Factors Influencing Mental Health Outcomes Amongst Senescent County Residents


Abstract
1. Introduction
2. Materials and Methods
2.1. Survey Design
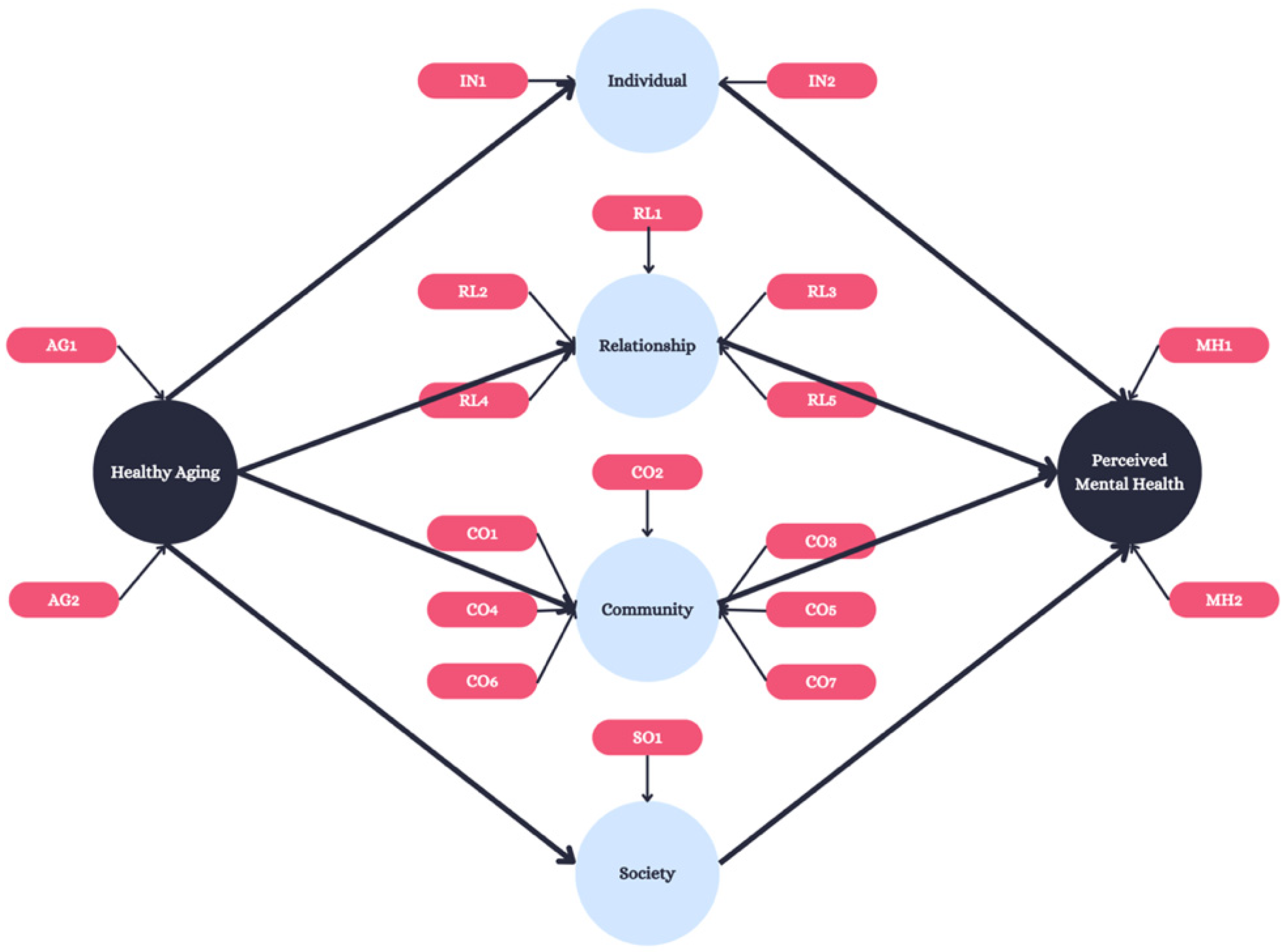
2.2. Proposed Model
2.3. Statistical Analysis
3. Results
3.1. Respondents
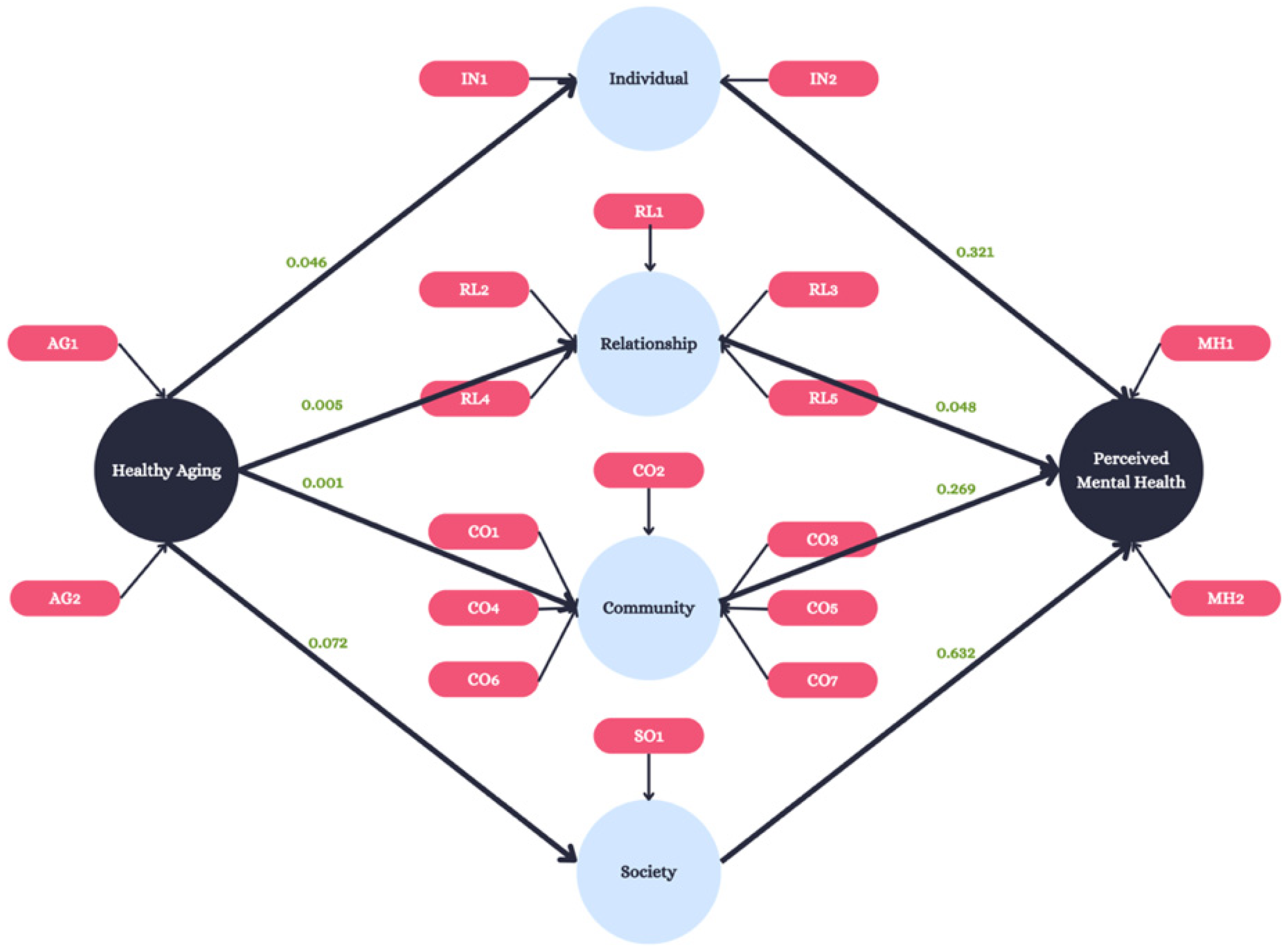
3.2. Model Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mental Health America. The State of Mental Health in America. Available online: https://mhanational.org/news/mha-releases-2024-state-of-mental-health-in-america-report/ (accessed on 7 August 2024).
- National Institute of Mental Health (NIMH). Mental Illness. Available online: https://www.nimh.nih.gov/health/statistics/mental-illness (accessed on 7 August 2024).
