

Neuropsychological Effects of the Lockdown Due to the COVID-19 Pandemic on Patients with Alzheimer’s Disease and Their Caregivers: The “ACQUA” (Alzheimer–COVID QUArantine Questionnaire) Study

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
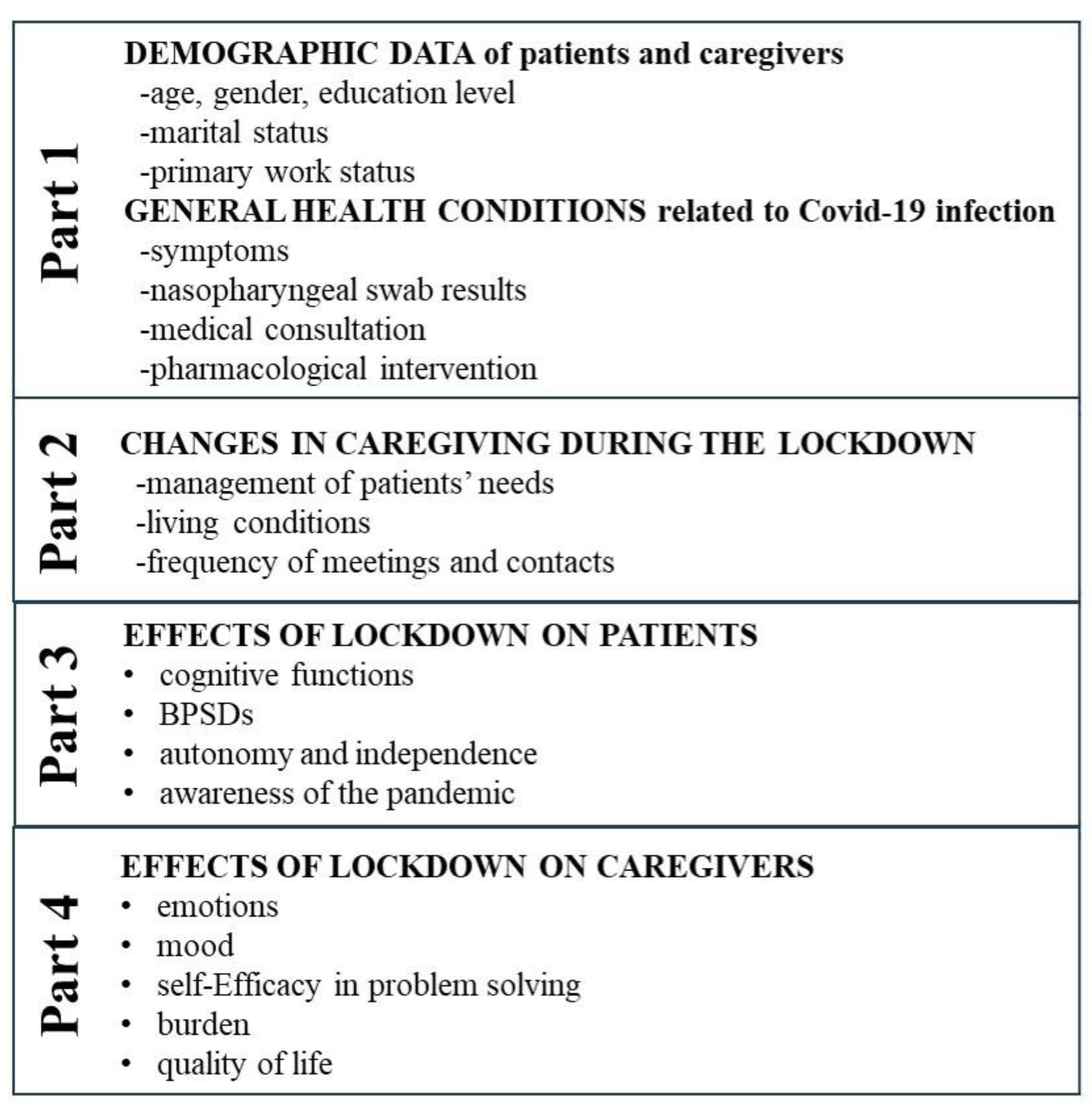
2.2. Alzheimer–COVID QUArantine (ACQUA) Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Demographic Data of the Study Sample and General Health Condition of the Patients
3.2. Daily Organization of Caregiving During the Pandemic and Lockdown
3.3. Effects of the Lockdown on the Patients
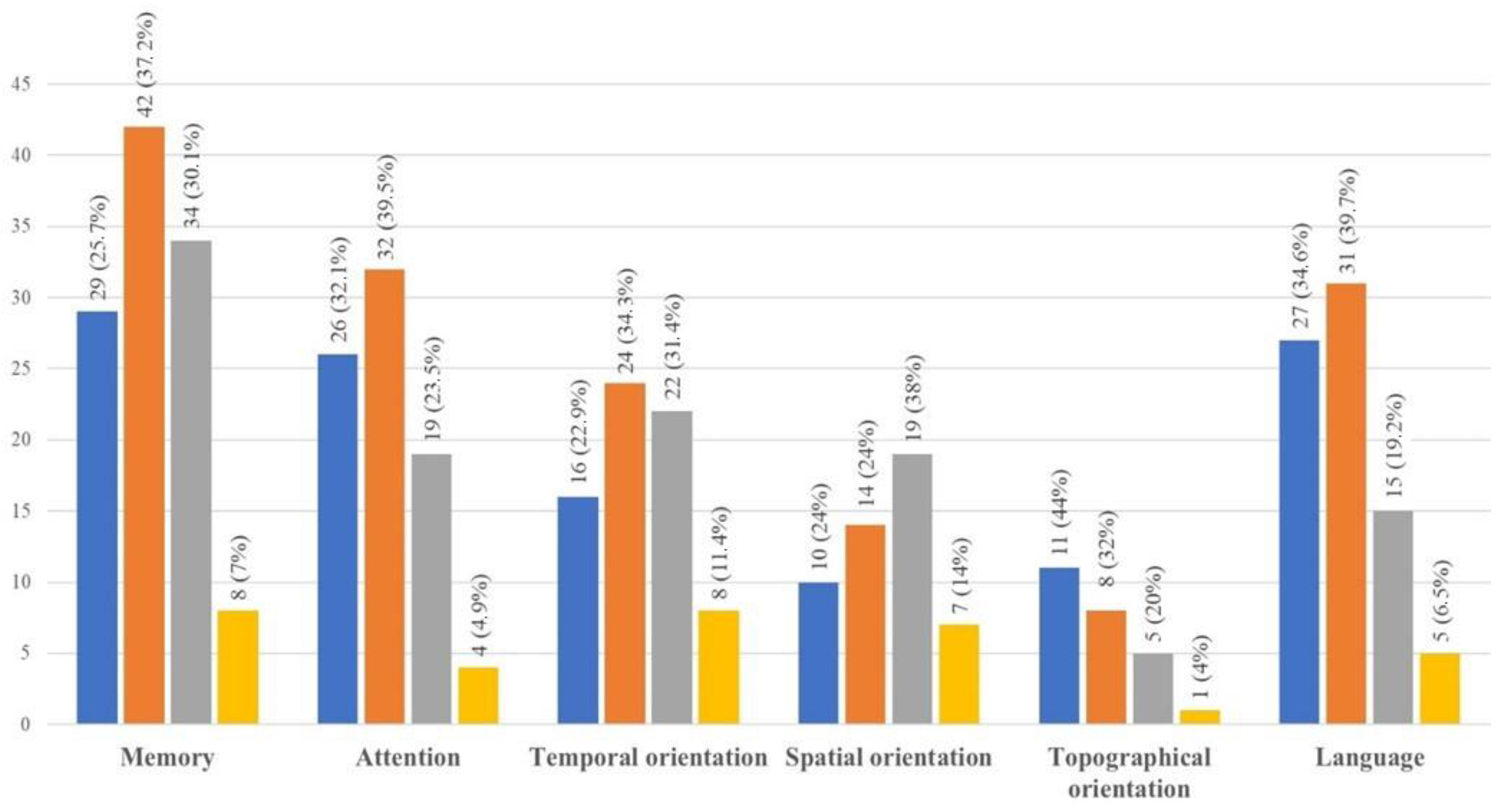
3.3.1. Cognitive Functions
3.3.2. Levels of Functional Independence
3.3.3. Awareness of COVID-19 Pandemic
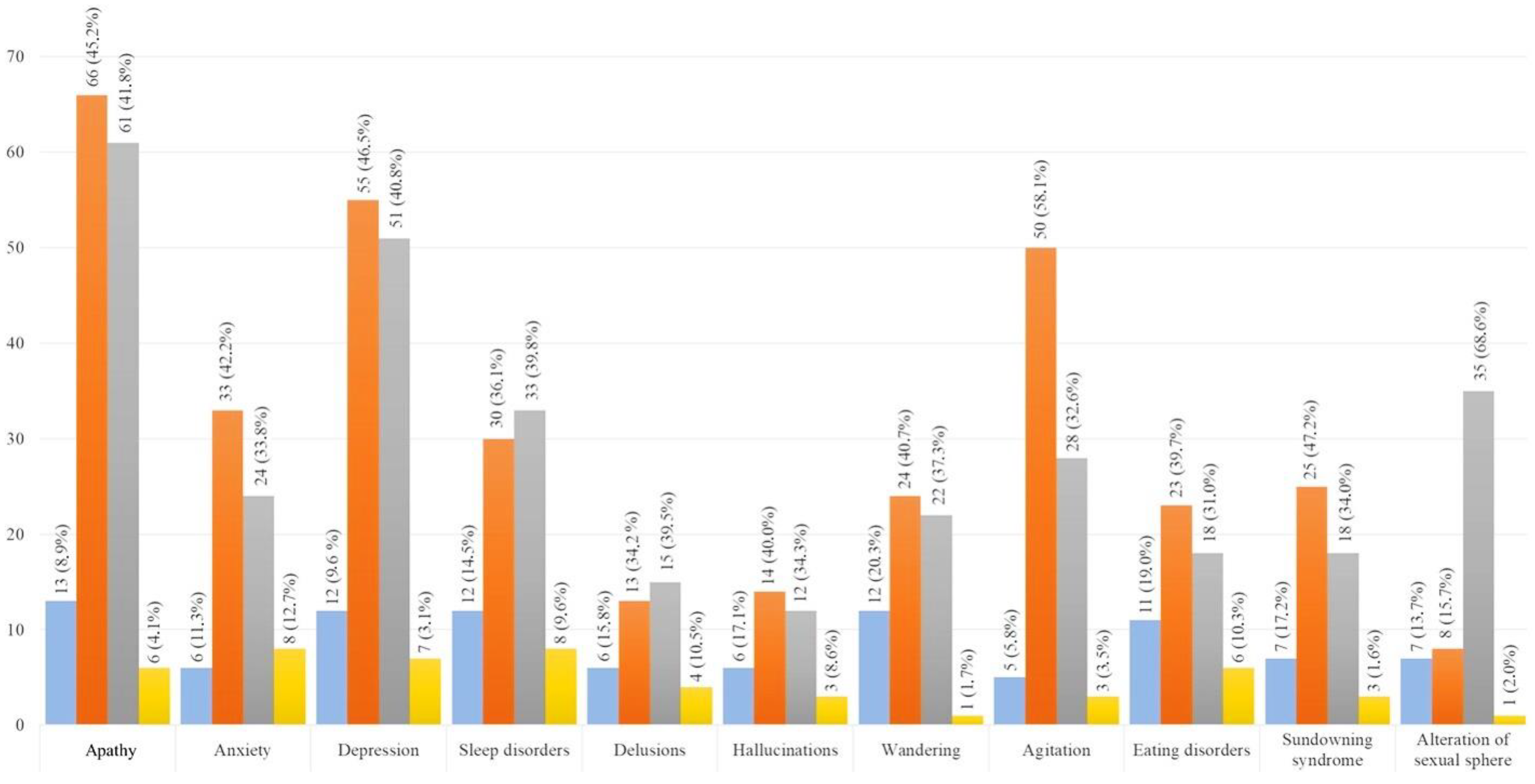
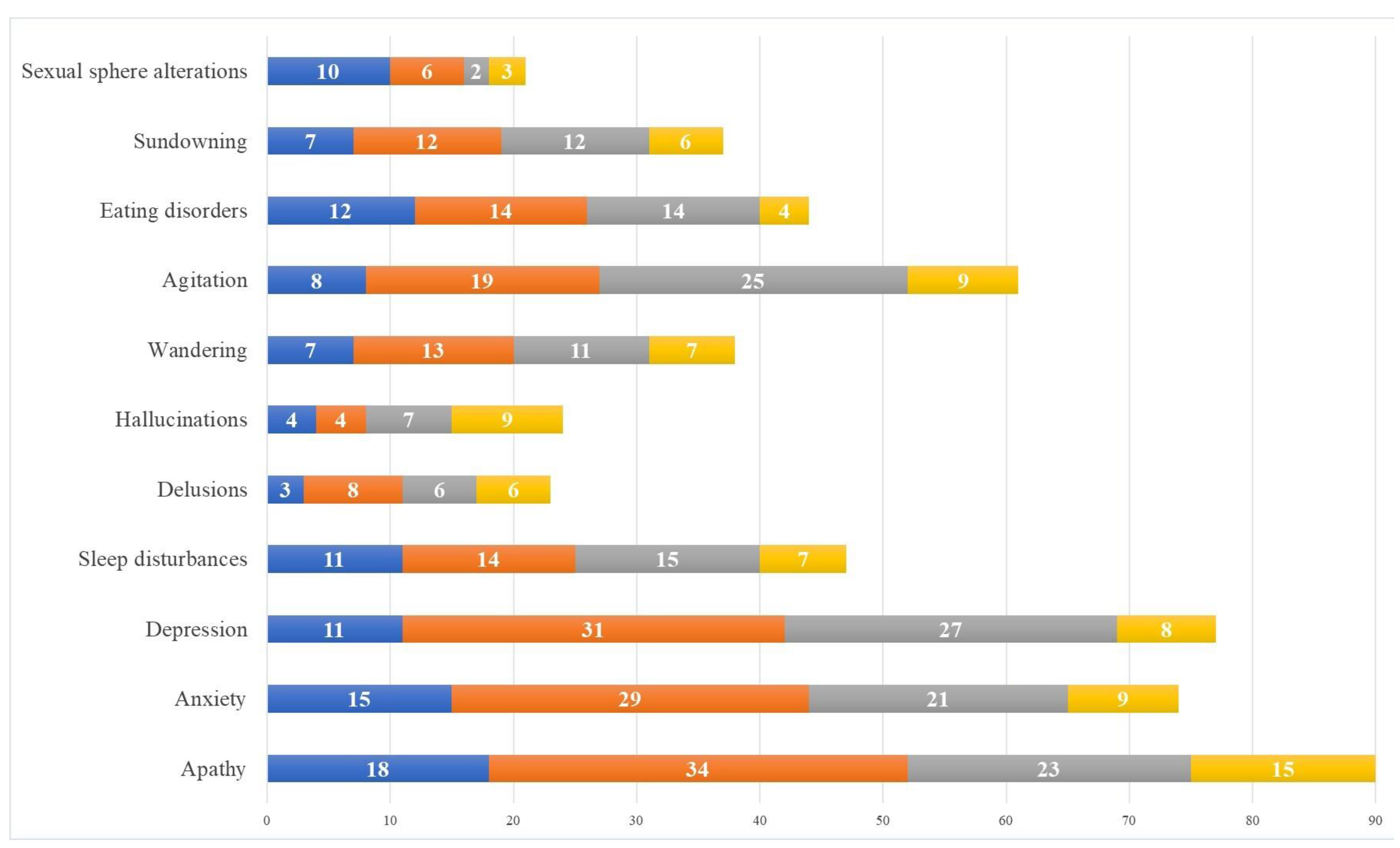
3.3.4. Behavioral and Psychological Symptoms of Dementia
3.4. Effects of the Lockdown on Caregivers
3.4.1. Mood and Emotions
3.4.2. Caregiver Burden, Self-Efficacy in Problem-Solving, and Quality of Life
3.4.3. Multivariable Logistic Regressions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Iodice, F.; Cassano, V.; Rossini, P.M. Direct and indirect neurological, cognitive, and behavioral effects of COVID-19 on the healthy elderly, mild-cognitive-impairment, and Alzheimer’s disease populations. Neurol Sci. 2021, 42, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Hugo, J.; Ganguli, M. Dementia and cognitive impairment: Epidemiology, diagnosis, and treatment. Clin. Geriatr. Med. 2014, 30, 421–442. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.-F.; Tan, L.; Wang, H.-F.; Jiang, T.; Tan, M.-S.; Tan, L.; Xu, W.; Li, J.-Q.; Wang, J.; Lai, T.-J.; et al. The prevalence of neuropsychiatric symptoms in Alzheimer’s disease: Systematic review and meta-analysis. J. Affect. Disord. 2016, 190, 264–271. [Google Scholar] [CrossRef]
