
An Evaluation of Dental Caries Status in Children with Oral Clefts: A Cross-Sectional Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Clinical Examination
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grewcock, R.E.; Innes, N.P.T.; Mossey, P.A.; Robertson, M.D. Caries in children with and without orofacial clefting: A systematic review and meta-analysis. Oral Dis. 2022, 28, 1400–1411. [Google Scholar] [CrossRef]
- McKinney, C.M.; Chowchuen, B.; Pitiphat, W.; Derouen, T.; Pisek, A.; Godfrey, K. Micronutrients and oral clefts: A case-control study. J. Dent. Res. 2013, 92, 1089–1094. [Google Scholar] [CrossRef]
- Wu, Q.; Li, Z.; Zhang, Y.; Peng, X.; Zhou, X. Dental caries and periodontitis risk factors in cleft lip and palate patients. Front. Pediatr. 2023, 10, 1092809. [Google Scholar] [CrossRef]
- Das Neves, L.T.; de Carvalho, I.M.M.; Cobourne, M.T.; Gomide, M.R. Dental anomalies in non-syndromic orofacial clefts: A clinical approach. Oral Dis. 2022, 28, 1351–1368. [Google Scholar] [CrossRef]
- Durhan, M.A.; Topcuoglu, N.; Kulekci, G.; Ozgentas, E.; Tanboga, I. Microbial profile and dental caries in cleft lip and palate babies between 0 and 3 years old. Cleft Palate-Craniofacial J. 2018, 56, 349–356. [Google Scholar] [CrossRef]
- Mossey, P.A. Global perspectives in orofacial cleft management and research. Br. Dent. J. 2023, 234, 953–957. [Google Scholar] [CrossRef]
- Freitas, J.A.S.; Neves, L.T.; Almeida, A.L.P.F.; Garib, D.G.; Trindade-Suedam, I.K.; Yaedú, R.Y.F.; Lauris, R.C.M.C.; Soares, S.; Oliveira, T.M.; Pinto, J.H.N. Rehabilitative treatment of cleft lip and palate: Experience of the Hospital for Rehabilitation of Craniofacial Anomalies/USP (HRAC/USP)-Part 1: Overall aspects. J. Appl. Oral Sci. 2012, 20, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 25, 17030. [Google Scholar] [CrossRef] [PubMed]
- Ghazal, T.; Levy, S.M.; Childers, N.K.; Broffitt, B.; Cutter, G.R.; Wiener, H.W.; Kempf, M.C.; Warren, J.; Cavanaugh, J.E. Factors associated with early childhood caries incidence among high caries-risk children. Community Dent. Oral Epidemiol. 2015, 43, 366–374. [Google Scholar] [CrossRef]
- Saikia, A.; Muthu, M.S.; Orenuga, O.O.; Mossey, P.; Ousehal, L.; Yan, S.; Campodonico, M.; England, R.; Taylor, S.; Sheeran, P. Systematic Review of Clinical Practice Guidelines for Oral Health in Children with Cleft Lip and Palate. Cleft Palate-Craniofacial J. 2022, 59, 800–814. [Google Scholar] [CrossRef] [PubMed]
- King, N.M.; Wong, W.L.; Wong, H.M. Caries experience of chinese children with cleft lip and palate. Cleft Palate-Craniofacial J. 2013, 50, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Abirami, S.; Panchanadikar, N.T.; Muthu, M.S.; Swaminathan, K.; Vignesh, K.C.; Agarwal, A.; Kirubakaran, R. Dental Caries Experience among Children and Adolescents with Cleft Lip and/or Palate: An Umbrella Review. Int. J. Clin. Pediatr. Dent. 2022, 15, S261–S268. