
Looking beyond Body Structure and Function: ICF Foci and Who Is Being Assessed in Research about Adolescents and Young Adults with Cerebral Palsy—A Scoping Review
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Identifying the Research Question
2.2. Identifying Relevant Studies
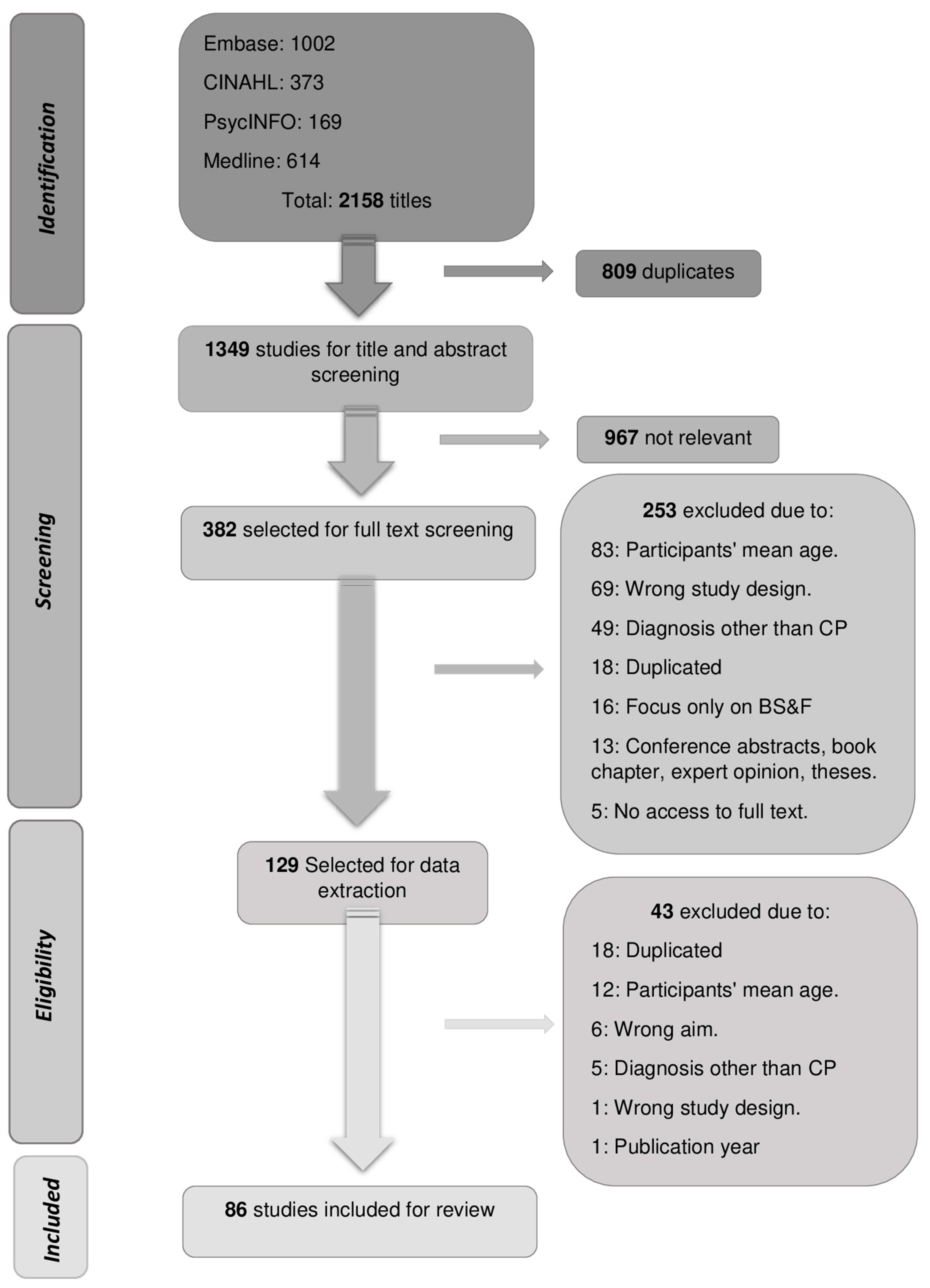
2.3. Study Selection
2.4. Charting the Data
2.5. Collating, Summarizing, and Reporting the Results
