
Multivariate Techniques for Monitoring Susceptible, Exposed, Infected, Recovered, Death, and Vaccination Model Parameters for the COVID-19 Pandemic for Qatar




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
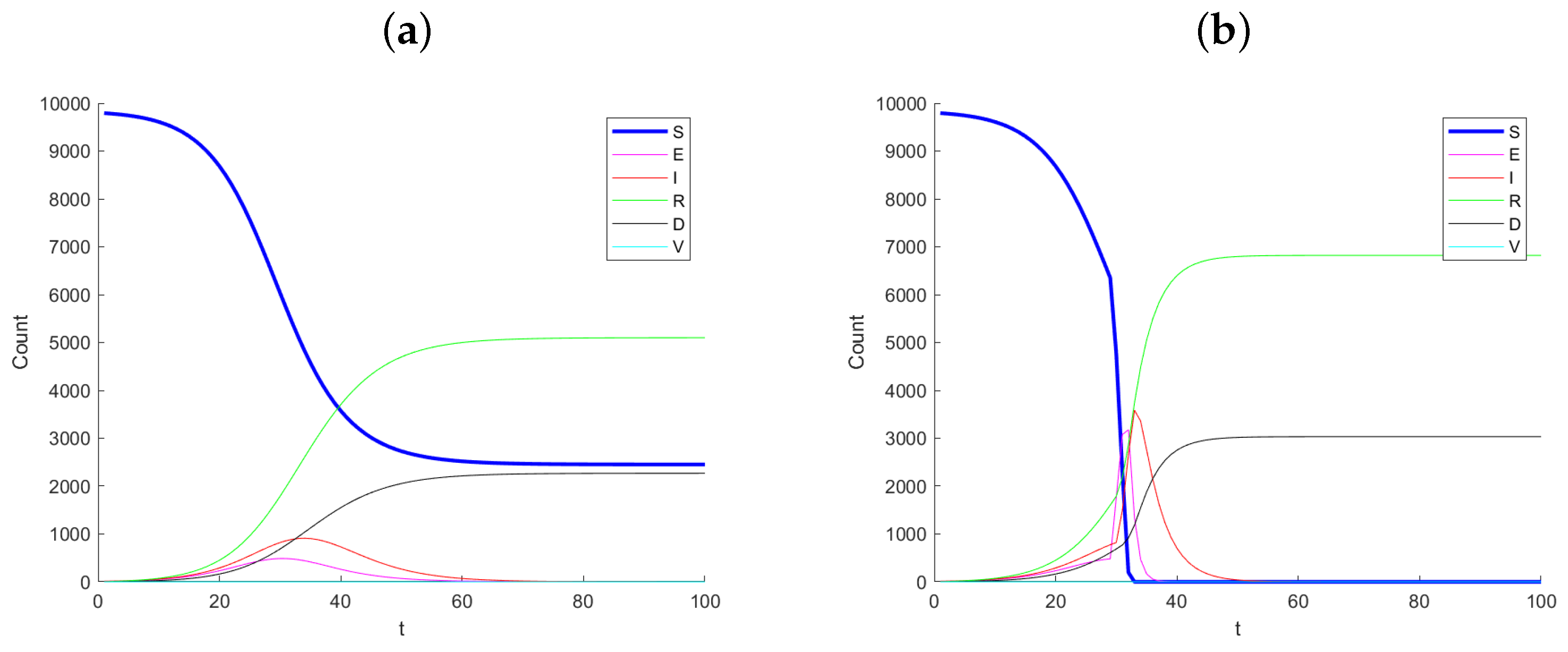
2. The SEIRDV Model for Predicting Outcomes with Vaccination
- : Expected number of susceptible individuals at time t.
- : Expected number of exposed individuals at time t.
- : Expected number of infected individuals at time t.
- : Expected number of recovered individuals at time t.
- : Expected number of deceased individuals at time t.