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, G.S.; Palaska, P.K.; Herzog, G. Caries prevalence in non-syndromic patients with cleft lip and/or palate: A meta-analysis. Caries Res. 2013, 47, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Worth, V.; Perry, R.; Ireland, T.; Wills, A.K.; Sandy, J.; Ness, A. Are people with an orofacial cleft at a higher risk of dental caries? A systematic review and meta-analysis. Br. Dent. J. 2017, 223, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Lucas, V.S.; Gupta, R.; Ololade, O.; Gelbier, M.; Roberts, G.J. Dental health indices and caries associated microflora in children with unilateral cleft lip and palate. Cleft Palate-Craniofacial J. 2000, 37, 447–452. [Google Scholar] [CrossRef]
- Howe, B.J.; Cooper, M.E.; Wehby, G.L.; Resick, J.M.; Nidey, N.L.; Valencia-Ramirez, L.C.; Lopez-Palacio, A.M.; Rivera, D.; Vieira, A.R.; Weinberg, S.M.; et al. Dental Decay Phenotype in nonsyndromic Orofacial Clefting. J. Dent. Res. 2017, 96, 1106–1114. [Google Scholar] [CrossRef]
- Tannure, P.N.; Costa, M.d.C.; Küchler, E.C.; Romanos, H.F.; Granjeiro, J.M.; Vieira, A.R. Caries experience in individuals with cleft lip and palate. Pediatr. Dent. 2012, 34, 127–131. [Google Scholar]
- Paul, T.; Brandt, R.S. Oral and dental health status of children with cleft lip and/or palate. Cleft Palate-Craniofacial J. 1998, 35, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Chapple, J.R.; Nunn, J.H. The oral health of children with clefts of the lip palate, or both. Cleft Palate-Craniofacial J. 2001, 38, 525–528. [Google Scholar] [CrossRef]
- Dahllof, G.; Ussisso-Joandi, R.; Ideberg, M.; Modeer, T. Caries gingivitis, and dental abnormalities in preschool children with cleft lip and/or palate. Cleft Palate J. 1989, 26, 233–238. [Google Scholar]
- Sundell, A.L.; Nilsson, A.K.; Ullbro, C.; Twetman, S.; Marcusson, A. Caries prevalence and enamel defects in 5- and 10-year-old children with cleft lip and/or palate: A case-control study. Acta Odontol. Scand. 2016, 74, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Sunderji, S.; Acharya, B.; Flaitz, C.; Chiquet, B. Dental Caries Experience in Texan Children with Cleft Lip and Palate. Pediatr. Dent. 2017, 39, 397–402. [Google Scholar] [PubMed]
- Feldens, C.A.; Braga, V.S.; Kramer, P.F.; Vítolo, M.R.; Rodrigues, P.H.; de Barros Coelho, E.M.R.; Chaffee, B.W. Primary Dentition Caries Patterns as Predictors of Permanent Dentition Caries: A Prospective Cohort Study. Caries Res. 2023, 57, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.; Du, Q.; Ge, L.; Wang, J.; Wang, X.; Li, Y.; Song, G.; Zhao, W.; Chen, X.; Jiang, B.; et al. Expert consensus on early childhood caries management. Int. J. Oral Sci. 2022, 14, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Hall-Scullin, E.; Whitehead, H.; Milsom, K.; Tickle, M.; Su, T.L.; Walsh, T. Longitudinal study of caries development from childhood to adolescence. J. Dent. Res. 2017, 96, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Okoye, L.O.; Onah, I.I.; Ekwueme, O.C.; Agu, K.A. Pattern of malocclusion and caries experience in unrepaired cleft lip and palate patients in Enugu. Niger. J. Clin. Pract. 2020, 23, 59–64. [Google Scholar] [CrossRef]