- Hersi, M.; Irvine, B.; Gupta, P.; Gomes, J.; Birkett, N.; Krewski, D. Risk factors associated with the onset and progression of Alzheimer’s disease: A systematic review of the evidence. Neurotoxicology 2017, 61, 143–187. [Google Scholar] [CrossRef]
- Guure, C.B.; Ibrahim, N.A.; Adam, M.B.; Said, S.M. Impact of Physical Activity on Cognitive Decline, Dementia, and Its Subtypes: Meta-Analysis of Prospective Studies. BioMed Res. Int. 2017, 2017, 9016924. [Google Scholar] [CrossRef]
- Cheng, S.T. Dementia Caregiver Burden: A Research Update and Critical Analysis. Curr. Psychiatry Rep. 2017, 19, 64. [Google Scholar] [CrossRef]
- Folstein, M.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State” a Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Rico-Blázquez, M.; Sánchez-Ruano, R.; Oter-Quintana, C.; Polentinos-Castro, E.; Martín-García, Á.; Otones-Reyes, P.; González-Beltrán, D.; Martínez-Marcos, M. Family Caregivers’ Experiences during the COVID-19 Pandemic: Qualitative Study. Healthcare 2024, 12, 970. [Google Scholar] [CrossRef]
- Mukherjee, R.; Bhattacharyya, B.; Mukherjee, A.; Das, G.; Das, S.; Biswas, A. Exploring Caregiver Burden and Health Condition of Dementia Patients during Lockdown due to COVID-19 Pandemic. Ann. Indian Acad. Neurol. 2022, 25, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Rising, K.L.; Salcedo, V.J.; Amadio, G.; Casten, R.; Chang, A.; Gentsch, A.; O’Hayer, C.V.; Sarpoulaki, N.; Worster, B.; Gerolamo, A.M. Living Through the Pandemic: The Voices of Persons with Dementia and Their Caregivers. J. Appl. Gerontol. 