
Low Physical Performance Could Be Associated with Adverse Health Outcomes over Time: Results from a Cohort of Older Adults

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
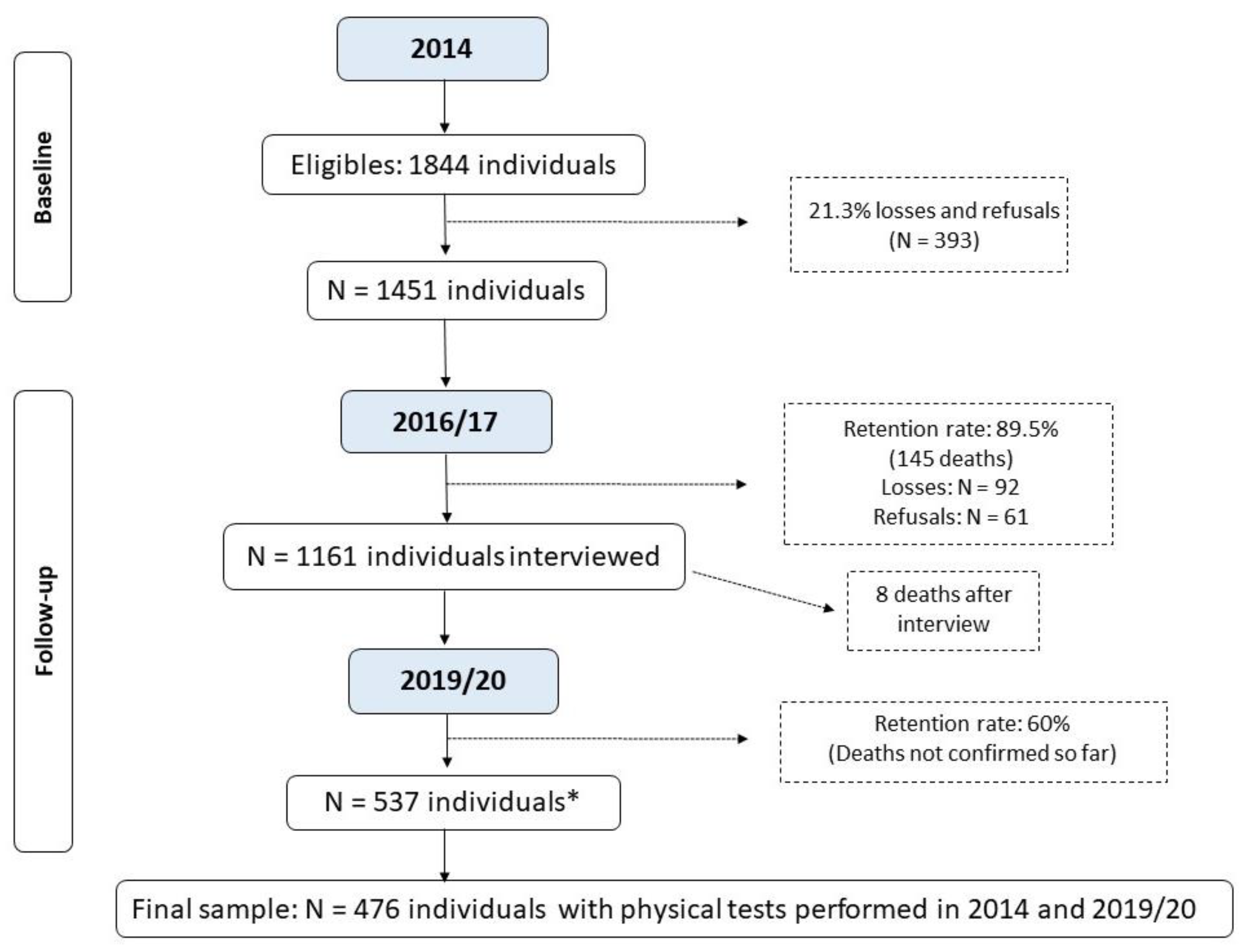
2.1. Study Population
2.2. Physical Performance Assessments
2.3. Outcomes
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pan American Health Organization (PAHO). UN Decade of Healthy Ageing 2020. Available online: https://www.who.int/docs/default-source/decade-of-healthy-ageing/final-decade-proposal/decade-proposal-final-apr2020-en.pdf (accessed on 19 June 2023).
