
Models of Aviation Noise Impact in the Context of Operation Decrease at Tan Son Nhat Airport †

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
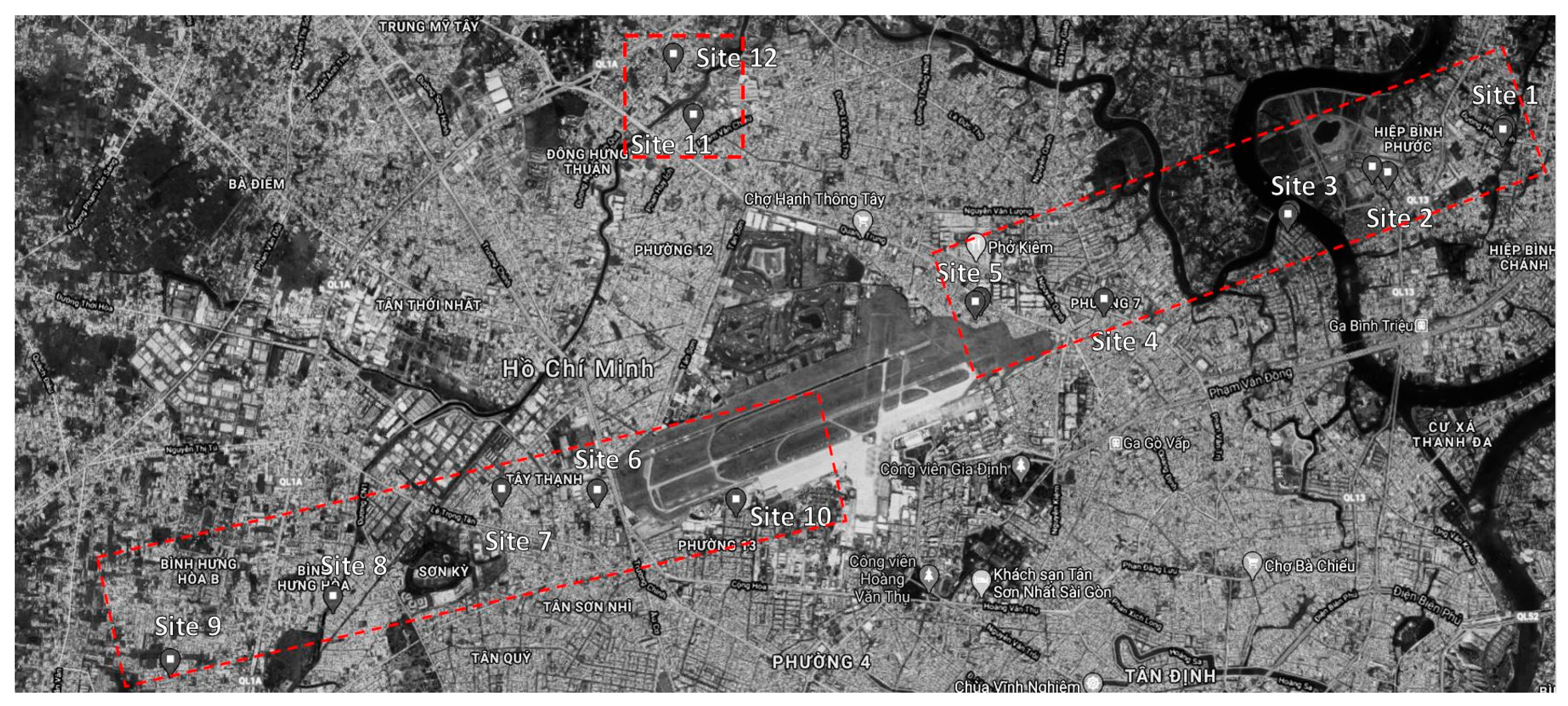
2.1. Survey Plan
2.2. Questionnaire and Measuring Scales
2.3. Aircraft Noise Estimation
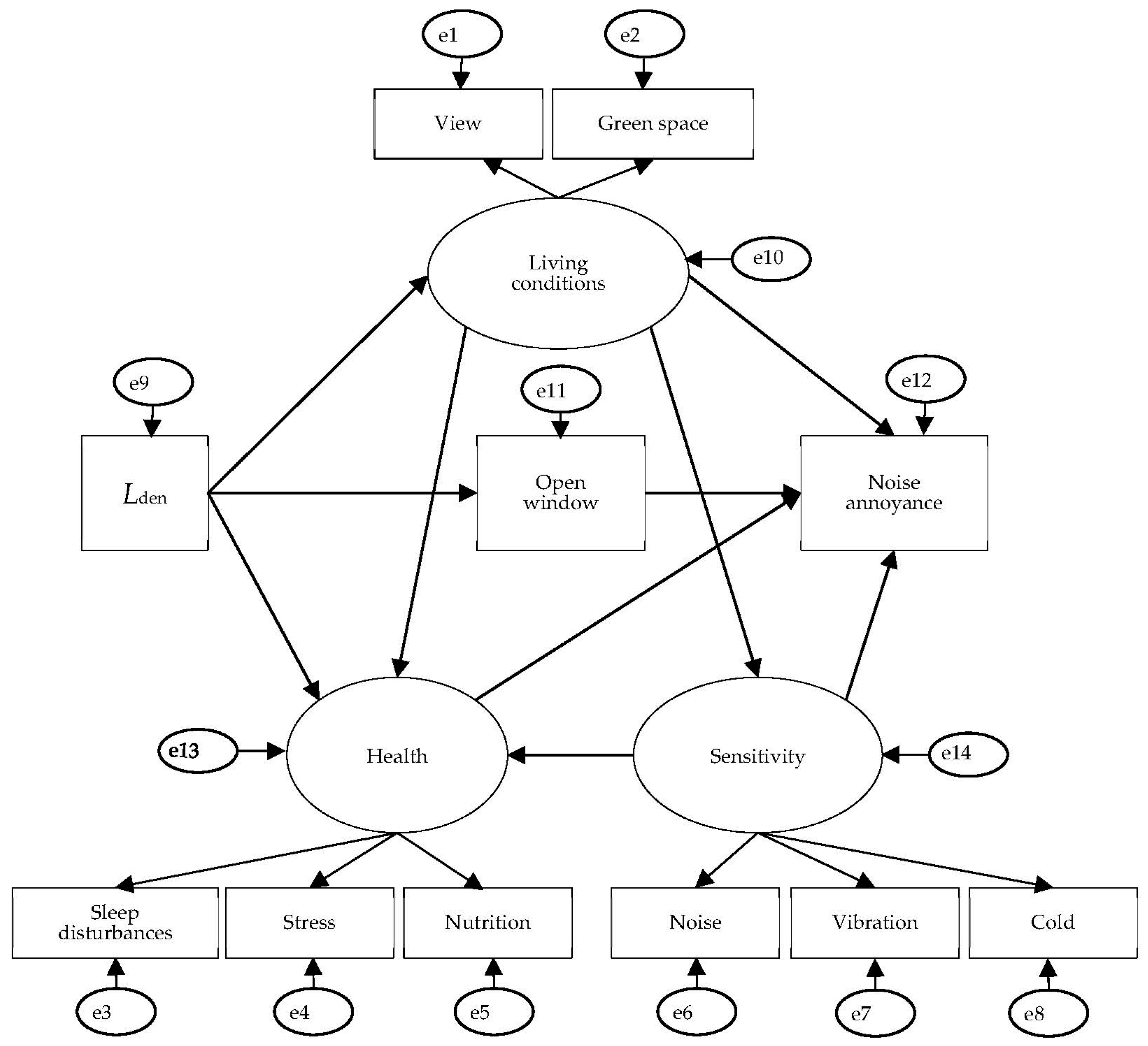
2.4. Model Development
3. Results
3.1. Demographic Data of the Survey Respondents
3.2. Noise Exposure and Community Response
3.3. Variables in the Model
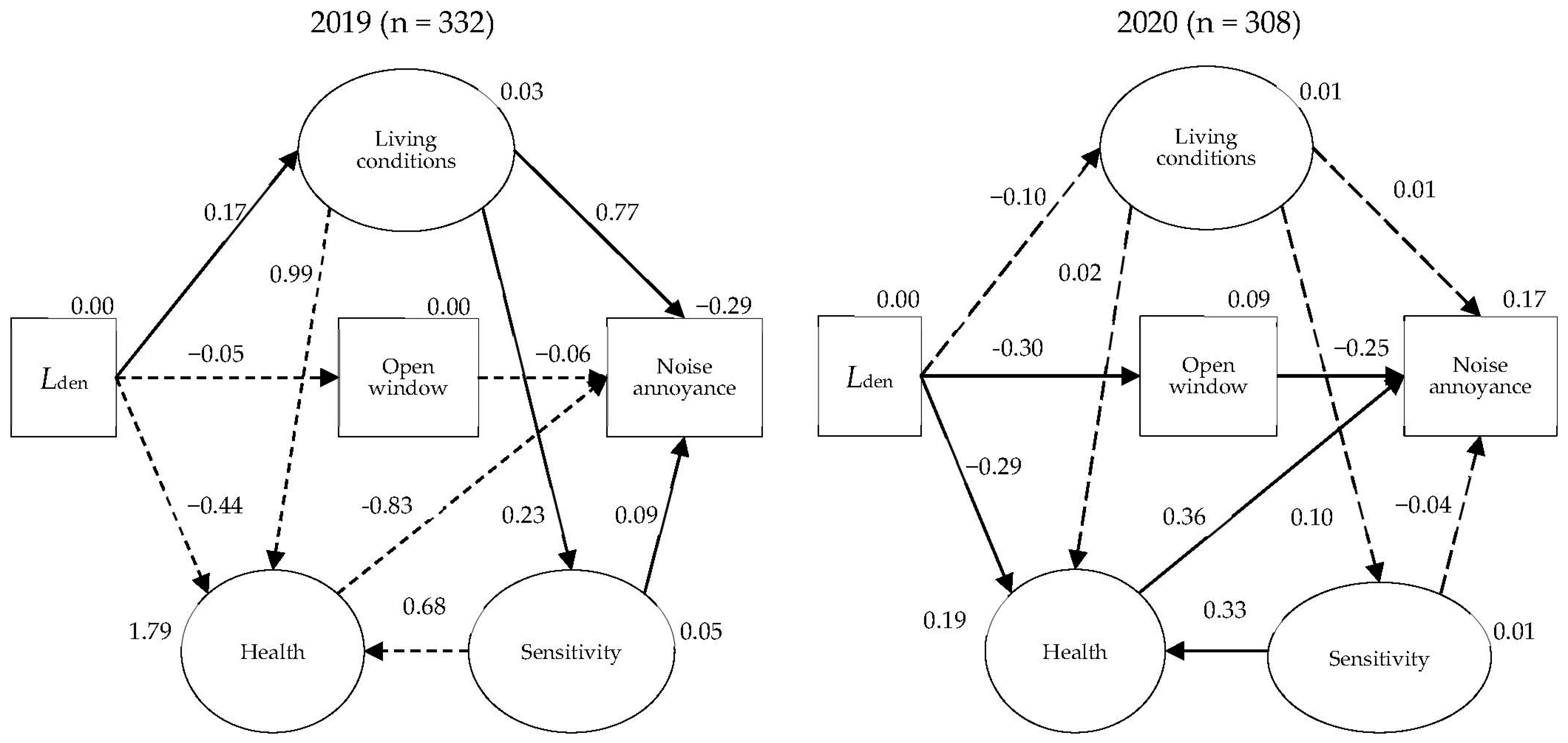
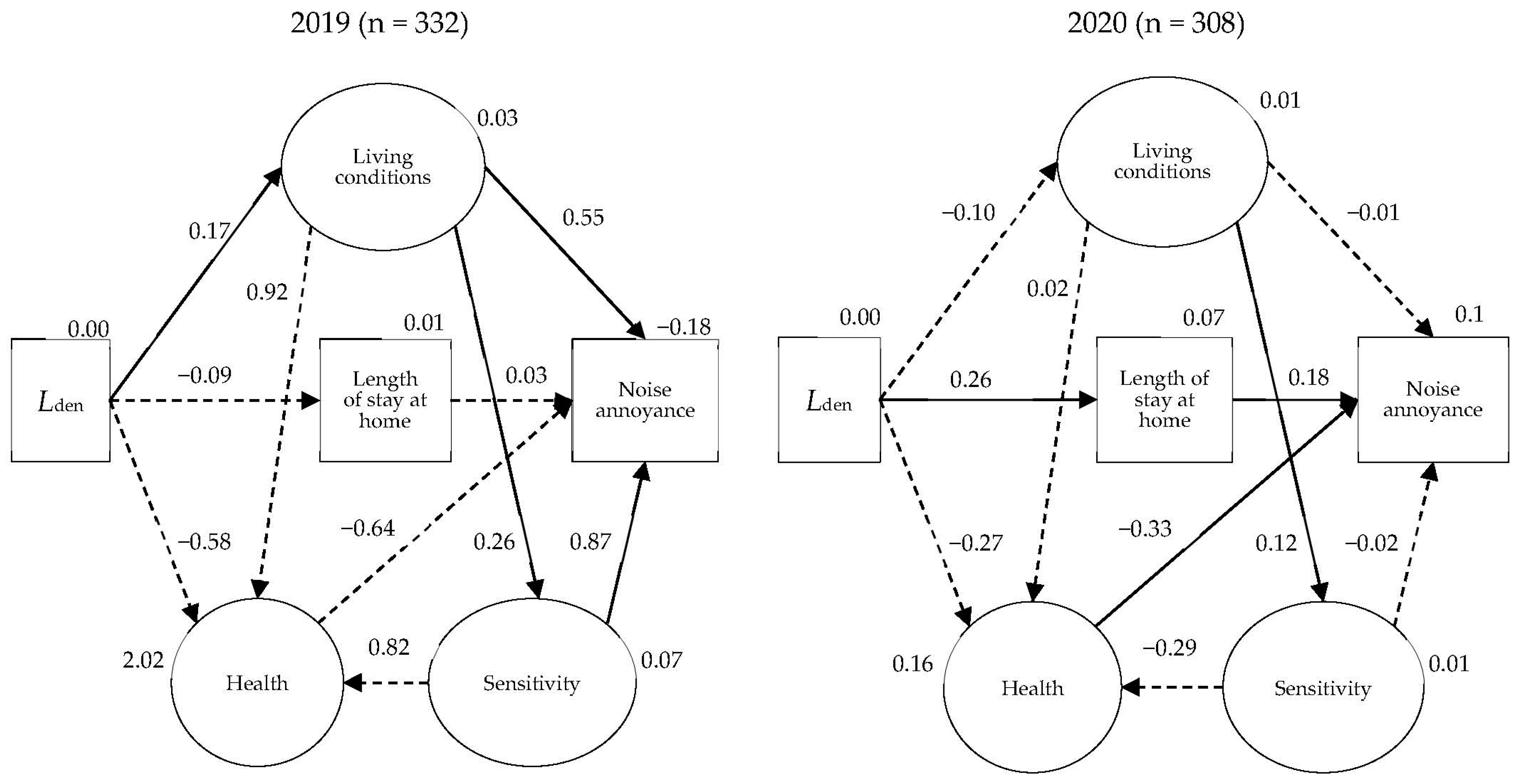
3.4. Comparison of Noise Annoyance Models between 2019 and 2020 Surveys
- Noise annoyance was directly influenced by opening bedroom windows during the dry season, sensitivity, health, and living conditions.
- Living conditions were influenced directly by noise exposure (Lden).
- Living conditions directly and indirectly influenced noise annoyance through sensitivity.
- Noise exposure (Lden) indirectly influenced noise annoyance via the opening of bedroom windows during the dry season.
- Health status was directly influenced by noise exposure (Lden), living conditions, and noise sensitivity.
