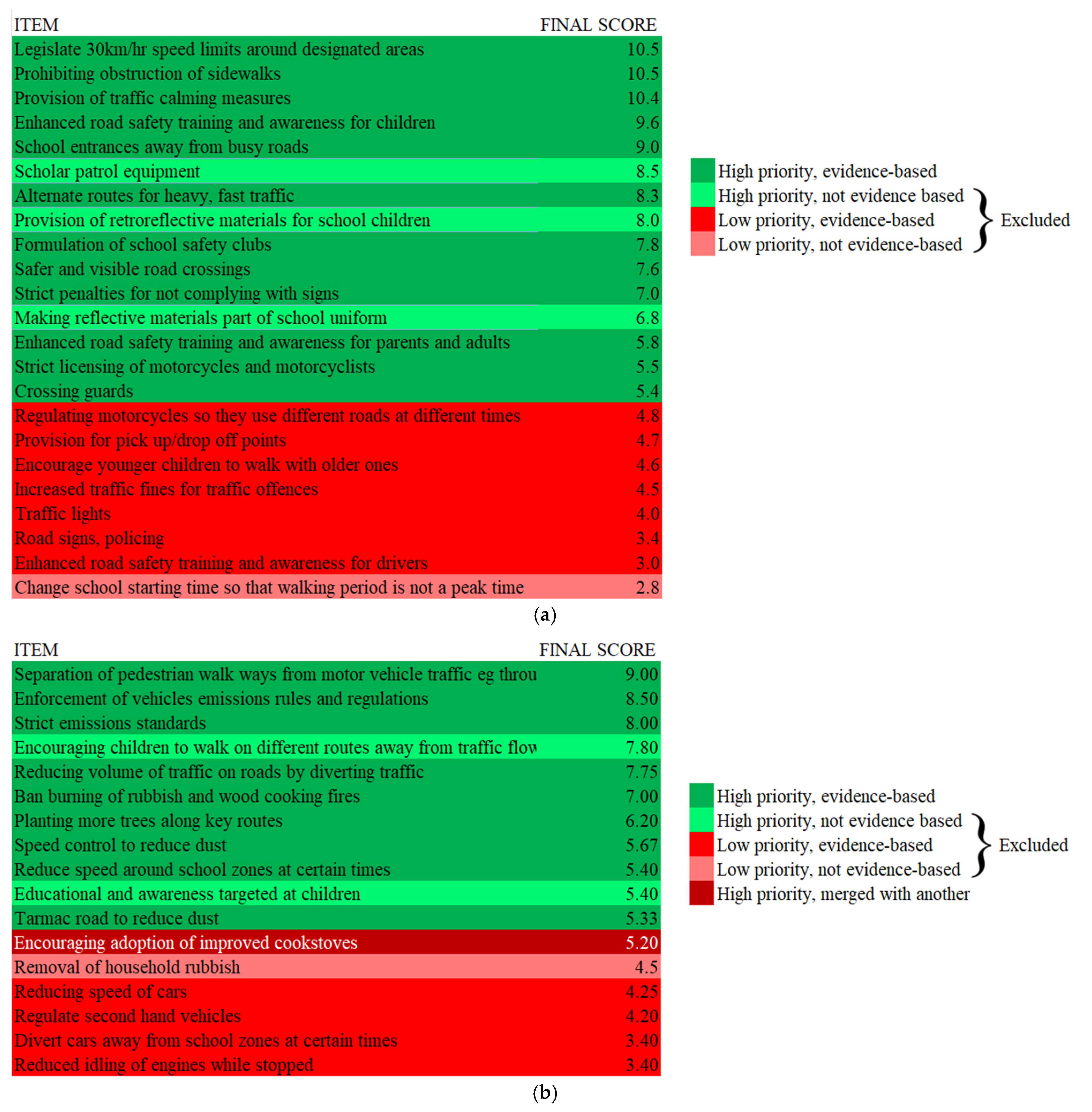
3.2. Response Analysis and Reduction
3.3. Community and Expert Perspectives on Barriers and Facilitators
“I think it is impossible because some licenses are issued out illegally” (Participant A).