- IBGE. Censo Demográfico 2022—População Por Idade e Sexo; Instituto Brasileiro de Geografia e Estatística: Rio de Janeiro, Brazil, 2023. [Google Scholar]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking Speed: The Functional Vital Sign. J. Aging Phys. Act. 2015, 23, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Santiago, L.M.; Luz, L.L.; Mattos, I.E.; Gobbens, R.J.J.; van Assen, M.A.L.M. Psychometric properties of the Brazilian version of the Tilburg frailty indicator (TFI). Arch. Gerontol. Geriatr. 2013, 57, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Abellan Van Kan, G.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette-Guyonnet, S.; Inzitari, M.; et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Cooper, R.; Shardell, M.; Simonsick, E.M.; Schrack, J.A.; Kuh, D. Age-Related Change in Mobility: Perspectives from Life Course Epidemiology and Geroscience. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1184–1194. [Google Scholar] [CrossRef] [PubMed]
- Figgins, E.; Pieruccini-Faria, F.; Speechley, M.; Montero-Odasso, M. Potentially modifiable risk factors for slow gait in community dwelling older adults: A systematic review. Ageing Res. Rev. 2021, 66, 101253. [Google Scholar] [CrossRef] [PubMed]
- Gomes, D.R.d.P.; Santos, L.P.; Gonzalez, M.C.; Vieira, E.R.; Bielemann, R.M. Changes in Physical Performance among Community-Dwelling Older Adults in Six Years. Int. J. Environ. Res. Public Health 2023, 20, 5579. [Google Scholar] [CrossRef]
- Aartolahti, E.; Lönnroos, E.; Hartikainen, S.; Häkkinen, A. Long-term strength and balance training in prevention of decline in muscle strength and mobility in older adults. Aging Clin. Exp. Res. 2020, 32, 59–66. [Google Scholar] [CrossRef]
- Pacheco, T.B.F.; de Medeiros, C.S.P.; de Oliveira, V.H.B.; Vieira, E.R.; de Cavalcanti, F.A.C. Effectiveness of exergames for improving mobility and balance in older adults: A systematic review and meta-analysis. Syst. Rev. 2020, 9, 163. [Google Scholar] [CrossRef]
- Silva, A.M.; Pereira, D.S.; Torres, J.L.; de Souza, M.G.; de Carvalho, D.G.; Kosour, C.; Viana, J.U.; da Silva, S.L.A. Association Between Physical Functioning and Time Until a New Hospitalization in Community-Dwelling Older Adults: A Prospective Cohort Study. J. Geriatr. Phys. Ther. 2023, 46, 161–167. [Google Scholar] [CrossRef]
- Bortone, I.; Sardone, R.; Lampignano, L.; Castellana, F.; Zupo, R.; Lozupone, M.; Moretti, B.; Giannelli, G.; Panza, F. How gait influences frailty models and health-related outcomes in clinical-based and population-based studies: A systematic review. J. Cachexia Sarcopenia Muscle 2021, 12, 274–297. [Google Scholar] [CrossRef]
- Bergland, A.; Jørgensen, L.; Emaus, N.; Strand, B.H. Mobility as a predictor of all-cause mortality in older men and women: 11.8 year follow-up in the Tromsø study. BMC Health Serv. Res. 2017, 17, 22. [Google Scholar] [CrossRef]
- Shuman, V.; Coyle, P.C.; Perera, S.; Van Swearingen, J.M.; Albert, S.M.; Brach, J.S. Association Between Improved Mobility and Distal Health Outcomes. Magaziner J, organizador. J. Gerontol. Ser. A 2020, 75, 2412–2417. [Google Scholar] [CrossRef]
- Mateo-Abad, M.; Vrotsou, K.; Padilla Ruiz, M.; Montiel-Luque, A.; Saucedo Figueredo, M.d.C.; Machón, M.; Ruiz, F.R.; Vergara, I. Use of health care services according to functional performance in community-dwelling older adults in Spain. An approach using GAMLSS models. PLoS ONE 2022, 17, e0277681. [Google Scholar] [CrossRef]
- Brasil, Ministério da Saúde. Orientações Técnicas para a Implementação de Linha de Cuidado para Atenção Integral à Saúde da Pessoa Idosa no Sistema Único de Saúde—SUS. Brasília, 2018. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/linha_cuidado_atencao_pessoa_idosa.pdf (accessed on 10 February 2024).