- Chopra, A.; Lakhanpal, M.; Rao, N.C.; Gupta, N.; Vashisth, S. Oral health in 4-6 years children with cleft lip/palate: A case control study. N. Am. J. Med. Sci. 2014, 6, 266–269. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Oral Health Surveys—Basic Methods, 4th ed.; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Lin, Y.-T.J.; Tsai, C.L. Caries prevalence and bottle-feeding practices in 2-year-old children with cleft lip, cleft palate, or both in Taiwan. Cleft Palate-Craniofacial J. 1999, 36, 522–526. [Google Scholar] [CrossRef]
- Alotaibi, R.N.; Howe, B.J.; Moreno Uribe, L.M.; Ramirez, C.V.; Restrepo, C.; Deleyiannis, F.W.B.; Padilla, C.; Orioli, I.M.; Buxó, C.J.; Hecht, J.T.; et al. Multivariate GWAS of Structural Dental Anomalies and Dental Caries in a Multi-Ethnic Cohort. Front. Dent. Med. 2021, 2, 771116. [Google Scholar] [CrossRef]
- Kirchberg, A.; Makuch, A.; Hemprich, A.; Hirsch, C. Dental caries in the primary dentition of german children with cleft lip, alveolus, and palate. Cleft Palate-Craniofacial J. 2014, 51, 308–313. [Google Scholar] [CrossRef]
- Britton, K.F.; Welbury, R.R. Dental caries prevalence in children with cleft lip/palate aged between 6 months and 6 years in the West of Scotland. Eur. Arch. Paediatr. Dent. 2010, 11, 236–241. [Google Scholar] [CrossRef]
- Bokhout, B.; Hofman, F.X.; van Limbeek, J.; Kramer, G.J.; Prahl-Andersen, B. Incidence of dental caries in the primary dentition in children with a cleft lip and/or palate. Caries Res. 1997, 31, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, D.C.; Dixon, M. Dental caries of primary incisors in children with cleft lip and palate. Cleft Palate J. 1984, 21, 104–109. [Google Scholar]
- Chaudhari, P.K.; Kharbanda, O.P.; Chaudhry, R.; Pandey, R.M.; Chauhan, S.; Bansal, K.; Sokhi, R.K. Factors Affecting High Caries Risk in Children With and Without Cleft Lip and/or Palate: A Cross-Sectional Study. Cleft Palate-Craniofacial J. 2021, 58, 1150–1159. [Google Scholar] [CrossRef] [PubMed]
- Kirthiga, M.; Muthu, M.S.; Ankita, S.; Kirubakaran, R. Risk factors for early childhood caries: A systematic review and meta-analysis of case control and cohort studies. Pediatr. Dent. 2019, 41, 95–106. [Google Scholar]
- Bokhout, B.; van Loveren, C.; Hofman, F.X.; Buijs, J.F.; van Limbeek, J.; Prahl-Andersen, B. Prevalence of Streptococcus mutans and lactobacilli in 18-month-old children with cleft lip and/or palate. Cleft Palate-Craniofacial J. 1996, 33, 424–428. [Google Scholar] [CrossRef]
- Sun, H.B.; Zhang, W.; Zhou, X.B. Risk Factors associated with Early Childhood Caries. Chin. J. Dent. Res. 2017, 20, 97–104. [Google Scholar] [CrossRef]