2022, 41, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Rainero, I.; Bruni, A.C.; Marra, C.; Cagnin, A.; Bonanni, L.; Cupidi, C.; Laganà, V.; Rubino, E.; Vacca, A.; Di Lorenzo, R.; et al. The Impact of COVID-19 Quarantine on Patients with Dementia and Family Caregivers: A Nation-Wide Survey and Family Caregivers: A Nation-Wide Survey. Front. Aging Neurosci. 2020, 12, 625781. [Google Scholar]
- Bruvik, F.K.; Ulstein, I.D.; Ranhoff, A.H.; Engedal, K. The effect of coping on the burden in family carers of persons with dementia. Aging Ment. Health 2013, 17, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Foubert-Samier, A.; Le Goff, M.; Helmer, C.; Pérès, K.; Orgogozo, J.M.; Barberger-Gateau, P.; Amieva, H.; Dartigues, J.F. Change in leisure and social activities and risk of dementia in elderly cohort. J. Nutr. Health Aging 2014, 18, 876–882. [Google Scholar] [CrossRef]
- Marioni, R.E.; Proust-Lima, C.; Amieva, H.; Brayne, C.; Matthews, F.E.; Dartigues, J.F.; Jacqmin-Gadda, H. Social activity, cognitive decline and dementia risk: A 20-year prospective cohort study. BMC Public Health 2015, 15, 1089. [Google Scholar] [CrossRef]
- Di Santo, S.G.; Franchini, F.; Filiputti, B.; Martone, A.; Sannino, S. The Effects of COVID-19 and Quarantine Measures on the Lifestyles and Mental Health of People Over 60 at Increased Risk of Dementia. Front. Psychiatry 2020, 11, 578628. [Google Scholar] [CrossRef]
- Manca, R.; De Marco, M.; Venneri, A. The Impact of COVID-19 Infection and Enforced Prolonged Social Isolation on Neuropsychiatric Symptoms in Older Adults with and Without Dementia: A Review. Front. Psychiatry 2020, 11, 585540. [Google Scholar] [CrossRef]