- Henderson, C.; Evans-Lacko, S.; Thornicroft, G. Mental illness stigma, help seeking, and public health programs. Am. J. Public Health 2013, 103, 777–780. [Google Scholar] [CrossRef]
- Merz, S.M.; Fache, S.M. Behavioral health in the pandemic: Making the shift from mental illness to mental well-being. Front. Health Serv. Manag. 2021, 38, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Stepanova, E.; Thompson, A.; Yu, G.; Fu, Y. Changes in mental health services in response to the COVID-19 pandemic in high-income countries: A rapid review. BMC Psychiatry 2024, 24, 103. [Google Scholar] [CrossRef]
- Parkar, S.R. Elderly Mental Health: Needs. Mens Sana Monogr. 2015, 13, 91–99. [Google Scholar] [CrossRef]
- Bradshaw, L.E.; Goldberg, S.E.; Lewis, S.A.; Whittamore, K.; Gladman, J.R.F.; Jones, R.G.; Harwood, R.H. Six-month outcomes following an emergency hospital admission for older adults with co-morbid mental health problems indicate complexity of care needs. Age Ageing 2013, 42, 582–588. [Google Scholar] [CrossRef]
- Goldberg, S.E.; Whittamore, K.H.; Harwood, R.H.; Bradshaw, L.E.; Gladman, J.R.F.; Jones, R.G.; Medical Crises in Older People Study Group. The prevalence of mental health problems among older adults admitted as an emergency to a general hospital. Age Ageing 2011, 41, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Turana, Y.; Tengkawan, J.; Chia, Y.C.; Shin, J.; Chen, C.; Park, S.; Tsoi, K.; Buranakitjaroen, P.; Soenarta, A.A.; Siddique, S.; et al. Mental health problems and hypertension in the elderly: Review from the HOPE Asia Network. J. Clin. Hypertens. 2020, 23, 504–512. [Google Scholar] [CrossRef]
- Reynolds, C.F.; Jeste, D.V.; Sachdev, P.S.; Blazer, D.G. Mental health care for older adults: Recent advances and new directions in clinical practice and research. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2022, 21, 336–363. [Google Scholar] [CrossRef]
- Ruiz-Comellas, A.; Valmaña, G.S.; Peña, J.M.; Poch, P.R.; Carrera, A.S.; Pujol, I.C.; Baena, I.G.; Solà, À.C.; Vila, C.S.; Gamisans, M.F.; et al. Physical activity, emotional state and socialization in the elderly: Study protocol for a clinical multicentre randomized trial. J. Int. Med. Res. 2021, 49, 3000605211016735. [Google Scholar] [CrossRef]
- Lee, S.H.; Lee, H.; Yu, S. Effectiveness of Social Support for Community-Dwelling Elderly with Depression: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 1598. [Google Scholar] [CrossRef]
- Steptoe, A.; Deaton, A.; A Stone, A. Subjective wellbeing, health, and ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef]
- US Census Bureau. Census.gov|U.S. Census Bureau Homepage. Available online: https://www.census.gov/ (accessed on 9 September 2024).
- County of Greenville. County of Greenville Budget Document; County of Greenville: Greenville, SC, USA, 2022; pp. 181–187. Available online: https://www.greenvillecounty.org/managementandbudget/pdf/2022/Appendix.pdf (accessed on 7 August 2024).
- Institute for Health Metrics and Evaluation. US County Profile: Greenville County, South Carolina; Institute for Health Metrics and Evaluation: Washington, DC, USA, 2016; Available online: https://www.healthdata.org/sites/default/files/files/county_profiles/US/2015/County_Report_Greenville_County_South_Carolina.pdf (accessed on 7 August 2024).
- Chapter 1: Models and Frameworks|Principles of Community Engagement|ATSDR. Available online: http://medbox.iiab.me/modules/en-cdc/www.atsdr.cdc.gov//communityengagement/pce_models.html (accessed on 7 August 2024).
- Bamuya, C.; Correia, J.C.; Brady, E.M.; Beran, D.; Harrington, D.; Damasceno, A.; Crampin, A.M.; Magaia, A.; Levitt, N.; Davies, M.J.; et al. Use of the socio-ecological model to explore factors that influence the implementation of a diabetes structured education programme (EXTEND project) inLilongwe, Malawi and Maputo, Mozambique: A qualitative study. BMC Public Health 2021, 21, 1355. [Google Scholar] [CrossRef]
- Tholen, R.; Wouters, E.; Ponnet, K.; De Bruyn, S.; Van Hal, G. A Social Ecological Approach to Hazardous Alcohol Use among Flemish Higher Education Students. Int. J. Environ. Res. Public Health 2020, 17, 8288. [Google Scholar] [CrossRef] [PubMed]
- National Poll on Healthy Aging. Survey. Available online: https://www.healthyagingpoll.org/reports-more/data (accessed on 7 August 2024).