3. Multivariate Profile Monitoring Techniques
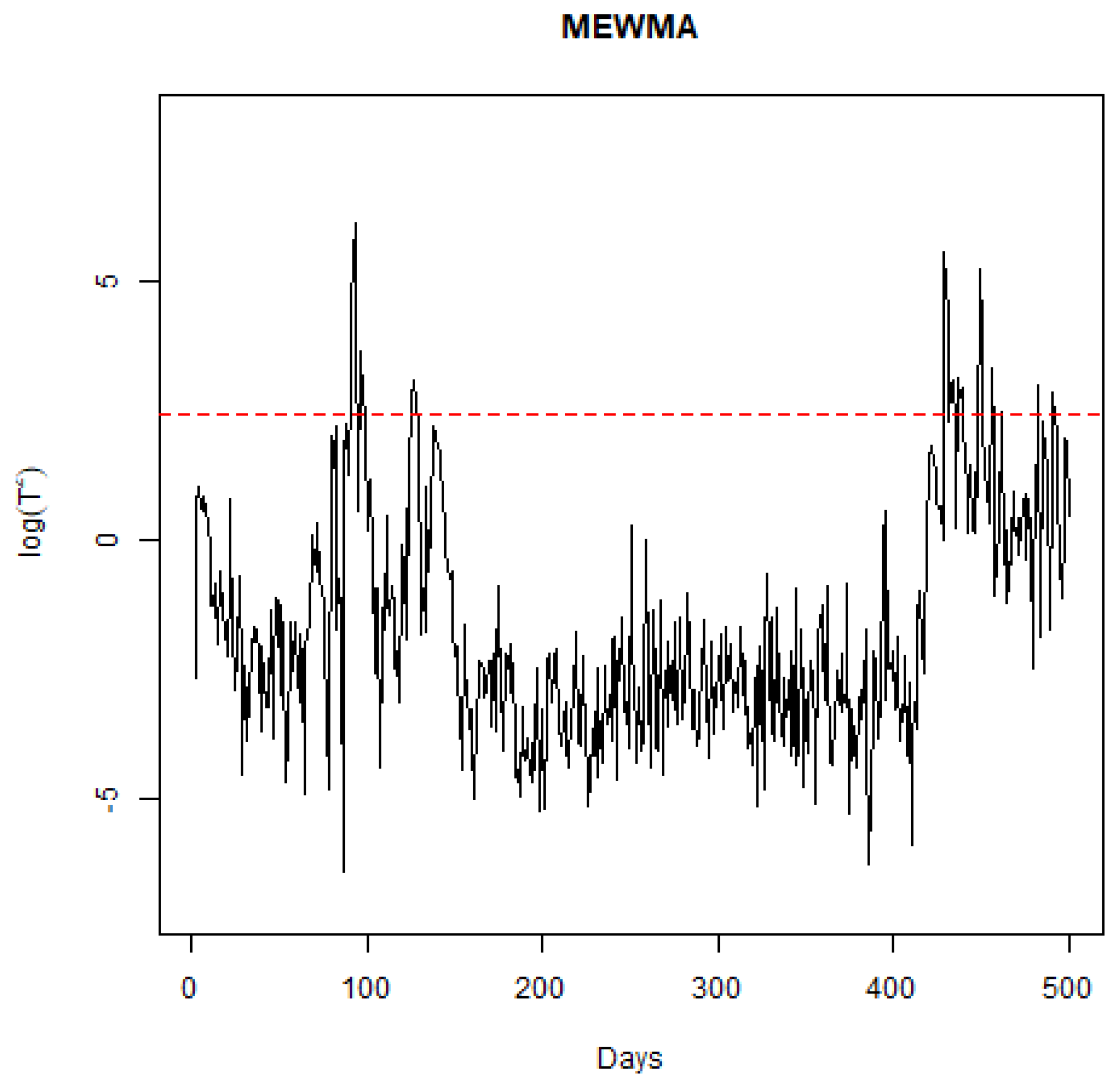
3.1. The MEWMA Control Chart
3.2. The MCUSUM Control Chart
- Initialize the MCUSUM control chart with an initial estimate of the parameters based on historical data. This estimate can be obtained using prior information or initial modeling.
- Continuously collect data on the number of infected individuals (), recovered individuals (), deaths (), and vaccinated individuals () at each time point, t. These observed data points are used to update the model parameters and the MCUSUM chart.
- Employ a Bayesian methodology, such as the sequential sampling with particle augmentation technique, to estimate the time-varying parameters , , , and at each time step. This technique updates the posterior distribution of the parameters based on the observed data, providing a more accurate estimate of the parameters over time.
- Calculate the MCUSUM statistics for each parameter to monitor deviations from the expected values.