3. Results
3.1. Studies Characteristics
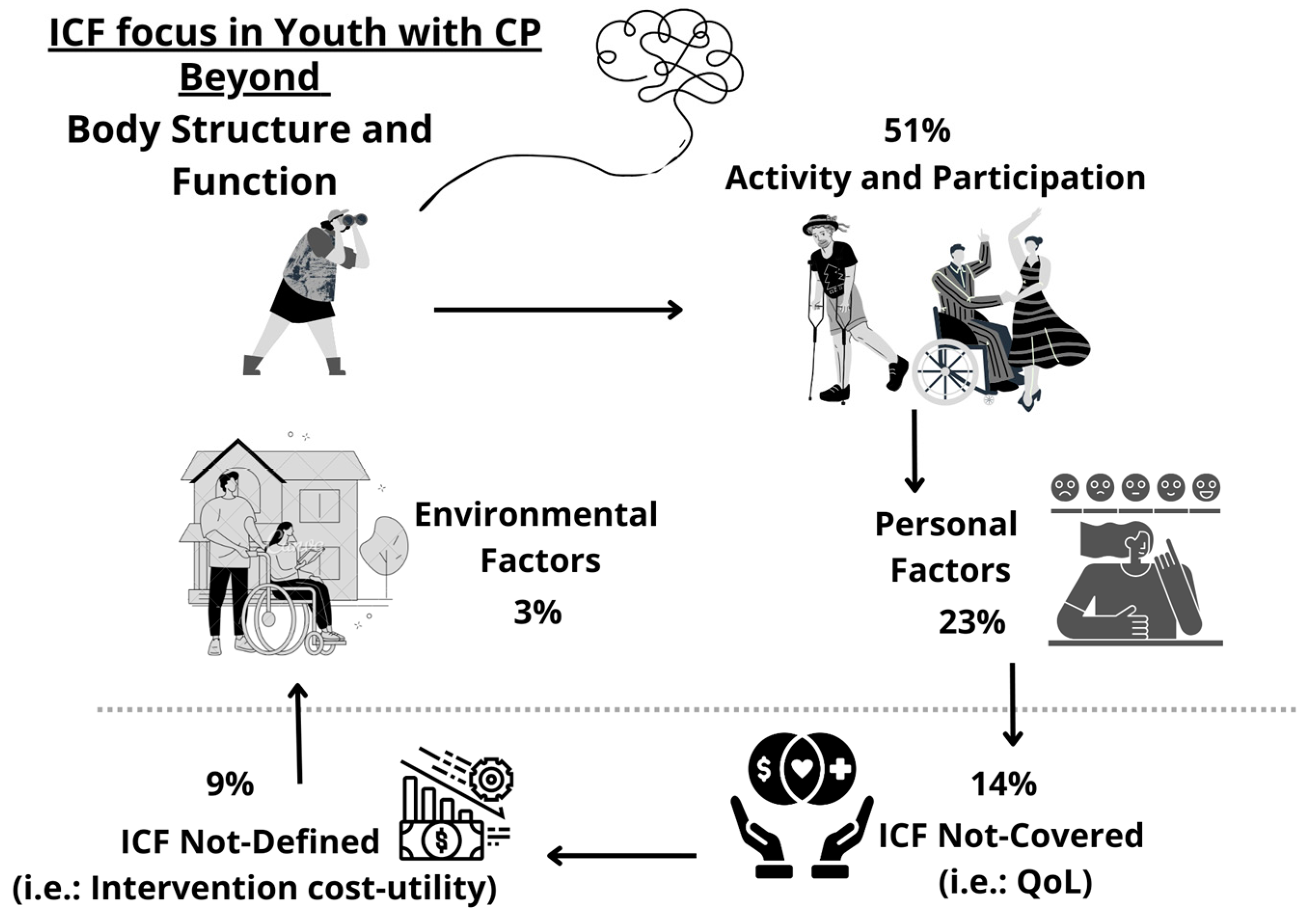
3.2. ICF Foci beyond BSF
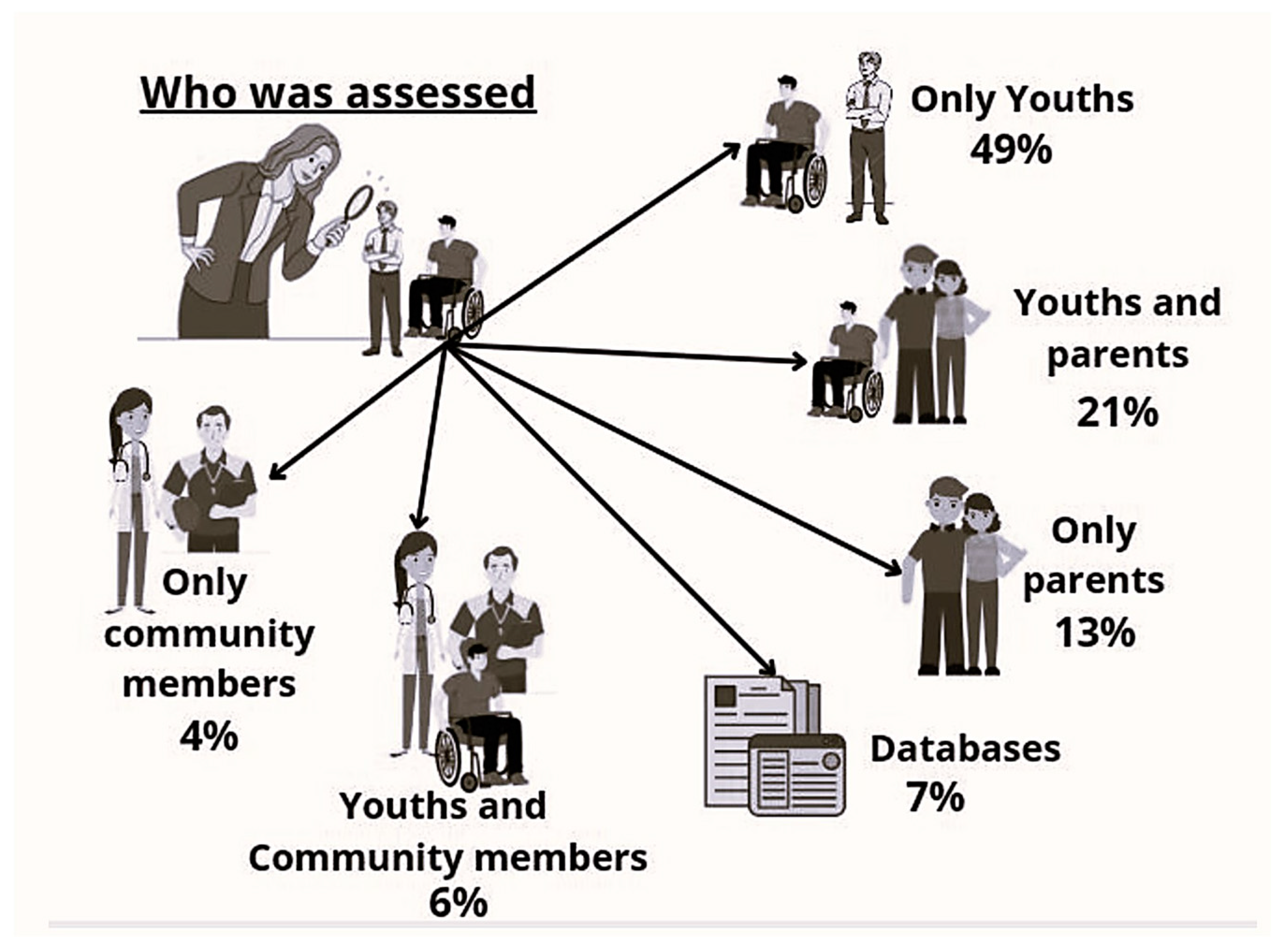
3.3. Who Was Assessed
4. Discussion
5. Conclusions
6. Study Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO—World Health Organization. International Classification of Functioning, Disability and Health: ICF; WHO Library: Geneva, Switzerland, 2001.
