

The Effectiveness of Mobility Restrictions on Controlling the Spread of COVID-19 in a Resistant Population


Abstract
1. Introduction
2. Datasets
2.1. COVID-19 Dataset
2.2. Google Mobility Dataset
2.3. COVID-19 Variants
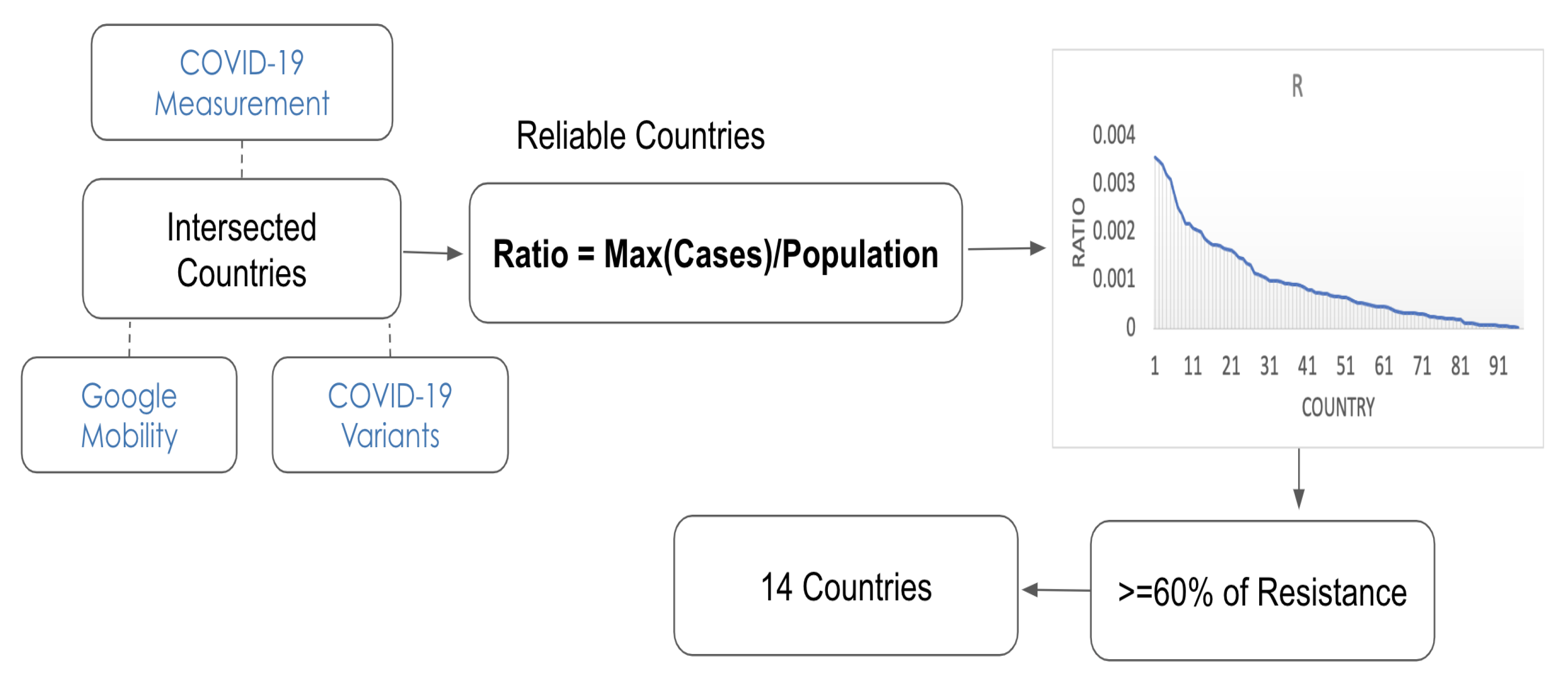
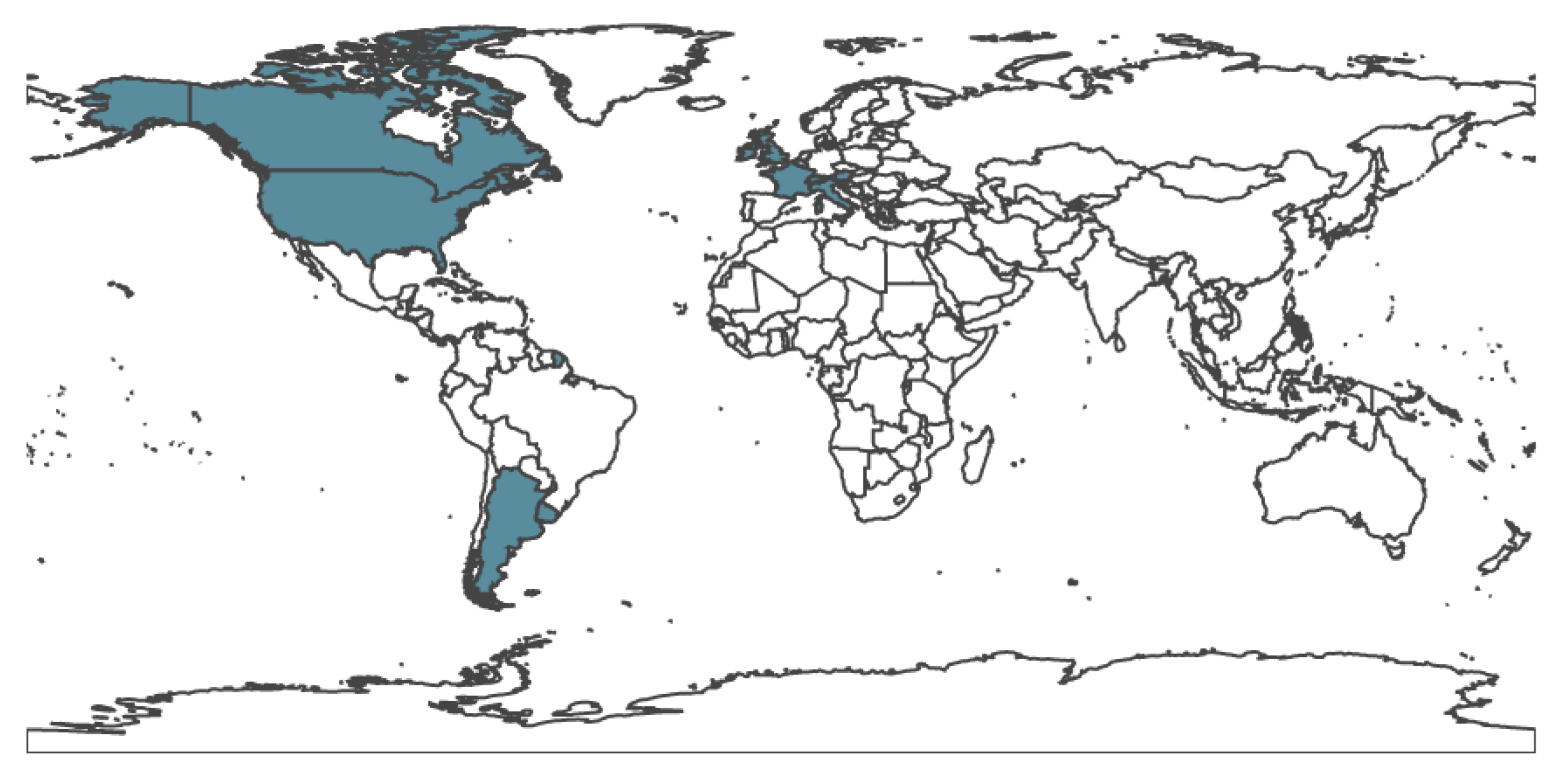
2.4. Country Selection
3. Methodology
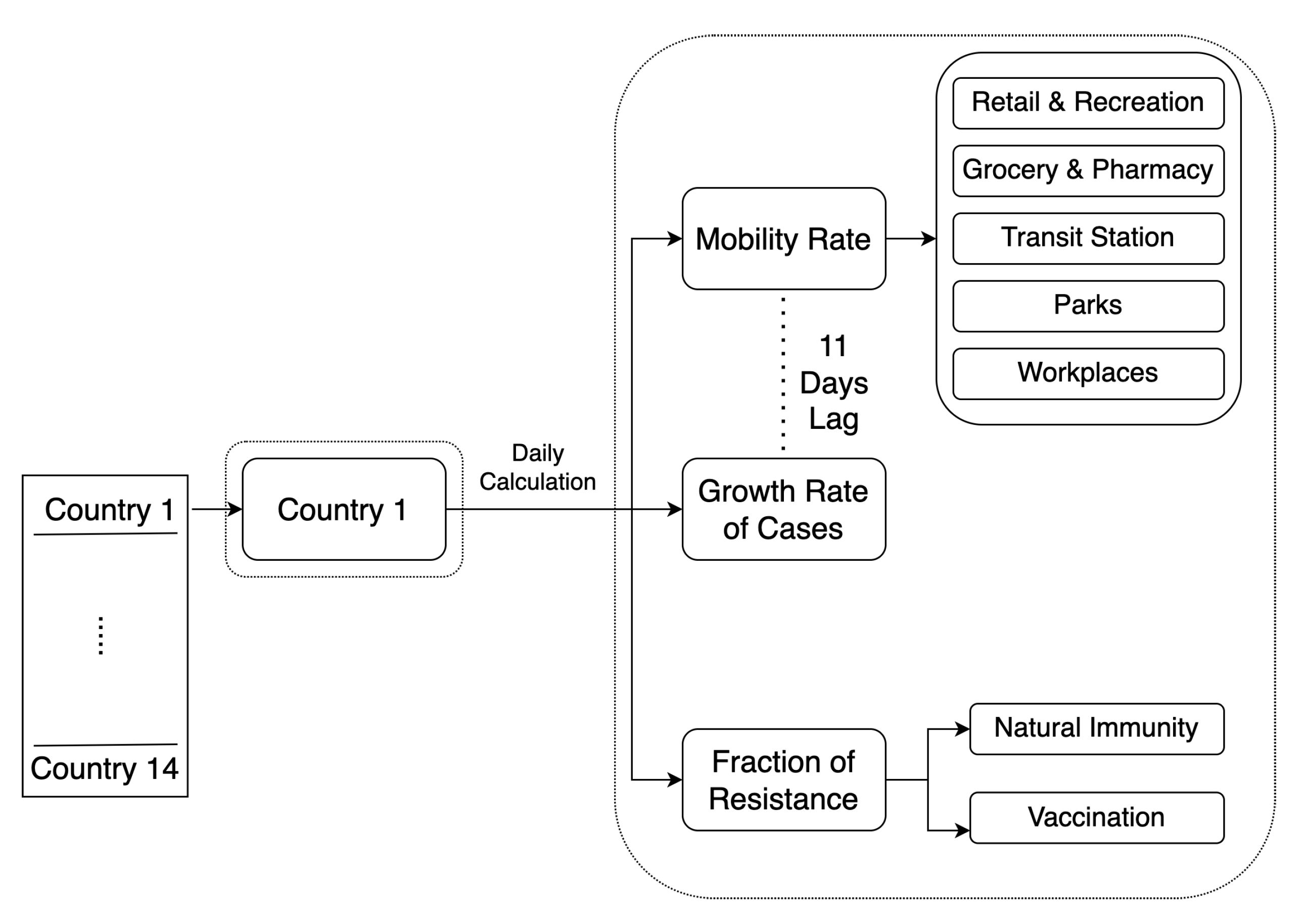
3.1. Daily Measurements
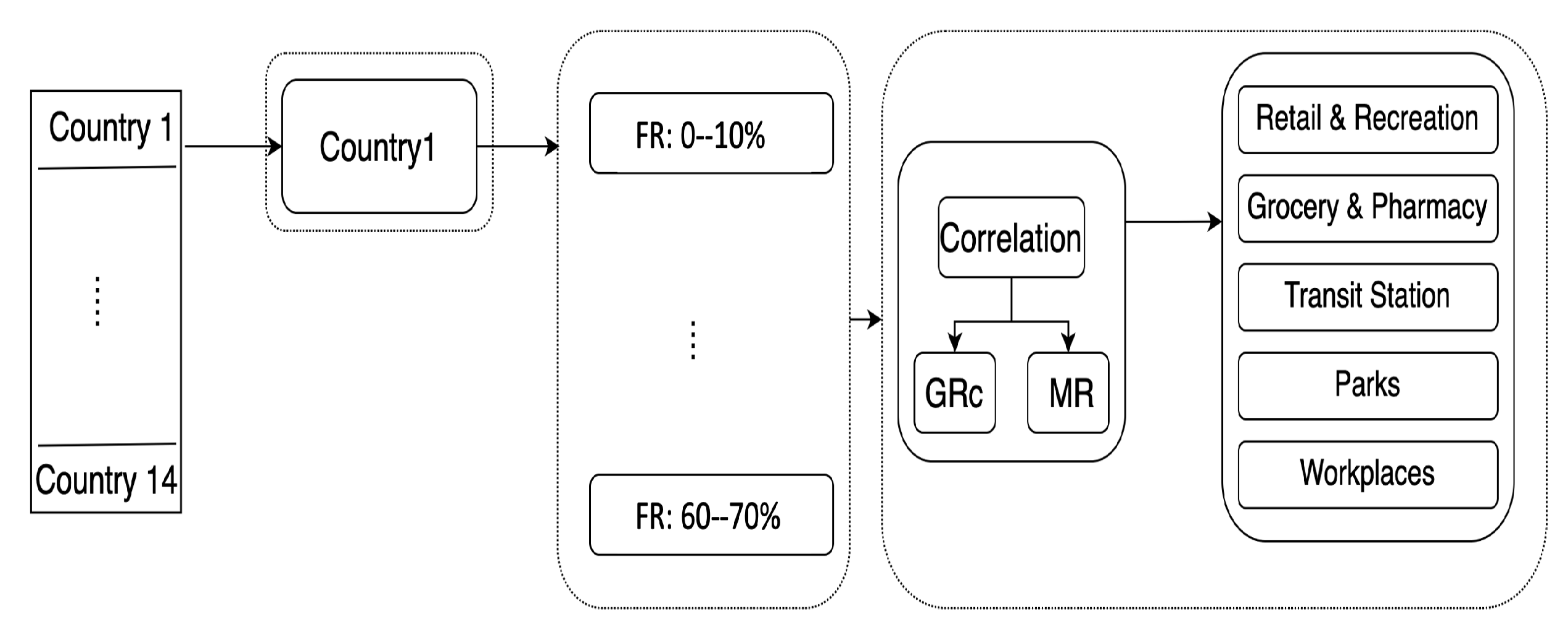
3.2. Correlations and Population Resistance Ranges
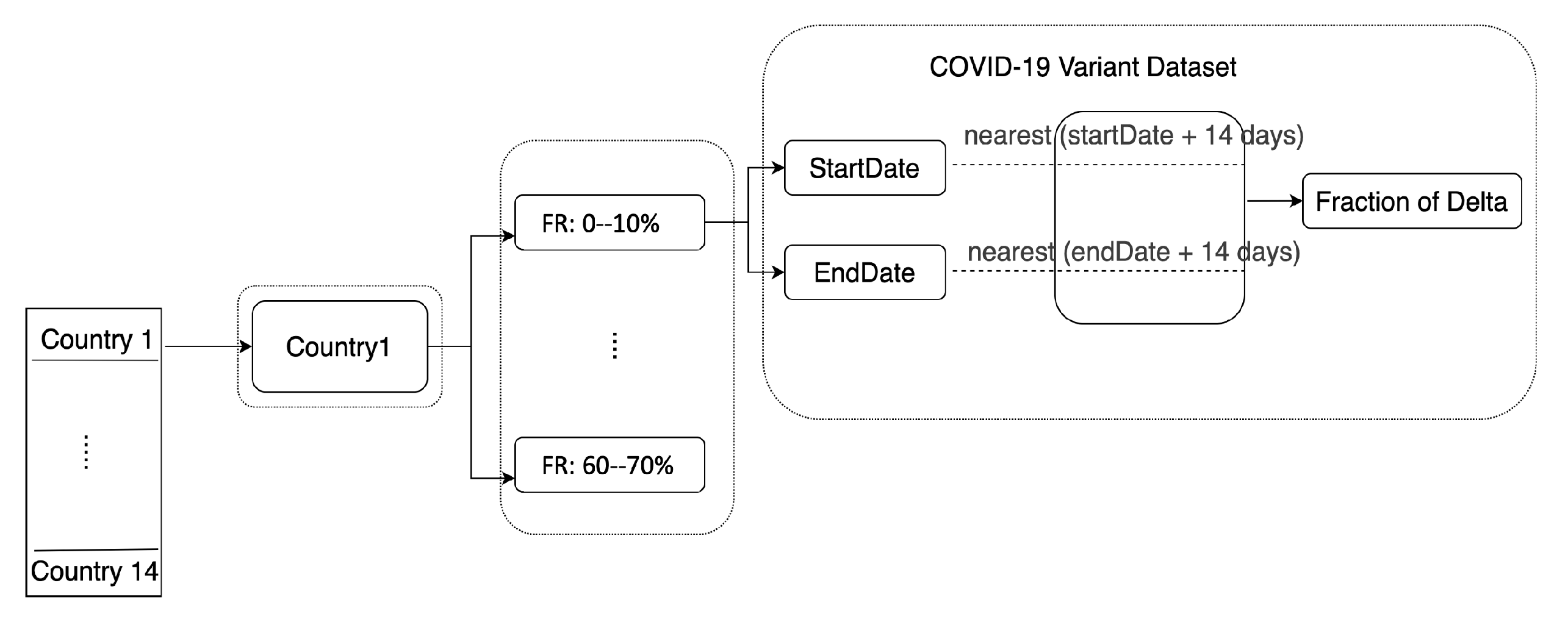
3.3. Delta Variant Estimates
4. Results
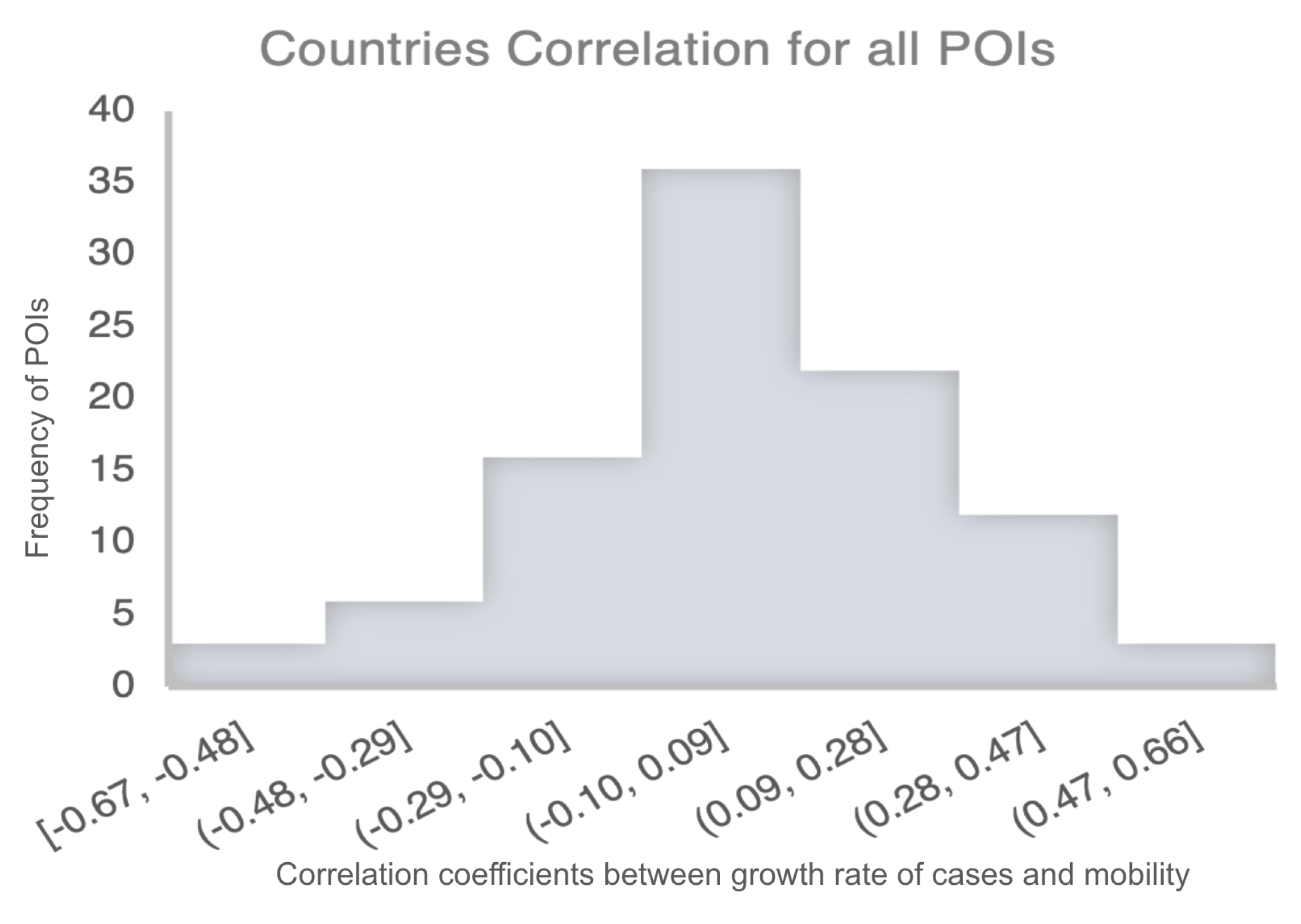
4.1. Correlation between Mobility and COVID-19 Cases
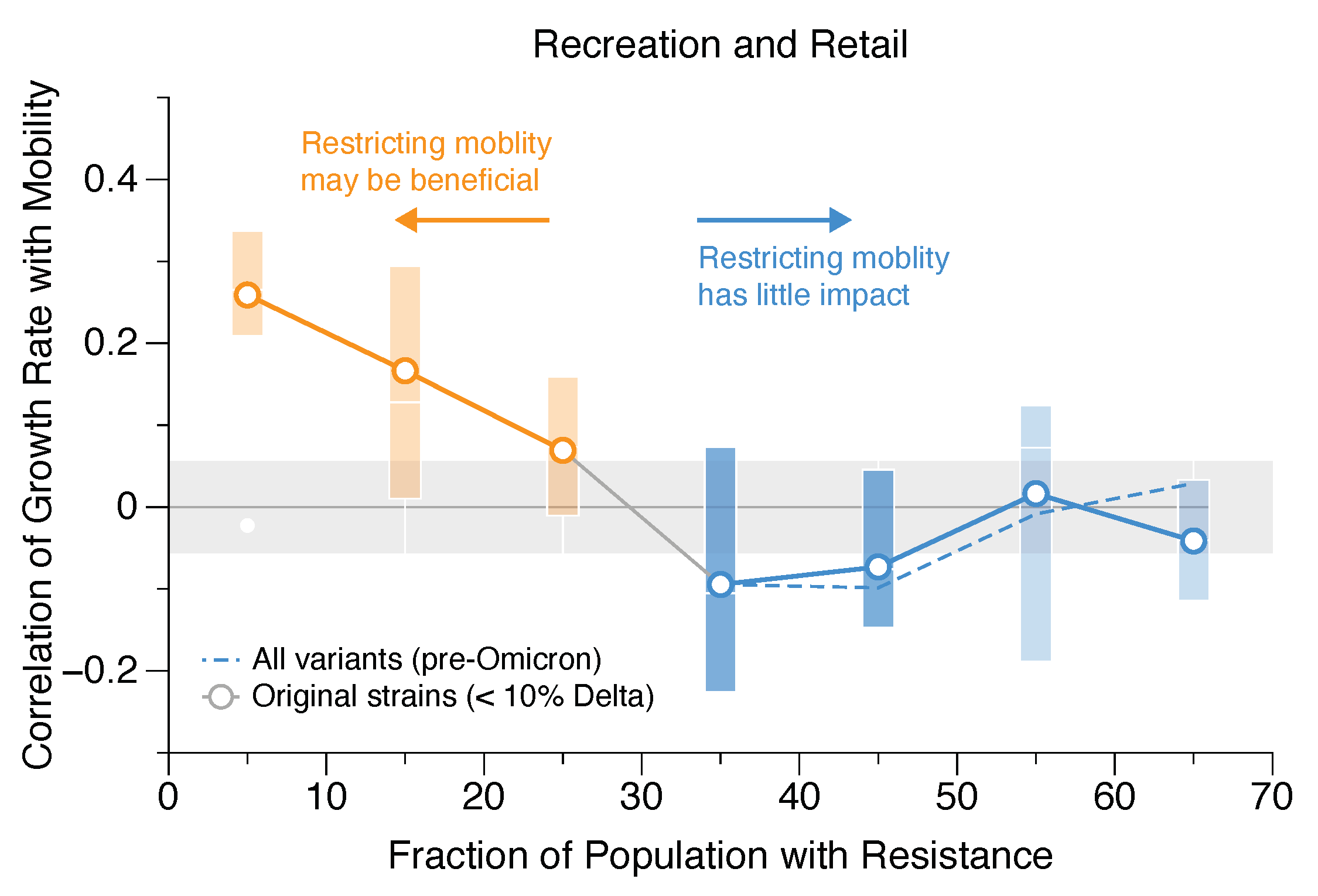
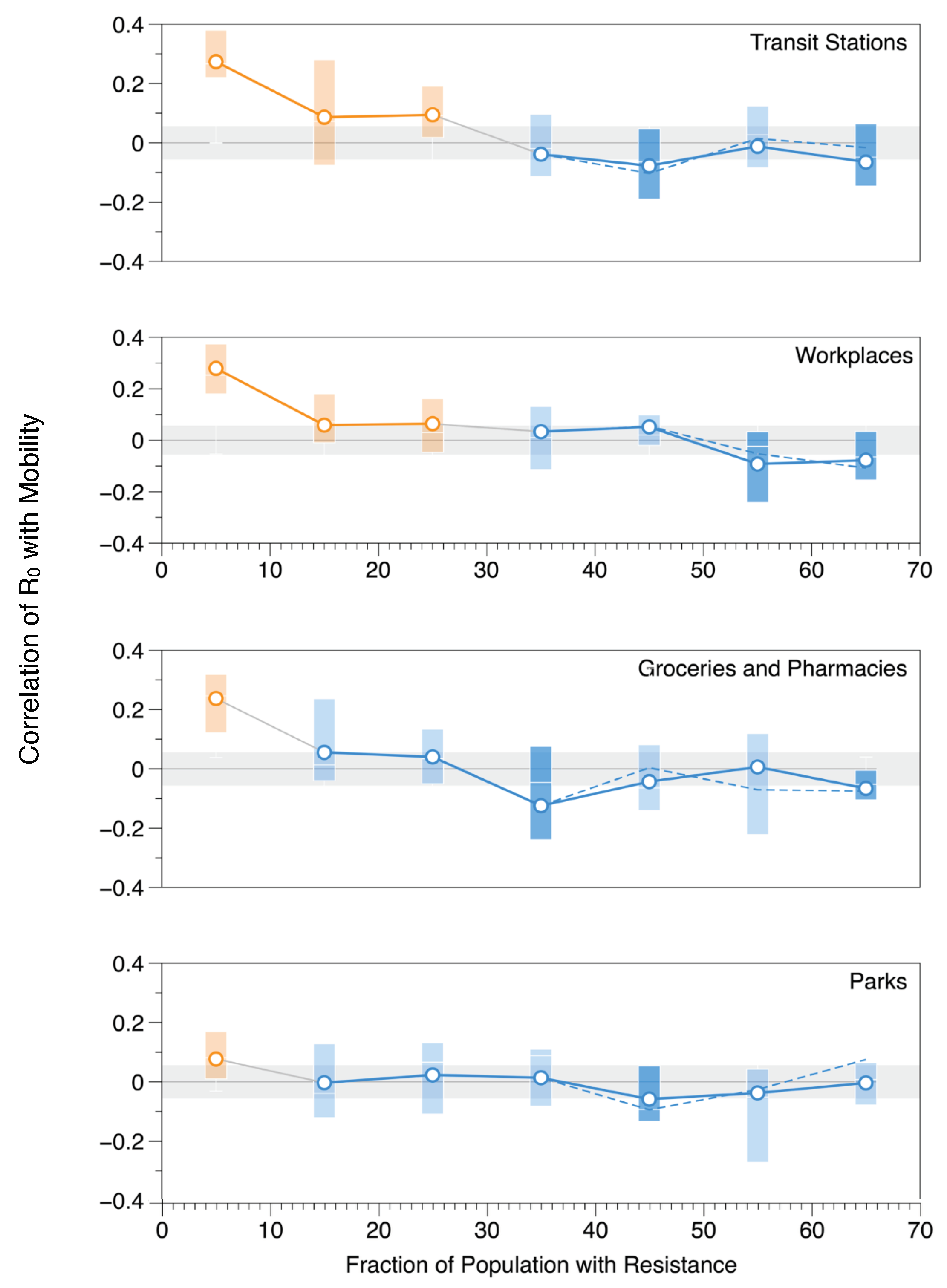
4.2. The Effect of Population Resistance on COVID-19 Transmission
5. Discussion
5.1. Implications for Mobility-Restricting Policies
5.2. The Effect of Delta Variant on COVID-19 Transmission
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan. N. Engl. J. Med. 2020, 382, 1199–1207. Available online: https://www.researchgate.net/publication/338904336_Early_Transmission_Dynamics_in_Wuhan_China_of_Novel_Coronavirus-Infected_Pneumonia (accessed on 15 August 2021).