- Hoekstra, T.; Rojer, A.G.M.; van Schoor, N.M.; Maier, A.B.; Pijnappels, M. Distinct Trajectories of Individual Physical Performance Measures across 9 Years in 60- to 70-Year-Old Adults. J. Gerontol. Ser. A 2020, 75, 1951–1959. [Google Scholar] [CrossRef] [PubMed]
- Farías-Antúnez, S.; Fassa, A.G. Prevalência e fatores associados à fragilidade em população idosa do Sul do Brasil, 2014. Epidemiol. Serv. Saúde 2019, 28, e2017405. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-Silva, T.G.; Bielemann, R.M.; Gonzalez, M.C.; Menezes, A.M.B. Prevalence of sarcopenia among community-dwelling elderly of a medium-sized South American city: Results of the COMO VAI? study: Sarcopenia prevalence in a South American city. J. Cachexia Sarcopenia Muscle 2016, 7, 136–143. [Google Scholar] [CrossRef] [PubMed]
- IBGE. Censo 2010. In Instituto Brasileiro de Geografia e Estatística. Available online: https://biblioteca.ibge.gov.br/visualizacao/periodicos/93/cd_2010_caracteristicas_populacao_domicilios.pdf (accessed on 6 September 2022).
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Perera, S.; Mody, S.H.; Woodman, R.C.L.; Studenski, S.A. Meaningful Change and Responsiveness in Common Physical Performance Measures in Older Adults: Meaningful change and performance. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Rodrigues, R.A.S.; Teodózio, M.M.; Espinosa, M.M.; Fett, W.C.R.; Melo, C.D.; Fett, C.A. Timed up and go test and self-perceived health in elderly: Population-based study. Rev. Bras. Cineantropom Desempenho Hum. 2018, 20, 247–257. [Google Scholar] [CrossRef]
- Santos, E.C.d.; Couto, B.D.M.; Bastone, A.D.C. Fatores associados à autoavaliação negativa da saúde em idosos cadastrados nas Unidades Básicas de Saúde. ABCS Health Sci. 2018, 43, 47–54. [Google Scholar] [CrossRef][Green Version]
- Liebzeit, D.; King, B.; Bratzke, L. Measurement of function in older adults transitioning from hospital to home: An integrative review. Geriatr. Nurs. 2018, 39, 336–343. [Google Scholar] [CrossRef]
- Ramsey, K.A.; Rojer, A.G.M.; van Garderen, E.; Struik, Y.; Kay, J.E.; Lim, W.K.; Meskers, C.G.; Reijnierse, E.M.; Maier, A.B. The Association of Changes in Physical Performance during Geriatric Inpatient Rehabilitation with Short-Term Hospital Readmission, Institutionalization, and Mortality: RESORT. J. Am. Med. Dir. Assoc. 2022, 23, 1883.e1–1883.e8. [Google Scholar] [CrossRef]
- Alexandre, T.S.; Meira, D.M.; Rico, N.C.; Mizuta, S.K. Accuracy of Timed Up and Go Test for screening risk of falls among community-dwelling elderly. Braz. J. Phys. Ther. 2012, 16, 381–388. [Google Scholar] [CrossRef]
- Asai, T.; Oshima, K.; Fukumoto, Y.; Yonezawa, Y.; Matsuo, A.; Misu, S. Association of fall history with the Timed Up and Go test score and the dual task cost: A cross-sectional study among independent community-dwelling older adults. Geriatr. Gerontol. Int. 2018, 18, 1189–1193. [Google Scholar] [CrossRef]
- Kang, L.; Han, P.; Wang, J.; Ma, Y.; Jia, L.; Fu, L.; Yu, H.; Chen, X.; Niu, K.; Guo, Q. Timed up and go test can predict recurrent falls: A longitudinal study of the community-dwelling elderly in China. Clin. Interv. Aging 2017, 12, 2009–2016. [Google Scholar] [CrossRef]
- Kyrdalen, I.L.; Thingstad, P.; Sandvik, L.; Ormstad, H. Associations between gait speed and well-known fall risk factors among community-dwelling older adults. Physiother. Res. Int. 2019, 24, e1743. [Google Scholar] [CrossRef]
- Welch, S.A.; Ward, R.E.; Kurlinski, L.A.; Kiely, D.K.; Goldstein, R.; VanSwearingen, J.; Brach, J.S.; Bean, J.F. Straight and Curved Path Walking among Older Adults in Primary Care: Associations with Fall-Related Outcomes. PM&R 2016, 8, 754–760. [Google Scholar] [CrossRef]
- Batko-Szwaczka, A.; Wilczyński, K.; Hornik, B.; Janusz-Jenczeń, M.; Włodarczyk, I.; Wnuk, B.; Szołtysek, J.; Durmała, J.; Szuster-Kowolik, K.; Antoniak-Sobczak, K.; et al. Predicting adverse outcomes in healthy aging community-dwelling early-old adults with the timed up and go test. Clin. Interv. Aging 2020, 15, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- ABEP. Critério de Classificação Econômica Brasil Associação Brasileira de Empresas de Pesquisa. 2014. Available online: https://www.abep.org/criterio-brasil (accessed on 20 September 2022).