“Then it is impossible. This is because those entrusted with the responsibility of collecting the fines are corrupt so it would be a way of enriching themselves” (Participant B).
“People are buying licenses” (Participant C).
“Police officers …would demand money… That would not deter the would-be offenders” (Participant D).
“People have not yet been told about the offenses and penalties” (Participant E).
“It is impossible because it is too expensive” (Participant C).
“Impossible, 30 km/h is just a small speed limit” (Participant F),
“Would lead to congestion” (Participant A)
“Impossible, Blantyre was already given a small speed limit which is 60 km/h” (Participant G).
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Unfinished Journey: The Global Health Response to Children & Road Traffic; FIA Foundation: London, UK, 2019.
- Global Status Report on Road Safety 2023. Available online: https://www.who.int/publications/i/item/9789240086517 (accessed on 31 October 2024).
- Dondi, A.; Carbone, C.; Manieri, E.; Zama, D.; Del Bono, C.; Betti, L.; Biagi, C.; Lanari, M. Outdoor Air Pollution and Childhood Respiratory Disease: The Role of Oxidative Stress. Int. J. Mol. Sci. 2023, 24, 4345. [Google Scholar] [CrossRef]
- Atkinson, R.W.; Mills, I.C.; Walton, H.A.; Anderson, H.R. Fine Particle Components and Health—A Systematic Review and Meta-Analysis of Epidemiological Time Series Studies of Daily Mortality and Hospital Admissions. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Sager, L. Estimating the Effect of Air Pollution on Road Safety Using Atmospheric Temperature Inversions. J. Environ. Econ. Manag. 2019, 98, 102250. [Google Scholar] [CrossRef]
- Wan, I.Y.P.; Wat, K.H.Y.; Ng, C.S.H.; Thung, K.H.; Lam, S.; Lee, T.W.; Wan, S.; Yim, A.P.C. Evaluation of the Emotional Status of Patients on a Waiting List for Thoracic Surgery during the Outbreak of Severe Acute Respiratory Syndrome (SARS). Stress Health 2004, 20, 209–212. [Google Scholar] [CrossRef]
- Zhang, K.; Batterman, S. Air Pollution and Health Risks Due to Vehicle Traffic. Sci. Total Environ. 2013, 450–451, 307–316. [Google Scholar] [CrossRef]
- WHO Global Air Quality Guidelines. In Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organisation: Geneva, Switzerland, 2021.
- Sundet, M.; Grudziak, J.; Charles, A.; Banza, L.; Varela, C.; Young, S. Paediatric Road Traffic Injuries in Lilongwe, Malawi: An Analysis of 4776 Consecutive Cases. Trop. Doct. 2018, 48, 316–322. [Google Scholar] [CrossRef]
- Rylance, S.; Nightingale, R.; Naunje, A.; Mbalume, F.; Jewell, C.; Balmes, J.R.; Grigg, J.; Mortimer, K. Lung Health and Exposure to Air Pollution in Malawian Children (CAPS): A Cross-Sectional Study. Thorax 2019, 74, 1070–1077. [Google Scholar] [CrossRef]
- Kweon, B.-S.; Mohai, P.; Lee, S.; Sametshaw, A.M. Proximity of Public Schools to Major Highways and Industrial Facilities, and Students’ School Performance and Health Hazards. Environ. Plan. B Urban Anal. City Sci. 2018, 45, 312–329. [Google Scholar] [CrossRef]
- Peden, M.M.; Khayesi, M. Save LIVES Technical Package: 22 Interventions That Could Make a Difference. Inj. Prev. 2018, 24, 381–383. [Google Scholar] [CrossRef]
- Pedestrian Safety: A Road Safety Manual for Decision-Makers and Practitioners. Available online: https://www.who.int/publications-detail-redirect/pedestrian-safety-a-road-safety-manual-for-decision-makers-and-practitioners (accessed on 10 April 2024).
- Ten Strategies for Keeping Children Safe on the Road; World Health Organisation: Geneva, Switzerland, 2015.