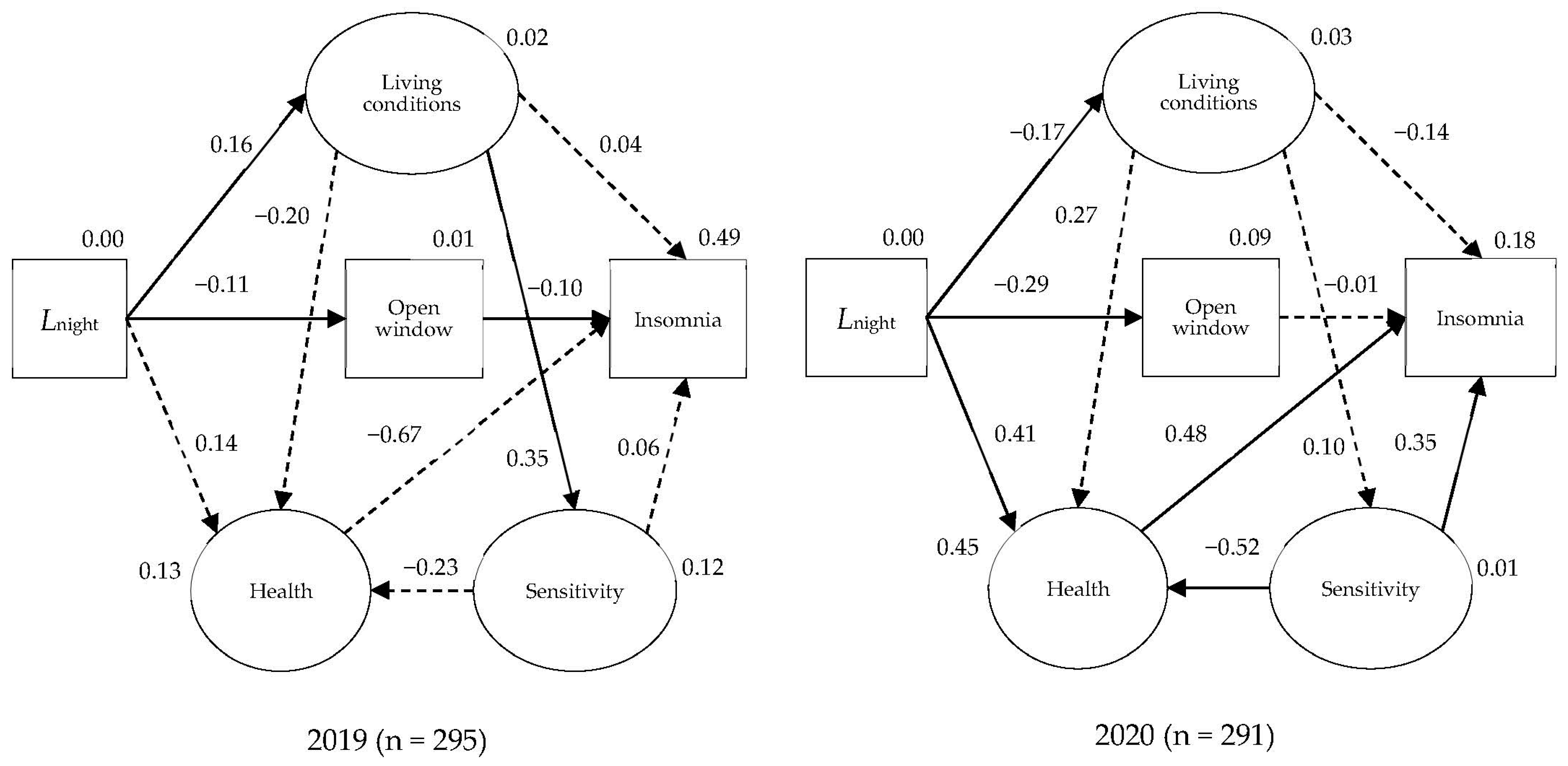
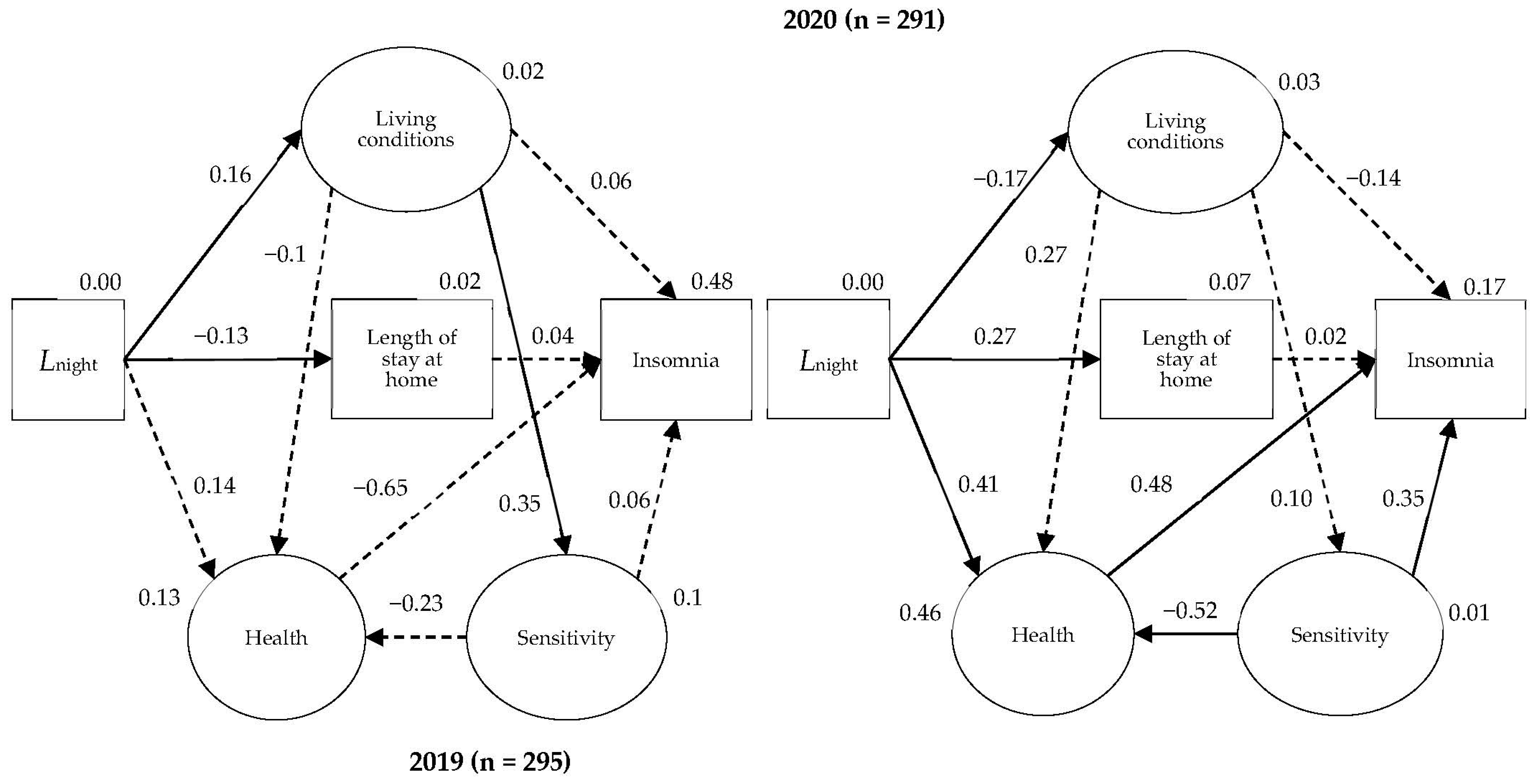
3.5. Comparison of Insomnia Model between the 2019 and 2020 Surveys
- Insomnia was influenced by sensitivity, health, living conditions, and the opening of the bedroom window during the dry season.
- Noise exposure (Lnight) had a direct impact on living conditions.
- Insomnia was influenced directly or indirectly by living conditions through sensitivity.
- Noise exposure (Lnight) indirectly influenced insomnia via the opening of bedroom windows during the dry season.
- Noise exposure (Lnight), living conditions, and sensitivity had an impact on health.
4. Discussion
4.1. Causal Structure of Noise Annoyance and Insomnia in the Context of the Noise Reduction
4.2. Effect of COVID-19 Pandemic on Community Perception of Aircraft Noise
4.3. Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Commission. Position Paper on Dose Response Relationships between Transportation Noise and Annoyance, EU’s Future Noise Policy WG2–Dose/Effect; European Commission: Brussels, Belgium, 2002. [Google Scholar]
- Guski, R.; Schreckenberg, D.; Schuemer, R. WHO environmental noise guidelines for the European region: A systematic review on environmental noise and annoyance. Int. J. Environ. Res. Public Health 2017, 14, 1539. [Google Scholar] [CrossRef] [PubMed]
- Basner, M.; McGuire, S. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Effects on Sleep. Int. J. Environ. Res. Public Health 2018, 15, 519. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Regional Office for Europe. WHO Environmental Noise Guidelines for the European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- World Health Organization. Burden of Disease from Environmental Noise. Quantification of Healthy Life Years Lost in Europe; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2011. [Google Scholar]
- Floud, S.; Blangiardo, M.; Clark, C.; de Hoogh, K.; Babisch, W.; Houthuijs, D.; Swart, W.; Pershagen, G.; Katsouyanni, K.; Velonakis, M.; et al. Exposure to aircraft and road traffic noise and associations with heart disease and stroke in six European countries: A cross-sectional study. Environ. Health 2013, 12, 89. [Google Scholar] [CrossRef]
- Münzel, T.; Sørensen, M.; Gori, T.; Schmidt, F.P.; Rao, X.; Brook, J.R.; Chen, L.C.; Brook, R.D.; Rajagopalan, S. Environmental stressors and cardio-metabolic disease: Part I-Epidemiologic evidence supporting a role for noise and air pollution and effects of mitigation strategies. Eur. Hear. J. 2017, 38, 550–556. [Google Scholar] [CrossRef] [PubMed]
- De Kluizenaar, Y.; Salomons, E.M.; Janssen, S.A.; van Lenthe, F.J.; Vos, H.; Zhou, H.; Miedema, H.M.E.; Mackenbach, J.P.; Julkunen, J.; Roininen, J. Urban road traffic noise and annoyance: The effect of a quiet façade. Eur. J. Public Health 2011, 21, 232–237. [Google Scholar] [CrossRef]
- Miedema, H.M.E.; Vos, H. Demographic and attitudinal factors that modify annoyance from transportation noise. J. Acoust. Soc. Am. 1999, 105, 3336–3344. [Google Scholar] [CrossRef]
- Guski, R. Chapter 4. Community response to environmental noise. In Environmental Urban Noise; Garcia, A., Ed.; WIT Press: Southampton, UK, 2001. [Google Scholar]
- Schreckenberg, D.; Hong, J. Research on Community Response to Noise 2017 to 2021. In Proceedings of the 13th ICBEN Congress on Noise as a Public Health Problem, Stockholm, Sweden, 14–17 June 2021. [Google Scholar]
- Basner, M.; Griefahn, B.; Berg, M.D. Aircraft noise effects on sleep: Mechanisms, mitigation and research needs. Noise Health 2014, 16, 123–137. [Google Scholar] [CrossRef]
- Schütte, M.; Marks, A.; Wenning, E.; Griefahn, B.; Theorell, T. Annoyance caused by environmental noise: Elements for evidence-based noise policies. J. Environ. Psychol. 2014, 40, 246–258. [Google Scholar] [CrossRef]
- Civil Aviation Authority of Vietnam. Delay in Flight Operations at Tan Son Nhat-Causes and Solutions. 2019. Available online: https://caa.gov.vn/hoat-dong-nganh/cham-tre-hoat-dong-bay-tai-tan-son-nhat-nguyen-nhan-va-giai-phap-20190820095050690.htm (accessed on 22 February 2021).