- Halfon, N.; Larson, K.; Lu, M.; Tullis, E.; Russ, S. Lifecourse health development: Past, present and future. Matern. Child Health J. 2014, 18, 344–365. [Google Scholar] [CrossRef] [PubMed]
- Vargus-Adams, J.N.; Majnemer, A. International Classification of Functioning, Disability and Health (ICF) as a framework for change: Revolutionizing rehabilitation. J. Child Neurol. 2014, 29, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Rathert, C.; Wyrwich, M.D.; Boren, S.A. Patient-centered care and outcomes: A systematic review of the literature. Med. Care Res. Rev. 2013, 70, 351–379. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, S.J.; Cramm, J.M.; Nieboer, A.P. The importance of patient-centered care and co-creation of care for satisfaction with care and physical and social well-being of patients with multi-morbidity in the primary care setting. BMC Health Serv. Res. 2019, 19, 13. [Google Scholar] [CrossRef] [PubMed]
- Phillips, L.; Soeters, H.; Jokonya, M.; Kyendikuwa, A.; Hatane, L. Person-centred care: Shifting the power dynamic in the delivery of adolescent and youth-friendly health services. J. Int. AIDS Soc. 2023, 26. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. 2007, 49, 8–14. [Google Scholar]
- Gorter, J.W.; Stewart, D.; Woodbury-Smith, M. Youth in transition: Care, health and development. Child Care Health Dev. 2011, 37, 757–763. [Google Scholar] [CrossRef]
- World Health Organization (WHO). The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Colver, A.; Rapp, M.; Eisemann, N.; Ehlinger, V.; Thyen, U.; Dickinson, H.O.; Parkes, J.; Parkinson, K.; Nystrand, M.; Fauconnier, J.; et al. Self-reported quality of life of adolescents with cerebral palsy: A cross-sectional and longitudinal analysis. Lancet 2015, 385, 705–716. [Google Scholar] [CrossRef]
- Bagazgoïtia, N.V.D.; Ehlinger, V.; Duffaut, C.; Fauconnier, J.; Schmidt-Schuchert, S.; Thyen, U.; Himmelmann, K.; Marcelli, M.; Arnaud, C. Quality of Life in Young Adults With Cerebral Palsy: A Longitudinal Analysis of the SPARCLE Study. Front. Neurol. 2021, 12, 733978. [Google Scholar] [CrossRef]
- King, G.; Imms, C.; Stewart, D.; Freeman, M.; Nguyen, T. A transactional framework for pediatric rehabilitation: Shifting the focus to situated contexts, transactional processes, and adaptive developmental outcomes. Disabil. Rehabil. 2018, 40, 1829–1841. [Google Scholar] [CrossRef] [PubMed]
- Di Rezze, B.; Nguyen, T.; Mulvale, G.; Barr, N.G.; Longo, C.J.; Randall, G.E. A scoping review of evaluated interventions addressing developmental transitions for youth with mental health disorders. Child Care Health Dev. 2016, 42, 176–187. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.J.; Di Rezze, B.; Stewart, D.; Rosenbaum, P.L.; Hlyva, O.; Freeman, M.; Nguyen, T.; Gorter, J.W. Life course health development of individuals with neurodevelopmental conditions. Dev. Med. Child Neurol. 2017, 59, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Bagatell, N.; Chan, D.; Rauch, K.K.; Thorpe, D. “Thrust into adulthood”: Transition experiences of young adults with cerebral palsy. Disabil. Health J. 2017, 10, 80–86. [Google Scholar] [CrossRef]
- Freeman, M.; Stewart, D.; Cunningham, C.E.; Gorter, J.W. “If I had been given that information back then”: An interpretive description exploring the information needs of adults with cerebral palsy looking back on their transition to adulthood. Child Care Health Dev. 2018, 44, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.J.; Di Rezze, B.; Stewart, D.; Freeman, M.; Rosenbaum, P.L.; Hlyva, O.; Wolfe, L.; Gorter, J.W. Promoting capacities for future adult roles and healthy living using a lifecourse health development approach. Disabil. Rehabil. 2020, 42, 2002–2011. [Google Scholar] [CrossRef]
- Furtado, M.A.S.; Ayupe, K.M.A.; Christovao, I.S.; Sousa Junior, R.R.; Rosenbaum, P.; Camargos, A.C.R.; Leite, H.R. Physical therapy in children with cerebral palsy in Brazil: A scoping review. Dev. Med. Child Neurol. 2022, 64, 550–560. [Google Scholar] [CrossRef]
- Chagas, P.S.C.; Magalhães, E.D.D.; Sousa Junior, R.R.; Romeros, A.C.S.F.; Palisano, R.J.; Leite, H.R.; Rosenbaum, P. Development of children, adolescents, and young adults with cerebral palsy according to the ICF: A scoping review. Dev. Med. Child Neurol. 2023, 5, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Mcintyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: State of the evidence. Dev. Med. Child Neurol. 2013, 55, 885–910. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Gorter, J.W. The “F-words” in childhood disability: I swear this is how we should think. Child Care Health Dev. 2012, 38, 457–463. [Google Scholar] [CrossRef]
- Arksey, H.; O’malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Wildridge, V.; Bell, L. How CLIP became ECLIPSE: A mnemonic to assist in searching for health policy/management information. Health Inf. Libr. J. 2002, 19, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software. Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org (accessed on 14 May 2024).
- Palisano, R.; Rosenbaum, P.; Bartlett, D.; Livingston, M. GMFCS—E&R Gross Motor Function Classification System Expanded and Revised. 2007. Available online: https://www.canchild.ca/system/tenon/assets/attachments/000/000/058/original/GMFCS-ER_English.pdf (accessed on 14 May 2024).