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Wesolowski, A.; Buckee, C.O.; Engø-Monsen, K.; Metcalf, C.J.E. Connecting mobility to infectious diseases: The promise and limits of mobile phone data. J. Infect. Dis. 2016, 214, S414–S420. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Sun, K.; Chinazzi, M.; Pastore y Piontti, A.; Dean, N.E.; Rojas, D.P.; Merler, S.; Mistry, D.; Poletti, P.; Rossi, L.; et al. Spread of Zika virus in the Americas. Proc. Natl. Acad. Sci. USA 2017, 114, E4334–E4343. [Google Scholar] [CrossRef]
- Davies, N.G.; Kucharski, A.J.; Eggo, R.M.; Gimma, A.; Edmunds, W.J.; Jombart, T.; O’Reilly, K.; Endo, A.; Hellewell, J.; Nightingale, E.S.; et al. Effects of non-pharmaceutical interventions on COVID-19 cases, deaths, and demand for hospital services in the UK: A modelling study. Lancet Public Health 2020, 5, e375–e385. [Google Scholar] [CrossRef]
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020, 585, 410–413. [Google Scholar] [CrossRef]
- Kwon, H.; Hom, K.; Rifkin, M.; Tian, B.; Koylu, C. Exploring the spatiotemporal heterogeneity in the relationship between human mobility and COVID-19 prevalence using dynamic time warping. arXiv 2021, arXiv:2109.13765. [Google Scholar]