- Cagnin, A.; Di Lorenzo, R.; Marra, C.; Bonanni, L.; Cupidi, C.; Laganà, V.; Rubino, E.; Vacca, A.; Provero, P.; Isella, V.; et al. Behavioral and Psychological Effects of Coronavirus Disease-19 Quarantine in Patients with Dementia. Front. Psychiatry 2020, 11, 578015. [Google Scholar] [CrossRef]
- Kang, S. Predictors of emotional strain among spouse and adult child caregivers. J. Gerontol. Soc. Work. 2006, 47, 107–131. [Google Scholar] [CrossRef]
- Carruth, A.K.; Tate, U.S.; Moffett, B.S.; Hill, K. Reciprocity, emotional well-being, and family functioning as determinants of family satisfaction in caregivers of elderly parents. Nurs. Res. 1997, 46, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Altieri, M.; Santangelo, G. The Psychological Impact of COVID-19 Pandemic and Lockdown on Caregivers of People with Dementia. Am. J. Geriatr. Psychiatry: Off. J. Am. Assoc. Geriatr. Psychiatry 2021, 29, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.F.; Hwang, W.S.; Lee, J.J.; Wang, W.F.; Huang, L.C.; Huang, L.K.; Lee, W.J.; Sung, P.S.; Liu, Y.C.; Hsu, C.C.; et al. Predictors of caregiver burden in aged caregivers of demented older patients. BMC Geriatr. 2021, 21, 59. [Google Scholar] [CrossRef] [PubMed]
- Chiao, C.Y.; Wu, H.S.; Hsiao, C.Y. Caregiver burden for informal caregivers of patients with dementia: A systematic review. Int. Nurs. Rev. 2015, 62, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Novick, G. Is there a bias against telephone interviews in qualitative research? Res. Nurs. Health 2008, 31, 391–398. [Google Scholar] [CrossRef]