- Eliasson, A.-C.; Krumlinde-Sundholm, L.; Rösblad, B.; Beckung, E.; Arner, M.; Öhrvall, A.-M.; Rosenbaum, P. The Manual Ability Classification System (MACS) for children with cerebral palsy: Scale development and evidence of validity and reliability. Dev. Med. Child Neurol. 2006, 48, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Hidecker, M.J.C.; Paneth, N.; Rosenbaum, P.L.; Kent, R.D.; Lillie, J.; Eulenberg, J.B.; Chester, K., Jr.; Johnson, B.; Michalsen, L.; Evatt, M.; et al. Developing and validating the Communication Function Classification System for individuals with cerebral palsy. Dev. Med. Child Neurol. 2011, 53, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Sellers, D.; Mandy, A.; Pennington, L.; Hankins, M.; Morris, C. Development and reliability of a system to classify the eating and drinking ability of people with cerebral palsy. Dev. Med. Child Neurol. 2014, 56, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Baranello, G.; Signorini, S.; Tinelli, F.; Guzzetta, A.; Pagliano, E.; Rossi, A.; Foscan, M.; Tramacere, I.; Romeo, D.M.M.; Ricci, D.; et al. Visual Function Classification System for children with cerebral palsy: Development and validation. Dev. Med. Child Neurol. 2020, 62, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Brockow, T.; Ewert, T.; Amman, E.; Kollerits, B.; Chatterji, S.; Üstün, T.B.; Stucki, G. Linking Health-Status Measurements to the International Classification of Functioning, Disability and Health. J. Rehabil. Med. 2002, 34, 205–210. [Google Scholar] [CrossRef]
- Cieza, A.; Fayed, N.; Bickenbach, J.; Prodinger, B. Refinements of the ICF Linking Rules to strengthen their potential for establishing comparability of health information. Disabil. Rehabil. 2019, 41, 574–583. [Google Scholar] [CrossRef]
- APTA. Academy of Pediatric Physical Therapy. Available online: https://pediatricapta.org/includes/fact-sheets/pdfs/FactSheet_ListofPediatricAssessmentToolsCategorizedbyICFModel_2013.pdf (accessed on 14 May 2024).
- Schiariti, V.; Tatla, S.; Sauve, K.; O’Donnell, M. Toolbox of multiple-item measures aligning with the ICF Core Sets for children and youth with cerebral palsy. Eur. J. Paediatr. Neurol. 2017, 21, 252–263. [Google Scholar] [CrossRef]
- RMD-The Rehabilitation Measures Database-Shirley Ryan AbilityLab. 2022. Available online: https://www.sralab.org/rehabilitation-measures (accessed on 14 May 2024).
- WHO-World Health Organization. WHO-ICF Browser. Available online: http://apps.who.int/classifications/icfbrowser/ (accessed on 14 May 2024).
- Liljenquist, K.; O’Neil, M.E.; Bjornson, K.F. Utilization of Physical Therapy Services During Transition for Young People With Cerebral Palsy: A Call for Improved Care Into Adulthood. Phys. Ther. 2018, 98, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Slaman, J.; Van Den Berg-Emons, H.; van Meeteren, J.; Twisk, J.; van Markus, F.; Stam, H.; van der Slot, W.; Roebroeck, M. A lifestyle intervention improves fatigue, mental health and social support among adolescents and young adults with cerebral palsy: Focus on mediating effects. Clin. Rehabil. 2015, 29, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Smits, D.-W.; van Gorp, M.; van Wely, L.; Verheijden, J.; Voorman, J.; Wintels, S.; van der Cruijsen, J.; Ketelaar, M.; Dallmeijer, A.; Roebroeck, M.; et al. Participation in Social Roles of Adolescents With Cerebral Palsy: Exploring Accomplishment and Satisfaction. Arch. Rehabil. Res. Clin. Transl. 2019, 1, 100021. [Google Scholar] [CrossRef] [PubMed]
- van Gorp, M.; Roebroeck, M.E.; van Eck, M.; Voorman, J.M.; Twisk, J.W.R.; Dallmeijer, A.J.; van Wely, L. Childhood factors predict participation of young adults with cerebral palsy in domestic life and interpersonal relationships: A prospective cohort study. Disabil. Rehabil. 2020, 42, 3162–3171. [Google Scholar] [CrossRef] [PubMed]
- Power, R.; Galea, C.; Muhit, M.; Heanoy, E.; Karim, T.; Badawi, N.; Khandaker, G. What predicts the proxy-reported health-related quality of life of adolescents with cerebral palsy in Bangladesh? BMC Public Health 2020, 20, 18. [Google Scholar] [CrossRef] [PubMed]
- Pagliano, E.; Casalino, T.; Mazzanti, S.; Bianchi, E.; Fazzi, E.; Picciolini, O.; Frigerio, A.; Rossi, A.; Gallino, F.; Villani, A.; et al. Being adults with cerebral palsy: Results of a multicenter Italian study on quality of life and participation. Neurol. Sci. 2021, 42, 4543–4550. [Google Scholar] [CrossRef] [PubMed]
- Blackman, J.A.; Conaway, M.R. Adolescents with cerebral palsy: Transitioning to adult health care services. Clin. Pediatr. 2014, 53, 356–363. [Google Scholar] [CrossRef]
- Chikwanha, T.M.; Chidhakwa, S.; Dangarembizi, N. Occupational therapy needs of adolescents and young adults with cerebral palsy in Zimbabwe: Caregivers’ perspectives. Cent. Afr. J. Med. 2015, 61, 38–44. [Google Scholar] [PubMed]
- Guyard, A.; Michelsen, S.I.; Arnaud, C.; Fauconnier, J. Family adaptation to cerebral palsy in adolescents: A European multicenter study. Res. Dev. Disabil. 2017, 61, 138–150. [Google Scholar] [CrossRef]
- Capati, V.; Covert, S.Y.; Paleg, G. Stander use for an adolescent with cerebral palsy at GMFCS level V with hip and knee contractures. Assist. Technol. 2019, 32, 335–341. [Google Scholar] [CrossRef]
- Kenyon, L.K.; Farris, J.; Brockway, K.; Hannum, N.; Proctor, K. Promoting Self-exploration and Function Through an Individualized Power Mobility Training Program. Pediatr. Phys. Ther. 2015, 27, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Lennon, N.; Church, C.; Shrader, M.W.; Robinson, W.; Henley, J.; Salazar-Torres, J.d.J.; Niiler, T.; Miller, F. Mobility and gait in adults with cerebral palsy: Evaluating change from adolescence. Gait Posture 2021, 90, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Kusumoto, Y.; Takaki, K.; Matsuda, T.; Nitta, O. Relevant factors of self-care in children and adolescents with spastic cerebral palsy. PLoS ONE 2021, 16, e0254899. [Google Scholar] [CrossRef] [PubMed]
- Teixeira-Machado, L.; Azevedo-Santos, I.; DeSantana, J.M. Dance Improves Functionality and Psychosocial Adjustment in Cerebral Palsy. Am. J. Phys. Med. Rehabil. 2017, 96, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Bell, B.G.; Shah, S.; Coulson, N.; McLaughlin, J.; Logan, P.; Luke, R.; Avery, A.J. The impact of ageing on adults with cerebral palsy: The results of a national online survey. BJGP Open 2023, 7, BJGPO.2023.0028. [Google Scholar] [CrossRef] [PubMed]