- Set control limits for each parameter, tailored to the desired levels of sensitivity and specificity. These limits are critical for determining when a parameter’s change is statistically significant and warrants further attention.
- Continuously monitor the MCUSUM statistics for each parameter. If any of the statistics exceed the defined control limits, it indicates a potential shift or change in the model parameters. At this point, further investigation and action may be required to understand the underlying causes of the change.
- As new data become available, continuously update the parameter estimates and the MCUSUM chart. This dynamic adjustment allows for real-time monitoring of changes in the pandemic’s dynamics or the effectiveness of health interventions, facilitating timely decision-making.
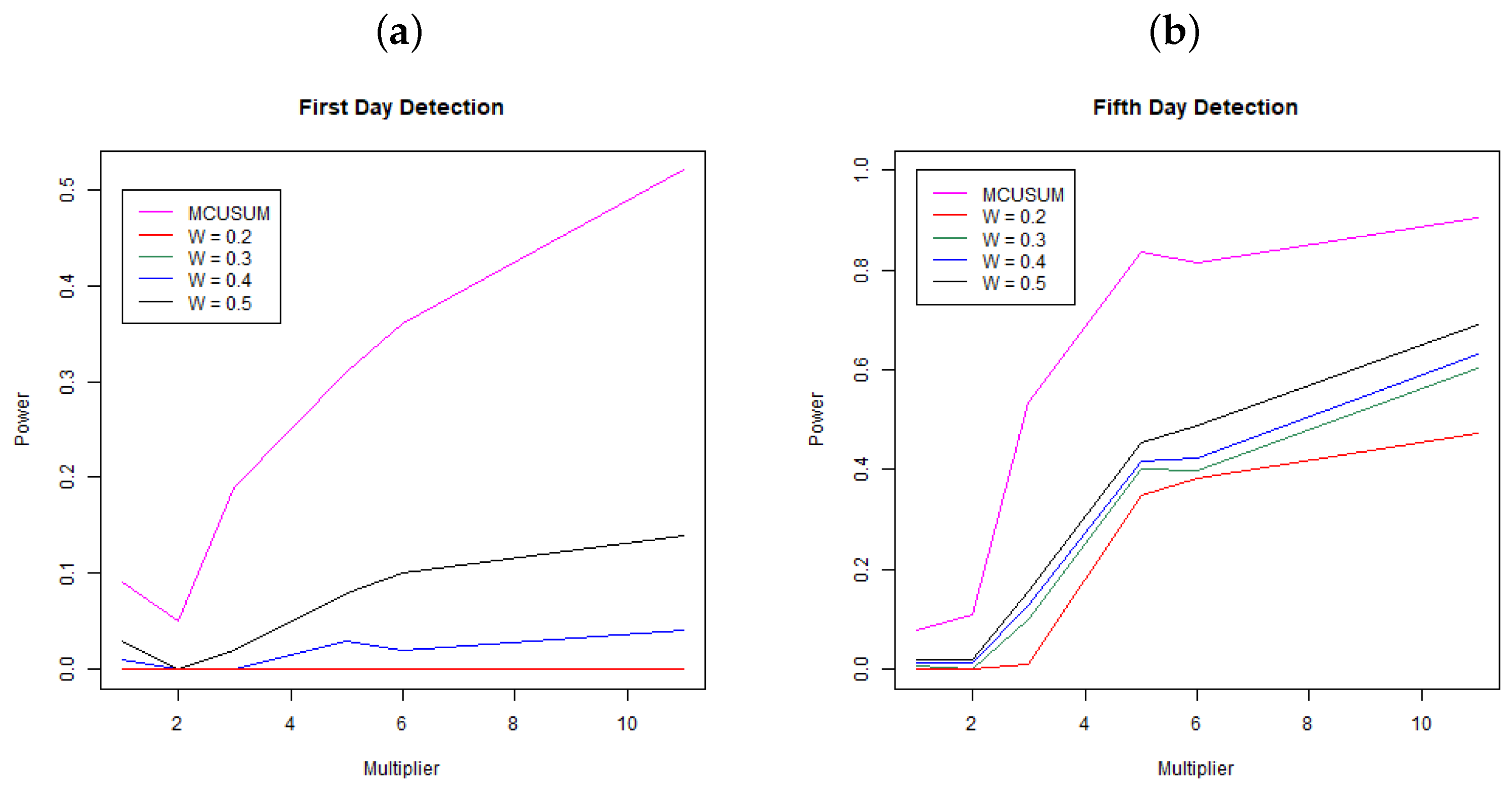
4. Simulation Study
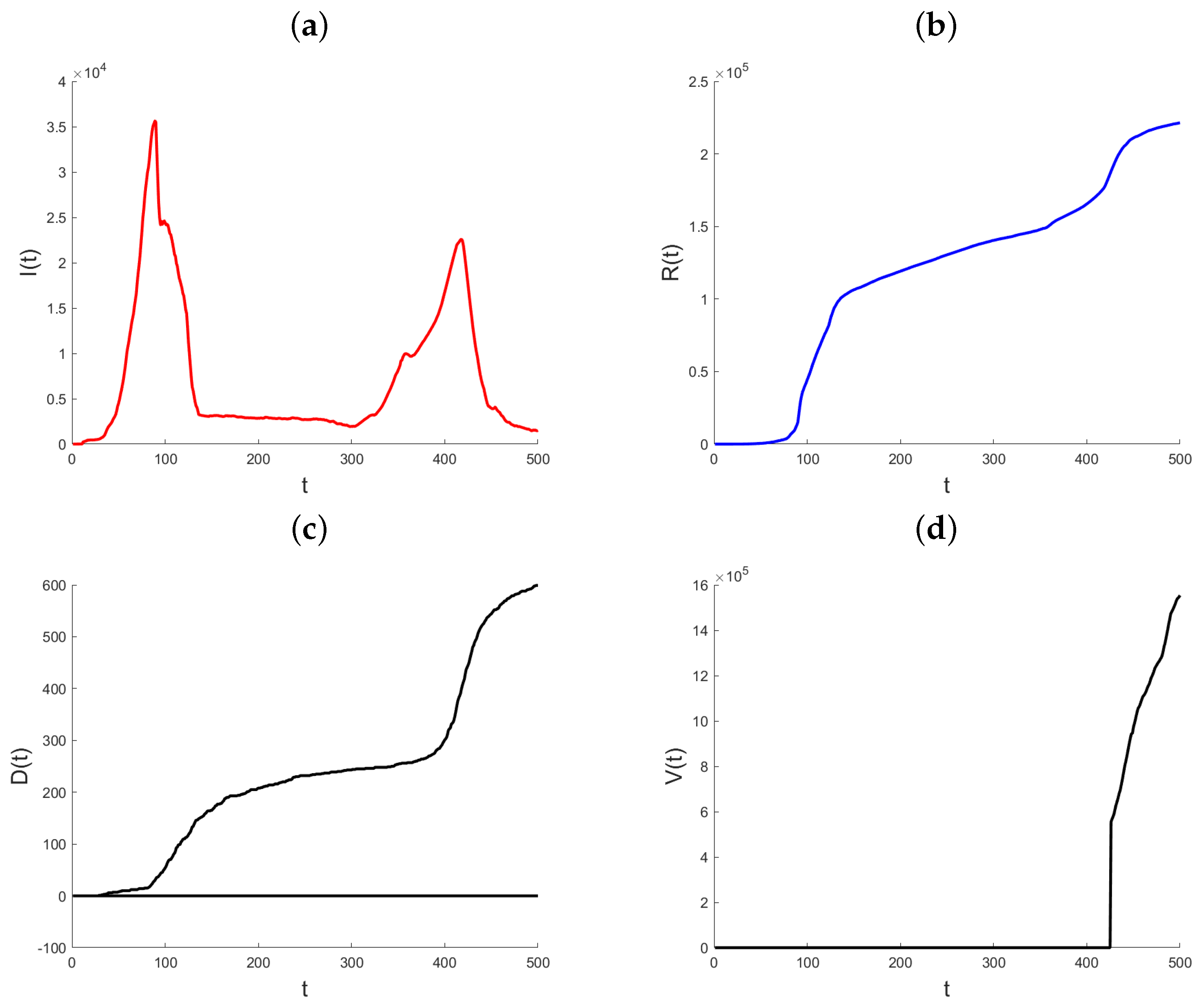
5. Real Application: State of Qatar
5.1. A Comprehensive Analysis of Qatar’s Response to the Pandemic
