
Development of Systemic Interventions to Decrease Breast Cancer Risk: A Group Concept Mapping Study


 ,
,
Abstract
1. Introduction
1.1. Background
1.2. Paths to Prevention: The California Breast Cancer Primary Prevention Plan
1.3. Aims and Objectives of the Current Project
2. Materials and Methods
2.1. Advisory Group
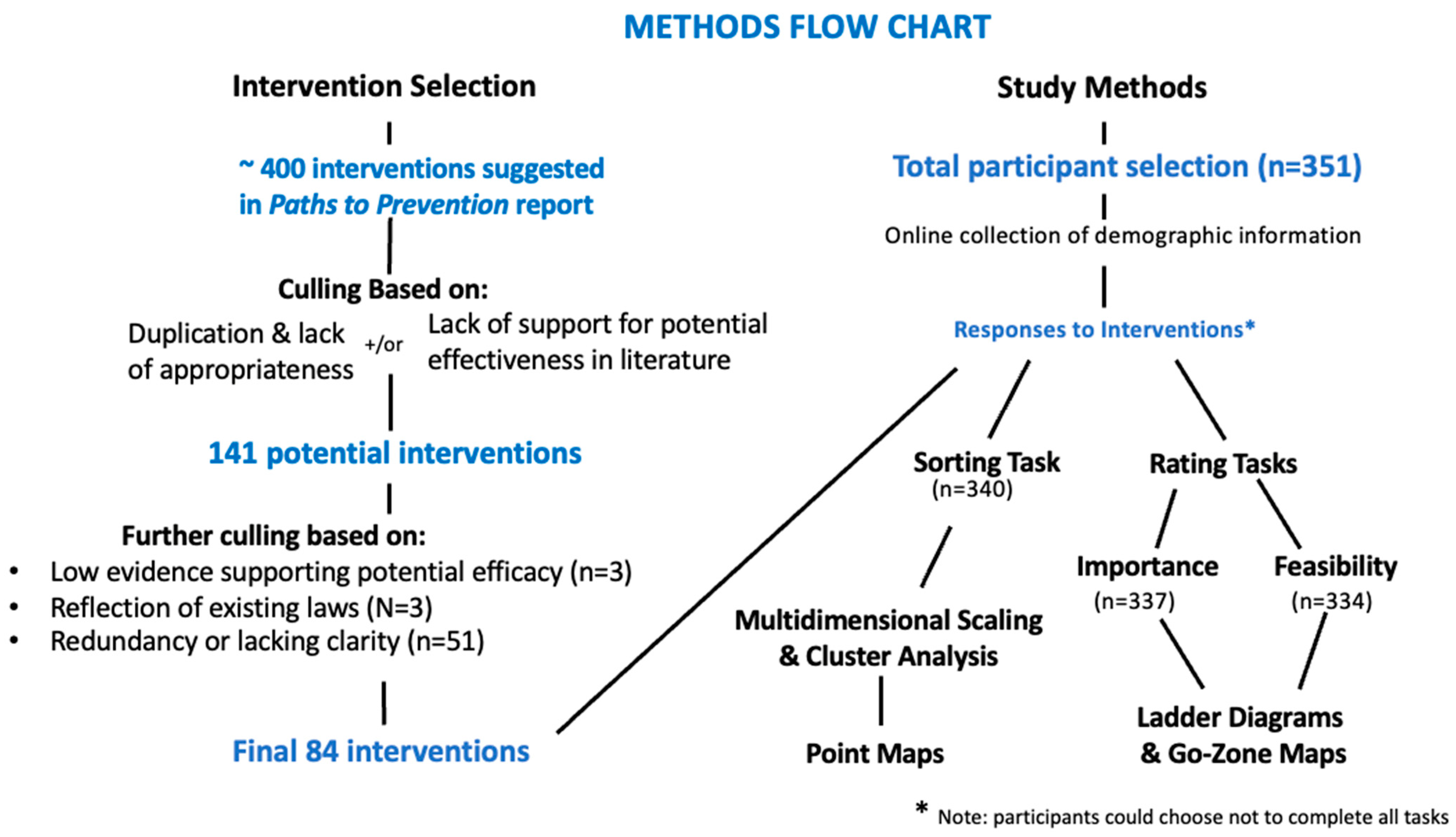
2.2. Development of the Target Interventions for the GCM Exercise
2.3. Participants
2.4. GCM Data Collection and Analysis
2.4.1. Online Data Collection
2.4.2. Multidimensional Scaling and Hierarchical Cluster Analysis
2.4.3. Pattern Match/Ladder Analyses
2.4.4. Go-Zone Maps
3. Results
3.1. Demographics of Study Participants
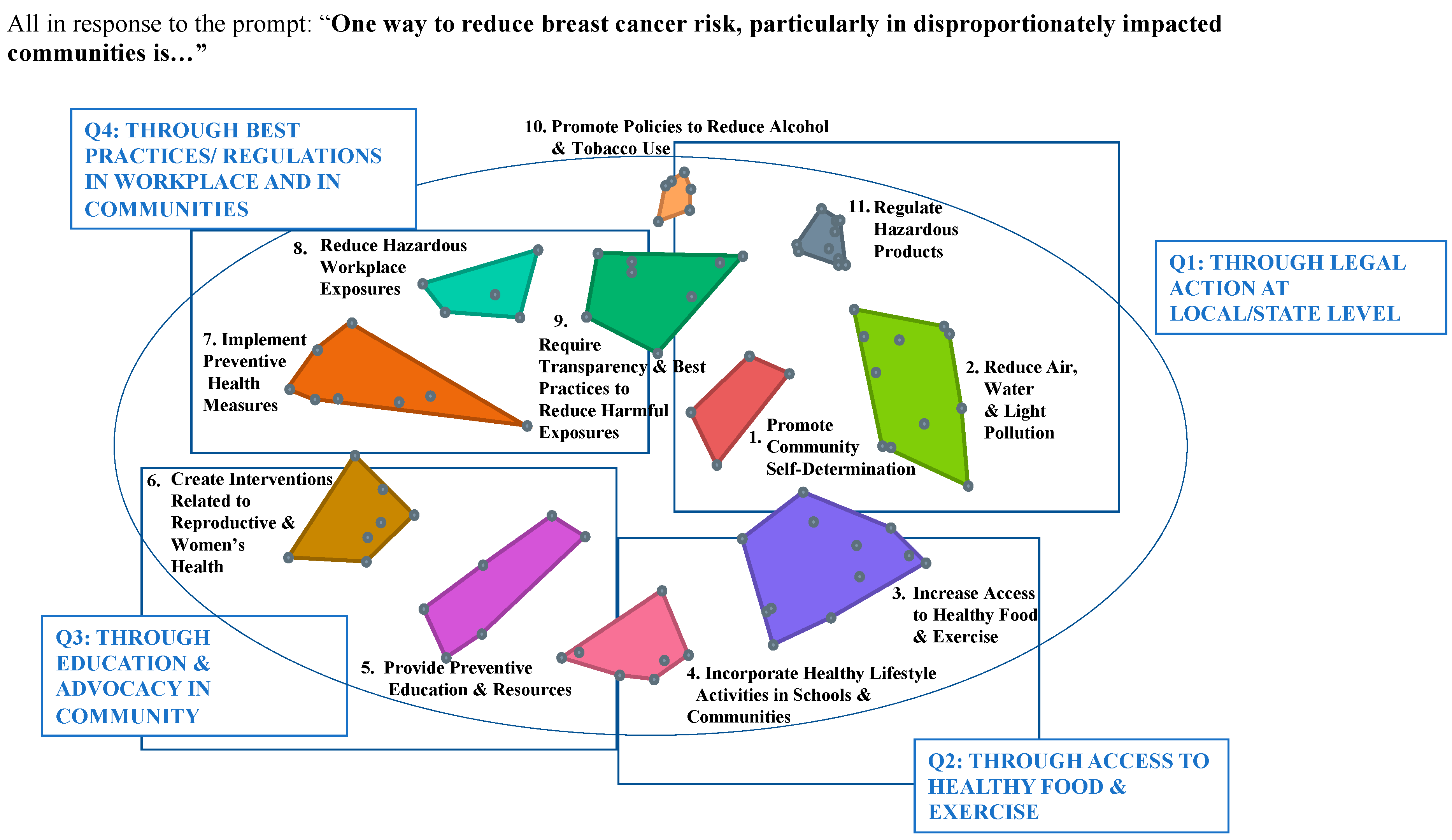
3.2. Cluster Analysis
3.3. Validity and Reliability of Cluster Analysis Results
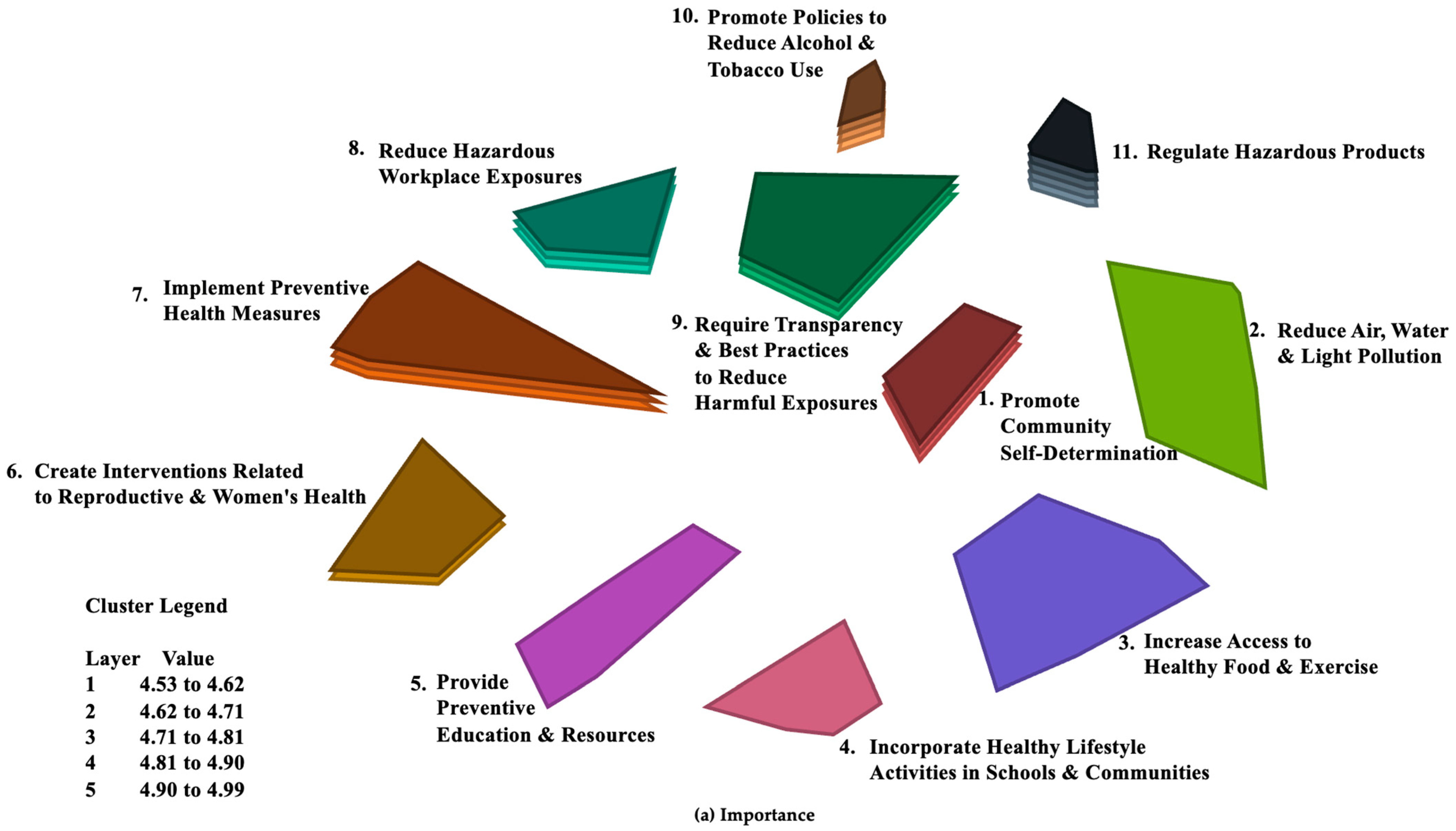
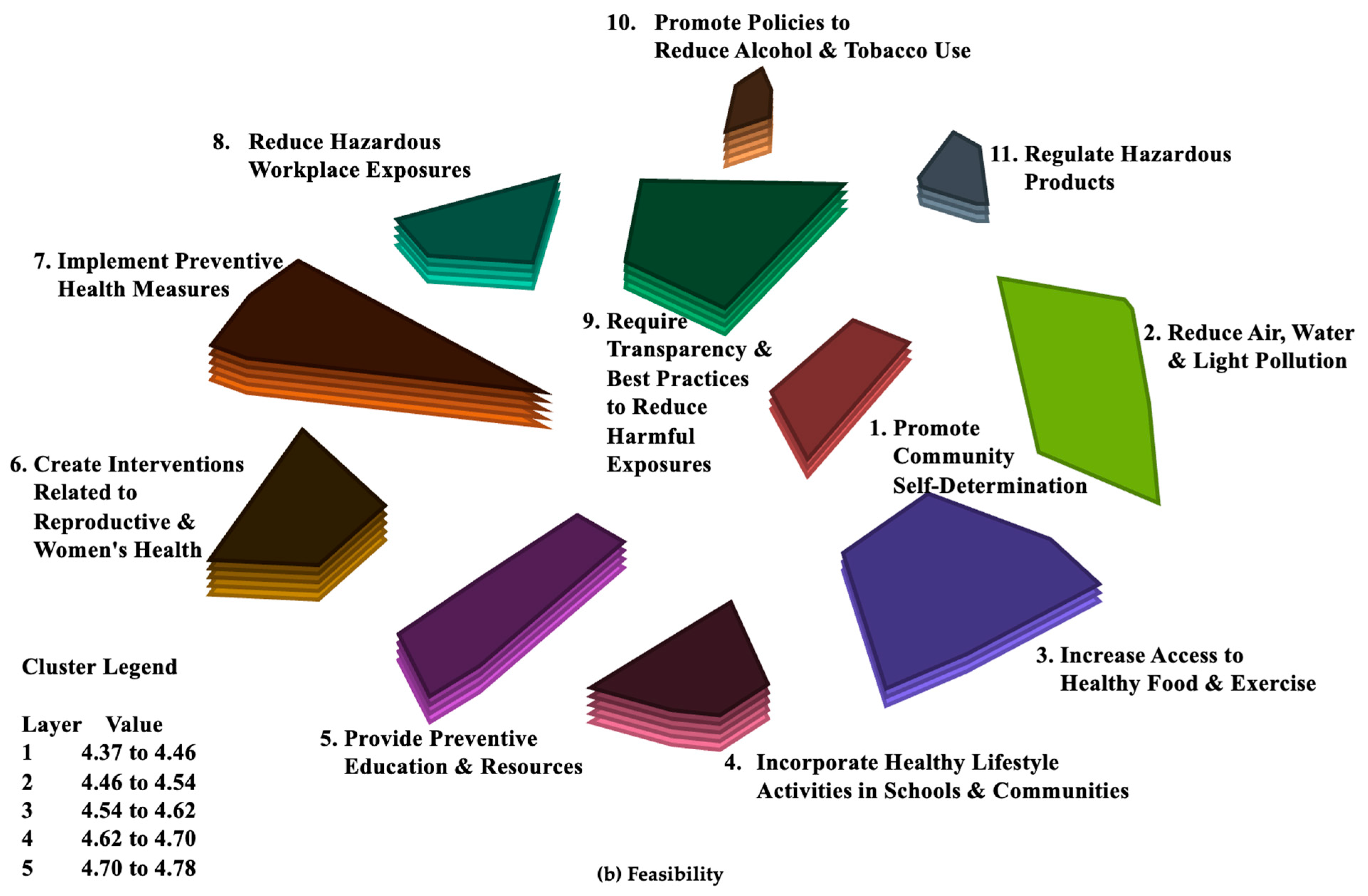