- Abid, M.; Cherni, Y.; Batcho, C.S.; Traverse, E.; Lavoie, M.D.; Mercier, C. Facilitators and barriers to participation in physical activities in children and adolescents living with cerebral palsy: A scoping review. Disabil. Rehabil. 2023, 45, 4322–4337. [Google Scholar] [CrossRef] [PubMed]
- Sienko, S. Understanding the factors that impact the participation in physical activity and recreation in young adults with cerebral palsy (CP). Disabil. Health J. 2019, 12, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Aviram, R.; Khvorostianov, N.; Harries, N.; Bar-Haim, S. Perceived barriers and facilitators for increasing the physical activity of adolescents and young adults with cerebral palsy: A focus group study. Disabil. Rehabil. 2022, 44, 6649–6659. [Google Scholar] [CrossRef]
- Michelsen, S.I.; Flachs, E.M.; Damsgaard, M.T.; Parkes, J.; Parkinson, K.; Rapp, M.; Arnaud, C.; Nystrand, M.; Colver, A.; Fauconnier, J.; et al. European study of frequency of participation of adolescents with and without cerebral palsy. Eur. J. Paediatr. Neurol. 2014, 18, 282–294. [Google Scholar] [CrossRef]
- van Gorp, M.; Van Wely, L.; Dallmeijer, A.J.; de Groot, V.; Ketelaar, M.; Roebroeck, M.E. Long-term course of difficulty in participation of individuals with cerebral palsy aged 16 to 34 years: A prospective cohort study. Dev. Med. Child Neurol. 2019, 61, 194–203. [Google Scholar] [CrossRef]
- Majnemer, A.; Shikako-Thomas, K.; Schmitz, N.; Shevell, M.; Lach, L. Stability of leisure participation from school-age to adolescence in individuals with cerebral palsy. Res. Dev. Disabil. 2015, 47, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Schwellnus, H.; King, G.; Baldwin, P.; Keenan, S.; Hartman, L.R. A Solution-Focused Coaching Intervention with Children and Youth with Cerebral Palsy to Achieve Participation-Oriented Goals. Phys. Occup. Ther. Pediatr. 2020, 40, 423–440. [Google Scholar] [CrossRef]
- Dang, V.M.; Colver, A.; Dickinson, H.O.; Marcelli, M.; Michelsen, S.I.; Parkes, J.; Parkinson, K.; Rapp, M.; Arnaud, C.; Nystrand, M.; et al. Predictors of participation of adolescents with cerebral palsy: A European multi-centre longitudinal study. Res. Dev. Disabil. 2015, 36, 551–564. [Google Scholar] [CrossRef]
- Carroll, E.M. Health Care Transition Experiences of Young Adults With Cerebral Palsy. J. Pediatr. Nurs. 2015, 30, e157–e164. [Google Scholar] [CrossRef] [PubMed]
- Normann, G.; Arntz Boisen, K.; Uldall, P.; Brødsgaard, A. Navigating being a young adult with cerebral palsy: A qualitative study. Int. J. Adolesc. Med. Health 2020, 34, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Dehghanizadeh, M.; Khalafbeigi, M.; Akbarfahimi, M.; Yazdani, F.; Zareiyan, A. Exploring the contributing factors that influence the volition of adolescents with cerebral palsy: A directed content analysis. Scand. J. Occup. Ther. 2021, 28, 553–563. [Google Scholar] [CrossRef]
- Sienko, S.E. An exploratory study investigating the multidimensional factors impacting the health and well-being of young adults with cerebral palsy. Disabil. Rehabil. 2018, 40, 660–666. [Google Scholar] [CrossRef]
- Wintels, S.C.; Smits, D.; van Wesel, F.; Verheijden, J.; Ketelaar, M.; the PERRIN PiP Study Group. How do adolescents with cerebral palsy participate? Learning from their personal experiences. Health Expect. 2018, 21, 1024–1034. [Google Scholar] [CrossRef]
- Galambos, N.L.; Magill-Evans, J.; Darrah, J. Psychosocial maturity in the transition to adulthood for people with and without motor disabilities. Rehabil. Psychol. 2008, 53, 498. [Google Scholar] [CrossRef]
- Bergqvist, L.; Öhrvall, A.-M.; Himmelmann, K.; Peny-Dahlstrand, M. When I do, I become someone: Experiences of occupational performance in young adults with cerebral palsy. Disabil. Rehabil. 2019, 41, 341–347. [Google Scholar] [CrossRef]
- Schneidert, M.; Hurst, R.; Miller, J.; Üstün, B. The role of environment in the International Classification of Functioning, Disability and Health (ICF). Disabil. Rehabil. 2003, 25, 588–595. [Google Scholar] [CrossRef]
- van der Kemp, J.; Ketelaar, M.; Gorter, J.W. Environmental factors associated with participation and its related concepts among children and youth with cerebral palsy: A rapid review. Disabil. Rehabil. 2022, 44, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.Y.; Cleary, S.L.; Morgan, P.E. Participation experiences of young people with cerebral palsy in key life situations: A qualitative study. Dev. Med. Child Neurol. 2024; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Rapp, M.; Eisemann, N.; Arnaud, C.; Ehlinger, V.; Fauconnier, J.; Marcelli, M.; Michelsen, S.I.; Nystrand, M.; Colver, A.; Thyen, U. Predictors of parent-reported quality of life of adolescents with cerebral palsy: A longitudinal study. Res. Dev. Disabil. 2017, 62, 259–270. [Google Scholar] [CrossRef]
- Sentenac, M.; Rapp, M.; Ehlinger, V.; Colver, A.; Thyen, U.; Arnaud, C. Disparity of child/parent-reported quality of life in cerebral palsy persists into adolescence. Dev. Med. Child Neurol. 2021, 63, 68–74. [Google Scholar] [CrossRef]
- Alriksson-Schmidt, A.; Hägglund, G.; Rodby-Bousquet, E.; Westbom, L. Follow-up of individuals with cerebral palsy through the transition years and description of adult life: The Swedish experience. J. Pediatr. Rehabil. Med. 2014, 7, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, D.N.O.; Löwing, K.; Tedroff, K. Health-related quality of life, pain, and fatigue in young adults with cerebral palsy. Dev. Med. Child Neurol. 2020, 62, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Shrader, M.W.; Church, C.; Lennon, N.; Shields, T.; Salazar-Torres, J.J.; Howard, J.J.; Miller, F. Well-Being of Ambulatory Adults With Cerebral Palsy: Education, Employment, and Physical Function of a Cohort Who Received Specialized Pediatric Care. Front. Neurol. 2021, 12, 732906. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, D.; Gorter, J.W. GMFCS—E&R Self Report Questionnaire: For Young People Aged 12–18 Years. 2011. Available online: https://canchild.ca/system/tenon/assets/attachments/000/000/481/original/GMFCS_Family.pdf (accessed on 14 May 2024).