- Trieu, B.L.; Nguyen, T.L.; Hiraguri, Y.; Morinaga, M.; Morihara, T. How does a community respond to changes in aircraft noise? A comparison of two surveys conducted 11 years apart in Ho Chi Minh City. Int. J. Environ. Res. Public Health 2021, 18, 4307. [Google Scholar] [CrossRef]
- Brown, A.L.; Van Kamp, I. WHO environmental noise guidelines for the European region: A systematic review of transport noise interventions and their impacts on health. Int. J. Environ. Res. Public Health 2017, 14, 873. [Google Scholar] [CrossRef]
- Brink, M.; Wirth, K.E.; Schierz, C.; Thomann, G.; Bauer, G. Annoyance responses to stable and changing aircraft noise exposure. J. Acoust. Soc. Am. 2008, 124, 2930–2941. [Google Scholar] [CrossRef]
- Fidell, S.; Silvati, L.; Haboly, E. Social survey of community response to a step change in aircraft noise exposure. J. Acoust. Soc. Am. 2002, 111, 200–209. [Google Scholar] [CrossRef]
- Nguyen, T.T.H.N.; Trieu, B.L.; Nguyen, T.L.; Morinaga, M.; Morihara, T.; Hiraguri, Y.; Sasazawa, Y. How the causal structures of noise annoyance and sleep effects changed under the significant decrease of aircraft noise. In Proceedings of the INTER-NOISE and NOISE-CON Congress, InterNoise 22, Glasgow, UK, 21–24 August 2022; Institute of Noise Control Engineering: Glasgow, UK, 2022; pp. 5873–5883. [Google Scholar]
- Nguyen, T.L.; Trieu, B.L.; Hiraguri, Y.; Morinaga, M.; Morihara, T.; Yano, T. Effects of changes in acoustic and non-acoustic factors on public health and reactions: Follow-up surveys in the vicinity of the Hanoi Noi Bai International Airport. Int. J. Environ. Res. Public Health 2020, 17, 2597. [Google Scholar] [CrossRef]
- ISO/TS 15666:2021; Acoustics—Assessment of Noise Annoyance by Means of Social and Socio-Acoustic Surveys. International Organization for Standardization: Geneva, Switzerland, 2021.
- Asano, H.; Takeuchi, K.; Sasazawa, Y.; Otani, T.; Koyama, H.; Suzuki, S. Predictive validity of the total health index for all-cause mortality assessed in the Komo-Ise cohort. J. Epidemiol. 2008, 18, 68–76. [Google Scholar] [CrossRef]
- CESD. R Explanation. Available online: https://cesd-r.com (accessed on 12 May 2019).
- Sasazawa, Y.; Koja, A. Epidemiological Study in Order to the Effect of Kadena Base Noise on Resident’s Health—Focusing of Insomnia and Hypertention of Government Workers Near the Base. In Proceedings of Acoustical Society of Japan; [CD-ROM]; TC Noise and Vibration: Okinawa, Japan, 2018. (In Japanese) [Google Scholar]
- McCullagh, M.C. Validation of a questionnaire to identify hearing loss among farm operators. Noise Health 2012, 14, 32–38. [Google Scholar] [CrossRef]
- Buysse, D.J.; Ancoli-Israel, S.; Edinger, J.D.; Lichstein, K.L.; Morin, C.M. Recommendations for a standard research assessment of insomnia. Sleep 2006, 29, 1155–1173. [Google Scholar] [CrossRef]
- Federal Aviation Administration. Integrated Noise Model 7.0 (INM). 2015. Available online: https://www.faa.gov/regulations_policies/policy_guidance/noise/models/inm/ (accessed on 25 December 2019).
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- General Statistics Office of Vietnam. Viet Nam Population and HOUSING Census. 2019. Available online: http://tongdieutradanso.vn/ket-qua-tong-dieu-tra-dan-so-va-nha-o-thoi-diem-0-gio-ngay-01-thang-4-nam-2019.html (accessed on 22 February 2021).
- Stansfeld, S.A. Noise, noise sensitivity and psychiatric disorder: Epidemiological and psychophysiological studies. Psychol. Med. 2015, 45, 331–341. [Google Scholar] [CrossRef]
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and non-auditory effects of noise on health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef]
- Nguyen, T.L.; Morihara, T.; Yano, T.; Yokoshima, S. Structural equation models of road traffic and aircraft noise annoyance in Vietnam. Noise Control Eng. J. 2018, 66, 459–471. [Google Scholar] [CrossRef]
- Guski, R. Health effects of aircraft noise. Aviat. Space Environ. Med. 1999, 70 (Suppl. 5), A52–A60. [Google Scholar]
- Stansfeld, S.A.; Matheson, M.P. Noise pollution: Non-auditory effects on health. Br. Med. Bull. 2003, 68, 243–257. [Google Scholar] [CrossRef] [PubMed]
- Ristovska, G.; Laszlo, H.E.; Hansell, A.L.; Clark, C.; Smith, B.H. Associations between self-reported sleep disturbance and environmental noise based on reanalyses of pooled data from 24 studies. Behav. Sleep Med. 2014, 14, 1–23. [Google Scholar]
- Janssen, S.A.; Vos, H.; Eisses, A.R.; Pedersen, E. A comparison between exposure-response relationships for wind turbine annoyance and annoyance due to other noise sources. J. Acoust. Soc. Am. 2011, 130, 3746–3753. [Google Scholar] [CrossRef]
- Muzet, A. Environmental noise, sleep and health. Sleep Med. Rev. 2007, 11, 135–142. [Google Scholar] [CrossRef]
- Shepherd, D.; Welch, D.; Dirks, K.N. Exploring the relationship between noise sensitivity, annoyance and health-related quality of life in a sample of adults exposed to environmental noise. Int. J. Environ. Res. Public Health 2010, 7, 3579–3594. [Google Scholar] [CrossRef]
- Croy, I.; Smith, M.G.; Ellermeier, W. A cross-modal comparison of perceived and physiological responses to environmental acoustics. J. Environ. Psychol. 2013, 35, 40–47. [Google Scholar]
- Hornberg, J.; Haselhoff, T.; Lawrence, B.; Fischer, J.; Ahmed, S.; Gruehn, D.; Moebus, S. Impact of the COVID-19 Lockdown Measures on Noise Levels in Urban Areas-A Pre/during Comparison of Long-Term Sound Pressure Measurements in the Ruhr Area, Germany. Int. J. Environ. Res. Public Health 2021, 18, 4653. [Google Scholar] [CrossRef]
- European Environment Agency. Environmental Noise in Europe: 2020; EEA Report No 14/2020; Publications Office of the European Union: Luxembourg, 2020. [Google Scholar]
- Jelicic, M.; Pavičić, D.; Jakovljević, B. The effect of the COVID-19 pandemic on noise annoyance in urban areas. Environ. Res. 2020, 191, 110177. [Google Scholar] [CrossRef]
- Wojciechowska, W.; Gocłowska, E.; Śliwińska-Kowalska, M.; Kaczmarska, J.; Kowalski, M.L.; Skarżyński, P.H.; Pawlaczyk-Łuszczyńska, M. Blood pressure and arterial stiffness in association with aircraft noise exposure: Long- term observation and the potential effect of COVID-19 lockdown. Hypertension 2021, 78, 325–334. [Google Scholar]