3.4. Relative Ratings of Mean Values for Importance and Feasibility across Clusters
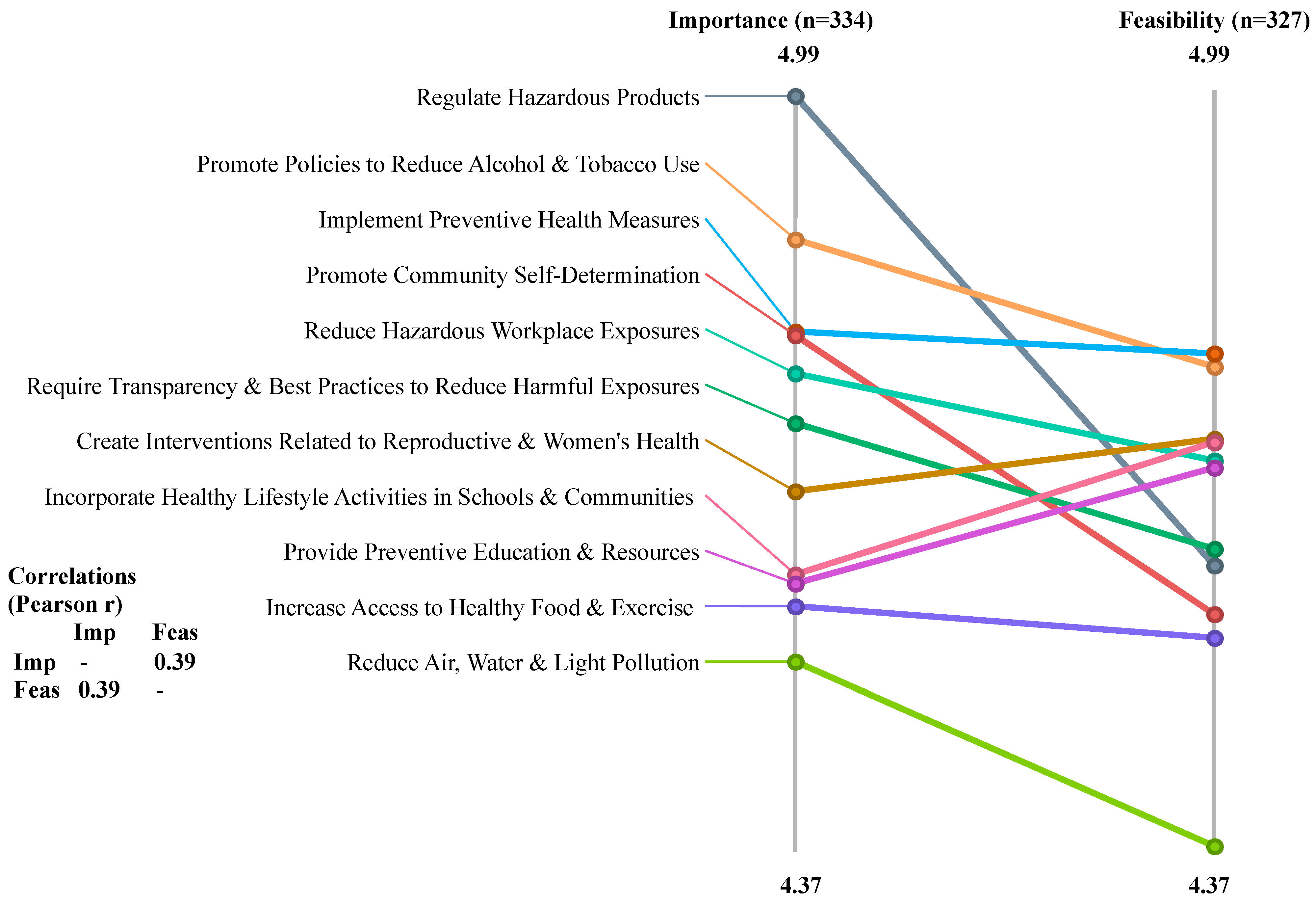
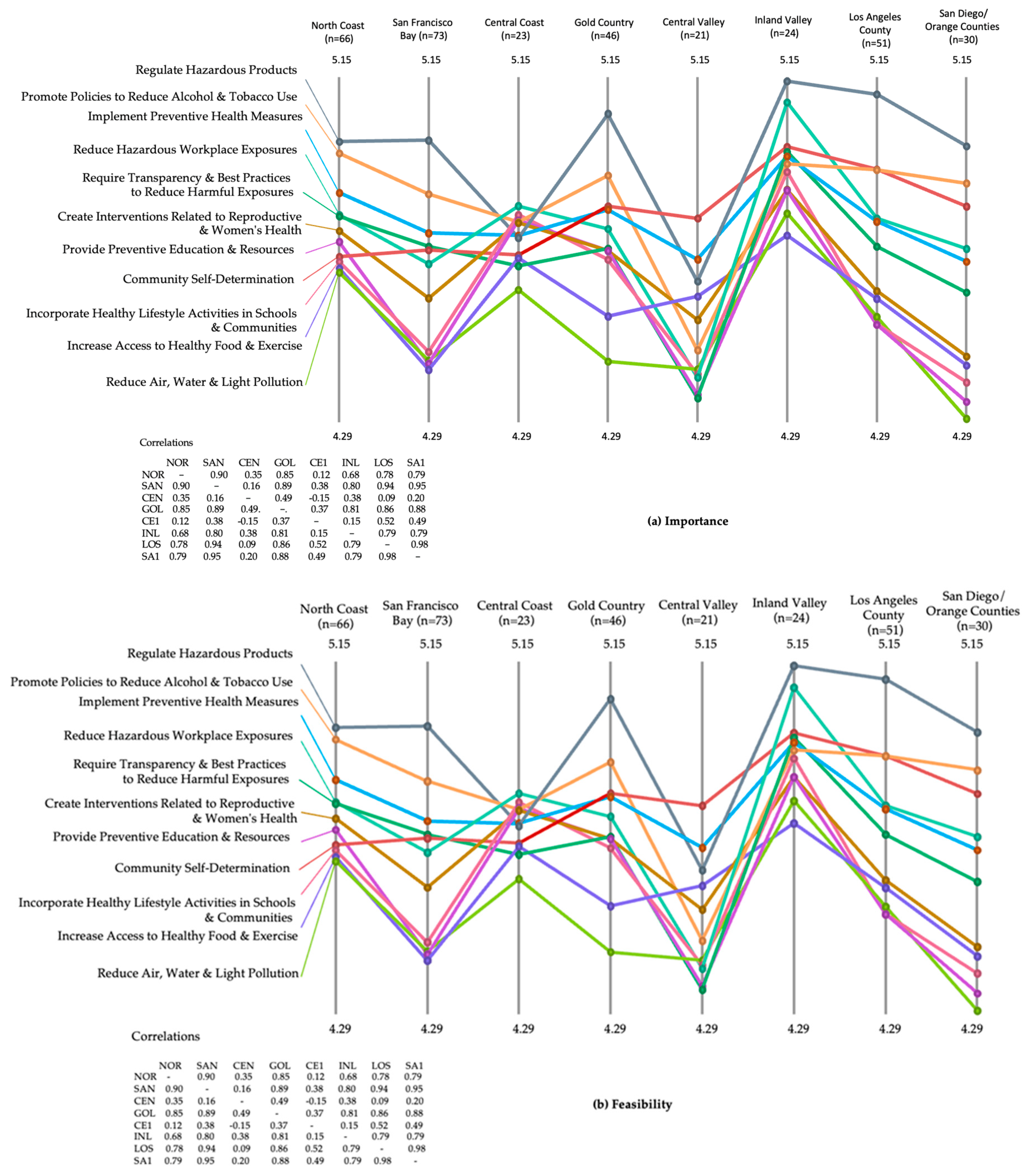
3.5. Pattern Match/Ladder Analyses
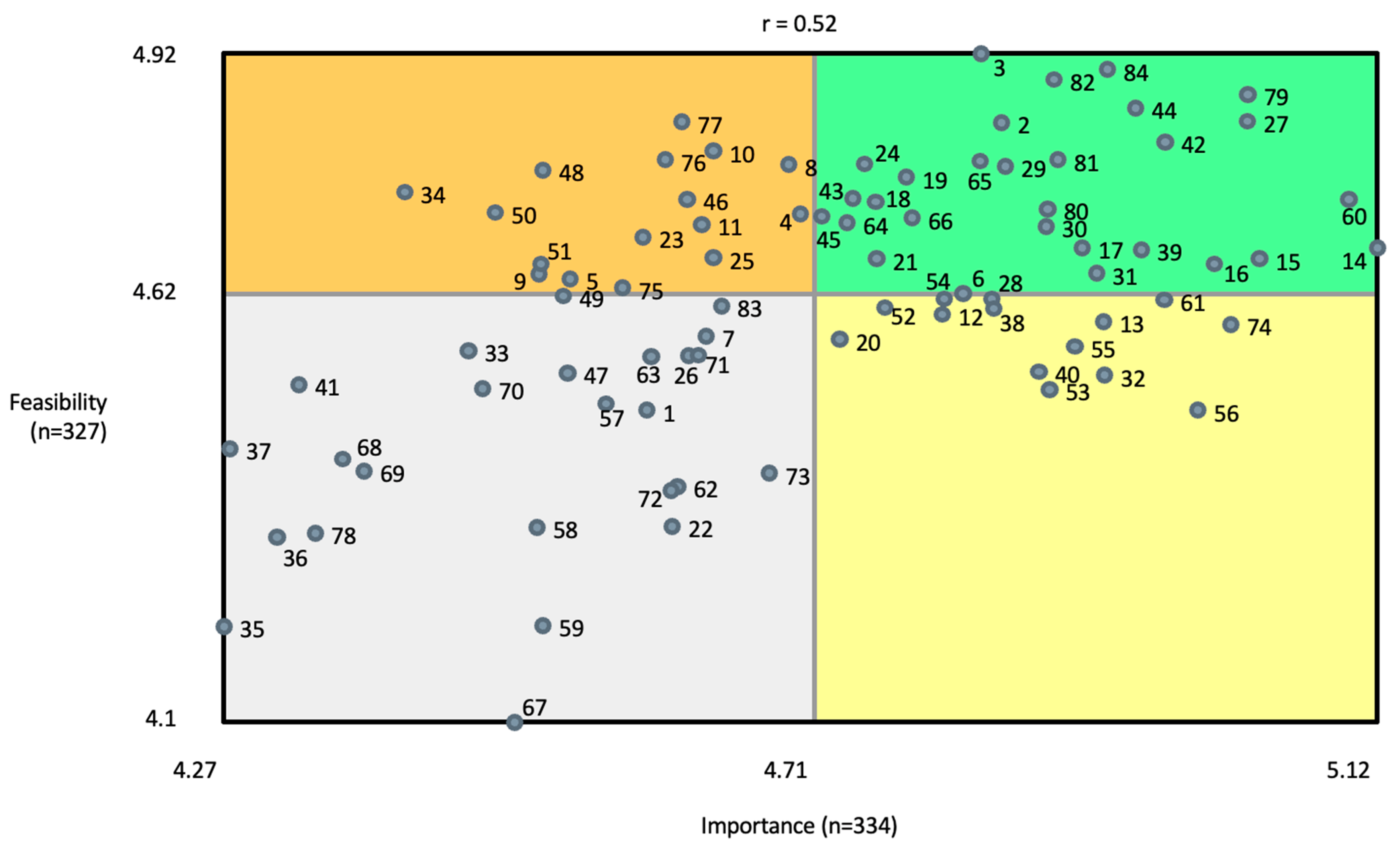
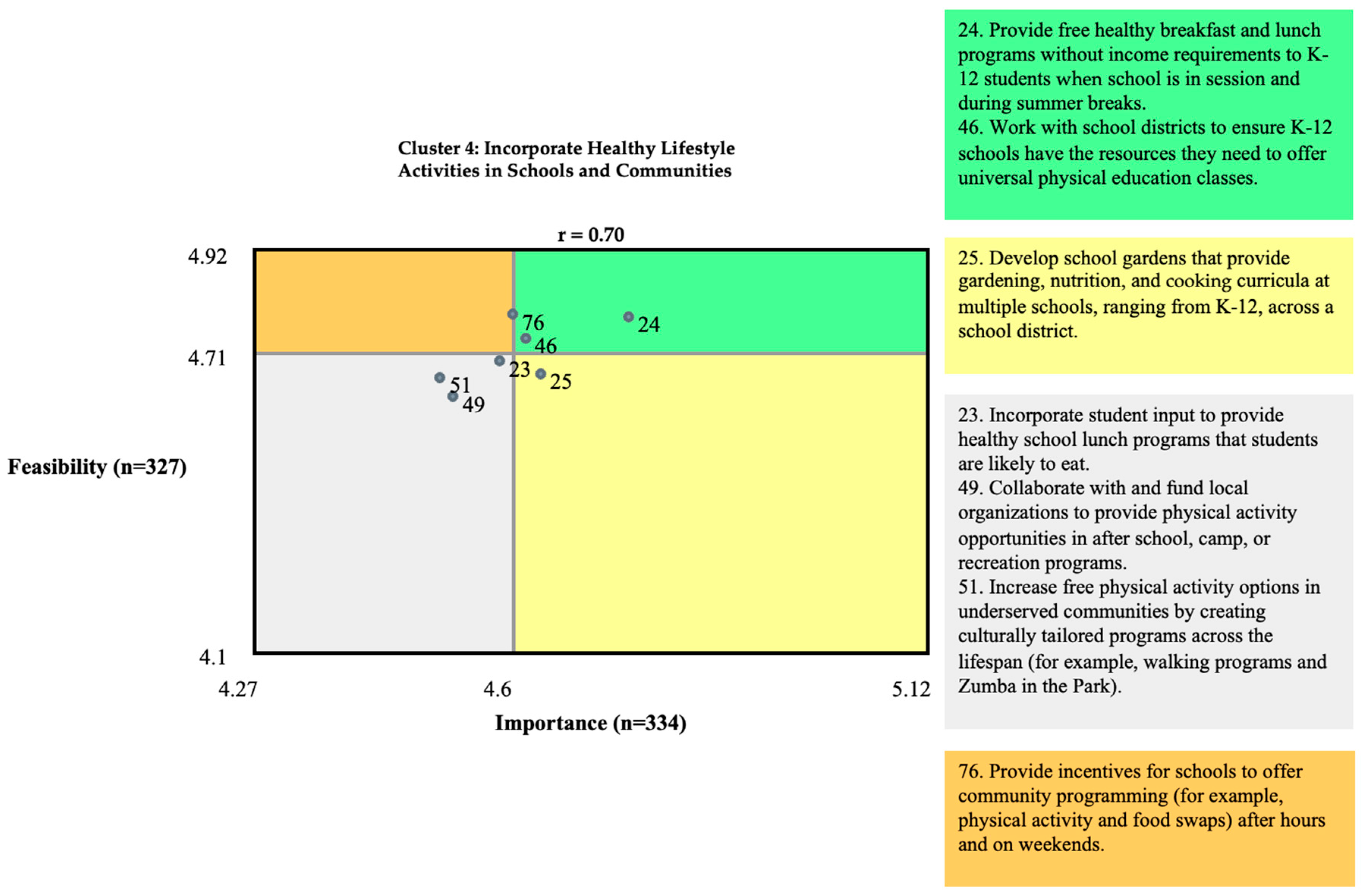
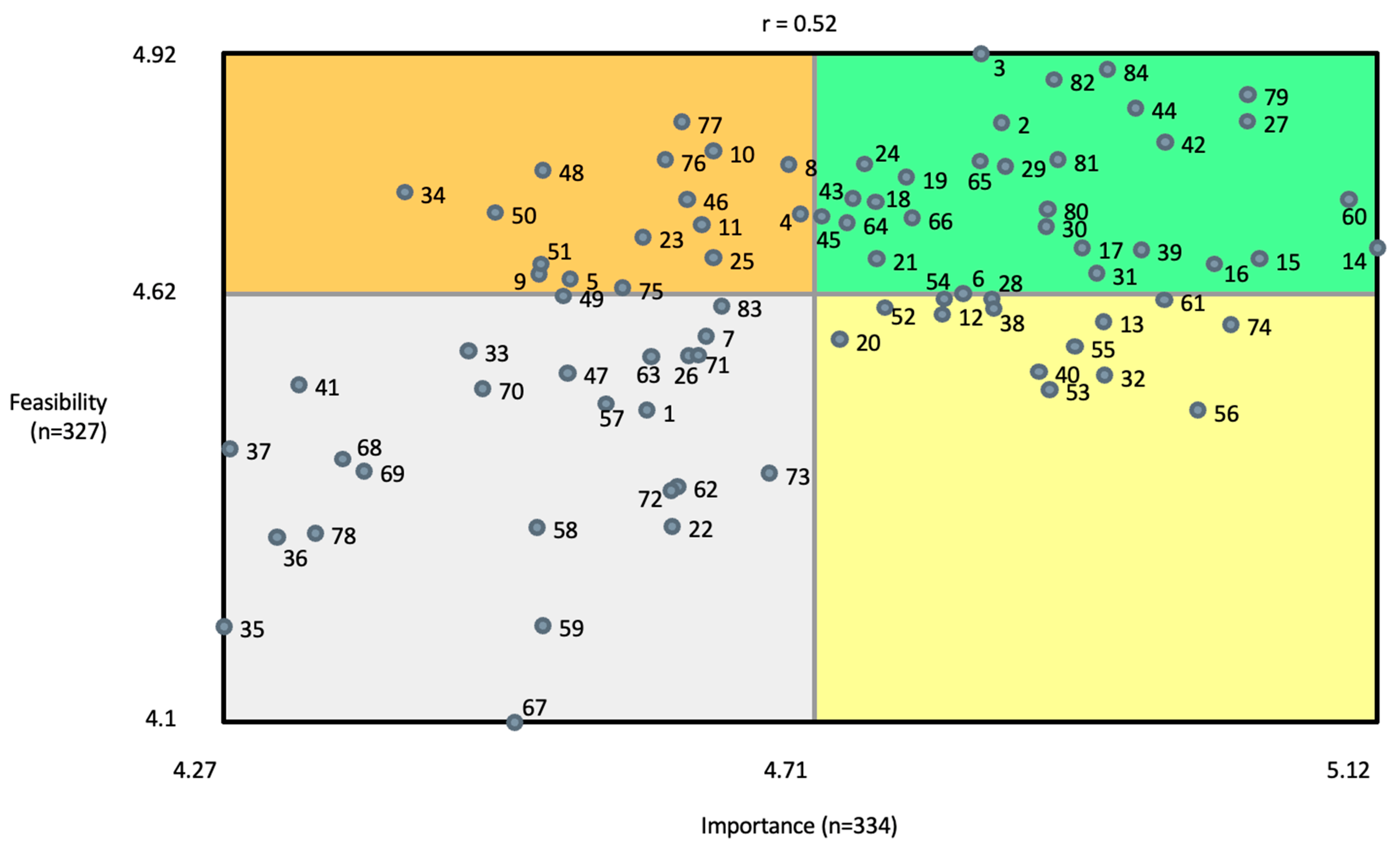
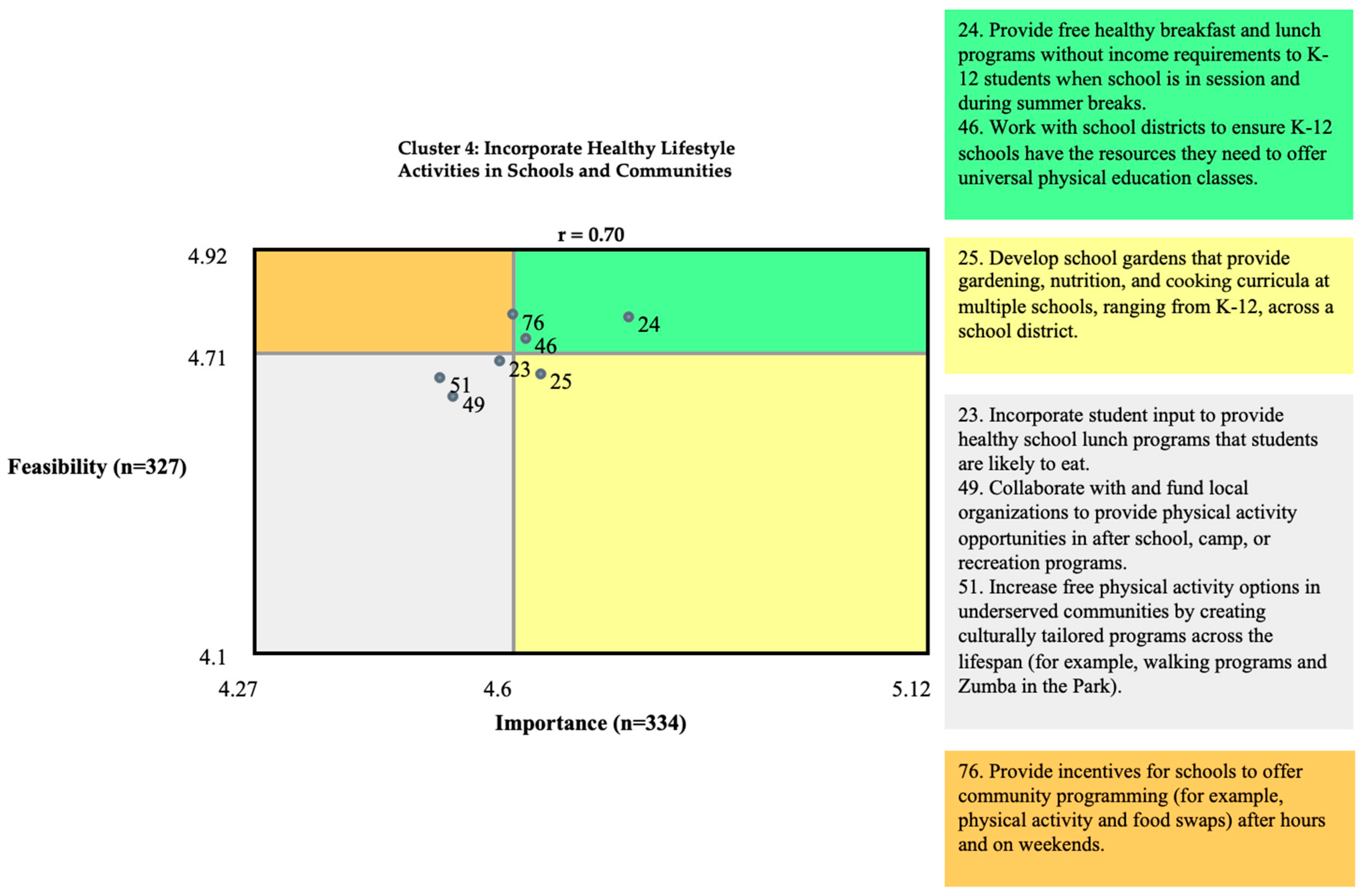
3.6. Go-Zone Maps
4. Discussion
4.1. Community-Partnered Participatory Approach
4.2. Strengths and Limitations of the Project
4.3. Moving Forward: Implications for Research, Policy, and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Cancer Facts & Figures 2023; American Cancer Society: Atlanta, GA, USA, 2023. [Google Scholar]
- Eom, E.Y.; Berg, K.A.; Joseph, N.E.; Runner, K.; Tarabichi, Y.; Khiyami, A.; Perzynski, A.; Sossey-Alaoui, K. Neighborhood and racial influences on triple negative breast cancer: Evidence from Northeast Ohio. Breast Cancer Res. Treat. 