- King, G.; Hartman, L.R.; McPherson, A.C.; DeFinney, A.; Kehl, B.; Rudzik, A.; Morrison, A. Exploring the after-hours social experiences of youth with disabilities in residential immersive life skills programs: A photo elicitation study. Disabil. Rehabil. 2020, 44, 3104–3112. [Google Scholar] [CrossRef]
- Hanes, J.E.; Hlyva, O.; Rosenbaum, P.; Freeman, M.; Nguyen, T.; Palisano, R.J.; Gorter, J.W. Beyond stereotypes of cerebral palsy: Exploring the lived experiences of young Canadians. Child Care Health Dev. 2019, 45, 613–622. [Google Scholar] [CrossRef]
- Gray, S.H.; Wylie, M.; Christensen, S.; Khan, A.; Williams, D.; Glader, L. Puberty and menarche in young females with cerebral palsy and intellectual disability: A qualitative study of caregivers’ experiences. Dev. Med. Child Neurol. 2021, 63, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Ramstad, K.; Loge, J.H.; Jahnsen, R.; Diseth, T.H. Self-reported mental health in youth with cerebral palsy and associations to recurrent musculoskeletal pain. Disabil. Rehabil. 2015, 37, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Butner, J.; Berg, C.A.; Osborn, P.; Butler, J.M.; Godri, C.; Fortenberry, K.T.; Barach, I.; Le, H.; Wiebe, D.J. Parent–adolescent discrepancies in adolescents’ competence and the balance of adolescent autonomy and adolescent and parent well-being in the context of Type 1 diabetes. Dev. Psychol. 2009, 45, 835–849. [Google Scholar] [CrossRef] [PubMed]
- Cleary, S.L.; Taylor, N.F.; Dodd, K.J.; Shields, N. Barriers to and facilitators of physical activity for children with cerebral palsy in special education. Dev. Med. Child Neurol. 2019, 61, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.; Imms, C.; Kerr, C.; Adair, B. Sustained participation in community-based physical activity by adolescents with cerebral palsy: A qualitative study. Disabil. Rehabil. 2018, 41, 3043–3051. [Google Scholar] [CrossRef]
- Gorter, J.W.; Galuppi, B.E.; Gulko, R.; Wright, M.; Godkin, E. Consensus Planning Toward a Community-Based Approach to Promote Physical Activity in Youth with Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2017, 37, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Verhoef, J.; Bramsen, I.; Miedema, H.; Stam, H.; Roebroeck, M.; Transition and Lifespan Research Group South West Netherlands. Development of work participation in young adults with cerebral palsy: A longitudinal study. J. Rehabil. Med. 2014, 46, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Ben-Pazi, H.; Barzilay, Y.; Shoval, N. Can global positioning systems quantify participation in cerebral palsy? J. Child Neurol. 2014, 29, 823–825. [Google Scholar] [CrossRef]
- Nooijen, C.F.; Slaman, J.; Stam, H.J.; Roebroeck, M.E.; Berg-Emons, R.J.; Learn2Move Research Group. Inactive and sedentary lifestyles amongst ambulatory adolescents and young adults with cerebral palsy. J. Neuroeng. Rehabil. 2014, 11, 49. [Google Scholar] [CrossRef]
- Slaman, J.; van den Berg-Emons, R.; Tan, S.; Russchen, H.; Meeteren, J.; Stam, H.; Roebroeck, M. Cost-utility of a lifestyle intervention in adolescents and young adults with spastic cerebral palsy. J. Rehabil. Med. 2015, 47, 338–345. [Google Scholar] [CrossRef]
- Usuba, K.; Oddson, B.; Gauthier, A.; Young, N.L. Leisure-Time Physical Activity in adults with Cerebral Palsy. Disabil. Health J. 2015, 8, 611–618. [Google Scholar] [CrossRef] [PubMed]
- McDowell, B.C.; Duffy, C.; Parkes, J. Service use and family-centred care in young people with severe cerebral palsy: A population-based, cross-sectional clinical survey. Disabil. Rehabil. 2015, 37, 2324–2329. [Google Scholar] [CrossRef]
- Vles, G.F.; Hendriksen, R.G.; Hendriksen, J.G.; van Raak, E.P.; Soudant, D.; Vles, J.S.; Gavilanes, A.W. Quality of Life of Children with Cerebral Palsy: A Cross-Sectional KIDSCREEN study in the Southern part of the Netherlands. CNS Neurol. Disord. Drug Targets 2015, 14, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Slaman, J.; Roebroeck, M.; Dallmijer, A.; Twisk, J.; Stam, H.; Berg-Emons, R.v.D.; Learn 2 Move Research Group. Can a lifestyle intervention programme improve physical behaviour among adolescents and young adults with spastic cerebral palsy? A randomized controlled trial. Dev. Med. Child Neurol. 2015, 57, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Hynan, A.; Goldbart, J.; Murray, J. A grounded theory of Internet and social media use by young people who use augmentative and alternative communication (AAC). Disabil. Rehabil. 2015, 37, 1559–1575. [Google Scholar] [CrossRef]
- Bantjes, J.; Swartz, L.; Conchar, L.; Derman, W. When they call me cripple: A group of South African adolescents with cerebral palsy attending a special needs school talk about being disabled. Disabil. Soc. 2015, 30, 241–254. [Google Scholar] [CrossRef]
- Bantjes, J.; Swartz, L.; Conchar, L.; Derman, W. Developing programmes to promote participation in sport among adolescents with disabilities: Perceptions expressed by a group of South African adolescents with cerebral palsy. Int. J. Disabil. Dev. Educ. 2015, 62, 288–302. [Google Scholar] [CrossRef]