- Xiong, C.; Hu, S.; Yang, M.; Luo, W.; Zhang, L. Mobile device data reveal the dynamics in a positive relationship between human mobility and COVID-19 infections. Proc. Natl. Acad. Sci. USA 2020, 117, 27087–27089. [Google Scholar] [CrossRef]
- Casa Nova, A.; Ferreira, P.; Almeida, D.; Dionísio, A.; Quintino, D. Are mobility and COVID-19 related? A dynamic analysis for Portuguese districts. Entropy 2021, 23, 786. [Google Scholar] [CrossRef]
- Steiger, E.; Mussgnug, T.; Kroll, L.E. Causal graph analysis of COVID-19 observational data in German districts reveals effects of determining factors on reported case numbers. PLoS ONE 2021, 16, e0237277. [Google Scholar] [CrossRef]
- Cartenì, A.; Di Francesco, L.; Martino, M. How mobility habits influenced the spread of the COVID-19 pandemic: Results from the Italian case study. Sci. Total Environ. 2020, 741, 140489. [Google Scholar] [CrossRef]
- Noland, R.B. Mobility and the effective reproduction rate of COVID-19. J. Transp. Health 2021, 20, 101016. [Google Scholar] [CrossRef] [PubMed]
- Wielechowski, M.; Czech, K.; Grzęda, Ł. Decline in Mobility: Public Transport in Poland in the time of the COVID-19 Pandemic. Economies 2020, 8, 78. [Google Scholar] [CrossRef]
- Oh, J.; Lee, H.Y.; Khuong, Q.L.; Markuns, J.F.; Bullen, C.; Barrios, O.E.A.; Hwang, S.S.; Suh, Y.S.; McCool, J.; Kachur, S.P.; et al. Mobility restrictions were associated with reductions in COVID-19 incidence early in the pandemic: Evidence from a real-time evaluation in 34 countries. Sci. Rep. 2021, 11, 13717. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Alomar, A.; Sarker, A.; Shah, D.; Shen, D.; Yang, C. Two Burning Questions on COVID-19: Did shutting down the economy help? Can we (partially) reopen the economy without risking the second wave? arXiv 2020, arXiv:2005.00072. [Google Scholar]
- Nouvellet, P.; Bhatia, S.; Cori, A.; Ainslie, K.E.; Baguelin, M.; Bhatt, S.; Boonyasiri, A.; Brazeau, N.F.; Cattarino, L.; Cooper, L.V.; et al. Reduction in mobility and COVID-19 transmission. Nat. Commun. 2021, 12, 1090. [Google Scholar] [CrossRef]