- Rodrigues, R.; Fernandes, M.H.; Bessa Monteiro, A.; Furfuro, R.; Carvalho Silva, C.; Vardasca, R.; Mendes, J.; Manso, M.C. Are there any solutions for improving the cleft area hygiene in patients with cleft lip and palate? A systematic review. Int. J. Dent. Hyg. 2019, 17, 130–141. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Groups (Months) | Male | Female | Total Number (%) |
|---|---|---|---|
| G1 (7–12 months) | 15 | 15 | 30 (10%) |
| G2 (13–18 months) | 15 | 15 | 30 (10%) |
| G3 (19–24 months) | 15 | 15 | 30 (10%) |
| G4 (25–30 months) | 15 | 15 | 30 (10%) |
| G5 (31–36 months) | 15 | 15 | 30 (10%) |
| G6 (37–42 months) | 15 | 15 | 30 (10%) |
| G7 (43–48 months) | 15 | 15 | 30 (10%) |
| G8 (49–54 months) | 15 | 15 | 30 (10%) |
| G9 (55–60 months) | 15 | 15 | 30 (10%) |
| G10 (61–66 months) | 15 | 15 | 30 (10%) |
| Total | 150 | 150 | 300 (100%) |
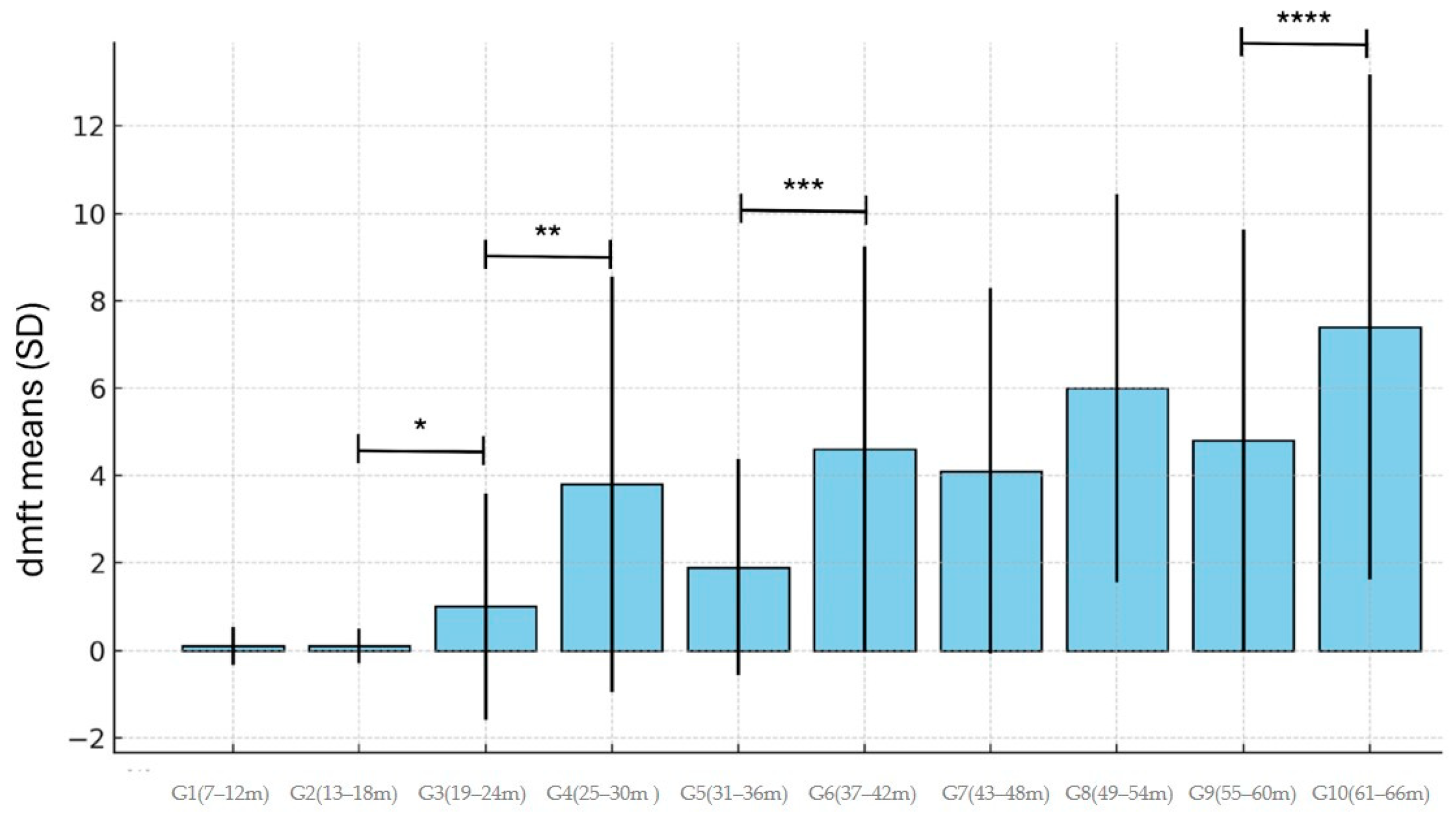
| Age Groups (Months) | Mean dmft ± Standard Deviation (SD) | Mean Number of Present Teeth |
|---|---|---|
| G1 (7–12 months) | 0.1 ± 0.43 | 4.6 |
| G2 (13–18 months) | 0.1 ± 0.40 | 8.1 |
| G3 (19–24 months) | 1.0 ± 2.59 | 14.1 |
| G4 (25–30 months) | 3.8 ± 4.76 | 17.2 |
| G5 (31–36 months) | 1.9 ± 2.48 | 18.7 |
| G6 (37–42 months) | 4.6 ± 4.64 | 19.7 |
| G7 (43–48 months) | 4.1 ± 4.18 | 19.7 |
| G8 (49–54 months) | 6.0 ± 4.45 | 19.6 |
| G9 (55–60 months) | 4.8 ± 4.82 | 19.3 |
| G10 (61–66 months) | 7.4 ± 5.78 | 19.2 |
| Total | 3.4 ± 4.51 | 16.0 |
| Variable | Regression Coefficient | Standard Error | p Value |
|---|---|---|---|
| Intercept | −1.917 | 0.8671 | |
| Age | 0.131 | 0.0132 | <0.001 |
| Child Sex: Male–Female (Reference = F) | −0.388 | −0.857 | 0.392 |
| Type of Cleft (Reference = uCL) | |||
| uCLP vs. uCLA | 1.016 | 0.7512 | 1.352 |
| bCLP vs. uCLA | 0.634 | 0.8139 | 0.437 |
| bCLA vs. uCLA | −1.850 | 1.4745 | 0.210 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neves, L.T.d.; Costa, B.; Lauris, J.R.P.; Ciamponi, A.L.; Gomide, M.R. An Evaluation of Dental Caries Status in Children with Oral Clefts: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2025, 22, 227. https://doi.org/10.3390/ijerph22020227
Neves LTd, Costa B, Lauris JRP, Ciamponi AL, Gomide MR. An Evaluation of Dental Caries Status in Children with Oral Clefts: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2025; 22(2):227. https://doi.org/10.3390/ijerph22020227
Chicago/Turabian StyleNeves, Lucimara Teixeira das, Beatriz Costa, José Roberto Pereira Lauris, Ana Lídia Ciamponi, and Marcia Ribeiro Gomide. 2025. "An Evaluation of Dental Caries Status in Children with Oral Clefts: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 22, no. 2: 227. https://doi.org/10.3390/ijerph22020227
APA StyleNeves, L. T. d., Costa, B., Lauris, J. R. P., Ciamponi, A. L., & Gomide, M. R. (2025). An Evaluation of Dental Caries Status in Children with Oral Clefts: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 22(2), 227. https://doi.org/10.3390/ijerph22020227