- Burns, J.; Boogaard, H.; Polus, S.; Pfadenhauer, L.M.; Rohwer, A.C.; Erp, A.M.V.; Turley, R.; Rehfuess, E. Interventions to Reduce Ambient Particulate Matter Air Pollution and Their Effect on Health. Cochrane Database Syst. Rev. 2019, 20, CD010919. [Google Scholar] [CrossRef]
- Maher, B.A.; Gonet, T.; Karloukovski, V.V.; Wang, H.; Bannan, T.J. Protecting Playgrounds: Local-Scale Reduction of Airborne Particulate Matter Concentrations through Particulate Deposition on Roadside ‘Tredges’ (Green Infrastructure). Sci. Rep. 2022, 12, 14236. [Google Scholar] [CrossRef] [PubMed]
- Poswayo, A.; Kalolo, S.; Rabonovitz, K.; Witte, J.; Guerrero, A. School Area Road Safety Assessment and Improvements (SARSAI) Programme Reduces Road Traffic Injuries among Children in Tanzania. Inj. Prev. 2019, 25, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Jack, D.W.; Asante, K.P.; Wylie, B.J.; Chillrud, S.N.; Whyatt, R.M.; Ae-Ngibise, K.A.; Quinn, A.K.; Yawson, A.K.; Boamah, E.A.; Agyei, O.; et al. Ghana Randomized Air Pollution and Health Study (GRAPHS): Study Protocol for a Randomized Controlled Trial. Trials 2015, 16, 420. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, E.; Lechat, L.; Ridde, V. What Interventions Are Required to Reduce Road Traffic Injuries in Africa? A Scoping Review of the Literature. PLoS ONE 2018, 13, e0208195. [Google Scholar] [CrossRef]
- Jessani, N.S.; Delobelle, P.; Balugaba, B.E.; Mpando, T.L.; Ayele, F.M.; Ntawuyirushintege, S.; Rohwer, A. Integrated Knowledge Translation for Non-Communicable Diseases: Stories from Sub-Saharan Africa. Ann. Glob. Health 2023, 89, 87. [Google Scholar] [CrossRef]
- Li, Q.; Alonge, O.; Hyder, A.A. Children and Road Traffic Injuries: Can’t the World Do Better? Arch. Dis. Child. 2016, 101, 1063–1070. [Google Scholar] [CrossRef]
- Gupta, U.G.; Clarke, R.E. Theory and Applications of the Delphi Technique: A Bibliography (1975–1994). Technol. Forecast. Soc. Change 1996, 53, 185–211. [Google Scholar] [CrossRef]
- Rowe, G.; Wright, G. The Delphi Technique: Past, Present, and Future Prospects—Introduction to the Special Issue. Technol. Forecast. Soc. Change 2011, 78, 1487–1490. [Google Scholar] [CrossRef]
- Barffour, M.; Gupta, S.; Gururaj, G.; Hyder, A.A. Evidence-Based Road Safety Practice in India: Assessment of the Adequacy of Publicly Available Data in Meeting Requirements for Comprehensive Road Safety Data Systems. Traffic Inj. Prev. 2012, 13, 17–23. [Google Scholar] [CrossRef]
- Chinkonda, B.; Piragauta, A.; Mazingi, D.; Chokotho, L.; Nzanga, M.; Manyozo, S.; Puvanachandra, P.; Peden, M. Parents’ and Teachers’ Perceptions of Risks Associated with Children’s Walks to School in Blantyre, Malawi. Int. J. Environ. Res. Public Health 2024, 21, 1479. [Google Scholar] [CrossRef]
- Odonkor, S.T.; Mitsotsou-Makanga, H.; Dei, E.N. Road Safety Challenges in Sub-Saharan Africa: The Case of Ghana. J. Adv. Transp. 2020, 2020, 7047189. [Google Scholar] [CrossRef]
- Sabi Boun, S.; Janvier, R.; Jean Marc, R.E.; Paul, P.; Senat, R.; Demes, J.A.E.; Burigusa, G.; Chaput, S.; Maurice, P.; Druetz, T. Environmental Measures to Improve Pedestrian Safety in Low- and Middle-Income Countries: A Scoping Review. Glob. Health Promot. 2024, 31, 44–55. [Google Scholar] [CrossRef]
