


Investigating the Health Impacts of Climate Change among People with Pre-Existing Mental Health Problems: A Scoping Review

Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Inclusion Criteria
2.3. Data Extraction and Synthesis
3. Results
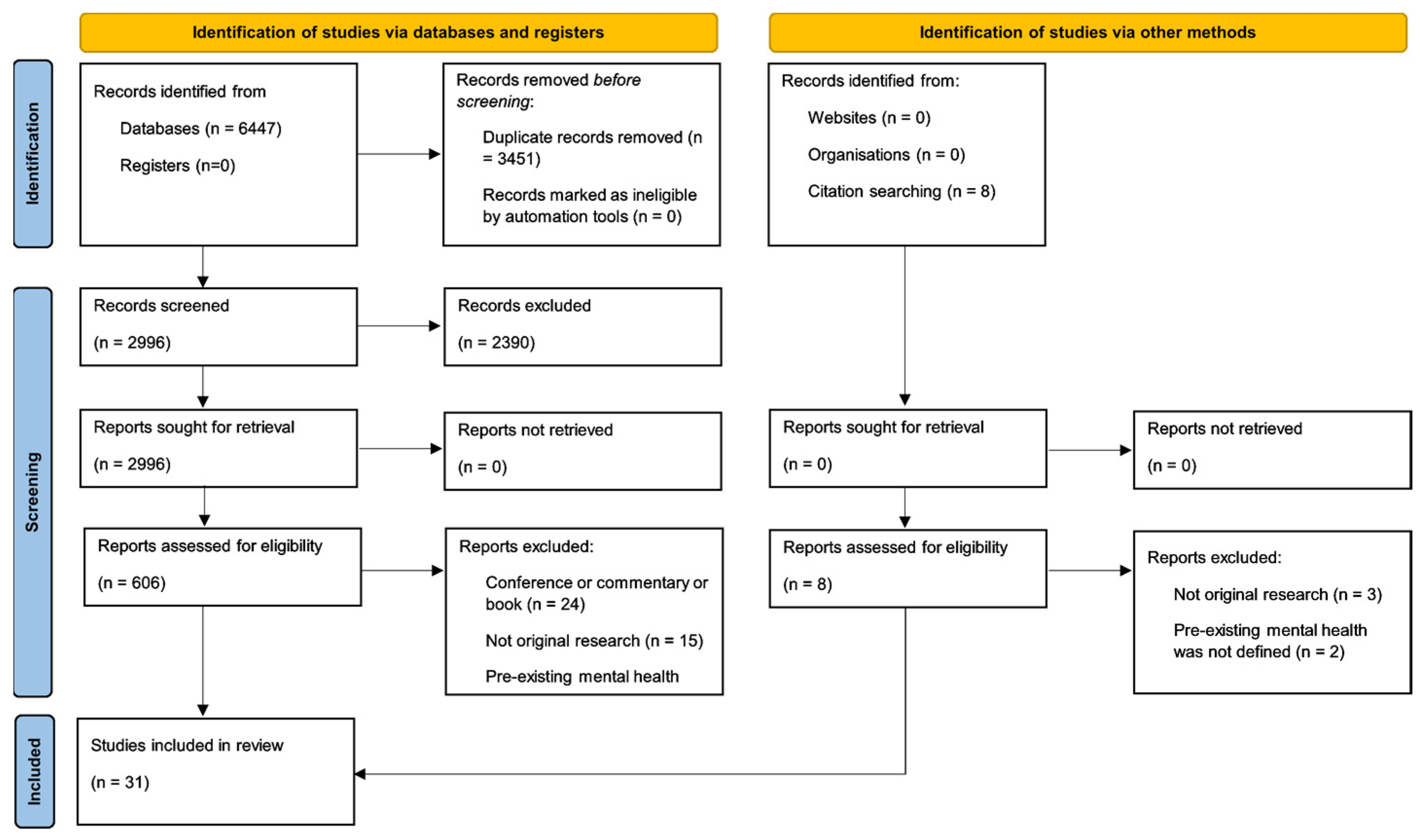
3.1. Study Selection
3.2. Study Characteristics
3.3. Heat Events
3.4. Floods
3.5. Wildfires
3.6. Wildfire and Flood/Cyclone
3.7. Hurricanes
3.8. Drought
4. Discussion
5. Limitations
6. Implications for Research and Practice
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Study | Country | Study Design | Total Participants n; Pre-Existing Mental Health (MH) n; Age (y = Years); % Male, % Female | Measurement/Definition of Pre-Existing Mental Health Problems Pre-Event | Measurement of Symptoms During and/or Post Event | Pre-Existing Mental Health (MH) Problem (‡) | Health Outcome | Effects on Health After the Climate-Driven Event |
|---|---|---|---|---|---|---|---|---|
| Heat | ||||||||
| De’donato, Stafoggia, Rognoni, Poncino, Caranci, Bisanti, Demaria, Forastiere, Michelozzi, Pelosini, and Perucci [29] | Italy | Quantitative case–crossover study | Adults Total n = 56,681; MH n = 588 (depression); 2038 (psychosis); Age = >35 y; Males = 48%; Females = 52% | Hospitalisation during the preceding two years (excluding the last 28 days) | Rome = four-year study period; Milan = five-year study period; Turin = seven-year study period | (i) Depression | (i) Mortality risk | (i) (a) Milan Airport: no increased risk (72% [95% CI −8–221]) (i) (b) Milan City: no increased risk (65% [95% CI −6–189]) (i) (c) Rome Airport: no increased risk (146% [95% CI 125–382]) (i) (d) Rome City: increased risk (166% (95% CI 35–424) (i) (e) Turin Airport: no increased risk (52% [95% CI −16–173]) (i) (f) Turin City: no increased risk (32% [95% CI −25–135]) |
| (ii) Psychosis | (ii) Mortality risk | (ii) (a) Milan Airport: increased risk (157% [95%, CI 82–264]) (ii) (b) Milan City: increased risk (91% [95% CI 40–161]) (ii) (c) Rome Airport: no increased risk (69% [95% CI 18–143]) (ii) (d) Rome City: no increased risk (82% [95% CI 28–158]) (ii) (e) Turin Airport: increased risk (93% [95% CI 47–152]) (ii) (f) Turin City: no increased risk (73% [95% CI 32–126]) | ||||||
| Kaiser, Rubin, Henderson, Wolfe, Kieszak, Parrott, and Adcock [30] | USA | Quantitative case–control study | Adults Total n = 51; MH n = 8; Age = 34–104 y; Males = 59%; Females = 41% | Reported retrospectively at the time of study | Twelve days during a heatwave | Aggregated (SZ, mentally handicapped, dementia, and alcohol abuse) | Mortality risk | Increased mortality risk: OR = 14.0 (95% CI 1.8–633) |
| Kim, Jo, Myung, and Jang [31] | South Korea | Quantitative case–control study | Children and adults Total n = 968; MH n = 261; Age = 0–19 y & 20–≥65 y; Males = 70%; Females = 30% | Reported retrospectively at the time of study | Four-month study period | Aggregated (SZ, dementia, depression, Parkinson’s disease, panic disorders, bipolar disorder, substance misuse, mental retardation, and unknown mental health diagnosis) | Heatstroke | (a) Increased heatstroke risk compared with mild heat illness: Fisher’s exact test, p < 0.001 (b) Increased heatstroke risk: adjusted OR = 7.69 (95% CI 4.06–14.54) |
| Naughton, Henderson, Mirabelli, Kaiser, Wilhelm, Kieszak, Rubin, and McGeehin [32] | USA | Quantitative case–control study | Adults Total n = 140; MH n = 36; Age = 35–93 y; Males = 49%; Females = 51% | Reported retrospectively at the time of study | Nine-day study period | (i) Depression | (i) Mortality risk | (i) Increased mortality risk: OR = 4.1 (95% CI 1.3–12.5) |
| (ii) Non-specified (excluding depression) | (ii) Mortality risk | (ii) Increased mortality risk: OR = 11.7 (95% CI 1.5–92.2) | ||||||
| (iii) Non-specified (including depression) | (iii) Mortality risk | (iii) Increased mortality risk: OR = 5.7 (95% CI 1.9–16.8) | ||||||
| Page, Hajat, Kovats, and Howard [33] | England | Quantitative cohort study | Unspecified Total n = 22,562; MH n = 22,562; Age = <65 y & ≥65 y; Males = unknown; Females = unknown | Registered diagnosis on medical records | Ten-year study period | (i) Psychosis | (i) Mortality risk | (i) No increased risk: RR = 1.02 (95% CI 0.95–1.09) |
| (ii) Dementia | (ii) Mortality risk | (ii) Increased risk of mortality for every 1 °C above 18 °C: RR = 1.03 (95% CI 1.00–1.07) | ||||||
| (iii) Alcohol misuse | (iii) Mortality risk | (iii) Increased risk of mortality for every 1 °C above 18 °C: RR = 1.08 (95% CI 1.04–1.13) | ||||||
| (iv) Other substance misuse | (iv) Mortality risk | (iv) Increased risk of mortality for every 1 °C above 18 °C: RR = 1.20 (95% CI 1.08–1.35) | ||||||
| (v) Aggregated (psychosis, dementia, and substance misuse) | (v) Mortality risk | (v) Increased risk for mortality for every 1 °C above 18 °C: RR = 1.05 (95% CI 1.02–1.08) | ||||||