- Basner, M.; Witte, M.; McGuire, S. Aircraft noise effects on sleep-results of a pilot study near Philadelphia International Airport. Int. J. Environ. Res. Public Health 2019, 16, 3178. [Google Scholar] [CrossRef]
- Gandotra, K.; E Jaskiw, G.; Wilson, B.; Konicki, P.E.; E Rosenberg, C.; Strohl, K.P. Infrasound emitted by wind turbines and sleep: Results from the randomized PiCross study. Sleep 2019, 42, zsz144. [Google Scholar] [CrossRef]
- Brink, M.; Schäffer, B.; Vos, H.; Ängquist, K.-A.; Larsen, J.C.; Almgren, O.; Krog, N.H.; Persson Waye, K.; Forssén, J.; Pedersen, E.; et al. Health effects from low-frequency noise and infrasound in the general population: Is it time to listen? Lancet 2011, 377, 246–248. [Google Scholar] [CrossRef]
- Fidell, S.; Silvati, L.; Pearsons, K.; Lind, S.; Howe, R. Field study of the annoyance of low-frequency runway sideline noise. J. Acoust. Soc. Am. 1995, 97, 31–41. [Google Scholar] [CrossRef]
- Buikema, E.; Vercammen, M.; van Wee, B.; Miedema, H. Development of a rating procedure for low frequency noise: Results of measurements near runways. J. Sound Vib. 2010, 329, 5163–5175. [Google Scholar] [CrossRef]
- Hodgdon, K.K.; Atchley, A.A.; Bernhard, R.J. Final Report PARTNER Low-Frequency Noise Study; No. PARTNER-COE-2007-001; Partnership for Air Transportation Noise and Emissions Reduction, Massachusetts Institute of Technology: Cambridge, MA, USA, 2017. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Annoyance |
| Question: Thinking about the last 12 months (1st survey)/3 months (2nd survey)/4 months (3rd survey) or so, what number from 0 to 10 best shows how much you are bothered, disturbed, or annoyed by aircraft noise? |
| Evaluation scale: 11-point numerical scale from 0 (not annoyed at all) to 10 (extremely annoyed) |
| Insomnia |
| Question: Please answer this question regarding your sleep: |
| (a) Do you have any trouble sleeping? No/Yes |
| (b) If you answered “Yes” to the above question, please choose the corresponding alternative (alternatives: rarely or not at all; once or twice a week; more than three times a week) for the following items: (1) it is difficult to fall asleep; (2) when awakened during the night, it is difficult to sleep again; (3) awakened early in the morning; (4) do not wake the next morning with the feeling of having slept well; (5) sleepy during daytime and cannot work well; (6) other |
| Evaluation scale: 1: have no insomnia symptoms (*); 2: have insomnia symptoms |
| (*) Respondents with insomnia symptoms responded affirmatively to question (a): Do you have any trouble with your sleep? They also responded with (5), sleepiness during daytime and inability to work well more than three times a week, and that they had experienced at least one of the other symptoms (1)–(4) more than three times per week. |
| Latent Variable | Observed Variable | Question | Scale |
|---|---|---|---|
| Residential factors | Housing type | What type of house ownership do you have? | 1: Owned 2: Rented 3: Other |
| Housing structure | Structure of the house? | 1: Wooden 2: Bricks 3: Prefabricated 4: Reinforced concrete 5: Reinforced concrete with brick wall 6: Other | |
| Number of glass layers in living room windows and doors | How many glass layers do your living room windows and doors have? If they are double-paned windows/doors, please specify as 2 layers. | 1: More than 3 layers 2: 2 layers 3: 1 layer 4: Other | |
| Type of frame of living room windows and doors | Which type of frame among the following types do your living room windows and doors have? | 1: Aluminum frame 2: Wooden frame 3: Plastic frame 4: Other | |
| Number of glass layers in bedroom windows and doors | How many glass layers do your bedroom windows and doors have? If they are multi-layer double-paned windows/doors, please specify as 2 layers. | 1: More than 3 layers 2: 2 layers 3: 1 layer 4: Other | |
| Type of frame of bedroom windows and doors | Which type of frame among the following types do your bedroom windows and doors have? | 1: Aluminum frame 2: Wooden frame 3: Plastic frame 4: Other | |
| Coping capacity | Opening of bedroom windows (% Often and Always) | Do you open bedroom windows while sleeping in the dry/rainy season? | 1: Rarely to 4: Always |
| Number of hours staying at home | Thinking about the last 4 months, how much of the day do you spend at home? | 1: Under 8 h 2: 8–15 h 3: Over 15 h hours | |
| Health | Effects on sleep | How often do you have any trouble getting to sleep or staying asleep? | 1: Often 2: Sometimes 3: Almost never |
| Stress | Thinking about the amount of stress in your life, how stressful would you say that most days are? | 0: Not at all to 10: Extremely | |
| Life satisfaction | How do you feel about your life as a whole right now? | 0: Very dissatisfied to 10: Satisfied | |
| Self-reported health status | Do you usually have periodic health examination? | 1: No 2: Yes | |
| Awareness of nutrition balance | Do you think about the nutritional balance of your diet? | 1: Do not think about it to 4: Think a lot | |
| Salt intake | Do you eat or drink salty food or soup? | 1: Not often 2: Once a day 3: Every meal | |
| Alcohol intake | How often do you drink alcohol? | 1: Not at all 2: 2–3 times a month or less 3: 1–4 days a week 4: Almost every day | |
| Smoking habit | Do you smoke cigarettes? | 1: Not at all 2: I smoked before but stopped 3: 20 or less per day 4: More than 20 per day | |
| Exercise frequency | How often do you engage in physical activity over 30 min? | 1: Almost everyday 2: 4–5 times a week 3: 2–3 times a week 4: About once a week 5: Once or twice a month 6: Not at all | |
| Morbidity | Have you ever had any of these conditions? 1. Heart trouble 2. High blood pressure or hypertension 3. Hyperlipidemia 4. Stroke, small stroke, or TIA 5. Asthma 6. Diabetes 7. Cancer 8. Depression or neurosis 9. Other | 0: No diseases 1: Diseases | |
| Body Mass Index (BMI) | What is your height and weight? | 0: BMI < 29 1: BMI > 29 (obese) | |
| Personal and attitudinal factors | In daily life, how sensitive are you to the following climatic factors and environmental conditions | ||
| Noise | Noise? | 1: Not at all to 5: Extremely | |
| Cold | Cold? | 1: Not at all to 5: Extremely | |
| Heat | Heat? | 1: Not at all to 5: Extremely | |