- Gomes, A.P.; Soares, A.L.G.; Gonçalves, H. Baixa qualidade da dieta de idosos: Estudo de base populacional no sul do Brasil. Ciênc. Saúde Coletiva 2016, 21, 3417–3428. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Montes, M.C.; Bortolotto, C.C.; Tomasi, E.; Gonzalez, M.C.; Barbosa-Silva, T.G.; Domingues, M.R.; Bielemann, R.M. Strength and multimorbidity among community-dwelling elderly from southern Brazil. Nutrition 2020, 71, 110636. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Almeida, O.P.; Almeida, S.A. Short versions of the geriatric depression scale: A study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int. J. Geriatr. Psychiatry 1999, 14, 858–865. [Google Scholar] [CrossRef]
- Ramos, L.R.; Tavares, N.U.L.; Bertoldi, A.D.; Farias, M.R.; Oliveira, M.A.; Luiza, V.L.; da Silva Dal Pizzol, T.; Arrais, P.S.D.; Mengue, S.S.; Ramos, L.R.; et al. Polifarmácia e polimorbidade em idosos no Brasil: Um desafio em saúde pública. Rev. De. Saúde Pública 2016, 50, s1518–s8787. [Google Scholar] [CrossRef]
- Lipschitz, D.A. Screening for nutritional status in the elderly. Prim. Care 1994, 21, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Barros, A.J.; Hirakata, V.N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 3, 21. [Google Scholar] [CrossRef]
- Textor, J.; Van der Zander, B.; Gilthorpe, M.K.; Liskiewicz, M.; Ellison, G.T.H. Robust causal inference using directed acyclic graphs: The R package ‘dagitty’. Int. J. Epidemiol. 2016, 45, 1887–1894. [Google Scholar] [CrossRef]
- Abe, T.; Kitamura, A.; Taniguchi, Y.; Amano, H.; Seino, S.; Yokoyama, Y.; Nishi, M.; Narita, M.; Ikeuchi, T.; Fujiwara, Y.; et al. Pathway from gait speed to incidence of disability and mortality in older adults: A mediating role of physical activity. Maturitas 2019, 123, 32–36. [Google Scholar] [CrossRef]
- Chen, T.; Honda, T.; Chen, S.; Kishimoto, H.; Kumagai, S.; Narazaki, K. Potential utility of physical function measures to improve the risk prediction of functional disability in community-dwelling older Japanese adults: A prospective study. BMC Geriatr. 2021, 21, 476. [Google Scholar] [CrossRef]
- Srithumsuk, W.; Kabayama, M.; Godai, K.; Klinpudtan, N.; Sugimoto, K.; Akasaka, H.; Takami, Y.; Takeya, Y.; Yamamoto, K.; Yasumoto, S.; et al. Association between physical function and long-term care in community-dwelling older and oldest people: The SONIC study. Env. Health Prev. Med. 2020, 25, 46. [Google Scholar] [CrossRef]
- Otsuka, H.; Kobayashi, H.; Suzuki, K.; Hayashi, Y.; Ikeda, J.; Kushimoto, M.; Omoto, W.; Hara, M.; Abe, M.; Kato, K.; et al. Mobility performance among healthy older adults eligible for long-term care in Japan: A prospective observational study. Aging Clin. Exp. Res. 2020, 32, 1931–1937. [Google Scholar] [CrossRef]
- Lee, J.E.; Chun, H.; Kim, Y.S.; Jung, H.W.; Jang, I.Y.; Cha, H.M.; Son, K.Y.; Cho, B.; Kwon, I.S.; Yoon, J.L. Association between Timed Up and Go Test and Subsequent Functional Dependency. J. Korean Med. Sci. 2020, 35, e25. [Google Scholar] [CrossRef]
- Jonkman, N.H.; Colpo, M.; Klenk, J.; Todd, C.; Hoekstra, T.; Del Panta, V.; Rapp, K.; van Schoor, N.M.; Bandinelli, S.; Heymans, M.W.; et al. Development of a clinical prediction model for the onset of functional decline in people aged 65–75 years: Pooled analysis of four European cohort studies. BMC Geriatr. 2019, 19, 179. [Google Scholar] [CrossRef]