| Stafoggia, Forastiere, Agostini, Biggeri, Bisanti, Cadum, Caranci, De’Donato, De Lisio, De Maria, Michelozzi, Miglio, Pandolfi, Picciotto, Rognoni, Russo, Scarnato, and Perucci [34] | Italy | Quantitative case–crossover study | Adults Total n =205,019; MH n = unknown; Age = ≥35 y; Males = 49%; Females = 51% | Hospital admission in the two years before death (excluding the last 28 days) | Three-to-six-year study period | (i) Depression | (i) Mortality | (i) Increased risk of mortality at 30 °C compared with that at 20 °C: OR = 1.71 (95% CI 1.23–1.28) |
| (ii) Psychosis | (ii) Mortality | (ii) Increased risk of mortality at 30 °C compared with that at 20 °C: OR = 1.70 (95% CI 1.39–2.09) | ||||||
| Stivanello, Chierzi, Marzaroli, Zanella, Miglio, Biavati, Perlangeli, Berardi, Fioritti, and Pandolfi [35] | Italy | Quantitative case–crossover study | Adults Total n = 48,286; MH n = 3008; Age = 18–≥84 y; Males = 47%; Females = 53% | Accessed mental health service | Fourteen-year study period | (i) Mania and bipolar affective disorders | (i) Mortality risk | (i) No increased risk: OR = 1.03 (95% CI 0.88–1.20) |
| (ii) Depression | (ii) Mortality risk | (ii) Increased risk of mortality for every 1 °C above 24 °C: OR = 1.08 (95% CI 1.03–1.14) | ||||||
| (iii) Neurotic disorders | (iii) Mortality risk | (iii) No increased risk: OR = 0.99 (95% CI 0.90–1.08) | ||||||
| (iv) Personal and behaviour disorders | (iv) Mortality risk | (iv) No increased risk: OR = 0.96 (95% CI 0.84–1.10) | ||||||
| (v) Alcoholism and substance misuse | (v) Mortality risk | (v) No increased risk: OR = 0.96 (95% CI 0.72–1.29) | ||||||
| (vi) Dementia and cognitive decline | (vi) Mortality risk | (vi) Increased risk of mortality for every 1 °C above 24 °C: OR = 1.07 (95% CI 1.02–1.13) | ||||||
| (vii) Non-specified | (vii) Mortality risk | (vii) No increased risk: OR 0.90 (95% CI 0.67–1.21) | ||||||
| (viii) Aggregated (SZ and other functional psychosis) | (viii) Mortality risk | (viii) No increased risk: OR = 1.05 (95% CI 0.95–1.16) | ||||||
| Brierley, Albertella, do Rosario, Ferrao, Miguel, and Fontenelle [36] | Brazil | Quantitative cross-sectional study | Adults Total n =742; MH n =742; Mean age =32.6 y; Males = 56%; Females = 54% | Reported retrospectively at the time of study | Six-year study period | OCD | OCD symptoms | Exacerbation of OCD symptoms β = 0.153 [95% CI 1.49–4.30], (p < 0.001) |
| Hoffmann, Oliveira, Lobato, and Belmonte-De-Abreu [37] * | Brazil | Qualitative case study | Adults Total n = 1; MH n = 1; Age = 60 y; Male = 100% | Onset of mental health problem aged 19 years | During event | SZ | Heatstroke | Glasgow Coma Scale 9/15, diagnosed with heat stroke, body temperature 41.9 °C |
| Kao and Kelly [38] * | Canada | Qualitative case study | Adults Total n = 1; MH n = 1; Age = 36 y; Male = 100% | History of mental health problems | During event | SZ and bipolar | Heatstroke | Glasgow Coma Scale 3/15, patient unresponsive and diagnosed with heat stroke, body temperature 42.2 °C |
| Kwok and Chan [39] * | Hong Kong | Qualitative case study | Adults Total n = 1; MH n = 1; Age = 48 y; Male = 100% | History of mental health problems | During event (two hospital admissions) | SZ and diabetes mellitus | Heatstroke | Admission 1: Glasgow Coma Scale 3/15, patient comatose, body temperature 42.4 °C Admission 2: Heat exhaustion (he was alert), body temperature 38.6 °C |
| Lee, Chen, and Chang [40] * | Taiwan | Qualitative case study | Adults Total n = 1; MH n = 1; Age = 49 y; Male = 100% | Onset of mental health problem aged 29 years | During event | SZ | Heatstroke | Glasgow Coma Scale 14/15, patient drowsy, weak, and slurring, body temperature 40.9 °C |
| Flood | ||||||||
| Felton, Cole, and Martin [41] | USA | Quantitative longitudinal study | Children Total n = 227; MH n = unknown; Age = 10–15 y; Males = unknown Females = unknown | Six months before | Ten days after | Depression | Depression | Association: r = 0.72, p < 0.001 |
| Ginexi, Weihs, Simmens, and Hoyt [42] | USA | Quantitative longitudinal study | Adults Total n = 1735; MH n = unknown Age = 18–98 y; Males = 34%; Females = 66% | One year before | Sixty to ninety days after | Depression | Depression | (a) Association: r = 0.54, b = 0.51, p < 0.001 (b) Increased depression risk: OR = 8.55 (95% CI 5.54–13.21); r = 0.35, b = 2.15, p < 0.001 |
| Hayes, Mason, Brown, and Mather [43] | England | Qualitative study | Elderly Adults Total n = 87; MH n = 87; Age = 73–90 y; Males = 41%; Females = 59% | Accessed mental health services | Immediate and up to nine months after | (i) Dementia | (i) Changes in symptoms and/or behaviour | (i) (a) Appearance of new symptoms (i) (b) Exacerbation of symptoms |
| (ii) Depression | (ii) Changes in symptoms and/or behaviour | (ii) (a) Appearance of new symptoms (ii) (b) Exacerbation of symptoms | ||||||
| (iii) Paranoid personality disorder | (iii) Changes in symptoms and/or behaviour | (iii) Appearance of new symptoms | ||||||
| (iv) Chronic mixed anxiety and depression | (iv) Changes in symptoms and/or behaviour | (iv) Exacerbation of symptoms | ||||||
| Hetherington, McDonald, Wu, and Tough [44] | Canada | Quantitative longitudinal study | Women Total n = 923; MH n = unknown; Age (mean) = 34.5 y; Women = 100% | Differed between participants, up to 18–36 months before | Five months after | (i) Depression | (i) (a) Depression | (i) (a) No increased risk: adjusted OR = 1.15 (95% CI 0.47–2.82) |