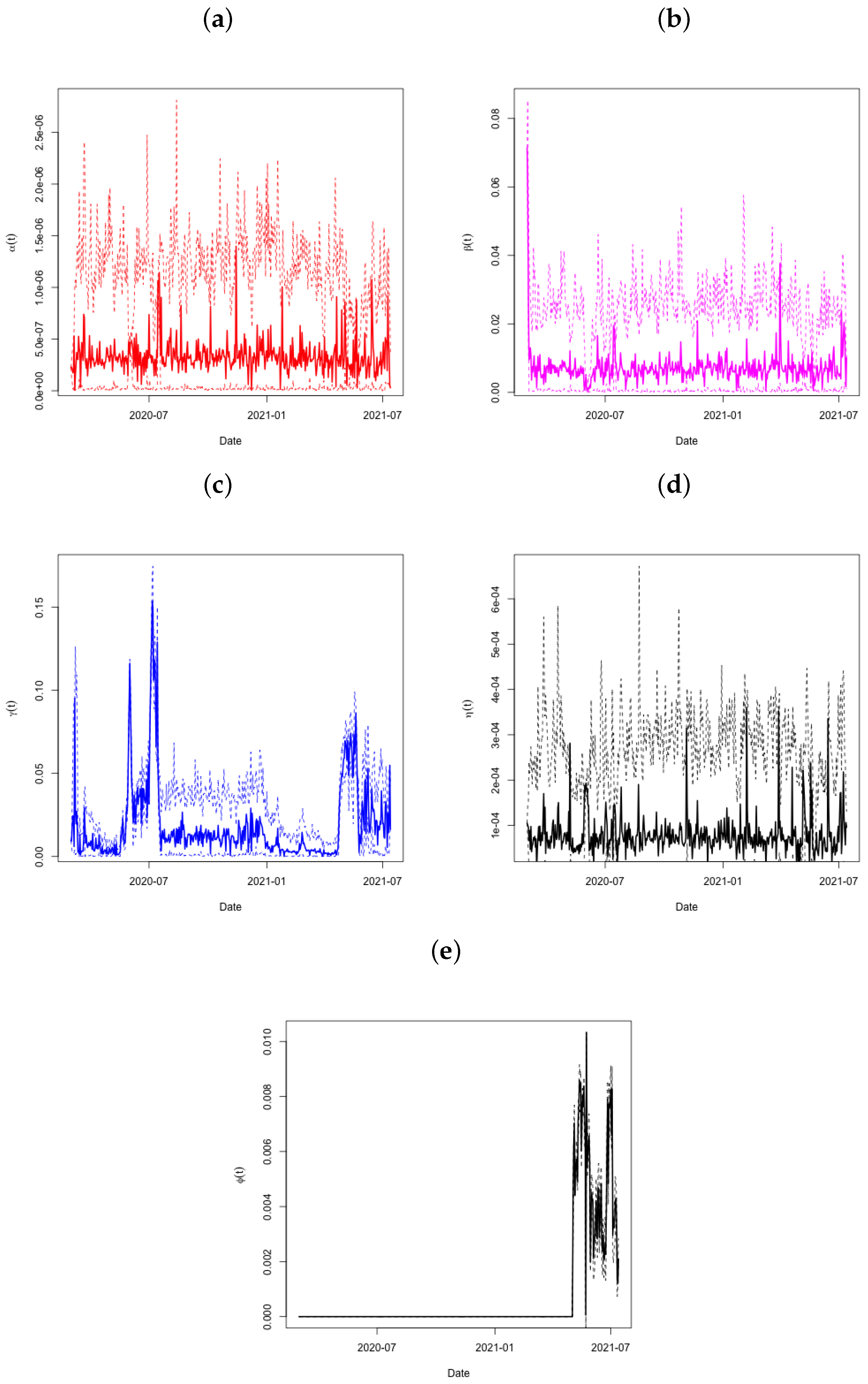
5.2. Results of the Analysis
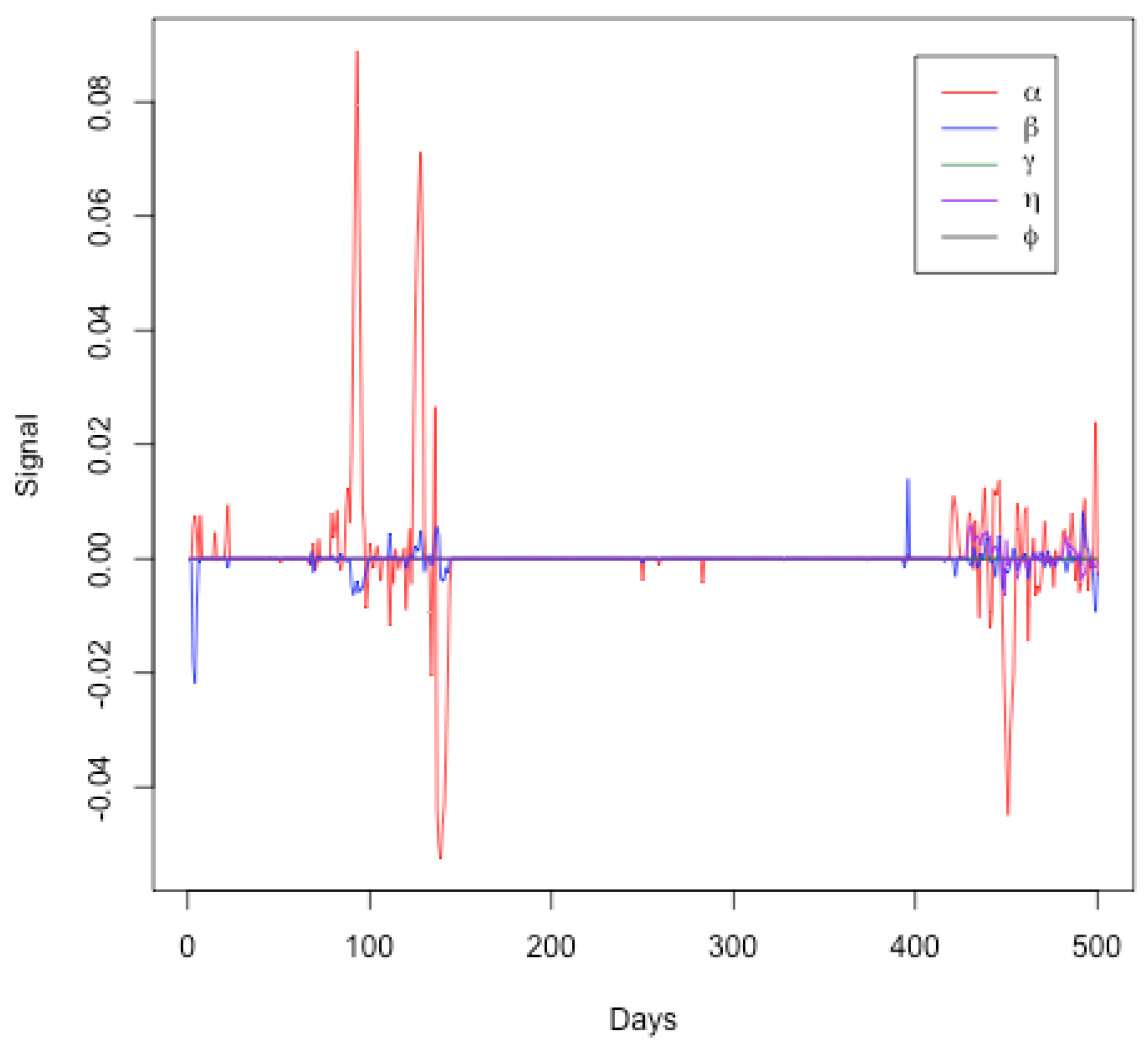
- Initial Period (Days 0–100): The parameter (red line) shows significant fluctuations, indicating changes in the transmission rate. This aligns with the initial phase of the pandemic where interventions and public behavior may have varied significantly. Parameters ( and ) exhibit minor fluctuations, suggesting relatively stable infection, recovery, and death rates initially.
- Middle Period (Days 100–400): During this period, the parameters generally remain close to zero, indicating a period of relative stability in the model parameters. This may correspond to a phase where the public health measures were effective and the spread of the virus was relatively controlled. Minor fluctuations in the signals of ( and ) suggest occasional changes in transmission, infection, and death rates, possibly due to minor policy changes or the emergence of new variants.