- Björquist, E.; Nordmark, E.; Hallström, I. Living in transition—Experiences of health and well-being and the needs of adolescents with cerebral palsy. Child Care Health Dev. 2015, 41, 258–265. [Google Scholar] [CrossRef]
- Koldoff, E.A.; Holtzclaw, B.J. Physical Activity Among Adolescents with Cerebral Palsy: An Integrative Review. J. Pediatr. Nurs. 2015, 30, e105–e117. [Google Scholar] [CrossRef]
- Jiang, B.; Walstab, J.; Reid, S.M.; Davis, E.; Reddihough, D. Quality of life in young adults with cerebral palsy. Disabil. Health J. 2016, 9, 673–681. [Google Scholar] [CrossRef]
- Eken, M.M.; Houdijk, H.; Doorenbosch, C.A.M.; Kiezebrink, F.E.M.; Bennekom, C.A.M.v.; Harlaar, J.; Dallmeijer, A.J. Relations between muscle endurance and subjectively reported fatigue, walking capacity, and participation in mildly affected adolescents with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 814–821. [Google Scholar] [CrossRef]
- Conchar, L.; Bantjes, J.; Swartz, L.; Derman, W. Barriers and facilitators to participation in physical activity: The experiences of a group of South African adolescents with cerebral palsy. J. Health Psychol. 2016, 21, 152–163. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.E.; Robb, J.; Shearer, M.C. Transition from paediatric to adult health services in Scotland for young people with cerebral palsy. J. Child Health Care 2016, 20, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Mumford, L.; Chau, T. Application of an access technology delivery protocol to two children with cerebral palsy. Disabil. Rehabil. Assist. Technol. 2016, 11, 166–175. [Google Scholar] [CrossRef]
- Monbaliu, E.; De Cock, P.; Mailleux, L.; Dan, B.; Feys, H. The relationship of dystonia and choreoathetosis with activity, participation and quality of life in children and youth with dyskinetic cerebral palsy. Eur. J. Paediatr. Neurol. 2017, 21, 327–335. [Google Scholar] [CrossRef]
- Frank, A.O.; De Souza, L.H. Problematic clinical features of children and adults with cerebral palsy who use electric powered indoor/outdoor wheelchairs: A cross-sectional study. Assist. Technol. 2017, 29, 68–75. [Google Scholar] [CrossRef]
- Voyer, A.-P.; Tessier, R.; Nadeau, L. Sociometric status and the attribution of intentions in a sample of adolescents with cerebral palsy. Disabil. Rehabil. 2017, 39, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Caron, J.G.; Light, J. Social media experiences of adolescents and young adults with cerebral palsy who use augmentative and alternative communication. Int. J. Speech Lang. Pathol. 2017, 19, 30–42. [Google Scholar] [CrossRef]
- Koldoff, E.A. Parental perspectives on physical activity of adolescents with cerebral palsy: A pilot study. J. Res. Nurs. 2017, 22, 297–310. [Google Scholar] [CrossRef]
- Michalska, A.; Markowska, M.; Śliwiński, Z.; Pogorzelska, J.A. Quality of life in children and young people with tetraplegic cerebral palsy. Med. Stud./Stud. Med. 2018, 34, 112–119. [Google Scholar] [CrossRef]
- King, G.; Schwellnus, H.; Keenan, S.; Chiarello, L.A. Youth Engagement in Pediatric Rehabilitation: Service Providers’ Perceptions in a Real-Time Study of Solution-Focused Coaching for Participation Goals. Phys. Occup. Ther. Pediatr. 2018, 38, 527–547. [Google Scholar] [CrossRef] [PubMed]
- Taherian, S.; Davies, C. Multiple stakeholder perceptions of assistive technology for individuals with cerebral palsy in New Zealand. Disabil. Rehabil. Assist. Technol. 2018, 13, 648–657. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.; Stewart, D.; Cunningham, C.E.; Gorter, J.W. Information needs of young people with cerebral palsy and their families during the transition to adulthood: A scoping review. J. Transit. Med. 2018, 1. [Google Scholar] [CrossRef]
- Burak, M.; Kavlak, E. Investigation of the relationship between quality of life, activity participation and environmental factors in adolescents with cerebral palsy. NeuroRehabilitation 2019, 45, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, D.N.O.; Löwing, K.; Hjalmarsson, E.; Tedroff, K. Exploring social participation in young adults with cerebral palsy. J. Rehabil. Med. 2019, 51, 167–174. [Google Scholar] [CrossRef]
- Power, R.; Muhit, M.; Heanoy, E.; Karim, T.; Badawi, N.; Akhter, R.; Khandaker, G. Health-related quality of life and mental health of adolescents with cerebral palsy in rural Bangladesh. PLoS ONE 2019, 14, e0217675. [Google Scholar] [CrossRef] [PubMed]
- Remijn, L.; van den Engel-Hoek, L.; Satink, T.; de Swart, B.J.M.; Nijhuis-van der Sanden, M.W.G. “Everyone sees you sitting there struggling with your food”: Experiences of adolescents and young adults with cerebral palsy. Disabil. Rehabil. 2019, 41, 1898–1905. [Google Scholar] [CrossRef]
- Lopes, P.B.; Shikako-Thomas, K.; Cardoso, R.; Simões Matsukura, T. Social participation: The perspectives of adolescents with cerebral palsy and their mothers. Int. J. Dev. Disabil. 2019, 67, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Grace, E.; Raghavendra, P.; McMillan, J.M.; Gunson, J.S. Exploring participation experiences of youth who use AAC in social media settings: Impact of an e-mentoring intervention. Augment. Altern. Commun. 2019, 35, 132–141. [Google Scholar] [CrossRef]