- Cabana, Á.; Etcheverry, L.; Fariello, M.I.; Bermolen, P.; Fiori, M. Assessing the impact of mobility reduction in the second wave of COVID-19. In Proceedings of the 2021 XLVII Latin American Computing Conference (CLEI), Vienna, Austria, 21–23 April 2021; pp. 1–10. [Google Scholar]
- da Silva, T.T.; Francisquini, R.; Nascimento, M.C. Meteorological and human mobility data on predicting COVID-19 cases by a novel hybrid decomposition method with anomaly detection analysis: A case study in the capitals of Brazil. Expert Syst. Appl. 2021, 182, 115190. [Google Scholar] [CrossRef]
- Bhowmik, T.; Tirtha, S.D.; Iraganaboina, N.C.; Eluru, N. A comprehensive analysis of COVID-19 transmission and mortality rates at the county level in the United States considering socio-demographics, health indicators, mobility trends and health care infrastructure attributes. PLoS ONE 2021, 16, e0249133. [Google Scholar] [CrossRef]
- Badr, H.S.; Du, H.; Marshall, M.; Dong, E.; Squire, M.M.; Gardner, L.M. Association between mobility patterns and COVID-19 transmission in the USA: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 1247–1254. [Google Scholar] [CrossRef]
- Chang, S.; Pierson, E.; Koh, P.W.; Gerardin, J.; Redbird, B.; Grusky, D.; Leskovec, J. Mobility network models of COVID-19 explain inequities and inform reopening. Nature 2021, 589, 82–87. [Google Scholar] [CrossRef]