| (i) (b) PTSD | (i) (b) No increased risk: adjusted OR = 1.37 (95% CI 0.62–3.07) | |||||||
| (ii) Anxiety | (ii) (a) Depression | (ii) (a) Increased risk: adjusted OR = 9.85 (95% CI 4.06–23.96) | ||||||
| (ii) (b) Anxiety | (ii) (b) Increased risk: adjusted OR = 7.07 (95% CI 4.36–11.45) | |||||||
| (ii) (c) PTSD | (ii) (c) Increased risk: adjusted OR = 2.49 (95% CI 1.17–5.26) | |||||||
| Martin, Felton, and Cole [45] | USA | Quantitative longitudinal study | Children Total n = 125; MH n = unknown; Age = 10–15 y; Males = unknown; Females = unknown | Six months before | Ten days after | Depression | PTSD | (a) Association: r = 0.35, p < 0.001 (b) Significantly predicted PTSD symptoms: β = 0.24, p < 0.05. |
| McMillen, North, Mosley, and Smith [46] | USA | Quantitative cross-sectional study | Adults Total n = 162; MH n = 71; Age (mean) = 49.5 y; Males = 34%; Females = 66% | Reported retrospectively at the time of study (one month to at least four years prior) | One to six months after | Aggregated (PTSD, major depression, panic disorder, generalised anxiety disorder, and alcohol and drug misuse disorders) | (i) PTSD | (i) Increased risk: 34% compared with 11% without a history of mental health problems (x2 (1) = 12.27, p = 0.001) |
| (ii) Substance misuse | (ii) Increased alcohol misuse risk: 24% compared with 8% without a history of mental health problems (x2 (1) = 7.96, p = 0.005) | |||||||
| North, Kawasaki, Spitznagel, and Hong [47] | USA | Quantitative longitudinal study | Adults Total n = 162; MH n = 72; Age = 18–≥65 y; Males = 33%; Females = 67% | Reported retrospectively at the time of study | Four months and sixteen months post | Aggregated (PTSD, major depression, panic disorder, generalised anxiety disorder, alcohol and drug misuse disorders, and somatization disorder) | (i) PTSD | (i) Increased risk: 35% compared with 11% without a history of mental health problems at four-month follow-up (x2 (1) = 13.17, p < 0.001) |
| (ii) Somatoform symptoms | (ii) Increased risk of developing new somatoform symptoms: 37% compared with 16% without a history of mental health problems (x2 (1) = 9.79, p < 0.002) | |||||||
| Hoffman [48] | USA | Quantitative longitudinal study | Adults Total n = 463; MH n = 463; Age = 19–89 y; Males = 32%; Females = 68% | One year before | Two months after | (i) Depression | (i) Depression | (i) Association: β = 0.41, p < 0.001 |
| (ii) Anxiety | (ii) Association: β = 0.38, p < 0.001 | |||||||
| (iii) PTSD | (iii) No increased risk: β = 0.05, p > 0.05 | |||||||
| (iv) Aggregated (depression, anxiety, and PTSD) | (iv) Association: β = 0.421, p < 0.001 | |||||||
| Wildfires | ||||||||
| Rodney, Swaminathan, Calear, Christensen, Lal, Lane, Leviston, Reynolds, Trevenar, Vardoulakis, and Walker [49] | Australia | Quantitative cross-sectional survey | Adults Total n = 2084; MH n = 441; Age = 18–85 y; Males =40%; Females = 60% | Reported retrospectively at the time of study | Two weeks to four months | Non-specified | (i) Mental health symptoms | (i) Increased worsening symptoms risk: adjusted OR = 1.30 (1.01–1.66), p = 0.038 |
| (ii) Physical health symptoms | (ii) Increased physical symptoms risk: adjusted OR = 1.64 (95% CI 1.28–2.09), p < 0.001 | |||||||
| (iii) Poor sleep | (iii) No increased risk: OR = 1.19 (95% CI 0.95 to 1.50), p = 0.133 | |||||||
| Agyapong, Hrabok, Juhas, Omeje, Denga, Nwaka, Akinjise, Corbett, Moosavi, Brown, Chue, Greenshaw, and Li [50] | Canada | Quantitative cross-sectional survey | Adults (n = 486, 18–≥40 y, 33%, 67%) 103 with mental health problems | Reported retrospectively at the time of study | Six months after | (i) Depression | (i) Anxiety | (i) No increased risk: OR = 3.26 (95% CI 0.97–10.95) |
| (ii) Anxiety | (ii) Anxiety | (ii) Increased risk for GAD: OR = 6.76 (95% CI 1.65–27.70) | ||||||
| (iii) Non-specified | (iii) Anxiety | (iii) No increased risk: OR = 2.81 (95% CI 0.56–14.01) | ||||||
| Moosavi, Nwaka, Akinjise, Corbett, Chue, Greenshaw, Silverstone, Li, and Agyapong [51] | Canada | Quantitative cross-sectional survey | Adults Total n = 290; MH n = 66; Age = ≥18 y; 45%, 55% | Reported retrospectively at the time of study | 18 months after | (i) Depression | (i) (a) Depression | (i) (a) (a) Association: x2 = 0.36, p < 0.001 (i) (a) (b) Increased risk: OR = 4.63 (95% CI 1.77–12.12), p < 0.001 |
| (i) (b) Anxiety | (i) (b) (a) Association: x2 = 0.34, p < 0.001 (i) (b) (b) Increased risk: OR = 3.04 (95% CI 1.21–7.61), p = 0.02 | |||||||
| (i) (c) PTSD | (i) (c) (a) Association: x2 = 0.31, p < 0.001 (i) (c) (b) No increased risk: OR = 1.73 (95% CI 0.56–5.39), p = 0.34 | |||||||
| (ii) Anxiety | (ii) (a) Depression | (ii) (a) (a) Association: x2 = 0.29, p < 0.001 (ii) (a) (b) No increased risk: OR = 1.28 (95% CI 0.47–3.53), p = 0.63 | ||||||
| (ii) (b) Anxiety | (ii) (b) (a) Association: x2 = 0.30, p < 0.001 (ii) (b) (b) Increased risk: OR = 2.68 (95% CI 1.04–6.89), p = 0.04 | |||||||
| (ii) (c) PTSD | (ii) (c) (a) Association: x2 = 0.34, p < 0.001 (ii) (c) (b) Increased risk: OR = 5.80 (95% CI 1.92–17.50), p = 0.002 | |||||||