- Jonkman, N.H.; Del Panta, V.; Hoekstra, T.; Colpo, M.; van Schoor, N.M.; Bandinelli, S.; Cattelani, L.; Helbostad, J.L.; Vereijken, B.; Pijnappels, M.; et al. Predicting Trajectories of Functional Decline in 60- to 70-Year-Old People. Gerontology 2018, 64, 212–221. [Google Scholar] [CrossRef]
- Beaudart, C.; Rolland, Y.; Cruz-Jentoft, A.J.; Bauer, J.M.; Sieber, C.; Cooper, C.; Al-Daghri, N.; Araujo de Carvalho, I.; Bautmans, I.; Bernabei, R.; et al. Assessment of Muscle Function and Physical Performance in Daily Clinical Practice: A position paper endorsed by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Calcif. Tissue Int. 2019, 105, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, M.K.; Kuspinar, A.; Sohel, N.; Mayhew, A.; D’Amore, C.; Griffith, L.E.; Raina, P. Mobility screening for fall prediction in the Canadian Longitudinal Study on Aging (CLSA): Implications for fall prevention in the decade of healthy ageing. Age Ageing 2022, 51, afac095. [Google Scholar] [CrossRef] [PubMed]
- Quach, L.; Galica, A.M.; Jones, R.N.; Procter-Gray, E.; Manor, B.; Hannan, M.T.; Lipsitz, L.A. The nonlinear relationship between gait speed and falls: The maintenance of balance, independent living, intellect, and zest in the elderly of boston study. J. Am. Geriatr. Soc. 2011, 59, 1069–1073. [Google Scholar] [CrossRef] [PubMed]
- Bongers, K.T.J.; Schoon, Y.; Graauwmans, M.J.; Schers, H.J.; Melis, R.J.; Olde rikkert, M.G.M. The predictive value of gait speed and maximum step length for falling in community-dwelling older persons. Age Ageing 2015, 44, 294–299. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kojima, G.; Masud, T.; Kendrick, D.; Morris, R.; Gawler, S.; Treml, J.; Iliffe, S. Does the timed up and go test predict future falls among British community-dwelling older people? Prospective cohort study nested within a randomised controlled trial. BMC Geriatr. 2015, 15, 38. [Google Scholar] [CrossRef] [PubMed]
- Choo, P.L.; Tou, N.X.; Jun Pang, B.W.; Lau, L.K.; Jabbar, K.A.; Seah, W.T.; Chen, K.K.; Ng, T.P.; Wee, S.-L. Timed Up and Go (TUG) Reference Values and Predictive Cutoffs for Fall Risk and Disability in Singaporean Community-Dwelling Adults: Yishun Cross-Sectional Study and Singapore Longitudinal Aging Study. J. Am. Med. Dir. Assoc. 2021, 22, 1640–1645. [Google Scholar] [CrossRef]
- Carneiro, J.A.; Ramos, G.C.F.; Barbosa, A.T.F.; Vieira, É.D.S.; Silva, J.S.R.; Caldeira, A.P. Quedas em idosos não institucionalizados no norte de Minas Gerais: Prevalência e fatores associados. Rev. Bras. de Geriatr. e Gerontol. 2016, 19, 613–625. [Google Scholar] [CrossRef]
- Sanchez, M.; Vidal, J.S.; Bichon, A.; Mairesse, C.; Flouquet, C.; Hanon, O.; Raynaud-Simon, A. Impact of a public open-access community-based physical activity and fall prevention program on physical performance in older adults. Eur. J. Public. Health 2023, 33, 132–138. [Google Scholar] [CrossRef]
- Mose, M.; Brodersen, K.; Rittig, N.; Schmidt, J.; Jessen, N.; Mikkelsen, U.; Jørgensen, J.O.L.; Møller, N. Anabolic effects of oral leucine-rich protein with and without β-hydroxybutyrate on muscle protein metabolism in a novel clinical model of systemic inflammation—A randomized crossover trial. Am. J. Clin. Nutr. 2021, 114, 1159–1172. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Sáez De Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; García-Hermoso, A.; Recarey, A.E.; Fernández-Irigoyen, J.; Santamaría, E.; Palomino-Echeverría, S.; Izquierdo, M. Circulating Cytokines and Lower Body Muscle Performance in Older Adults at Hospital Admission. J. Nutr. Health Aging 2020, 24, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Moreland, B.L.; Durbin, L.L.; Kasper, J.D.; Mielenz, T.J. Rehabilitation Utilization for Falls Among Community-Dwelling Older Adults in the United States in the National Health and Aging Trends Study. Arch. Phys. Med. Rehabil. 2018, 99, 1568–1575. [Google Scholar] [CrossRef] [PubMed]