- Kang, H.; Ahn, J.-W. Model Setting and Interpretation of Results in Research Using Structural Equation Modeling: A Checklist with Guiding Questions for Reporting. Asian Nurs. Res. (Korean Soc. Nurs. Sci.) 2021, 15, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Rigdon, E.E. Structural equations modeling. In Marcoulides; George, Ed.; Modern Methods for Business Research, Lawrence-Erlbaum Associates: Mahwah, NJ, USA, 1998; pp. 251–294. [Google Scholar]
- Freeze, R.; Raschke, R.L. An Assessment of Formative and Reflective Constructs in IS Research. In Proceedings of the ECIS 2007, St. Gallen, Switzerland, 7–9 June 2007; p. 171. [Google Scholar]
- Golder, J.; Jerge, M.; Sundstrom, B.; Dziobak, M.; Hart, L.B. Factors influencing CDC- recommended preventative behaviors through the COVID-19 pandemic in college students. J. Am. Coll. Health 2024, 72, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, A.K.; Mallawaarachchi, I.; Alvarado, L.A. Analysis of small sample size studies using nonparametric bootstrap test with pooled resampling method. Stat. Med. 2017, 36, 2187–2205. [Google Scholar] [CrossRef]
- Memon, A.H.; Rahman, I.A. SEM-PLS analysis of inhibiting factors of cost performance for large construction projects in Malaysia: Perspective of clients and consultants. Sci. World J. 2014, 2014, 165158. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.; Danks, N.P.; Ray, S. Partial Least Squares Structural Equation Modeling (PLS-SEM) Using R: A Workbook; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Ringle, C.M.; Wende, S.; Becker, J. SmartPLS; SmartPLS GmbH: Boenningstedt, Germany, 2015. [Google Scholar]
- Jeste, D.V.; Depp, C.A.; Vahia, I.V. Successful cognitive and emotional aging. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2010, 9, 78–84. [Google Scholar] [CrossRef]
- Zenebe, Y.; Akele, B.; W/Selassie, M.; Necho, M. Prevalence and determinants of depression among old age: A systematic review and meta-analysis. Ann. Gen. Psychiatry 2021, 20, 55. [Google Scholar] [CrossRef]
- El Ibrahimi, S.; Xiao, Y.; Bergeron, C.D.; Beckford, N.Y.; Virgen, E.M.; Smith, M.L. Suicide Distribution and Trends Among Male Older Adults in the U.S., 1999–2018. Am. J. Prev. Med. 2021, 60, 802–811. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhen, Z. Community Participation and Subjective Well-Being of Older Adults: The Roles of Sense of Community and Neuroticism. Int. J. Environ. Res. Public Health 2022, 19, 3261. [Google Scholar] [CrossRef] [PubMed]
- NCOA, Explore Mental Health Programs for Older Adults. Available online: https://www.ncoa.org/article/advancing-behavioral-health-programs-for-older-adults/ (accessed on 19 July 2024).
- Beishon, L.; Hickey, B.; Desai, B.; Chithiramohan, T.; Evley, R.; Subramaniam, H.; Maniatopoulos, G.; Rajkumar, A.P.; Dening, T.; Mukateova-Ladinska, E.; et al. Integrated Physical-Mental Healthcare Services in Specialist Settings to Improve Outcomes for Older People Living With Mental Health Diagnoses: A Systematic Review. Int. J. Geriatr. Psychiatry 2024, 39, e6146. [Google Scholar] [CrossRef] [PubMed]
- Horgan, S.; Prorok, J.; Ellis, K.; Mullaly, L.; Cassidy, K.-L.; Seitz, D.; Checkland, C. Optimizing Older Adult Mental Health in Support of Healthy Ageing: A Pluralistic Framework to Inform Transformative Change across Community and Healthcare Domains. Int. J. Environ. Res. Public Health 2024, 21, 664. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Model | Definition |
|---|---|
| Individual | The first level identifies historical biological and personal factors that increase the likelihood of becoming a victim or perpetrator of violence. Some of these factors are age, education, income, substance use, or a history of abuse. Prevention strategies at this level promote attitudes, beliefs, and behaviors that prevent violence. Specific approaches may include conflict resolution and life skills training, social–emotional learning, and safe dating and healthy relationship skills programs. |
| Relationship | The second level examines close relationships that may increase the risk of experiencing violence as a victim or perpetrator. A person’s closest social circle—peers, partners, and family members—influences their behavior and contributes to their experience. Prevention strategies at this level may include parenting or family-focused prevention programs and mentoring and peer programs designed to strengthen parent–child communication and promote positive peer norms, problem-solving skills, and healthy relationships. |