- Boland, M.; Sweeney, M.; Scallan, E.; Harrington, M.; Staines, A. Emerging advantages and drawbacks of telephone surveying in public health research in Ireland and the U.K. BMC Public Health 2006, 6, 208. [Google Scholar] [CrossRef]
- Suárez-González, A.; Rajagopalan, J.; Livingston, G.; Alladi, S. The effect of COVID-19 isolation measures on the cognition and mental health of people living with dementia: A rapid systematic review of one year of quantitative evidence. EClinicalMedicine 2021, 39, 101047. [Google Scholar] [CrossRef]
- Soysal, P.; Veronese, N.; Smith Lee Chen, Y.; Soylemez, B.A.; Coin, A.; Religa, D.; Välimäki, T.; Alves, M.; Shenkin, S.D. The Impact of the COVID-19 Pandemic on the Psychological Well-Being of Caregivers of People with Dementia or Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Geriatrics 2023, 8, 97. [Google Scholar] [CrossRef]
- Bailey, C.; Guo, P.; MacArtney, J.; Finucane, A.; Swan, S.; Meade, R.; Wagstaff, E. The Experiences of Informal Carers during the COVID-19 Pandemic: A Qualitative Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 13455. [Google Scholar] [CrossRef]
- García-Casal, J.A.; Loizeau, A.; Csipke, E.; Franco-Martín, M.; Perea-Bartolomé, M.V.; Orrell, M. Computer-based cognitive interventions for people living with dementia: A systematic literature review and meta-analysis. Aging Ment. Health 2017, 21, 454–467. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Total (n = 197) |
| Age (years, mean ± SD) Sex (female, %) | 77.2 ± 6.8 124 (63%) |
| Education (years, mean ± SD) -primary/lower secondary school -high school -undergraduate/postgraduate | 9.7 ± 4.9 116 (58.9%) 69 (35%) 12 (6.1%) |
| MMSE (mean ± SD) Marital status (married, %) Widowed/separated (mean ± SD) | 20.1 ± 2.4 131 (66.5%) 66 (33.5%) |