- Lester, D.; Tiedemann, A.; Sherrington, C. Objectively measured mobility of rural community-dwelling people aged 80 and over is strongly associated with greater use of services for community integration and social support: An observational study. Aust. J. Rural. Health 2019, 27, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Gell, N.M.; Patel, K.V. Rehabilitation Services Use of Older Adults According to Fall-Risk Screening Guidelines: Fall-Risk and Rehabilitation Services Use. J. Am. Geriatr. Soc. 2019, 67, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Guedes, R.D.C.; Dias, R.C.; Neri, A.L.; Ferriolli, E.; Lourenço, R.A.; Lustosa, L.P. Declínio da velocidade da marcha e desfechos de saúde em idosos: Dados da Rede Fibra. Fisioter. Pesqui. 2019, 26, 304–310. [Google Scholar] [CrossRef]
- Duan-Porter, W.; Vo, T.N.; Ullman, K.; Langsetmo, L.; Strotmeyer, E.S.; Taylor, B.C.; Santanasto, A.J.; Cawthon, P.M.; Newman, A.B.; Simonsick, E.M.; et al. Hospitalization-Associated Change in Gait Speed and Risk of Functional Limitations for Older Adults. Magaziner J, organizador. J. Gerontol. Ser. A 2019, 74, 1657–1663. [Google Scholar] [CrossRef] [PubMed]
- Ge, L.; Yap, C.W.; Heng, B.H. Association of Nutritional Status with Physical Function and Disability in Community-Dwelling Older Adults: A Longitudinal Data Analysis. J. Nutr. Gerontol. Geriatr. 2020, 39, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, A.; Vetrano, D.L.; Grande, G.; Calderón-Larrañaga, A.; Fratiglioni, L.; Marengoni, A.; Rizzuto, D. Comparing the prognostic value of geriatric health indicators: A population-based study. BMC Med. 2019, 17, 185. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Complete Sample in 2014 | Study Sample in 2019 | |||
|---|---|---|---|---|
| Variables | N = 1451 | % (95%CI) a | N = 476 | % (95%CI) a |
| Sex | ||||
| Female | 914 | 63.0 (60.5; 65.4) | 310 | 65.1 (60.7; 69.3) |
| Male | 537 | 37.0 (34.6; 39.5) | 166 | 34.9 (30.7; 39.3) |
| Age (completed years) | ||||
| 60–69 | 756 | 52.3 (49.7; 54.9) | 289 | 60.7 (56.2; 65.0) |
| 70–79 | 460 | 31.8 (29.5; 34.3) | 151 | 31.7 (27.7; 36.1) |
| 80+ | 230 | 15.9 (14.1; 17.9) | 36 | 7.6 (5.5; 10.3) |
| Skin color | ||||
| White | 1211 | 83.7 (81.7; 85.6) | 389 | 81.7 (78.0; 85.0) |
| Other than white | 236 | 16.3 (14.5; 18.3) | 87 | 18.3 (15.0; 22.0) |
| Marital status | ||||
| Married/with a partner | 763 | 52.7 (50.2; 55.3) | 286 | 60.1 (55.6; 64.4) |
| Without a partner/separated | 225 | 15.6 (13.8; 17.6) | 72 | 15.1 (12.2; 18.6) |
| Widow(er) | 459 | 31.7 (29.4; 34.2) | 118 | 24.8 (21.1; 28.9) |
| Economic level b | ||||
| A/B | 483 | 35.2 (32.7; 37.8) | 161 | 35.4 (31.1; 39.9) |
| C | 720 | 52.5 (49.8; 55.1) | 248 | 54.5 (49.9; 59.0) |
| D/E | 169 | 12.3 (10.7; 14.2) | 46 | 10.1 (7.7; 13.2) |
| Education level (completed years) | ||||
| None | 196 | 13.6 (12.0; 15.5) | 54 | 11.4 (8.8; 14.6) |
| 1–7 | 782 | 54.4 (51.8; 57.0) | 270 | 56.8 (52.3; 61.2) |