2023, 198, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Terman, E.; Sheade, J.; Zhao, F.; Howard, F.M.; Jaskowiak, N.; Tseng, J.; Chen, N.; Hahn, O.; Fleming, G.; Huo, D.; et al. The impact of race and age on response to neoadjuvant therapy and long-term outcomes in Black and White women with early-stage breast cancer. Breast Cancer Res. Treat. 2023, 200, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Buermeyer, N.; Engel, C.; Nudelman, J.; Rasanayagam, S.; Sarantis, H. Paths to Prevention: The California Breast Cancer Prevention Primary Plan. 2020. Available online: https://www.bcpp.org/wp-content/uploads/2020/09/Paths-to-Prevention-CaliforniaBreast-Cancer-Primary-Prevention-Plan_September-2020.pdf (accessed on 30 November 2023).
- Lyons, M.J.; Poole, S.F.; Brownson, R.C.; Lyn, R. Place is power: Investing in communities as a systemic leverage point to reduce breast cancer disparities by race. Int. J. Environ. Res. Public Health 2022, 19, 632. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, K.M.; Udesky, J.O.; Rudel, R.A.; Brody, J.G. Environmental chemicals and breast cancer: An updated review of epidemiological literature informed by biological mechanisms. Environ. Res. 2018, 160, 152–182. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.M.; Rasanayagam, S.; Engel, C.; Rizzo, J. The state of the evidence 2017: An update on the connection between breast cancer and the environment. Environ. Health 2017, 16, 94. [Google Scholar] [CrossRef] [PubMed]
- President’s Cancer Panel. Reducing Environmental Cancer Risk: What We Can Do Now; National Cancer Institute: Bethesda, MD, USA, 2010. Available online: https://deainfo.nci.nih.gov/advisory/pcp/annualReports/pcp08-09rpt/PCP_Report_08-09_508.pdf (accessed on 12 January 2023).