| Caregivers | Total (n = 197) |
| Age (years, mean ± SD) Sex (female, %) | 60.1 ± 14.0 127 (64.5%) |
| Education (years, mean ± SD) -primary/secondary school -high school -undergraduate/postgraduate | 13.9 ± 4.2 74 (37.6%) 93 (47.2%) 30 (15.2%) |
| Marital status (married, %) | 151 (76.7%) |
| Widowed/separated (%) Cohabitant before lockdown (%) | 46 (23.3%) 76 (37.1%) |
| Degree of kinship | n |
| Spouse | 66 (33.5%) |
| Son/daughter | 114 (57.8%) |
| Other | 17 (8.7%) |
| Need for Medical Consultation | n | % |
|---|---|---|
| General practitioner | 61 | 31.0% |
| Other specialized physicians | 7 | 3.6% |
| Both | 10 | 5.1% |
| No need | 129 | 65.5% |
| Activities of Daily Living | Improved | Stable | Worsened |
|---|---|---|---|
| Use of the telephone | 15 | 144 | 38 |
| Practicing hobbies | 12 | 159 | 26 |
| Housekeeping | 8 | 152 | 37 |
| Use of household appliances | 4 | 180 | 13 |
| Therapy management | 2 | 170 | 25 |
| Awareness of the Pandemic | Yes | Not |
|---|---|---|
| Remembers that the COVID-19 emergency is underway | 104 (52.8%) | 93 (47.2%) |
| Engages in appropriate behaviors without awareness | 10 (5.1%) | 187 (94.9%) |
| Remembers what they can/cannot do | 160 (81.2%) | 37 (18.8%) |
| Speaks spontaneously about confinement/restrictions | 161 (81.7%) | 36 (18.3%) |
| Depressive Symptoms | n | % |
|---|---|---|
| None | 95 | 48.2% |
| Low mood or sadness | 68 | 34.5% |
| Feeling tearful | 57 | 28.9% |
| Having less motivation or interests | 48 | 24.4% |
| Feeling irritable and intolerant of others | 28 | 14.2% |
| Feeling hopeless and helpless | 25 | 12.7% |
| Feeling guilt-ridden | 22 | 11.2% |