| ≥8 | 459 | 32.0 (29.6; 34.4) | 151 | 31.8 (27.7; 36.1) |
| Current work situation | ||||
| No (unemployed) | 1084 | 80.4 (78.2; 82.4) | 344 | 77.0 (72.8; 80.6) |
| Yes (employed) | 264 | 19.6 (17.6; 21.8) | 103 | 23.0 (19.4; 27.2) |
| Diet quality c | ||||
| Low | 481 | 33.7 (31.3; 36.2) | 143 | 30.2 (26.3; 34.6) |
| Average | 534 | 37.5 (35.0; 40.0) | 177 | 37.5 (33.2; 41.9) |
| High | 411 | 28.8 (26.5; 31.2) | 153 | 32.3 (28.3; 36.7) |
| Leisure-time physical activity d | ||||
| ≤150 min/week | 1133 | 81.5 (79.3; 83.4) | 378 | 80.4 (76.6; 83.8) |
| >150 min/week | 258 | 18.5 (16.6; 20.7) | 92 | 19.6 (16.2; 23.4) |
| Smoking | ||||
| Not a smoker | 781 | 54.0 (51.4; 56.6) | 262 | 55.0 (50.5; 59.5) |
| Smoker | 182 | 12.6 (11.0; 14.4) | 58 | 12.2 (9.5; 15.5) |
| Former smoker | 483 | 33.4 (31.0; 35.9) | 156 | 32.8 (28.7; 37.1) |
| Alcohol consumption e | ||||
| No | 1138 | 78.8 (76.6; 80.8) | 355 | 74.6 (70.5; 78.3) |
| Yes | 307 | 21.2 (19.2; 23.4) | 121 | 25.4 (21.7; 29.5) |
| Multimorbidity | ||||
| Up to 4 diseases | 473 | 35.3 (32.8; 37.9) | 175 | 37.6 (33.3; 42.1) |
| 5 or more diseases | 866 | 64.7 (62.1; 67.2) | 291 | 62.4 (57.9; 66.7) |
| Depression f | ||||
| No | 1182 | 84.8 (82.8; 86.6) | 408 | 86.4 (83.0; 89.3) |
| Yes | 212 | 15.2 (13.4; 17.2) | 64 | 13.6 (10.7; 17.0) |
| Polypharmacy g | ||||
| 0–4 medications | 513 | 35.6 (33.1; 38.1) | 150 | 31.5 (27.5; 35.8) |
| ≥5 medications | 929 | 64.4 (61.9; 66.9) | 326 | 68.5 (64.2; 72.5) |
| BMI h | ||||
| <22.0 kg/m2 | 126 | 9.2 (7.8; 10.9) | 26 | 5.5 (3.8; 8.0) |
| 22.0–27.0 kg/m2 | 471 | 34.5 (32.1; 37.1) | 152 | 32.1 (28.1; 36.4) |
| >27.0 kg/m2 | 767 | 56.3 (53.6; 58.8) | 295 | 62.4 (57.9; 66.6) |
| Physical Performance Tests | ||||
| Gait Speed (GS) in 2014 i | ||||
| Normal (>0.8 m/s) | 994 | 76.2 (73.8; 78.4) | 385 | 82.1 (78.3; 85.3) |
| Low (≤0.8 m/s) | 311 | 23.8 (21.6; 26.2) | 84 | 17.9 (14.7; 21.7) |
| Change in GS (2014–2019) j | ||||
| Stable–Improvement | - | - | 152 | 31.9 (27.9; 36.3) |
| Decline | - | - | 324 | 68.1 (63.7; 72.1) |
| Timed Up and Go (TUG) in 2014 k | ||||
| Normal (≤11 s) | 881 | 67.3 (64.7; 69.7) | 340 | 72.2 (68.0; 76.1) |
| Low performance (>11 s) | 429 | 32.7 (30.3; 35.3) | 131 | 27.8 (23.9; 32.0) |
| Change in TUG (2014–2019) j | ||||
| Stable–Improvement | - | - | 150 | 31.9 (27.8; 36.2) |
| Worsening | - | - | 321 | 68.1 (63.8; 72.2) |
| Variables | Negative Health Self-Perception a N = 32 | Health Consultations (≥5 Per Year) N = 156 | ||
|---|---|---|---|---|
| Crude p-Value PR (95%CI) | Adjusted p-Value b PR (95%CI) | Crude p-Value PR (95%CI) | Adjusted p-Value b PR (95%CI) | |
| GS (m/s) in 2014 c (n = 1305) | 0.007 | 0.327 | 0.272 | 0.261 |
| Normal (>0.8 m/s) (n = 994) | 1.00 | 1.00 | 1.00 | 1.00 |
| Low (≤0.8 m/s) (n = 311) | 2.65 (1.31; 5.37) | 1.52 (0.66; 3.52) | 1.19 (0.88; 1.61) | 1.21 (0.87; 1.69) |
| Change in GS (2014–2019) d (n = 476) | 0.791 | 0.488 | 0.910 | 0.718 |
| Stable–Improvement (n = 152) | 1.00 | 1.00 | 1.00 | 0.820 |
| Decline (n = 324) | 1.11 (0.52; 2.36) | 1.28 (0.63; 2.61) | 0.98 (0.75; 1.29) | 1.04 (0.77; 1.39) |
| TUG (s) in 2014 e (n = 1433) | 0.003 | 0.085 | 0.121 | 0.243 |
| Normal (≤11 s) (n = 1231) | 1.00 | 1.00 | 1.00 | 1.00 |
| Low performance (>11 s) (n = 202) | 2.77 (1.41; 5.44) | 1.83 (0.92; 3.64) | 1.23 (0.95; 1.60) | 1.18 (0.89; 1.57) |
| Change in TUG (2014–2019) d (n = 471) | 0.653 | 0.836 | 0.699 | 0.796 |