- Mesic, A.; Damsere-Derry, J.; Gyedu, A.; Mock, C.; Larley, J.; Opoku, I.; Wuaku, D.H.; Kitali, A.; Osei-Ampofo, M.; Donkor, P.; et al. Generating Consensus on Road Safety Issues and Priorities in Ghana: A Modified Delphi Approach. Injury 2023, 54, 110765. [Google Scholar] [CrossRef] [PubMed]
- Sam, E.F. How Effective Are Police Road Presence and Enforcement in a Developing Country Context? Humanit. Soc. Sci. Commun. 2022, 9, 55. [Google Scholar] [CrossRef]
- Muula, A.S.; Misiri, H.E. Physical Trauma Experience among School Children in Periurban Blantyre, Malawi. Int. Arch. Med. 2009, 2, 20. [Google Scholar] [CrossRef] [PubMed]
- Delavary, M.; Mesic, A.; Krebs, E.; Sesonga, P.; Uwase-Gakwaya, B.; Nzeyimana, I.; Vanlaar, W. Assessing the Effect of Automated Speed Enforcement and Comprehensive Measures on Road Safety in Rwanda. Traffic Inj. Prev. 2024, 25, 947–955. [Google Scholar] [CrossRef]
- News, T. Government Yields to Pressure on Used Car Imports Duty; The Times Group: Mumbai, India, 8 July 2023. [Google Scholar]
- Kessi, M.; Sokoni, D.; Kitambi, M.; Katopola, D.; Fedjo, G.; Kileo, N.; Murphy, E.; Maxmillan, M.; Rweyemamu, L.; John, J.J.; et al. Reducing Deaths and Injury from Road Traffic Crashes through Multisectoral Collaboration. Pan. Afr. Med. J. 2023, 45, 1. [Google Scholar] [CrossRef]
- Hanson, D.; Finch, C.; Allegrante, J.; Sleet, D. Closing the Gap: Progressing from Injury Prevention Research to Safety Promotion Practice. Inj. Prev. 2012, 18, A8–A9. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Type of Participant | Criteria for Eligibility |
|---|---|
| Academic researcher | Lead author or co-author in at least one article pertaining to either road safety or air pollution in Malawi published after 2010. |
| Clinicians | Medically qualified clinicians with at least 2 years’ experience in the field of emergency medicine, trauma, respiratory diseases, or pediatrics. |
| Non-Governmental Organizations and policymakers | At least 6 months’ experience in the arena of road safety, environmental health, or child health. |
| Invitations (n = 38) | Round 1 (n = 27) | Round 2 (n = 11) | Round 3 (n = 10) | |
|---|---|---|---|---|
| Gender | ||||
| Male | 22 | 14 | 4 | 4 |
| Female | 15 | 12 | 7 | 6 |
| Prefer not to say | 1 | 1 | 0 | 0 |
| Country of residence | ||||
| Local | 21 | 12 | 5 | 4 |
| International | 17 | 15 | 6 | 6 |
| Current Role | ||||
| Academia | 11 | 11 | 4 | 4 |
| NGO | 6 | 6 | 3 | 3 |
| Multi-lateral organisation | 2 | 1 | 0 | 0 |
| Government | 11 | 5 | 2 | 1 |
| Clinical | 8 | 4 | 2 | 2 |
| Domain of expertise | ||||
| Road Safety | 25 | 17 | 11 | 10 |
| Air pollution | 10 | 7 | 0 | 0 |
| Combination | 3 | 3 | 0 | 0 |
| Save LIVES Component | Interventions Identified by Experts | Code Frequency * |
| Speed Management | Provision of traffic calming measures | 8 |
| Legislate 30 km/h speed limits around designated areas | 3 | |
| Leadership on road safety | Enhanced road safety training and awareness for children | 6 |
| Enhanced road safety training and awareness for drivers | 4 | |
| Enhanced road safety training and awareness for parents and adults | 2 | |
| Formulation of school safety clubs | 1 | |
| Crossing guards | 1 | |
| Encourage younger children to walk with older ones | 1 | |
| Infrastructure design and improvement | Safer and visible road crossings | 5 |
| Alternate routes for heavy, fast traffic | 2 | |
| School entrances away from busy roads | 1 | |