| Having low self-esteem | 10 | 5.1% |
| Emotional Experience | |||
|---|---|---|---|
| Less than before | As before | More than before | |
| Dealing with unpleasant emotions | 5 (2.5%) | 92 (46.7%) | 100 (50.8%) |
| Lack of emotional closeness to people | 4 (2.0%) | 98 (49.7%) | 95 (48.2%) |
| Lack of companionship | 7 (3.5%) | 70 (35.5%) | 120 (61.0%) |
| Feeling alone in solving problems | 12 (6.0%) | 130 (66.0%) | 55 (28.0%) |
| Time to be on their own | 77 (39.1%) | 102 (51.8%) | 18 (9.1%) |
| Activities for their well-being | 91 (46.2%) | 60 (30.5%) | 46 (23.3%) |
| Emerging Feelings Towards the Patients | Positive | Negative |
|---|---|---|
| No | n = 72 (36.5%) | n = 139 (70.5%) |
| Yes | n = 125 (63.5%) | n = 58 (30.5) |
| -Sometimes | n = 39 (19.8%) | n = 31 (15.8%) |
| -Often | n = 37 (18.8%) | n = 9 (4.5%) |
| -Very often | n = 40 (20.3%) | n = 14 (7.2%) |
| -Always/everyday | n = 9 (4.6%) | n = 4 (2.0%) |
| Change in Caregivers’ Burden | n | % |
|---|---|---|
| No | 87 | 44.2% |
| Less than before | 13 | 6.6% |
| More than before | 97 | 49.2% |
| -Very mildly | 18 | 9.0% |
| -Mildly | 29 | 14.6% |
| -Moderately | 30 | 15.1% |
| -Severely | 20 | 10.5% |
| Change in Caregivers’ Quality of Life | n | % |
|---|---|---|
| No | 50 | 25.4% |
| Yes | 147 | 75.6% |
| -Very mild | 38 | 19.3% |
| -Mild | 38 | 19.3% |
| -Moderate | 57 | 28.9% |
| -Severe | 14 | 7.1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trebbastoni, A.; Margiotta, R.; D’Antonio, F.; Barbetti, S.; Canevelli, M.; Diana, S.; Di Vita, A.; Imbriano, L.; Sepe Monti, M.; Talarico, G.; et al. Neuropsychological Effects of the Lockdown Due to the COVID-19 Pandemic on Patients with Alzheimer’s Disease and Their Caregivers: The “ACQUA” (Alzheimer–COVID QUArantine Questionnaire) Study. Int. J. Environ. Res. Public Health 2024, 21, 1622. https://doi.org/10.3390/ijerph21121622