- García-Cremades, S.; Morales-García, J.; Hernández-Sanjaime, R.; Martínez-España, R.; Bueno-Crespo, A.; Hernández-Orallo, E.; López-Espín, J.J.; Cecilia, J.M. Improving prediction of COVID-19 evolution by fusing epidemiological and mobility data. Sci. Rep. 2021, 11, 15173. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Wang, J.; Song, W.; Xiu, C.; Ma, L.; Pei, T. Spread of COVID-19 in China: Analysis from a city-based epidemic and mobility model. Cities 2021, 110, 103010. [Google Scholar] [CrossRef] [PubMed]
- Kuzdeuov, A.; Baimukashev, D.; Karabay, A.; Ibragimov, B.; Mirzakhmetov, A.; Nurpeiissov, M.; Lewis, M.; Varol, H.A. A network-based stochastic epidemic simulator: Controlling covid-19 with region-specific policies. IEEE J. Biomed. Health Inform. 2020, 24, 2743–2754. [Google Scholar] [CrossRef] [PubMed]
- Baniasad, M.; Mofrad, M.G.; Bahmanabadi, B.; Jamshidi, S. COVID-19 in Asia: Transmission factors, re-opening policies, and vaccination simulation. Environ. Res. 2021, 202, 111657. [Google Scholar] [CrossRef]