- Jalón, E.G.G.; Merrick, H.; Colver, A.; Linden, M. Transition Collaborative Group; Transition Collaborative Group. Did previous involvement in research affect recruitment of young people with cerebral palsy to a longitudinal study of transitional health care? BMJ Open 2020, 10, e035525. [Google Scholar] [CrossRef]
- Schmidt, A.K.; van Gorp, M.; van Wely, L.; Ketelaar, M.; Hilberink, S.R.; Roebroeck, M.E.; Roebroeck, M.E.; Tan, S.S.; van Meeteren, J.; van der Slot, W.; et al. Autonomy in participation in cerebral palsy from childhood to adulthood. Dev. Med. Child Neurol. 2020, 62, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Kwon, K.B.; Choi, Y.; Sung, K.H.; Chung, C.Y.; Lee, K.M.; Kwon, S.-S.; Cho, G.H.; Park, M.S. Correlation between Accelerometer and Questionnaire-Based Assessment of Physical Activity in Patients with Cerebral Palsy. Clin. Orthop. Surg. 2020, 12, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.; Colquitt, G.; Elliot, S.; Emter, M.; Li, L. Using participatory action research to examine barriers and facilitators to physical activity among rural adolescents with cerebral palsy. Disabil. Rehabil. 2020, 42, 3838–3849. [Google Scholar] [CrossRef] [PubMed]
- Tu, A.; Steinbok, P. Long term outcome of Selective Dorsal Rhizotomy for the management of childhood spasticity-functional improvement and complications. Childs Nerv. Syst. 2020, 36, 1985–1994. [Google Scholar] [CrossRef] [PubMed]
- Jahnsen, R.; Ramstad, K.; Myklebust, G.; Elkjaer, S.; Pripp, A.H.; Klevberg, G.L. Independence of young people with cerebral palsy during transition to adulthood: A population-based 3 year follow-up study. J. Transit. Med. 2020, 2, 20190002. [Google Scholar] [CrossRef]
- Power, R.; Wiley, K.; Muhit, M.; Heanoy, E.; Karim, T.; Badawi, N.; Khandaker, G. ‘Flower of the body’: Menstrual experiences and needs of young adolescent women with cerebral palsy in Bangladesh, and their mothers providing menstrual support. BMC Womens Health 2020, 20, 160. [Google Scholar] [CrossRef] [PubMed]
- Towns, M.; Lindsay, S.; Arbour-Nicitopoulos, K.; Mansfield, A.; Wright, F.V. Balance confidence and physical activity participation of independently ambulatory youth with cerebral palsy: An exploration of youths’ and parents’ perspectives. Disabil. Rehabil. 2020, 44, 2305–2316. [Google Scholar] [CrossRef] [PubMed]
- Feitosa, A.M.; Mancini, M.C.; Silvério, A.P.M.; Gordon, A.M.; Brandão, M.B. “Help Me to Improve my Own Priorities!”: A Feasibility Study of an Individualized Intensive Goal Training for Adolescents with Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2021, 41, 601–619. [Google Scholar] [CrossRef]
- Lai, B.; Lee, E.; Kim, Y.; Matthews, C.; Swanson-Kimani, E.; Davis, D.; Vogtle, L.; Rimmer, J.H. Leisure-time physical activity interventions for children and adults with cerebral palsy: A scoping review. Dev. Med. Child Neurol. 2021, 63, 162–171. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1—Articles published in the English language. | 1—Population mean age or age range for cerebral palsy not comprised between 13 and 30 years old. |
| 2—Between January 2014 to December 2021. | 2—Studies published as “online first” and not issued in the journal between 2014–2021. |
| 3—Main focus of interest being Cerebral palsy. | 3—Studies with interventions or assessments focused only on body structures and function. |
| 4—About adolescents and/or young adults (13–30 years old (key transition period)). | 4—Studies focusing on scale validation, translation, or protocols. |
| 5—Evaluating constructs related to the development of health, independence, or participation. | 5—Documents other than scientific papers, such as theses, abstracts, expert opinions, etc. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santana, C.A.S.; Rosenbaum, P.; van der Kemp, J.; de Campos, A.C. Looking beyond Body Structure and Function: ICF Foci and Who Is Being Assessed in Research about Adolescents and Young Adults with Cerebral Palsy—A Scoping Review. Int. J. Environ. Res. Public Health 2024, 21, 670. https://doi.org/10.3390/ijerph21060670
Santana CAS, Rosenbaum P, van der Kemp J, de Campos AC. Looking beyond Body Structure and Function: ICF Foci and Who Is Being Assessed in Research about Adolescents and Young Adults with Cerebral Palsy—A Scoping Review. International Journal of Environmental Research and Public Health. 2024; 21(6):670. https://doi.org/10.3390/ijerph21060670
Chicago/Turabian StyleSantana, Camila Araújo Santos, Peter Rosenbaum, Jet van der Kemp, and Ana Carolina de Campos. 2024. "Looking beyond Body Structure and Function: ICF Foci and Who Is Being Assessed in Research about Adolescents and Young Adults with Cerebral Palsy—A Scoping Review" International Journal of Environmental Research and Public Health 21, no. 6: 670. https://doi.org/10.3390/ijerph21060670
APA StyleSantana, C. A. S., Rosenbaum, P., van der Kemp, J., & de Campos, A. C. (2024). Looking beyond Body Structure and Function: ICF Foci and Who Is Being Assessed in Research about Adolescents and Young Adults with Cerebral Palsy—A Scoping Review. International Journal of Environmental Research and Public Health, 21(6), 670. https://doi.org/10.3390/ijerph21060670