Trebbastoni A, Margiotta R, D’Antonio F, Barbetti S, Canevelli M, Diana S, Di Vita A, Imbriano L, Sepe Monti M, Talarico G, et al. Neuropsychological Effects of the Lockdown Due to the COVID-19 Pandemic on Patients with Alzheimer’s Disease and Their Caregivers: The “ACQUA” (Alzheimer–COVID QUArantine Questionnaire) Study. International Journal of Environmental Research and Public Health. 2024; 21(12):1622. https://doi.org/10.3390/ijerph21121622
Chicago/Turabian StyleTrebbastoni, Alessandro, Roberta Margiotta, Fabrizia D’Antonio, Sonia Barbetti, Marco Canevelli, Sofia Diana, Antonella Di Vita, Letizia Imbriano, Micaela Sepe Monti, Giuseppina Talarico, and et al. 2024. "Neuropsychological Effects of the Lockdown Due to the COVID-19 Pandemic on Patients with Alzheimer’s Disease and Their Caregivers: The “ACQUA” (Alzheimer–COVID QUArantine Questionnaire) Study" International Journal of Environmental Research and Public Health 21, no. 12: 1622. https://doi.org/10.3390/ijerph21121622
APA StyleTrebbastoni, A., Margiotta, R., D’Antonio, F., Barbetti, S., Canevelli, M., Diana, S., Di Vita, A., Imbriano, L., Sepe Monti, M., Talarico, G., Guariglia, C., & Bruno, G. (2024). Neuropsychological Effects of the Lockdown Due to the COVID-19 Pandemic on Patients with Alzheimer’s Disease and Their Caregivers: The “ACQUA” (Alzheimer–COVID QUArantine Questionnaire) Study. International Journal of Environmental Research and Public Health, 21(12), 1622. https://doi.org/10.3390/ijerph21121622