- Moghadas, S.M.; Vilches, T.N.; Zhang, K.; Wells, C.R.; Shoukat, A.; Singer, B.H.; Meyers, L.A.; Neuzil, K.M.; Langley, J.M.; Fitzpatrick, M.C.; et al. The impact of vaccination on coronavirus disease 2019 (COVID-19) outbreaks in the United States. Clin. Infect. Dis. 2021, 73, 2257–2264. [Google Scholar] [CrossRef]
- Alagoz, O.; Sethi, A.K.; Patterson, B.W.; Churpek, M.; Alhanaee, G.; Scaria, E.; Safdar, N. The impact of vaccination to control COVID-19 burden in the United States: A simulation modeling approach. PLoS ONE 2021, 16, e0254456. [Google Scholar] [CrossRef]
- Gupta, S.; Cantor, J.; Simon, K.I.; Bento, A.I.; Wing, C.; Whaley, C.M. Vaccinations Against COVID-19 May Have Averted Up to 140,000 Deaths in the United States: Study Examines Role of COVID-19 Vaccines and Deaths Averted in the United States. Health Aff. 2021, 40, 1465–1472. [Google Scholar] [CrossRef]
- Guo, J.; Deng, C.; Gu, F. Vaccinations, mobility and COVID-19 transmission. Int. J. Environ. Res. Public Health 2021, 19, 97. [Google Scholar] [CrossRef]
- Ritchie, H.; Spooner, F.; Roser, M.; Giattino, C.; Ritchie, H.; Rosado, P. Our World in Data. Available online: https://ourworldindata.org (accessed on 10 August 2021).