- Golubnitschaja, O.; Debald, M.; Yeghiazaryan, K.; Kuhn, W.; Pešta, M.; Costigliola, V.; Grech, G. Breast cancer epidemic in the early twenty-first century: Evaluation of risk factors, cumulative questionnaires and recommendations for preventive measures. Tumour Biol. 2016, 37, 12941–12957. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, S.D.; Malow, R.M.; Jolly, C. Community-based participatory research (CBPR): A new and not-so-new approach to HIV/AIDS prevention, care, and treatment. AIDS Educ. Prev. 2010, 22, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; Hoague, D.; Spriggs, R.; Catalan, E.; Adams, N.; Watkins, T.; Tripati, A.; Norris, K.C. Establishing a framework for sustainable community research. Ethn. Dis. 2022, 32, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Sevelius, J.M.; Guttierez-Mock, L.; Zamudio-Haas, S.; McCree, N.; Ngo, A.; Jackson, A.; Clynes, C.; Venegas, L.; Salinas, A.; Herrera, C.; et al. Research with marginalized communities: Challenges to continuity during the COVID-19 pandemic. AIDS Behav. 2022, 24, 2009–2012. [Google Scholar] [CrossRef] [PubMed]
- Passmore, S.R.; Kisicki, A.; Gilmore-Bykovskyi, A.; Green-Harris, G.; Edwards, D.F. “There’s not much we can do…” Researcher-level barriers to the inclusion of underrepresented participants in translational research. J. Clin. Transl. Sci. 2021, 6, e4. [Google Scholar] [CrossRef] [PubMed]
- Kane, M.; Rosas, S. Conversations about Group Concept Mapping: Applications, Examples, and Enhancements; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Kane, M.; Trochim, W. Concept Mapping for Planning and Evaluation (Applied Social Research Methods), 1st ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2006. [Google Scholar]
- Kruskal, J.B.; Wish, M. Multidimensional Scaling; Sage Publishications, Inc.: Beverly Hills, CA, USA, 1978. [Google Scholar]
- Everitt, B. Cluster Analysis, 2nd ed.; Halsted Press: New York, NY, USA, 1980. [Google Scholar]
- Rosenberg, S.; Kim, M.P. The method of sorting as a data gathering procedure in multivariate research. Multivar. Behav. Res. 1975, 10, 489–502. [Google Scholar] [CrossRef] [PubMed]
- Trochim, W.M.K. The Reliability of Concept Mapping; Annual Conference of the American Evualtion Association: Dallas, TX, USA, 1993. [Google Scholar]
- Rosas, S.R.; Kane, M. Quality and rigor of the concept mapping methodology: A pooled study analysis. Eval. Program Plann. 2012, 35, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Bedi, N.; Lerner, S.; McGrory, K. Why the U.S. Is Losing the Fight to Ban Toxic Chemicals. ProPublica. 2022. Available online: https://www.propublica.org/article/toxic-chemicals-epa-regulation-failures (accessed on 27 February 2024).