| Belleville, Ouellet, Lebel, Ghosh, Morin, Bouchard, Guay, Bergeron, Campbell, and MacMaster [52] | Canada | Quantitative cross-sectional survey | Adults Total n = 1510; MH n = 177; Age = ≥18 y; Males = 44%; Females = 56% | Reported retrospectively at the time of study | 12 to 14 months after | Non-specified | (i) Depression | (i) Increased risk: adjusted β = 2.98 (95% CI 2.31–3.65), p < 0.0001 |
| (ii) Anxiety | (ii) Increased risk: adjusted β = 2.15 (95% CI 1.51–2.80), p < 0.0001 | |||||||
| (iii) PTSD | (iii) Increased risk: adjusted β = 3.94 (95% CI 2.21–5.66), p < 0.0001 | |||||||
| (iv) Insomnia | (iv) Increased risk: adjusted β = 2.26 (95% CI 1.38–3.13), p < 0.001 | |||||||
| (v) Substance use | (v) Increased risk: adjusted β = 0.33 (0.18–0.48), p < 0.0001 | |||||||
| Agyapong, Juhas, Omege, Denga, Nwaka, Akinjise, Corbett, Brown, Chue, Li, and Greenshaw [53] | Canada | Quantitative cross-sectional survey | Adults Total n = 486; MH n = 103; Age = 16–88 y; Males = 34%; Females = 66% | Reported retrospectively at the time of study | Six months after | (i) Depression (ii) Anxiety | (i) PTSD (ii) PTSD | (i) No increased risk: OR = 1.78 (95% CI 0.53–6.03) (ii) Increased risk: OR = 7.89 (95% CI 1.70–36.59) |
| Agyapong, Ritchie, Brown, Noble, Mankowsi, Denga, Nwaka, Akinjise, Corbett, Moosavi, Chue, Li, Silverstone, and Greenshaw [54] | Canada | Quantitative cross-sectional survey | Adults Total n = 197; MH n = unknown; Age = ≥18 y; Males = 15%; Females = 85% | Reported retrospectively at the time of study | 18 months after | (i) Depression | (i) (a) Depression | (i) (a) No increased risk: x2 = 0.13 (p = 0.14) |
| (i) (b) Anxiety | (i) (b) No increased risk: x2 = −0.01 (p = 1.0) | |||||||
| (i) (c) PTSD | (i) (c) No increased risk: x2 = 0.02 (p = 1.0) | |||||||
| (ii) Anxiety | (ii) (a) Depression | (ii) (a) No increased risk: x2 = −0.005 (p = 1.0) | ||||||
| (ii) (b) Anxiety | (ii) (b) No increased risk: x2 = −0.12 (p = 0.15) | |||||||
| (ii) (c) PTSD | (ii) (c) No increased risk: x2 = 0.02 (p = 0.69) | |||||||
| Agyapong, Juhas, Brown, Omege, Denga, Nwaka, Akinjise, Corbett, Hrabok, Li, Greenshaw, and Chue [55] | Canada | Quantitative cross-sectional survey | Adults Total n = 486; MH n = 103; Age = 18–≥40 y; Males = 34%; Females = 66% | Reported retrospectively at the time of study | Six months after | (i) Depression | (i) Depression | (i) No increased risk: OR = 1.10 (95%, CI 0.34–3.55) |
| (ii) Anxiety | (ii) Depression | (ii) Increased risk: OR = 5.13 (95% CI 1.31–20.12) | ||||||
| Wildfire and flood/cyclone | ||||||||
| Reifels, Bassilios, Spittal, King, Fletcher, and Pirkis [56] | Australia | Quantitative cross-sectional study | Unclear Total n = 2693; MH n = 1042; Mean = 41 y; Males = 39%; Females = 61% | Reported retrospectively at the time of study | Two-year study period | Non-specified | Number of mental health therapy sessions | (a) No increased risk: OR = 0.95 (95% CI 0.80–1.13), p = 0.583 (b) Number of sessions per mental health referral: 4.87 (95% CI 4.38 to 5.36) compared with 5.11 (95% CI 4.39 to 5.83) without a history of mental health problems |
| Hurricanes | ||||||||
| Caramanica, Brackbill, Stellman, and Farfel [57] | USA | Quantitative longitudinal survey | Adults Total n = 4137; MH n = 335 Age = ≥18 y; Males = 56%; Females = 43% | Seven to 17 months before | Five to 12 months after | PTSD | PTSD | Increased PTSD risk: adjusted OR = 6.6 (95% CI 4.6–9.6) |
| Airhia [58] | USA | Quantitative cross-analysis | Children Total n = 77; MH n = 77; Age = 5–19 y; Males = 65%; Females = 35% | Zero to 22 months before | Zero to 28 months after | ADHD | PTSD | Increased PTSD risk: β = 1.54, p = 0.049 |
| Drought | ||||||||
| Barreau, Conway, Haught, Jackson, Kreutzer, Lockman, Minnick, Roisman, Rozell, Smorodinsky, Tafoya, and Wilken [59] | USA | Quantitative cross-sectional study | Households Total n = Unknown; MH n = 2742; Age = ≤18–≥65 y; Males = Unknown; Females = Unknown | Reported retrospectively at the time of study | 22 months after drought state of emergency | Non-specified | Worsening of symptoms | No increased risk: (a) Household did not have running water: weighted OR = 0.83 (95% CI 0.13–5.54) (b) Household had private well before drought: weighted OR = 1.19 (95% CI 0.31–4.60) (c) Negatively affected household finances: weighted OR = 0.58 (95% CI 0.16–1.62) (d) Negatively affected household property: weighted OR = 1.02 (95% CI 0.31–3.34) |
References
- World Health Organization. Climate Change and Health; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Romanello, M.; Di Napoli, C.; Drummond, P.; Green, C.; Kennard, H.; Lampard, P.; Scamman, D.; Arnell, N.; Ayeb-Karlsson, S.; Ford, L.B.; et al. The 2022 report of the Lancet Countdown on health and climate change: Health at the mercy of fossil fuels. Lancet 2022, 400, 1619–1654. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Environmental Health Sciences. People Who Are Vulnerable to Climate Change. Available online: https://www.niehs.nih.gov/research/programs/climatechange/health_impacts/vulnerable_people/index.cfm#:~:text=In%20general%2C%20children%20and%20pregnant,events1%2C%202%2C%203 (accessed on 10 November 2022).