- Final Period (Days 400–500): An increase in the signal fluctuations for () is observed again, indicating another phase of significant changes in the transmission rate. This could correspond to the emergence of new variants, changes in public behavior, or modifications in public health policies. Fluctuations in other parameters ( and ) become more noticeable towards the end, indicating increased variability in the infection, recovery, death, and vaccination rates.
6. Discussion and Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rezabakhsh, A.; Ala, A.; Khodaei, S.H. Novel Coronavirus (COVID-19): A New Emerging Pandemic Threat. J. Res. Clin. Med. 2020, 8, 5–6. [Google Scholar] [CrossRef]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef]
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; Pastore y Piontti, A.; Mu, K.; Rossi, L.; Sun, K.; et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef]
- Giuliani, D.; Dickson, M.M.; Espa, G.; Santi, F. Modelling and predicting the spread of Coronavirus (COVID-19) infection in NUTS-3 Italian regions. arXiv 2020, arXiv:2003.06664. [Google Scholar]
- Fisher, D.; Heymann, D. Q&A: The novel coronavirus outbreak causing COVID-19. BMC Med. 2020, 18, 57. [Google Scholar] [CrossRef]
- McIntosh, K. Coronavirus Disease 2019 (COVID-19), Up-To-Date. Available online: https://www.uptodate.com/contents/coronaviruses (accessed on 8 May 2020).
- World Health Organization. Novel Coronavirus (2019-nCoV) Situation Reports; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Loli, P.E.; Zama, F. Monitoring Italian COVID-19 spread by a forced SEIRDV model. PLoS ONE 2020, 15, e0237417. [Google Scholar] [CrossRef]
- Bagal, D.K.; Rath, A.; Barua, A.; Patnaik, D. Estimating the parameters of susceptible-infected-recovered model of COVID-19 cases in India during lockdown periods. Chaos Solitons Fractals 2020, 140, 110–154. [Google Scholar] [CrossRef]
- Ghanam, R.; Boone, E.; Abdel-Salam, A.S. COVID-19: SEIRDV Model for Qatar COVID-19 Outbreak. Lett. Biomath. 2021, 8, 19–28. Available online: https://lettersinbiomath.org/manuscript/index.php/lib/article/view/126/118 (accessed on 22 September 2024).
- Clancy, D.; O’Neill, P.D. Bayesian estimation of the basic reproduction number in stochastic epidemic models. Bayesian Anal. 2008, 3, 737–757. [Google Scholar] [CrossRef]
- Jewell, C.P.; Kypraios, T.; Neal, P.; Roberts, G.O. Bayesian analysis for emerging infectious diseases. Bayesian Anal. 2009, 4, 465–496. [Google Scholar] [CrossRef]
- May, R.M.; Anderson, R.M. Infectious Diseases of Humans: Dynamics and Control; Oxford University Press: Oxford, UK, 1991; ISBN 0-19-854040-X. [Google Scholar]
- Vynnycky, E.; White, R.G. An Introduction to Infectious Disease Modelling; Oxford University Press: Oxford, UK, 2010; ISBN 978-0-19-856576-5. [Google Scholar]
- Chowell, G.; Brauer, F. The basic reproduction number of infectious diseases: Computation and estimation using compartmental epidemic models. In Mathematical and Statistical Estimation Approaches in Epidemiology; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Deb, S.; Majumdar, M. A time series method to analyze incidence pattern and estimate reproduction number of COVID-19. arXiv 2020, arXiv:2003.10655. [Google Scholar]
- Nikolopoulos, K.; Punia, S.; Schäfers, A.; Tsinopoulos, C.; Vasilakis, C. Forecasting and planning during a pandemic: COVID-19 growth rates, supply chain disruptions, and governmental decisions. Eur. J. Oper. Res. 2021, 290, 99–115. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.; Karmakar, S. Bayesian semiparametric time varying model for count data to study the spread of the COVID-19 cases. arXiv 2020, arXiv:2004.02281. [Google Scholar]
- Han, Z.; Li, T.; You, J. These Unprecedented Times: The Dynamic Pattern Of COVID-19 Deaths Around The World. arXiv 2020, arXiv:2011.02824. [Google Scholar]