| Odors | Odors? | 1: Not at all to 5: Extremely | |
| Vibration | Vibration? | 1: Not at all to 5: Extremely | |
| Sex | Gender of respondent? | 1: Male 2: Female | |
| Job | What is your job? | 1. Employed 2. Student 3. Homemaker 4. Retired 5. Unemployed | |
| Age | How old are you? | 0: <60 years old 1: >=60 years old | |
| Residence period length | How long have you been living in your present house? | 0: >5 years 1: <=5 years | |
| Living conditions | Please evaluate your living area according to the following items: | ||
| Green space | Green space? | 1: Extremely good to 5: Extremely bad | |
| Street scenery | Street scenery? | 1: Extremely good to 5: Extremely bad | |
| View | View? | 1: Extremely good to 5: Extremely bad | |
| Quietness | Quietness? | 1: Extremely good to 5: Extremely bad | |
| Work convenience | Work convenience? | 1: Extremely good to 5: Extremely bad | |
| Education convenience | Education convenience? | 1: Extremely good to 5: Extremely bad | |
| Health care convenience | Health care convenience? | 1: Extremely good to 5: Extremely bad | |
| Daily life service convenience | Daily life service convenience? | 1: Extremely good to 5: Extremely bad | |
| Transport convenience | Transport convenience? | 1: Extremely good to 5: Extremely bad |
| 1st Survey | 2nd Survey | 3rd Survey | Vietnam Census (2019) * | ||
|---|---|---|---|---|---|
| Number of respondents | 502 | 145 | 519 | ||
| Response rate (%) | 60.3 | 28.9 | 68.6 | ||
| Sex | Male | 46.2 | 46.5 | 49.2 | 49.9 |
| Female | 53.8 | 53.5 | 50.8 | 50.1 | |
| Age | <60 years old | 81.9 | 70.6 | 89.9 | 88.1 |
| ≥60 years old | 18.1 | 29.4 | 10.1 | 11.9 | |
| Length of Residence | 0–5 years | 51.1 | 27.7 | 40.0 | |
| More than 5 years | 48.9 | 72.3 | 60.0 | ||
| Occupation | Employed | 53.6 | 37.4 | 40.0 | 55.5 |
| Student, housewife, retired, unemployed | 46.4 | 62.6 | 60.0 | 44.5 | |
| Site | Lden a (in Parentheses: SD) | Lnight b (in Parentheses: SD) | ∆Lden | ∆Lnight | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1st (SD) | 2nd (SD) | 3rd (SD) | 1st (SD) | 2nd (SD) | 3rd (SD) | 2nd–1st | 3rd–1st | 2nd–1st | 3rd–1st | |
| 1 | 66 (0.9) | 61 (1.1) | 60 (0.9) | 58 (0.9) | 52 (1.1) | 52 (0.9) | −5 | −6 | −6 | −6 |
| 2 | 64 (0.9) | 61 (1.1) | 61 (0.9) | 57 (0.9) | 52 (1.1) | 53 (0.9) | −3 | −3 | −5 | −3 |
| 3 | 64 (2.3) | 60 (3.0) | 59 (1.6) | 56 (2.3) | 51 (3.0) | 51 (1.5) | −4 | −5 | −5 | −5 |
| 4 | 62 (1.1) | 57 (1.2) | 57 (1.1) | 55 (1.1) | 48 (1.2) | 49 (1.1) | −5 | −6 | −6 | −6 |
| 5 | 81 (1.4) | 76 (1.2) | 73 (1.8) | 73 (1.8) | 67 (1.3) | 66 (1.7) | −5 | −7 | −7 | −8 |
| 6 | 75 (0.4) | 71 (0.5) | 69 (0.7) | 67 (1.2) | 61 (0.5) | 61 (0.7) | −4 | −6 | −6 | −6 |
| 7 | 69 (0.6) | 65 (0.7) | 64 (1.5) | 61 (0.6) | 56 (0.6) | 56 (1.4) | −4 | −5 | −5 | −5 |
| 8 | 66 (0.2) | 62 (0.1) | 62 (0.1) | 58 (0.2) | 53 (0.1) | 54 (0.1) | −4 | −4 | −6 | −5 |
| 9 | 64 (0.2) | 59 (0.3) | 60 (0.2) | 57 (1.4) | 50 (0.3) | 52 (0.2) | −5 | −4 | −7 | −5 |
| 10 | 67 (1.3) | 62 (1.8) | 65 (0.6) | 59 (1.5) | 54 (1.7) | 57 (0.6) | −5 | −2 | −6 | −2 |
| 11 | 47 (0.5) | 43 (0.2) | 43 (0.3) | 40 (0.5) | 34 (0.2) | 36 (0.3) | −5 | −4 | −6 | −4 |
| 12 | 45 (0.9) | 41 (0.2) | 41 (0.2) | 38 (0.9) | 33 (0.2) | 34 (0.2) | −4 | −4 | −5 | −4 |
| Noise Level Ranges Lden a (dB) | |||||
| 0–44 | 45–50 | 51–55 | 56–81 | ||
| 1st survey (all data) | % | 0.0 | 12.2 | 0.0 | 87.8 |
| Response number/N | 0/502 | 61/502 | 0/502 | 441/502 | |
| 1st survey (145 data) | % | 0.0 | 11.7 | 0.0 | 88.3 |
| Response number/N | 0/502 | 17/145 | 0/145 | 128/145 | |
| 2nd survey | % | 12.4 | 0.0 | 29.7 | 57.9 |
| Response number/N | 18/145 | 0/145 | 43/145 | 84/145 | |
| 3rd survey | % | 17.0 | 0.0 | 0.0 | 83.0 |
| Response number/N | 88/519 | 0/519 | 0/519 | 431/519 | |
| Noise Level Ranges Lnight b (dB) | |||||
| 0–39 | 40–45 | 46–51 | 52–79 | ||
| 1st survey (all data) | % | 5.8 | 6.4 | 0.0 | 87.8 |
| Response number/N | 29/502 | 32/502 | 0/502 | 441/502 | |
| 1st survey (145 data) | % | 1.4 | 10.3 | 0 | 88.3 |
| Response number/N | 2/145 | 15/145 | 0/145 | 128/145 | |
| 2nd survey | % | 11.7 | 0.0 | 31.1 | 57.2 |
| Response number/N | 17/145 | 0/145 | 45/145 | 83/145 | |
| 3rd survey | % | 17.0 | 0.0 | 27.7 | 55.3 |
| Response number/N | 88/519 | 0/519 | 144/519 | 287/519 | |
| Site | 1st Survey (in Parentheses: All Data) | 2nd Survey | 3rd Survey | ||||||
|---|---|---|---|---|---|---|---|---|---|
| %HA a | %ISM b | N c | %HA a | %ISM b | N c | %HA a | %ISM b | N c | |
| 1 | 0.0 (0.0) | 0.0 (0.0) | 5 (49) | 40.0 | 0.0 | 5 | 2.0 | 11.9 | 50 |
| 2 | 0.0 (7.3) | 0.0 (2.6) | 2 (44) | 0.0 | 0.0 | 2 | 17.1 | 0.0 | 35 |
| 3 | 0.0 (0.0) | 40.0 (6.5) | 5 (31) | 0.0 | 20.0 | 5 | 28.6 | 2.0 | 49 |
| 4 | 0.0 (2.0) | 8.3 (2.0) | 36 (50) | 2.8 | 11.1 | 36 | 9.1 | 0.0 | 44 |
| 5 | 0.0 (3.0) | 0.0 (0.0) | 10 (33) | 30.0 | 10.0 | 10 | 7.9 | 5.3 | 38 |
| 6 | 7.7 (18.4) | 7.7 (6.4) | 13 (50) | 7.7 | 7.7 | 13 | 2.4 | 0.0 | 42 |
| 7 | 13.0 (12.5) | 0.0 (0.0) | 24 (50) | 4.3 | 0.0 | 24 | 0.0 | 0.0 | 40 |
| 8 | 8.3 (6.3) | 0.0 (2.8) | 14 (36) | 0.0 | 0.0 | 14 | 4.0 | 0.0 | 50 |
| 9 | 0.0 (0.0) | 0.0 (2.4) | 7 (48) | 0.0 | 20.0 | 7 | 4.0 | 0.0 | 50 |
| 10 | 10.0 (2.2) | 9.1 (2.0) | 12 (50) | 8.3 | 12.5 | 12 | 3.0 | 3.2 | 33 |
| 11 | 0.0 (0.0) | 0.0 (3.3) | 15 (32) | 0.0 | 0.0 | 15 | 72.5 | 0.0 | 40 |
| 12 | 0.0 (0.0) | 0.0 (0.0) | 2 (29) | 0.0 | 0.0 | 2 | 0.0 | 0.0 | 48 |
| Total | 4.4 (4.8) | 5.1 (2.3) | 145 (502) | 7.6 | 7.5 | 145 | 12.1 | 1.8 | 519 |
| Noise Level Ranges Lden a (dB) | p-Value | |||||
|---|---|---|---|---|---|---|
| 0–59 | 60–64 | 65–69 | 70–81 | |||
| 1st survey (all data) | %HA | 0.0 | 0.7 | 4.0 | 12.0 | 0.0012 * |
| Response number/N | 0/61 | 1/147 | 6/161 | 16/133 | ||
| 1st survey (145 data) | %HA | 0.0 | 0.0 | 5.4 | 8.7 | 0.2152 (n.s) |
| Response number/N | 0/17 | 0/45 | 2/37 | 4/46 | ||
| 2nd survey | %HA | 1.6 | 7.9 | 4.3 | 17.4 | 0.0085 * |
| Response number/N | 1/61 | 3/38 | 1/23 | 4/23 | ||
| 3rd survey | %HA | 15.5 | 13.8 | 0.0 | 5.0 | <0.0001 * |
| Response number/N | 36/232 | 23/167 | 0/40 | 4/80 | ||
| Noise Level Ranges Lnight a (dB) | p-Value | |||||
|---|---|---|---|---|---|---|
| 0–54 | 55–59 | 60–64 | 65–79 | |||
| 1st survey (all data) | %ISM | 1.6 | 2.3 | 2.0 | 3.6 | 0.5049 (n.s) |
| Response number/N | 1/61 | 6/258 | 2/100 | 3/83 | ||