- Intergovernmental Panel on Climate Change. Climate Change 2022 Impacts, Adaptation and Vulnerability; Intergovernmental Panel on Climate Change: Geneva, Switzerland, 2022. [Google Scholar]
- Lõhmus, M. Possible Biological Mechanisms Linking Mental Health and Heat—A Contemplative Review. Int. J. Environ. Res. Public Health 2018, 15, 1515. [Google Scholar] [CrossRef]
- Liu, J.; Varghese, B.M.; Hansen, A.; Xiang, J.; Zhang, Y.; Dear, K.; Gourley, M.; Driscoll, T.; Morgan, G.; Capon, A. Is there an association between hot weather and poor mental health outcomes? A systematic review and meta-analysis. Environ. Int. 2021, 153, 106533. [Google Scholar] [CrossRef]
- Cianconi, P.; Betro, S.; Janiri, L. The Impact of Climate Change on Mental Health: A Systematic Descriptive Review. Front. Psychiatry 2020, 11, 74. [Google Scholar] [CrossRef]
- Rocque, R.J.; Beaudoin, C.; Ndjaboue, R.; Cameron, L.; Poirier-Bergeron, L.; Poulin-Rheault, R.A.; Fallon, C.; Tricco, A.C.; Witteman, H.O. Health effects of climate change: An overview of systematic reviews. BMJ Open 2021, 11, e046333. [Google Scholar] [CrossRef] [PubMed]
- Romanello, M.; McGushin, A.; Di Napoli, C.; Drummond, P.; Hughes, N.; Jamart, L.; Kennard, H.; Lampard, P.; Solano Rodriguez, B.; Arnell, N.; et al. The 2021 report of the Lancet Countdown on health and climate change: Code red for a healthy future. Lancet 2021, 398, 1619–1662. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; de Pablo, G.S.; De Micheli, A.; Nieman, D.H.; Correll, C.U.; Kessing, L.V.; Pfennig, A.; Bechdolf, A.; Borgwardt, S.; Arango, C. What is good mental health? A scoping review. Eur. Neuropsychopharmacol. 2020, 31, 33–46. [Google Scholar] [CrossRef]
- World Health Organization. World Mental Health Report; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Cheema, H.A.; Rehan, S.T.; Shahid, A.; Head, M.G.; Jawad, M.Y.; Shah, J. The mental health of children in flood-affected areas in Pakistan needs urgent attention. Lancet Psychiatry 2023, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. UNICEF Pakistan Humanitarian Situation Report No. 4 (Floods): 28 September 2022; UNICEF: New York, NY, USA, 2022. [Google Scholar]
- Silveira, S.; Kornbluh, M.; Withers, M.C.; Grennan, G.; Ramanathan, V.; Mishra, J. Chronic Mental Health Sequelae of Climate Change Extremes: A Case Study of the Deadliest Californian Wildfire. Int. J. Environ. Res. Public Health 2021, 18, 1487. [Google Scholar] [CrossRef] [PubMed]
- Hayes, K.; Poland, B. Addressing mental health in a changing climate: Incorporating mental health indicators into climate change and health vulnerability and adaptation assessments. Int. J. Environ. Res. Public Health 2018, 15, 1806. [Google Scholar] [CrossRef]
- World Health Organization. Mental health and Climate Change: Policy Brief; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- European Climate and Health Observatory. Climate Change Impacts on Mental Health in Europe; European Climate and Health Observatory: Lübeck, Germany, 2022. [Google Scholar]
- Lawrance, E.; Thompson, R.; Fontana, G.; Jennings, N. The Impact of Climate Change on Mental Health and Emotional Wellbeing: Current Evidence and Implications for Policy and Practice; Institute of Global Health Innovation: London, UK, 2021. [Google Scholar]
- Stacey, B.; D’Arcy, C. No One Left Behind: Making Levelling Up Deliver for People with Mental Health Problems; Money and Mental Health Policy Institute: London, UK, 2022. [Google Scholar]
- Clayton, S.; Manning, C.; Krygsman, K.; Speiser, M. Mental Health and Our Changing Climate: Impacts, Implications, and Guidance; American Psychological Association: Washington, DC, USA; ecoAmerica: Washington, DC, USA, 2017. [Google Scholar]
- Berry, H.L.; Waite, T.D.; Dear, K.B.G.; Capon, A.G.; Murray, V. The case for systems thinking about climate change and mental health. Nat. Clim. Chang. 2018, 8, 282–290. [Google Scholar] [CrossRef]
- World Health Organization Mental Health. Available online: https://www.who.int/health-topics/mental-health#tab=tab_2 (accessed on 11 November 2022).
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [PubMed]
- United Nations Mental Health and Development. Available online: https://www.un.org/development/desa/disabilities/issues/mental-health-and-development.html (accessed on 11 November 2022).