| Community | The third level explores the settings, such as schools, workplaces, and neighborhoods, in which social relationships occur and seeks to identify the characteristics of these settings that are associated with becoming victims or perpetrators of violence. Prevention strategies at this level focus on improving the physical and social environment in these settings (e.g., by creating safe places where people live, learn, work, and play) and by addressing other conditions that give rise to violence in communities (e.g., neighborhood poverty, residential segregation, instability, and a high density of alcohol outlets). |
| Society | The fourth level looks at the broad societal factors that help create a climate in which violence is encouraged or inhibited. These factors include social and cultural norms that support violence as an acceptable way to resolve conflicts. Other large societal factors include the health, economic, educational, and social policies that help to maintain economic or social inequalities between groups in society. Prevention strategies at this level include efforts to promote societal norms that protect against violence as well as efforts to strengthen household financial security, education, and employment opportunities and other policies that affect the structural determinants of health. |
| Construct | Manifest Variable | Median Score (n = 27) |
|---|---|---|
| Healthy Aging | AG1 | 2.0 |
| AG2 | 2.0 | |
| Individual | IN1 | 1.0 |
| IN2 | 1.0 | |
| Relationship | RL1 | 1.0 |
| RL2 | 1.0 | |
| RL3 | 1.0 | |
| RL4 | 1.0 | |
| RL5 | 2.0 | |
| Community | CO1 | 2.0 |
| CO2 | 1.0 | |
| CO3 | 2.0 | |
| CO4 | 2.0 | |
| CO5 | 1.0 | |
| CO6 | 1.0 | |
| CO7 | 2.0 | |
| Society | SO1 | 2.0 |
| Perceived Mental Health | MH1 | 2.0 |
| MH2 | 2.0 |
| Community | Relationship | Society | |
|---|---|---|---|
| Community | 0.647 | ||
| Relationship | 0.699 | 0.626 | |
| Society | −0.270 | −0.267 | 1.000 |
| Community | Relationship | Society | |
|---|---|---|---|
| Community | |||
| Relationship | 1.032 | ||
| Society | 0.392 | 0.292 |
| Pathway | Beta | T-Statistic | p-Value |
|---|---|---|---|
| Aging → Individual | 0.555 | 1.753 | 0.046 |
| Aging → Relationship | 0.357 | 2.334 | 0.005 |
| Aging → Community | 0.517 | 3.494 | 0.001 |
| Aging → Society | −0.341 | 1.879 | 0.072 |
| Individual → Perceived Mental Health | 0.267 | 0.891 | 0.321 |
| Relationship → Perceived Mental Health | 0.255 | 1.546 | 0.048 |
| Community → Perceived Mental Health | 0.401 | 0.924 | 0.269 |
| Society → Perceived Mental Health | 0.070 | 0.450 | 0.632 |
| Pathway | Beta | Standard Deviation | T-Statistic | p-Value |
|---|---|---|---|---|
| Aging → Individual Mental Health | 0.091 | 0.129 | 0.709 | 0.479 |
| Aging → Relationship → Mental Health | 0.207 | 0.163 | 1.273 | 0.203 |
| Aging → Community → Mental Health | 0.148 | 0.173 | 0.856 | 0.392 |
| Aging → Society → Mental Health | 0.024 | 0.062 | 0.385 | 0.700 |
| Aging → Mental Health | 0.423 | 0.170 | 2.494 | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Golder, J.; Lagerberg, E.; Flanagan, W.; Blouin, J.; Horn, C.; Avanzato, S.; Scagliarini, R.; Stoner, A.M. Factors Influencing Mental Health Outcomes Amongst Senescent County Residents. Int. J. Environ. Res. Public Health 2025, 22, 451. https://doi.org/10.3390/ijerph22030451
Golder J, Lagerberg E, Flanagan W, Blouin J, Horn C, Avanzato S, Scagliarini R, Stoner AM. Factors Influencing Mental Health Outcomes Amongst Senescent County Residents. International Journal of Environmental Research and Public Health. 2025; 22(3):451. https://doi.org/10.3390/ijerph22030451
Chicago/Turabian StyleGolder, Jack, Evan Lagerberg, William Flanagan, Jennifer Blouin, Corey Horn, Sabrina Avanzato, Ryan Scagliarini, and Alexis M. Stoner. 2025. "Factors Influencing Mental Health Outcomes Amongst Senescent County Residents" International Journal of Environmental Research and Public Health 22, no. 3: 451. https://doi.org/10.3390/ijerph22030451
APA StyleGolder, J., Lagerberg, E., Flanagan, W., Blouin, J., Horn, C., Avanzato, S., Scagliarini, R., & Stoner, A. M. (2025). Factors Influencing Mental Health Outcomes Amongst Senescent County Residents. International Journal of Environmental Research and Public Health, 22(3), 451. https://doi.org/10.3390/ijerph22030451