| 1st survey (145 data) | %ISM | 0.0 | 7.1 | 0.0 | 0.0 | 0.4691 (n.s) |
| Response number/N | 0/17 | 5/70 | 0/35 | 0/23 | ||
| 2nd survey | %ISM | 9.8 | 0.0 | 0.0 | 0.0 | 0.5768 (n.s) |
| Response number/N | 9/92 | 0/23 | 0/13 | 0/10 | ||
| 3rd survey | %ISM | 1.9 | 1.7 | 0.0 | 5.3 | 0.1478 |
| Response number/N | 7/366 | 1/73 | 0/42 | 2/38 | ||
| Factors | Categories | 1st Survey—All Data | 1st Survey—145 Data | 2nd Survey | 3rd Survey |
|---|---|---|---|---|---|
| Residential factors | |||||
| Housing type | Owned | 64.9 (321) | 76.9 (110) | ※ | 78.4 (407) |
| Floor Area/Width of house | ≤50 m2 | 59.1 (269) | 65.9 (89) | ※ | 66.2 (129) |
| Housing structure | 1. Wooden | 2.1 (7) | 0 (0) | ※ | 0.8 (4) |
| 2. Brick | 14.5 (49) | 7.6 (7) | 25.1 (124) | ||
| 3. Prefabricated | 0.3 (1) | 0 (0) | 0.6 (3) | ||
| 4. Reinforced concrete | 44.8 (151) | 52.2 (48) | 20.4 (101) | ||
| 5. Reinforced concrete with brick wall | 34.4 (116) | 37 (34) | 53.1 (263) | ||
| 6. Other | 3.9 (13) | 3.3 (3) | 0.0 (0) | ||
| Number of glass layers in living room windows and doors | 1. More than 3 layers | 2.7 (13) | 1.4 (2) | ※ | 3.3 (16) |
| 2. 2 layers | 18.2 (89) | 19.3 (27) | 18.6 (91) | ||
| 3. 1 layer | 75.3 (369) | 74.3 (104) | 71.8 (351) | ||
| 4. Other (the window has no glass) | 3.9 (19) | 5 (7) | 6.1 (30) | ||
| Type of frame of living room windows and doors | 1. Aluminum frame | 31.7 (156) | 24.8 (35) | ※ | 42.2 (213) |
| 2. Wooden frame | 14.2 (70) | 7.1 (10) | 16 (81) | ||
| 3. Plastic frame | 1.4 (7) | 0 (0) | 1.4 (7) | ||
| 4. Other | 52.6 (259) | 68.1 (96) | 40.4 (204) | ||
| Number of glass layers in bedroom windows and doors | 1. More than 3 layers | 1.2 (6) | 37 (51) | ※ | 57.2 (214) |
| 2. 2 layers | 13.5 (66) | 6.5 (9) | 16.6 (62) | ||
| 3. 1 layer | 77.7 (379) | 0 (0) | 1.9 (7) | ||
| 4. Other (the window has no glass) | 7.6 (37) | 56.5 (78) | 24.3 (91) | ||
| Type of frame of bedroom windows and doors | 1. Aluminum frame | 37.3 (181) | 0 (0) | ※ | 2.2 (8) |
| 2. Wooden frame | 20.0 (97) | 12.9 (18) | 25.1 (91) | ||
| 3. Plastic frame | 2.7 (13) | 77.7 (108) | 64.2 (233) | ||
| 4. Other | 40.0 (194) | 9.4 (13) | 8.5 (31) | ||
| Personal and attitudinal factors | |||||
| Sex | Male | 46.2 (229) | 46.5 (66) | ※ | 49.2 (255) |
| Age | ≥60 years old | 18.1 (90) | 25.4 (36) | ※ | 10.1 (52) |
| Residence length | ≤5 years | 41.7 (204) | 27.7 (39) | ※ | 40.0 (204) |
| Residential area preference and quality (% bad and extremely bad) | 1. Green space | 12.3 (60) | 12.9 (18) | 4.9 (7) | 21.4 (110) |
| 2. Street scenery | 7.9 (38) | 7.2 (10) | 3.5 (5) | 16.7 (83) | |
| 3. View from houses | 8.0 (39) | 7.9 (11) | 7.0 (10) | 16.1 (80) | |
| 4. Quietness | 9.0 (43) | 13.0 (18) | 21.1 (30) | 9.0 (45) | |
| 5. Work convenience | 3.8 (18) | 2.2 (3) | 1.4 (2) | 2.0 (10) | |
| 6. Education convenience | 1.9 (9) | 0.7 (1) | 2.8 (4) | 2.0 (10) | |
| 7. Health care convenience | 3.4 (16) | 2.9 (4) | 1.4 (2) | 2.8 (14) | |
| 8. Daily life service convenience | 1.3 (6) | 1.5 (2) | 0.7 (1) | 2.0 (10) | |
| 9. Transport convenience | 4.4 (21) | 2.9 (4) | 10.5 (15) | 6.6 (33) | |
| Opening of bedroom windows (% often and always) | 1. Dry season | 31.2 (140) | 15.9 (20) | ※ | 45.1 (233) |
| 2. Rainy season | 17.9 (81) | 28.0 (35) | 32.5 (166) | ||
| Sensitivity (% very and extremely) | 1. Cold | 2.9 (14) | 1.4 (2) | 1.6 (2) | 2.2 (11) |
| 2. Heat | 15.6 (75) | 12.1 (17) | 17.5 (22) | 36.7 (177) | |
| 3. Noise | 16.1 (78) | 16.4 (23) | 14.3 (20) | 13.7 (67) | |
| 4. Vibration | 8.5 (41) | 7.9 (11) | 10.9 (15) | 6.6 (31) | |
| 5. Chemicals | 5.4 (26) | 5.0 (7) | 0.8 (1) | 3.4 (16) | |
| 6. Odors | 8.8 (42) | 8.6 (12) | 8.9 (11) | 12.9 (62) | |
| 7. Dust, pollen, polluted air | 6.7 (32) | 8.6 (12) | 5 (8) | 2.6 (12) | |
| Job | 1. Employed | 53.6 (266) | 51.8 (72) | 37.4 (52) | 40.0 (207) |
| 2. Student | 9.3 (46) | 5.0 (7) | 0 (0) | 4.3 (22) | |
| 3. Homemaker | 13.1 (65) | 15.8 (22) | 4.3 (6) | 16.2 (84) | |
| 4. Retired | 9.7 (48) | 15.8 (22) | 15.8 (22) | 6.8 (35) | |
| 5. Unemployed | 14.3 (71) | 14.4 (2) | 13.7 (19) | 32.7 (169) | |
| Number of hours staying at home | 1. Under 8 h | 30.6 (149) | 21.6 (30) | 7.7 (11) | 14.2 (72) |
| 2. From 8 to 15 h | 36.6 (178) | 35.3 (49) | 41.3 (59) | 60.6 (307) | |
| 3. Above 15 h | 32.6 (159) | 43.2 (60) | 50.3 (72) | 24.9 (126) | |
| Life satisfaction | Very dissatisfied | 1.0 (5) | 0.7 (1) | 4.2 (6) | 0.8 (4) |
| Health-related factors | |||||
| Self-rated health status | Fair or Poor | 23.6 (115) | 25.4 (36) | 25.9 (37) | 9.3 (47) |
| Stress | Quite or extremely stressful | 8.0 (39) | 0.0 (0) | 3.5 (5) | 5.6 (28) |
| Morbidity | 1. Heart trouble | 5.5 (24) | 7.6 (9) | 7.0 (9) | 1.4 (7) |
| 2. High blood pressure or hypertension | 8.4 (37) | 15.1 (18) | 20.1 (27) | 9.7 (49) | |
| 3. Hyperlipidemia | 4.3 (19) | 6.7 (8) | 3.0 (4) | 0.4 (2) | |
| 4. Stroke, small stroke, or TIA | 0.2 (1) | 0.8 (1) | 1.5 (2) | 0.0 (0) | |
| 5. Asthma | 0.7 (3) | 0.0 (0) | 0.0 (0) | 0.6 (3) | |
| 6. Diabetes | 3.9 (17) | 6.7 (8) | 7.5 (10) | 3.0 (15) | |
| 7. Cancer | 0.2 (1) | 0.0 (0) | 0.0 (0) | 0.0 (0) | |
| 8. Depression or Neurosis | 0.5 (2) | 0.8 (1) | 0.7 (1) | 0.0 (0) | |
| 9. Other | 8.7 (38) | 12.6 (15) | 8.2 (11) | 0.8 (4) | |
| Salt intake | Very high | 4.6 (22) | 5.0 (7) | 3.1 (13) | |
| Awareness of nutrition balance | No thought given to it | 12.7 (61) | 16.4 (23) | 10.3 (51) | |
| Alcohol intake | Almost everyday | 1.6 (8) | 1.4 (2) | 1.6 (8) | |
| Smoking habit | Smoking | 13.6 (67) | 15.3 (22) | 15.3 (22) | 18.6 (93) |
| Exercise frequency | Above 4 times a week | 37.0 (182) | 64.3 (92) | 56.0 (79) | 32.1 (161) |
| Body Mass Index (BMI) | Obesity (BMI > 29) | 2.3 (11) | 2.9 (4) | 3.5 (3) | 1.0 (5) |
| Variables | Question | Scale |
|---|---|---|
| Frequency of opening bedroom windows | Do you open bedroom windows while sleeping in the dry/rainy season? | 1: Rarely to 4: Always |
| Length of time at home | Thinking about the last twelve months (1st survey)/three months (2nd survey)/four months (3rd survey), how much of the day do you spend at home? | 1: <8 h 2: 8–15 h 3: >15 h |
| Sleep disturbances | How often do you have any trouble getting to sleep or staying asleep? | 1: Seldom 2: Sometimes 3: Often |