- Oprea, N.; Ardito, V.; Ciani, O. Implementing shared decision-making interventions in breast cancer clinical practice: A scoping review. BMC Med. Inform. Decis. Mak. 2023, 23, 164. [Google Scholar] [CrossRef] [PubMed]
- Maloney, E.K.; D’Agostino, T.A.; Heerdt, A.; Dickler, M.; Li, Y.; Ostroff, J.S.; Bylund, C.L. Sources and types of online information that breast cancer patients read and discuss with their doctors. Palliat. Support Care 2015, 13, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Hesse, B.W.; Nelson, D.E.; He, M.P. Trust and Sources of Health Information: The Impact of the Internet and Its Implications for Health Care Providers: Findings From the First Health Information National Trends Survey. Arch. Intern. Med. 2005, 165, 2618–2624. [Google Scholar] [CrossRef] [PubMed]
- Siddiq, H.; Jones, F.; Magnes, Z.; Booker-Vaughns, J.; Young-Brinn, A.; Williams, C.; Washington, M.; Agonafer, E.; Solomon, O.; Oliva, A.; et al. Unsing community-partnered participatory research to value the “community lens” and promote equity in community-academic partnerships. Health Equity 2023, 7, 543–554. [Google Scholar] [CrossRef] [PubMed]
- Jones, L. Commentary: 25 years of community-partnered participatory research. Ethn. Dis. 2018, 28 (Suppl. S2), 291–294. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.M.; Nickson, D.; Hetrick, C.; Wilson-Clark, D. “Nothing about us without us”: Tending to emancipatory ideologies and transformations in participatory research partnerships. Qualit. Res. 2023, 23, 1319–1341. [Google Scholar] [CrossRef]
- Albert, A.; Islam, S.; Haklay, M. Nothing about us without us: A co-production strategy for communities, researchers and stakeholders to identify ways oof improving health and reducing inequalities. Health Expect 2023, 26, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Nawaz, S.; Khan, E.; Islam, S. Nothing about us, without us: Is for us. Res. Involv. Engag. 2022, 8, 39. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Characteristic | Number (%) | |
|---|---|---|
| Stakeholder category | Community member | 194 (55.3) |
| Healthcare practitioner | 85 (24.2) | |
| Academic/Researcher | 37 (10.5) | |
| Policy expert/Advocate | 34 (9.7) | |
| No response | 1 (0.3) | |
| Region of California | Northern CA | 69 (19.7) |
| San Francisco Bay Area | 75 (21.4) | |
| Central Coast | 28 (8.0) | |
| Gold Country | 49 (14.0) | |
| Central Valley | 24 (6.8) | |
| Inland Valley (Imperial Valley) | 25 (7.1) | |
| Los Angeles County | 51 (14.5) | |
| San Diego and Orange Counties | 30 (8.6) | |
| Race/ethnicity | White | 191 (54.4) |
| Black/African American | 66 (18.8) | |
| Latina/Hispanic/Latinx | 48 (13.7) | |
| American Indigenous/Indian/Native Alaskan | 13 (3.7) | |
| Asian | 13 (3.7) | |
| Native Hawai’ian/Pacific Islander | 8 (2.3) | |
| Bi- or multi-racial | 7 (2.0) | |
| No response | 5 (1.4) | |
| Age (years) | ≤25 | 0 (0) |
| 26–40 | 224 (63.8) | |
| 41–59 | 94 (26.8) | |
| 60+ | 22 (6.3) | |
| No response | 11 (3.1) | |
| Gender identity | Female/Woman | 275 (78.4) |
| Male/Man | 66 (18.8) | |
| Gender non-conforming (non-binary, gender queer, gender fluid) | 2 (0.6) | |
| Transgender | 0 (0.0) | |
| No response | 8 (2.3) | |
| Living with a diagnosis of breast cancer? | Yes | 94 (26.8) |
| No | 256 (72.9) | |
| No response | 1 (0.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gray, J.; Petrucci, C.; Engel, C.; Green-Washington, N.; Buermeyer, N. Development of Systemic Interventions to Decrease Breast Cancer Risk: A Group Concept Mapping Study. Int. J. Environ. Res. Public Health 2024, 21, 318. https://doi.org/10.3390/ijerph21030318
Gray J, Petrucci C, Engel C, Green-Washington N, Buermeyer N. Development of Systemic Interventions to Decrease Breast Cancer Risk: A Group Concept Mapping Study. International Journal of Environmental Research and Public Health. 2024; 21(3):318. https://doi.org/10.3390/ijerph21030318
Chicago/Turabian StyleGray, Janet, Carrie Petrucci, Connie Engel, Nyisha Green-Washington, and Nancy Buermeyer. 2024. "Development of Systemic Interventions to Decrease Breast Cancer Risk: A Group Concept Mapping Study" International Journal of Environmental Research and Public Health 21, no. 3: 318. https://doi.org/10.3390/ijerph21030318
APA StyleGray, J., Petrucci, C., Engel, C., Green-Washington, N., & Buermeyer, N. (2024). Development of Systemic Interventions to Decrease Breast Cancer Risk: A Group Concept Mapping Study. International Journal of Environmental Research and Public Health, 21(3), 318. https://doi.org/10.3390/ijerph21030318