- COVID-19 Community Mobility Reports. Available online: https://www.google.com/covid19/mobility/ (accessed on 10 August 2021).
- Our World in Data. Available online: https://github.com/owid/covid-19-data/tree/master/public/data (accessed on 10 August 2021).
- Gisaid. Available online: https://www.gisaid.org./ (accessed on 10 August 2021).
- Xi, W.; Pei, T.; Liu, Q.; Song, C.; Liu, Y.; Chen, X.; Ma, J.; Zhang, Z. Quantifying the time-lag effects of human mobility on the COVID-19 transmission: A multi-city study in China. IEEE Access 2020, 8, 216752–216761. [Google Scholar] [CrossRef]
- Estimated COVID-19 Burden. Available online: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/burden.html (accessed on 10 August 2021).
- Undetected COVID Infections. Available online: https://www.timesofisrael.com/undetected-covid-infections-are-rare-tel-aviv-hospital-finds-in-staff-survey/ (accessed on 10 August 2021).
- Rocchetti, I.; Böhning, D.; Holling, H.; Maruotti, A. Estimating the size of undetected cases of the COVID-19 outbreak in Europe: An upper bound estimator. Epidemiol. Methods 2020, 9, 20200024. [Google Scholar] [CrossRef]
- Pullano, G.; Di Domenico, L.; Sabbatini, C.E.; Valdano, E.; Turbelin, C.; Debin, M.; Guerrisi, C.; Kengne-Kuetche, C.; Souty, C.; Hanslik, T.; et al. Underdetection of cases of COVID-19 in France threatens epidemic control. Nature 2021, 590, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Etchenique, R.; Quiroga, R. Estimate of the actual number of COVID-19 cases from the analysis of deaths. medRxiv 2020. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Measurement Rate | Countries Coverage | Temporal Coverage |
|---|---|---|---|
| COVID-19 Measurements | Daily | 231 | Jan 2020—present |
| Google Mobility | Daily | 123 | Feb 2020—present |
| COVID-19 Variants | Two Weeks | 110 | May 2020—present |
| Country | Multiplier | Source |
|---|---|---|
| US & Canada | 4 | [36] |
| Israel | 1.5 | [37] |
| France | 7.94 | [38,39] |
| Argentina | 8.1 | [40] |
| Uruguay | 4 | No Reference (used the US multiplier) |
| European countries | 4 | [38] |
| Mean | Color | Restriction Recommendation |
|---|---|---|
| >0.056 = standard error in the mean | Orange | Mobility and growth rate are positively correlated; may be helpful to restrict mobility |
| −0.056 and 0.056 | Light blue | No correlation between mobility and growth rate; restricting mobility has little impact |
| <−0.056 | Darker blue | Negative correlation between mobility and growth rate; restricting mobility potentially has an adverse effect. |
| POI | FR Need | Specification |
|---|---|---|
| Retail and Recreation | 25–30% | Closed, crowded, stay a long time |
| Transit Station | 25–30% | Closed, crowded |
| Workplaces | 25–30% | Closed, crowded, stay a long time |
| Grocery and Pharmacy | 10% | Closed but people just pick and go—might vary based on size |
| Parks | 5–10% | Open and more social distancing |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albassam, D.; Nouh, M.; Hosoi, A. The Effectiveness of Mobility Restrictions on Controlling the Spread of COVID-19 in a Resistant Population. Int. J. Environ. Res. Public Health 2023, 20, 5343. https://doi.org/10.3390/ijerph20075343
Albassam D, Nouh M, Hosoi A. The Effectiveness of Mobility Restrictions on Controlling the Spread of COVID-19 in a Resistant Population. International Journal of Environmental Research and Public Health. 2023; 20(7):5343. https://doi.org/10.3390/ijerph20075343
Chicago/Turabian StyleAlbassam, Dina, Mariam Nouh, and Anette Hosoi. 2023. "The Effectiveness of Mobility Restrictions on Controlling the Spread of COVID-19 in a Resistant Population" International Journal of Environmental Research and Public Health 20, no. 7: 5343. https://doi.org/10.3390/ijerph20075343
APA StyleAlbassam, D., Nouh, M., & Hosoi, A. (2023). The Effectiveness of Mobility Restrictions on Controlling the Spread of COVID-19 in a Resistant Population. International Journal of Environmental Research and Public Health, 20(7), 5343. https://doi.org/10.3390/ijerph20075343