| Provision for pick up/drop off points | 1 | |
| Vehicle safety | - | 0 |
| Enforcement of traffic laws | Strict licensing of motorcycles and motorcyclists | 4 |
| Strict penalties for not complying with signs | 3 | |
| Increased traffic fines for traffic offences | 3 | |
| Regulating motorcycles so they use different roads at different times | 3 | |
| Road signs, policing | 3 | |
| Survival | - | 0 |
| Non-evidence-based interventions | Making reflective materials part of school uniform | 2 |
| Provision of scholar patrol equipment | 1 | |
| Change school starting time so that walking period is not a peak time | 1 | |
| Provision of retroreflective materials for school children | 1 |
| Framework Component | Interventions Identified by Experts | Code Frequency * |
|---|---|---|
| Residential sources | Ban burning of rubbish and wood cooking fires | 3 |
| Encouraging adoption of improved cookstoves | 1 | |
| Industrial sources | - | 0 |
| Vehicular sources | Reducing volume of traffic on roads by diverting traffic | 4 |
| Enforcement of vehicles emissions rules and regulations | 4 | |
| Separation of pedestrian walkways from motor vehicle traffic, e.g., through parks | 3 | |
| Regulate second-hand vehicles | 3 | |
| Speed control to reduce dust | 3 | |
| Tarmac road to reduce dust | 3 | |
| Divert cars away from school zones at certain times | 2 | |
| Reduce speed around school zones at certain times | 1 | |
| Reducing speed of cars | 1 | |
| Strict emissions standards | 1 | |
| Reduced idling of engines while stopped | 1 | |
| Miscellaneous sources | Planting more trees along key routes | 1 |
| Limited-evidence based (as isolated interventions) | Education and awareness targeted at children | 5 |
| Removal of household rubbish | 3 | |
| Encouraging children to walk on different routes away from traffic flow | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazingi, D.; Puvanachandra, P.; Piragauta, A.; Chinkonda, B.E.; Nzanga, M.; Chokotho, L.; Peden, M.M. Leveraging Stakeholder Engagement for Adolescent School Journeys in Malawi: An Exploration of Road Safety and Air Pollution Interventions. Int. J. Environ. Res. Public Health 2025, 22, 758. https://doi.org/10.3390/ijerph22050758
Mazingi D, Puvanachandra P, Piragauta A, Chinkonda BE, Nzanga M, Chokotho L, Peden MM. Leveraging Stakeholder Engagement for Adolescent School Journeys in Malawi: An Exploration of Road Safety and Air Pollution Interventions. International Journal of Environmental Research and Public Health. 2025; 22(5):758. https://doi.org/10.3390/ijerph22050758
Chicago/Turabian StyleMazingi, Dennis, Prasanthi Puvanachandra, Alejandra Piragauta, Bosco Exson Chinkonda, Monica Nzanga, Linda Chokotho, and Margaret Mary Peden. 2025. "Leveraging Stakeholder Engagement for Adolescent School Journeys in Malawi: An Exploration of Road Safety and Air Pollution Interventions" International Journal of Environmental Research and Public Health 22, no. 5: 758. https://doi.org/10.3390/ijerph22050758
APA StyleMazingi, D., Puvanachandra, P., Piragauta, A., Chinkonda, B. E., Nzanga, M., Chokotho, L., & Peden, M. M. (2025). Leveraging Stakeholder Engagement for Adolescent School Journeys in Malawi: An Exploration of Road Safety and Air Pollution Interventions. International Journal of Environmental Research and Public Health, 22(5), 758. https://doi.org/10.3390/ijerph22050758