- The Endnote Team. Endnote; EndNote 20; Clarivate: Philadelphia, PA, USA, 2013. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- De’donato, F.K.; Stafoggia, M.; Rognoni, M.; Poncino, S.; Caranci, N.; Bisanti, L.; Demaria, M.; Forastiere, F.; Michelozzi, P.; Pelosini, R.; et al. Airport and city-centre temperatures in the evaluation of the association between heat and mortality. Int. J. Biometeorol. 2008, 52, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, R.; Rubin, C.H.; Henderson, A.K.; Wolfe, M.I.; Kieszak, S.; Parrott, C.L.; Adcock, M. Heat-related death and mental illness during the 1999 Cincinnati heat wave. Am. J. Forensic Med. Pathol. 2001, 22, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Jo, S.N.; Myung, H.N.; Jang, J.Y. The effect of pre-existing medical conditions on heat stroke during hot weather in South Korea. Environ. Res. 2014, 133, 246–252. [Google Scholar] [CrossRef]
- Naughton, M.P.; Henderson, A.; Mirabelli, M.C.; Kaiser, R.; Wilhelm, J.L.; Kieszak, S.M.; Rubin, C.H.; McGeehin, M.A. Heat-related mortality during a 1999 heat wave in Chicago. Am. J. Prev. Med. 2002, 22, 221–227. [Google Scholar] [CrossRef]
- Page, L.A.; Hajat, S.; Kovats, R.S.; Howard, L.M. Temperature-related deaths in people with psychosis, dementia and substance misuse. Br. J. Psychiatry 2012, 200, 485–490. [Google Scholar] [CrossRef]
- Stafoggia, M.; Forastiere, F.; Agostini, D.; Biggeri, A.; Bisanti, L.; Cadum, E.; Caranci, N.; De’Donato, F.; De Lisio, S.; De Maria, M.; et al. Vulnerability to heat-related mortality: A multicity, population-based, case-crossover analysis. Epidemiology 2006, 17, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Stivanello, E.; Chierzi, F.; Marzaroli, P.; Zanella, S.; Miglio, R.; Biavati, P.; Perlangeli, V.; Berardi, D.; Fioritti, A.; Pandolfi, P. Mental health disorders and summer temperature-related mortality: A case crossover study. Int. J. Environ. Res. Public Health 2020, 17, 9122. [Google Scholar] [CrossRef] [PubMed]
- Brierley, M.E.E.; Albertella, L.; do Rosario, M.C.; Ferrao, Y.A.; Miguel, E.C.; Fontenelle, L.F. How do daily routines and situational factors affect the severity of obsessive-compulsive disorder? J. Psychiatr. Res. 2021, 143, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.S.; Oliveira, L.M.; Lobato, M.I.R.; Belmonte-De-Abreu, P. Heat stroke during long-term clozapine treatment: Should we be concerned about hot weather? Trends Psychiatry Psychother. 2016, 38, 56–59. [Google Scholar] [CrossRef]
- Kao, R.L.; Kelly, L.M. Fatal exertional heat stroke in a patient receiving zuclopenthixol, quetiapine and benztropine. Can. J. Clin. Pharmacol. 2007, 14, e322-5. [Google Scholar]
- Kwok, J.S.S.; Chan, T.Y.K. Recurrent heat-related illnesses during antipsychotic treatment. Ann. Pharmacother. 2005, 39, 1940–1942. [Google Scholar] [CrossRef]
- Lee, C.P.; Chen, P.J.; Chang, C.M. Heat stroke during treatment with olanzapine, trihexyphenidyl, and trazodone in a patient with schizophrenia. Acta Neuropsychiatr. 2015, 27, 380–385. [Google Scholar] [CrossRef]
- Felton, J.W.; Cole, D.A.; Martin, N.C. Effects of rumination on child and adolescent depressive reactions to a natural disaster: The 2010 nashville flood. J. Abnorm. Psychol. 2013, 122, 64–73. [Google Scholar] [CrossRef]
- Ginexi, E.M.; Weihs, K.; Simmens, S.J.; Hoyt, D.R. Natural disaster and depression: A prospective investigation of reactions to the 1993 midwest floods. Am. J. Community Psychol. 2000, 28, 495–518. [Google Scholar] [CrossRef]
- Hayes, J.; Mason, J.; Brown, F.; Mather, R. Floods in 2007 and older adult services: Lessons learnt. Psychiatr. Bull. 2009, 33, 332–336. [Google Scholar] [CrossRef]
- Hetherington, E.; McDonald, S.; Wu, M.; Tough, S. Risk and Protective Factors for Mental Health and Community Cohesion After the 2013 Calgary Flood. Disaster Med. Public Health Prep. 2018, 12, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Martin, N.C.; Felton, J.W.; Cole, D.A. Predictors of Youths’ Posttraumatic Stress Symptoms Following a Natural Disaster: The 2010 Nashville, Tennessee, Flood. J. Clin. Child Adolesc. Psychol. Off. J. Soc. Clin. Child Adolesc. Psychol. Am. Psychol. Assoc. Div. 2016, 45, 335–347. [Google Scholar] [CrossRef] [PubMed]
- McMillen, C.; North, C.; Mosley, M.; Smith, E. Untangling the psychiatric comorbidity of posttraumatic stress disorder in a sample of flood survivors. Compr. Psychiatry 2002, 43, 478–485. [Google Scholar] [CrossRef]
- North, C.S.; Kawasaki, A.; Spitznagel, E.L.; Hong, B.A. The course of PTSD, major depression, substance abuse, and somatization after a natural disaster. J. Nerv. Ment. Dis. 2004, 192, 823–829. [Google Scholar] [CrossRef]
- Hoffman, S.J. Coping Processes of Midwest Flood Survivors: A Comparison of Those with and without Prior Natural Disaster Exposure. Ph.D. Thesis, University of Nebraska, Lincoln, NE, USA, 2006. [Google Scholar]
- Rodney, R.M.; Swaminathan, A.; Calear, A.L.; Christensen, B.K.; Lal, A.; Lane, J.; Leviston, Z.; Reynolds, J.; Trevenar, S.; Vardoulakis, S.; et al. Physical and Mental Health Effects of Bushfire and Smoke in the Australian Capital Territory 2019–20. Front. Public Health 2021, 9, 682402. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.O.; Hrabok, M.; Juhas, M.; Omeje, J.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Moosavi, S.; Brown, M.; et al. Prevalence rates and predictors of generalized anxiety disorder symptoms in residents of fort mcmurray six months after a wildfire. Front. Psychiatry 2018, 9, 345. [Google Scholar] [CrossRef] [PubMed]
- Moosavi, S.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Chue, P.; Greenshaw, A.J.; Silverstone, P.H.; Li, X.M.; Agyapong, V.I.O. Mental Health Effects in Primary Care Patients 18 Months After a Major Wildfire in Fort McMurray: Risk Increased by Social Demographic Issues, Clinical Antecedents, and Degree of Fire Exposure. Front. Psychiatry 2019, 10, 683. [Google Scholar] [CrossRef]
- Belleville, G.; Ouellet, M.C.; Lebel, J.; Ghosh, S.; Morin, C.M.; Bouchard, S.; Guay, S.; Bergeron, N.; Campbell, T.; MacMaster, F.P. Psychological Symptoms Among Evacuees From the 2016 Fort McMurray Wildfires: A Population-Based Survey One Year Later. Front. Public Health 2021, 9, 444. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Juhas, M.; Omege, J.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Brown, M.; Chue, P.; Li, X.-M.; et al. Prevalence Rates and Correlates of Likely Post-Traumatic Stress Disorder in Residents of Fort McMurray 6 Months After a Wildfire. Int. J. Ment. Health Addict. 2021, 19, 632–650. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Ritchie, A.; Brown, M.R.G.; Noble, S.; Mankowsi, M.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Moosavi, S.; et al. Long-Term Mental Health Effects of a Devastating Wildfire Are Amplified by Socio-Demographic and Clinical Antecedents in Elementary and High School Staff. Front. Psychiatry 2020, 11, 448. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Juhas, M.; Brown, M.R.; Omege, J.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Hrabok, M.; Li, X.-M.; et al. Prevalence rates and correlates of probable major depressive disorder in residents of Fort McMurray 6 months after a wildfire. Int. J. Ment. Health Addict. 2019, 17, 120–136. [Google Scholar] [CrossRef]