- Wang, L.; Zhou, Y.; He, J.; Zhu, B.; Wang, F.; Tang, L.; Kleinsasser, M.; Barker, D.; Eisenberg, M.C.; Song, P.X. An epidemiological forecast model and software assessing interventions on the COVID-19 epidemic in China. J. Data Sci. 2020, 18, 409–432. [Google Scholar] [CrossRef]
- Basu, D.; Salvatore, M.; Ray, D.; Kleinsasser, M.; Purkayastha, S.; Bhattacharyya, R.; Mukherjee, B. A comprehensive public health evaluation of lockdown as a non-pharmaceutical intervention on COVID-19 spread in India: National trends masking state level variations. medRxiv 2020. [Google Scholar] [CrossRef]
- Kyrychko, Y.N.; Blyuss, K.B.; Brovchenko, I. Mathematical modelling of the dynamics and containment of COVID-19 in Ukraine. Sci. Rep. 2020, 10, 19662. [Google Scholar] [CrossRef]
- Zhang, P.; Feng, K.; Gong, Y.; Lee, J.; Lomonaco, S.; Zhao, L. Usage of compartmental models in predicting COVID-19 outbreaks. Aaps J. 2022, 24, 98. [Google Scholar] [CrossRef]
- Roberts, S.W. Control chart tests based on geometric moving averages. Technometrics 2000, 42, 97–101. [Google Scholar] [CrossRef]
- Lowry, C.A.; Woodall, W.H.; Champ, C.W.; Rigdon, S.E. A multivariate exponentially weighted moving average control chart. Technometrics 1992, 34, 46–53. [Google Scholar] [CrossRef]
- Page, E.S. Continuous inspection schemes. Biometrika 1954, 41, 100–115. [Google Scholar] [CrossRef]
- Reynolds, M.R., Jr.; Stoumbos, Z.G. Comparisons of some exponentially weighted moving average control charts for monitoring the process mean and variance. Technometrics 2006, 48, 550–567. [Google Scholar] [CrossRef]
- Crosier, R.B. Multivariate generalizations of cumulative sum quality-control schemes. Technometrics 1988, 30, 291–303. [Google Scholar] [CrossRef]
- Miller, M. 2019 Novel Coronavirus COVID-19 (2019-nCoV) Data Repository. Bull.-Assoc. Can. Map Libr. Arch. (Acmla) 2020, 164, 47–51. [Google Scholar] [CrossRef]
- Al Khal, A.; Al-Kaabi, S.; Checketts, R.J. Qatar’s response to COVID-19 pandemic. Heart Views 2020, 32, 21–129. [Google Scholar] [CrossRef]
- Hamad Medical Corporation. Major Risks to Business Continuity; Hamad Medical Corporation: Doha, Qatar, 2020. [Google Scholar]
- Ministry of Public Health. Qatar National Preparedness and Response Plan for Communicable Diseases; Ministry of Public Health: Doha, Qatar, 2019. [Google Scholar]
- Rencher, A.C.; Schaalje, G.B. Linear Models in Statistics; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdel-Salam, A.-S.G.; Boone, E.L.; Ghanam, R. Multivariate Techniques for Monitoring Susceptible, Exposed, Infected, Recovered, Death, and Vaccination Model Parameters for the COVID-19 Pandemic for Qatar. Int. J. Environ. Res. Public Health 2024, 21, 1580. https://doi.org/10.3390/ijerph21121580
Abdel-Salam A-SG, Boone EL, Ghanam R. Multivariate Techniques for Monitoring Susceptible, Exposed, Infected, Recovered, Death, and Vaccination Model Parameters for the COVID-19 Pandemic for Qatar. International Journal of Environmental Research and Public Health. 2024; 21(12):1580. https://doi.org/10.3390/ijerph21121580
Chicago/Turabian StyleAbdel-Salam, Abdel-Salam G., Edward L. Boone, and Ryad Ghanam. 2024. "Multivariate Techniques for Monitoring Susceptible, Exposed, Infected, Recovered, Death, and Vaccination Model Parameters for the COVID-19 Pandemic for Qatar" International Journal of Environmental Research and Public Health 21, no. 12: 1580. https://doi.org/10.3390/ijerph21121580
APA StyleAbdel-Salam, A.-S. G., Boone, E. L., & Ghanam, R. (2024). Multivariate Techniques for Monitoring Susceptible, Exposed, Infected, Recovered, Death, and Vaccination Model Parameters for the COVID-19 Pandemic for Qatar. International Journal of Environmental Research and Public Health, 21(12), 1580. https://doi.org/10.3390/ijerph21121580