| Stable–Improvement (n = 150) | 1.00 | 1.00 | 1.00 | 1.00 |
| Worsening (n = 321) | 0.85 (0.42; 1.73) | 0.93 (0.46; 1.88) | 0.95 (0.73; 1.24) | 1.04 (0.77; 1.40) |
| Variables | Physical Disability a N = 162 | Falls (Last Year) N = 130 | Hospitalization (Last Year) N = 65 | |||
|---|---|---|---|---|---|---|
| Crude p-Value PR (95%CI) | Adjusted p-Value b PR (95%CI) | Crude p-Value PR (95%CI) | Adjusted p-Value b PR (95%CI) | Crude p-Value PR (95%CI) | Adjusted p-Value b PR (95%CI) | |
| GS (m/s) in 2014 c (n = 1305) | <0.001 | 0.002 | 0.032 | 0.104 | 0.914 | 0.980 |
| Normal (>0.8 m/s) (n = 994) | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Low (≤0.8 m/s) (n = 311) | 1.92 (1.50; 2.45) | 1.56 (1.18; 2.06) | 1.44 (1.03; 2.02) | 1.37 (0.94; 2.01) | 0.97 (0.53; 1.77) | 0.99 (0.53; 1.87) |
| Change in GS (2014–2019) d (n = 476) | 0.900 | 0.326 | 0.072 | 0.221 | 0.341 | 0.033 |
| Stable–Improvement (n = 152) | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Decline (n = 324) | 0.98 (0.75; 1.29) | 1.15 (0.87; 1.53) | 0.76 (0.56; 1.03) | 0.81 (0.58; 1.14) | 1.29 (0.76; 2.17) | 1.86 (1.05; 3.31) |
| TUG (s) in 2014 e (n = 1433) | <0.001 | <0.001 | 0.002 | 0.007 | 0.341 | 0.303 |
| Normal (≤11 s) (n = 1231) | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Low performance (>11 s) (n = 202) | 1.96 (1.54; 2.49) | 1.60 (1.24; 2.06) | 1.59 (1.18; 2.15) | 1.57 (1.13; 2.18) | 1.26 (0.78; 2.05) | 1.32 (0.78; 2.26) |
| Change in TUG (2014–2019) d (n = 471) | 0.651 | 0.065 | 0.254 | 0.717 | 0.682 | 0.303 |
| Stable–Improvement (n = 150) | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Worsening (n = 321) | 1.07 (0.81; 1.41) | 1.30 (0.98; 1.71) | 0.84 (0.61; 1.14) | 0.94 (0.65; 1.34) | 1.11 (0.67; 1.83) | 1.34 (0.77; 2.32) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomes, D.R.d.P.; Santos, L.P.; Vieira, E.R.; Bertoldi, A.D.; Tomasi, E.; Demarco, F.F.; Gonzalez, M.C.; Farias-Antunez, S.; Bielemann, R.M. Low Physical Performance Could Be Associated with Adverse Health Outcomes over Time: Results from a Cohort of Older Adults. Int. J. Environ. Res. Public Health 2024, 21, 319. https://doi.org/10.3390/ijerph21030319
Gomes DRdP, Santos LP, Vieira ER, Bertoldi AD, Tomasi E, Demarco FF, Gonzalez MC, Farias-Antunez S, Bielemann RM. Low Physical Performance Could Be Associated with Adverse Health Outcomes over Time: Results from a Cohort of Older Adults. International Journal of Environmental Research and Public Health. 2024; 21(3):319. https://doi.org/10.3390/ijerph21030319
Chicago/Turabian StyleGomes, Darlise Rodrigues dos Passos, Leonardo Pozza Santos, Edgar Ramos Vieira, Andréa Dâmaso Bertoldi, Elaine Tomasi, Flávio Fernando Demarco, Maria Cristina Gonzalez, Simone Farias-Antunez, and Renata Moraes Bielemann. 2024. "Low Physical Performance Could Be Associated with Adverse Health Outcomes over Time: Results from a Cohort of Older Adults" International Journal of Environmental Research and Public Health 21, no. 3: 319. https://doi.org/10.3390/ijerph21030319
APA StyleGomes, D. R. d. P., Santos, L. P., Vieira, E. R., Bertoldi, A. D., Tomasi, E., Demarco, F. F., Gonzalez, M. C., Farias-Antunez, S., & Bielemann, R. M. (2024). Low Physical Performance Could Be Associated with Adverse Health Outcomes over Time: Results from a Cohort of Older Adults. International Journal of Environmental Research and Public Health, 21(3), 319. https://doi.org/10.3390/ijerph21030319