- Reifels, L.; Bassilios, B.; Spittal, M.; King, K.; Fletcher, J.; Pirkis, J. Patterns and predictors of primary mental health service use following bushfire and flood disasters. Disaster Med. Public Health Prep. 2015, 9, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Caramanica, K.; Brackbill, R.M.; Stellman, S.D.; Farfel, M.R. Posttraumatic Stress Disorder after Hurricane Sandy among Persons Exposed to the 9/11 Disaster. Int. J. Emerg. Ment. Health 2015, 17, 356–362. [Google Scholar] [CrossRef]
- Airhia, E. Predicting Posttraumatic Stress Disorder in Children with Prior Mental Health Diagnoses Following Hurricane Katrina. Ph.D. Thesis, Walden University, Minneapolis, MN, USA, 2016. [Google Scholar]
- Barreau, T.; Conway, D.; Haught, K.; Jackson, R.; Kreutzer, R.; Lockman, A.; Minnick, S.; Roisman, R.; Rozell, D.; Smorodinsky, S.; et al. Physical, Mental, and Financial Impacts From Drought in Two California Counties, 2015. Am. J. Public Health 2017, 107, 783–790. [Google Scholar] [CrossRef]
- Basu, R.; Gavin, L.; Pearson, D.; Ebisu, K.; Malig, B. Examining the Association Between Apparent Temperature and Mental Health-Related Emergency Room Visits in California. Am. J. Epidemiol. 2018, 187, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Bundo, M.; de Schrijver, E.; Federspiel, A.; Toreti, A.; Xoplaki, E.; Luterbacher, J.; Franco, O.H.; Muller, T.; Vicedo-Cabrera, A.M. Ambient temperature and mental health hospitalizations in Bern, Switzerland: A 45-year time-series study. PLoS ONE 2021, 16, e0258302. [Google Scholar] [CrossRef]
- Dang, T.N.; Vy, N.T.T.; Thuong, D.T.H.; Phung, D.; Van Dung, D.; Le An, P. Main and added effects of heatwaves on hospitalizations for mental and behavioral disorders in a tropical megacity of Vietnam. Environ. Sci. Pollut. Res. Int. 2022, 29, 59094–59103. [Google Scholar] [CrossRef]
- Hansen, A.; Bi, P.; Nitschke, M.; Ryan, P.; Pisaniello, D.; Tucker, G. The effect of heat waves on mental health in a temperate Australian City. Environ. Health Perspect. 2008, 116, 1369–1375. [Google Scholar] [CrossRef] [PubMed]
- Bark, N. Deaths of Psychiatric Patients During Heat Waves. Psychiatr. Serv. 1998, 49, 1088–1090. [Google Scholar] [CrossRef]
- Martin-Latry, K.; Goumy, M.P.; Latry, P.; Gabinski, C.; Begaud, B.; Faure, I.; Verdoux, H. Psychotropic drugs use and risk of heat-related hospitalisation. Eur. Psychiatry 2007, 22, 335–338. [Google Scholar] [CrossRef]
- Alderman, K.; Turner, L.R.; Tong, S. Floods and human health: A systematic review. Environ. Int. 2012, 47, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Leyva, E.W.A.; Beaman, A.; Davidson, P.M. Health Impact of Climate Change in Older People: An Integrative Review and Implications for Nursing. J. Nurs. Sch. 2017, 49, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, A.; Black, J.; Jones, M.; Wilson, L.; Salvador-Carulla, L.; Astell-Burt, T.; Black, D. Flooding and Mental Health: A Systematic Mapping Review. PLoS ONE 2015, 10, e0119929. [Google Scholar] [CrossRef]
- Lechowska, E. What determines flood risk perception? A review of factors of flood risk perception and relations between its basic elements. Nat. Hazards 2018, 94, 1341–1366. [Google Scholar] [CrossRef]
- Ugwu, L.I.; Ugwu, D.I. Gender, floods and mental health: The way forward. Int. J. Asian Soc. Sci. 2013, 3, 1030–1042. [Google Scholar]
- Cvetković, V.; Roder, G.; Öcal, A.; Tarolli, P.; Dragićević, S. The Role of Gender in Preparedness and Response Behaviors towards Flood Risk in Serbia. Int. J. Environ. Res. Public Health 2018, 15, 2761. [Google Scholar] [CrossRef]
- Akerkar, S.; Fordham, M. Gender, place and mental health recovery in disasters: Addressing issues of equality and difference. Int. J. Disaster Risk Reduct. 2017, 23, 218–230. [Google Scholar] [CrossRef]
- Smid, G.E.; Van Der Velden, P.G.; Gersons, B.P.; Kleber, R.J. Late-onset posttraumatic stress disorder following a disaster: A longitudinal study. Psychol. Trauma: Theory Res. Pract. Policy 2012, 4, 312. [Google Scholar] [CrossRef]
- Stanke, C.; Kerac, M.; Prudhomme, C.; Medlock, J.; Murray, V. Health Effects of Drought: A Systematic Review of the Evidence. PLoS Curr. 2013, 5. [Google Scholar] [CrossRef] [PubMed]
- Vins, H.; Bell, J.; Saha, S.; Hess, J.J. The mental health outcomes of drought: A systematic review and causal process diagram. Int. J. Environ. Res. Public Health 2015, 12, 13251–13275. [Google Scholar] [CrossRef]
- Edwards, B.; Gray, M.; Hunter, B. The impact of drought on mental health in rural and regional Australia. Soc. Indic. Res. 2015, 121, 177–194. [Google Scholar] [CrossRef]
- Hanigan, I.C.; Schirmer, J.; Niyonsenga, T. Drought and Distress in Southeastern Australia. EcoHealth 2018, 15, 642–655. [Google Scholar] [CrossRef]
- Hanigan, I.C.; Butler, C.D.; Kokic, P.N.; Hutchinson, M.F. Suicide and drought in New South Wales, Australia, 1970–2007. Proc. Natl. Acad. Sci. USA 2012, 109, 13950–13955. [Google Scholar] [CrossRef]
- Brew, B.; Inder, K.; Allen, J.; Thomas, M.; Kelly, B. The health and wellbeing of Australian farmers: A longitudinal cohort study. BMC Public Health 2016, 16, 988. [Google Scholar] [CrossRef] [PubMed]
- Dean, J.G.; Stain, H.J. Mental health impact for adolescents living with prolonged drought. Aust. J. Rural Health 2010, 18, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Luong, T.T.; Handley, T.; Austin, E.K.; Kiem, A.S.; Rich, J.L.; Kelly, B. New Insights Into the Relationship Between Drought and Mental Health Emerging From the Australian Rural Mental Health Study. Front. Psychiatry 2021, 12, 719786. [Google Scholar] [CrossRef]
- Rigby, C.W.; Rosen, A.; Berry, H.L.; Hart, C.R. If the land’s sick, we’re sick:* the impact of prolonged drought on the social and emotional well-being of Aboriginal communities in rural New South Wales. Aust. J. Rural Health 2011, 19, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Rich, J.L.; Wright, S.L.; Loxton, D. ‘Patience, hormone replacement therapy and rain!’ Women, ageing and drought in Australia: Narratives from the mid-age cohort of the Australian Longitudinal Study on Women’s Health. Aust. J. Rural Health 2012, 20, 324–328. [Google Scholar] [CrossRef]
- World Health Organization Climate Action Must Include Mental Health. Available online: https://www.who.int/news/item/03-06-2022-why-mental-health-is-a-priority-for-action-on-climate-change (accessed on 1 March 2023).