| Stress | Thinking about the amount of stress in your life, would you say that most days are stressful? | 0: Not at all to 10: Extremely |
| Nutrition | Do you think about the nutritional balance of your diet? | 1: Think a lot to 4: Do not think about it |
| Personal sensitivity | In daily life, how sensitive are you to the following environmental conditions: noise, coldness, odors, vibration | 1: Not at all to 5: Extremely |
| Residential area preference and quality | Please evaluate your living area according to the following items: green space, street scenery, view from living areas. | 1: Extremely good to 5: Extremely bad |
| Parameter | 2019 | 2020 | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | SE | CR | p | Estimate | SE | CR | p | |
| Living conditions ← Lden | 0.010 | 0.004 | 2.549 | 0.011 | −0.005 | 0.004 | −1.282 | 0.200 |
| Sensitivity ← Living conditions | 0.555 | 0.149 | 3.724 | * | 0.070 | 0.038 | 1.838 | 0.066 |
| Health ← Lden | −0.001 | 0.001 | −0.912 | 0.362 | −0.005 | 0.003 | −2.093 | 0.036 |
| Open window ← Lden | −0.006 | 0.007 | −0.851 | 0.395 | −0.030 | 0.005 | −5.490 | * |
| Health ← Living conditions | 0.051 | 0.055 | 0.942 | 0.346 | 0.007 | 0.027 | 0.253 | 0.801 |
| Health ← Sensitivity | 0.155 | 0.016 | 0.931 | 0.352 | 0.180 | 0.087 | 2.058 | 0.040 |
| Annoyance ← Open window | −0.127 | 0.104 | −1.222 | 0.222 | −0.759 | 0.166 | −4.565 | * |
| Annoyance ← Health | −79.810 | 88.806 | −0.899 | 0.369 | 5.677 | 2.666 | 2.130 | 0.033 |
| Annoyance ← Sensitivity | 1.863 | 0.614 | 3.033 | 0.002 | −0.382 | 0.619 | −0.618 | 0.537 |
| Annoyance ← Living conditions | 3.861 | 1.743 | 2.215 | 0.027 | 0.063 | 0.279 | 0.225 | 0.822 |
| Parameter | 2019 Survey | 2020 Survey | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | SE | CR | p | Estimate | SE | CR | p | |
| Living conditions ← Lden | 0.010 | 0.004 | 2.568 | 0.010 | −0.005 | 0.004 | −1.267 | 0.205 |
| Sensitivity ← Living conditions | 0.579 | 0.150 | 3.823 | * | 0.092 | 0.042 | 2.174 | 0.030 |
| Health ← Lden | −0.009 | 0.005 | −1.674 | 0.094 | 0.011 | 0.006 | 1.775 | 0.076 |
| Length of time at home ← Lden | −0.009 | 0.005 | −1.663 | 0.096 | 0.018 | 0.004 | 4.725 | * |
| Health ← Living conditions | 0.246 | 0.143 | 1.722 | 0.085 | 0.003 | 0.053 | 0.050 | 0.960 |
| Health ← Sensitivity | 0.098 | 0.057 | 1.722 | 0.085 | −0.308 | 0.183 | −1.680 | 0.093 |
| Annoyance ← Length of time at home | 0.086 | 0.135 | 0.635 | 0.525 | 0.793 | 0.241 | 3.287 | 0.001 |
| Annoyance ← Health | −11.995 | 7.472 | −1.605 | 0.108 | −2.397 | 1.210 | −1.981 | 0.048 |
| Annoyance ← Sensitivity | 1.915 | 0.519 | 3.688 | * | −0.128 | 0.571 | −0.224 | 0.823 |
| Annoyance ← Living conditions | 2.719 | 1.136 | 2.393 | 0.017 | −0.068 | 0.271 | −0.250 | 0.803 |
| Parameter | 2019 Survey | 2020 Survey | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | SE | CR | p | Estimate | SE | CR | p | |
| Living conditions ← Lnight | 0.012 | 0.005 | 2.484 | 0.013 | −0.014 | 0.005 | 2.857 | 0.004 |
| Sensitivity ← Living conditions | 0.291 | 0.068 | 4.307 | * | 0.075 | 0.050 | 1.495 | 0.135 |
| Health ← Lnight | 0.000 | 0.001 | 0.404 | 0.686 | 0.007 | 0.003 | 2.307 | 0.021 |
| Open window ← Lnight | −0.014 | 0.007 | 1.872 | 0.061 | −0.029 | 0.006 | 5.231 | * |
| Health ← Living conditions | −0.007 | 0.018 | 0.405 | 0.686 | 0.059 | 0.032 | 1.812 | 0.070 |
| Health ← Sensitivity | −0.010 | 0.026 | 0.406 | 0.685 | −0.152 | 0.066 | 2.302 | 0.021 |
| Insomnia ← Open window | −0.043 | 0.019 | 2.236 | 0.025 | −0.006 | 0.029 | 0.222 | 0.825 |
| Insomnia ← Health | −13.148 | 32.090 | 0.410 | 0.682 | 0.286 | 0.101 | 2.844 | 0.004 |
| Insomnia ← Sensitivity | 0.052 | 0.053 | 0.977 | 0.328 | 1.347 | 0.647 | 2.082 | 0.037 |
| Insomnia ← Living conditions | 0.027 | 0.041 | 0.652 | 0.514 | −0.082 | 0.050 | 1.642 | 0.100 |
| Parameter | 2019 | 2020 | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | SE | CR | p | Estimate | SE | CR | p | |
| Living conditions ← Lnight | 0.012 | 0.005 | 2.487 | 0.013 | −0.014 | 0.005 | −2.857 | 0.004 |
| Sensitivity ← Living conditions | 0.291 | 0.067 | 4.307 | * | 0.075 | 0.050 | 1.494 | 0.135 |
| Health ← Lnight | 0.000 | 0.001 | 0.427 | 0.669 | 0.007 | 0.003 | 2.282 | 0.023 |
| Length of time at home ← Lnight | −0.013 | 0.006 | −2.234 | 0.025 | 0.017 | 0.004 | 4.839 | * |
| Health ← Living conditions | −0.008 | 0.018 | −0.429 | 0.668 | 0.058 | 0.032 | 1.799 | 0.072 |
| Health ← Sensitivity | −0.011 | 0.025 | −0.430 | 0.667 | −0.151 | 0.066 | −2.278 | 0.023 |
| Insomnia ← Length of time at home | 0.020 | 0.025 | 0.820 | 0.412 | 0.014 | 0.045 | 0.320 | 0.749 |
| Insomnia ← Health | −12.162 | 27.965 | −0.435 | 0.664 | 0.285 | 0.100 | 2.838 | 0.005 |
| Insomnia ← Sensitivity | 0.054 | 0.053 | 1.008 | 0.313 | 1.347 | 0.655 | 2.057 | 0.040 |
| Insomnia ← Living conditions | 0.047 | 0.041 | 1.136 | 0.256 | −0.083 | 0.050 | −1.661 | 0.097 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.T.H.N.; Trieu, B.L.; Nguyen, T.L.; Morinaga, M.; Hiraguri, Y.; Morihara, T.; Sasazawa, Y.; Nguyen, T.Q.H.; Yano, T. Models of Aviation Noise Impact in the Context of Operation Decrease at Tan Son Nhat Airport. Int. J. Environ. Res. Public Health 2023, 20, 5450. https://doi.org/10.3390/ijerph20085450
Nguyen TTHN, Trieu BL, Nguyen TL, Morinaga M, Hiraguri Y, Morihara T, Sasazawa Y, Nguyen TQH, Yano T. Models of Aviation Noise Impact in the Context of Operation Decrease at Tan Son Nhat Airport. International Journal of Environmental Research and Public Health. 2023; 20(8):5450. https://doi.org/10.3390/ijerph20085450
Chicago/Turabian StyleNguyen, Tran Thi Hong Nhung, Bach Lien Trieu, Thu Lan Nguyen, Makoto Morinaga, Yasuhiro Hiraguri, Takashi Morihara, Yosiaki Sasazawa, Tri Quang Hung Nguyen, and Takashi Yano. 2023. "Models of Aviation Noise Impact in the Context of Operation Decrease at Tan Son Nhat Airport" International Journal of Environmental Research and Public Health 20, no. 8: 5450. https://doi.org/10.3390/ijerph20085450
APA StyleNguyen, T. T. H. N., Trieu, B. L., Nguyen, T. L., Morinaga, M., Hiraguri, Y., Morihara, T., Sasazawa, Y., Nguyen, T. Q. H., & Yano, T. (2023). Models of Aviation Noise Impact in the Context of Operation Decrease at Tan Son Nhat Airport. International Journal of Environmental Research and Public Health, 20(8), 5450. https://doi.org/10.3390/ijerph20085450