- Clayton, S. Climate anxiety: Psychological responses to climate change. J. Anxiety Disord. 2020, 74, 102263. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.E.O.; Benoit, L.; Clayton, S.; Parnes, M.F.; Swenson, L.; Lowe, S.R. Climate change anxiety and mental health: Environmental activism as buffer. Curr. Psychol. 2022. [Google Scholar] [CrossRef] [PubMed]
- United States Government Build a Kit. Available online: https://www.ready.gov/kit (accessed on 1 March 2023).

| Climate-Driven Event | Pre-Existing Mental Health Problem | Impact on Health After a Climate-Driven Event (Health Problem) | No Significant Impacts on Health After a Climate-Driven Event | Inconclusive Impacts on Health After a Climate-Event |
|---|---|---|---|---|
| Heat events | Depression | Increased mortality risk [32,34,35] | Mortality risk [29] | |
| Psychosis | Increased mortality risk [34] | Mortality risk [33] | Mortality risk [29] | |
| Schizophrenia | Increased heatstroke risk [37,40] * | |||
| Schizophrenia and comorbidities | Increased heatstroke risk [38,39] * | |||
| Dementia | Increased mortality risk [33,35] | |||
| Substance misuse | Increased mortality risk [33] | Mortality risk [35] | ||
| Obsessive–compulsive disorder | Exacerbated symptoms (OCD) [36] | |||
| Neurotic disorders | Mortality risk [35] | |||
| Personality and behaviour disorders | Mortality risk [35] | |||
| Mania and bipolar | Mortality risk [35] | |||
| Non-specified ‡ | Increased mortality risk [32] | Mortality risk [35] | ||
| Aggregated ‡ | Increased mortality risk [30,33] | Mortality risk [35] | ||
| Increased heatstroke risk [31] | ||||
| Floods | Depression | Increased risk (depression) [41,42,48] | Depression [44] | |
| Increased risk (anxiety) [48] | ||||
| Increased risk (PTSD) [45] | PTSD [44,48] | |||
| New symptom presentation (non-specified) [43] | ||||
| Increased risk (aggregated) [48] | ||||
| Anxiety | Increased risk (depression) [44] | |||
| Increased risk (anxiety) [44] | ||||
| Increased risk (PTSD) [44] | ||||
| Chronic mixed anxiety and depression | New symptom presentation (non-specified) [43] | |||
| Paranoid personality disorder | New symptom presentation (non-specified) [43] | |||
| Dementia | New symptom presentation (non-specified) [43] | |||
| Aggregated ‡ | Increased risk (PTSD) [46,47] | |||
| Increased risk (substance misuse) [46] | ||||
| New symptom presentation (somatoform) [47] | ||||
| Wildfires | Depression | Increased risk (depression) [51] | Depression [54,55] | |
| Increased risk (anxiety) [51] | Anxiety [50,54] | |||
| PTSD [53,54] | PTSD [51] | |||
| Anxiety | Increased risk (depression) [55] | Depression [54] | Depression [51] | |
| Increased risk (anxiety) [50,51] | Anxiety [54] | |||
| Increased risk (PTSD) [51,53] | PTSD [54] | |||
| Non-specified ‡ | Increased risk (depression) [52] | |||
| Increased risk (anxiety) [52] | Anxiety [50] | |||
| Increased risk (PTSD) [52] | ||||
| Increased risk (insomnia) [52] | Poor sleep [49] | |||
| Increased risk (substance misuse) [52] | ||||
| Exacerbated symptoms (non-specified, physical health) [49] | ||||
| Exacerbated symptoms (non-specified, mental health) [49] | ||||
| Wildfire and flooding/cyclone | Non-specified ‡ | Use of mental health services [56] | ||
| Hurricanes | Post-traumatic stress disorder | Increased risk (PTSD) [57] | ||
| Attention-deficit hyperactivity disorder | Increased risk (PTSD) [58] | |||
| Drought | Non-specified ‡ | Non-specified [59] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woodland, L.; Ratwatte, P.; Phalkey, R.; Gillingham, E.L. Investigating the Health Impacts of Climate Change among People with Pre-Existing Mental Health Problems: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 5563. https://doi.org/10.3390/ijerph20085563
Woodland L, Ratwatte P, Phalkey R, Gillingham EL. Investigating the Health Impacts of Climate Change among People with Pre-Existing Mental Health Problems: A Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(8):5563. https://doi.org/10.3390/ijerph20085563
Chicago/Turabian StyleWoodland, Lisa, Priyanjali Ratwatte, Revati Phalkey, and Emma L. Gillingham. 2023. "Investigating the Health Impacts of Climate Change among People with Pre-Existing Mental Health Problems: A Scoping Review" International Journal of Environmental Research and Public Health 20, no. 8: 5563. https://doi.org/10.3390/ijerph20085563
APA StyleWoodland, L., Ratwatte, P., Phalkey, R., & Gillingham, E. L. (2023). Investigating the Health Impacts of Climate Change among People with Pre-Existing Mental Health Problems: A Scoping Review. International Journal of Environmental Research and Public Health, 20(8), 5563. https://doi.org/10.3390/ijerph20085563