
Evolutions of Self-Rated Health and Social Interactions during the COVID-19 Pandemic Affected by Pre-Pandemic Conditions: Evidence from a Four-Wave Survey


Abstract
1. Introduction
1.1. Research Purpose
1.2. Literature Review
1.3. Hypotheses
2. Materials and Methods
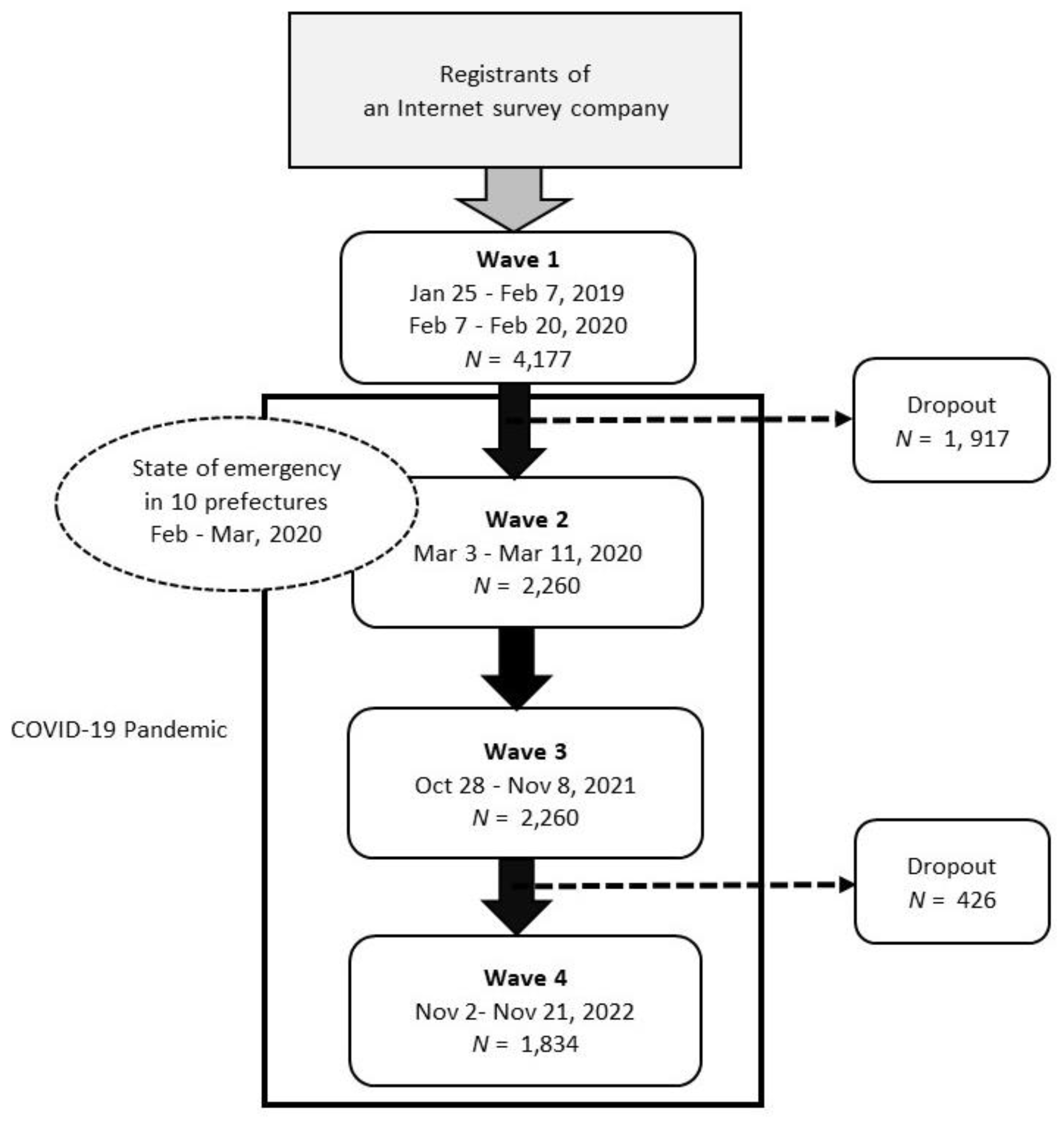
2.1. Study Samples
2.2. Self-Rated Health
2.3. Social Interactions
2.4. Individual-Level Covariates
2.5. Analytic Strategy
3. Results
3.1. Descriptive Analysis
3.2. Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Breslau, J.; Finucane, M.L.; Locker, A.R.; Baird, M.D.; Roth, E.A.; Collins, R.L. A longitudinal study of psychological distress in the United States before and during the COVID-19 pandemic. Prev. Med. 2021, 143, 106362. [Google Scholar] [CrossRef] [PubMed]
- Niedzwiedz, C.L.; Green, M.J.; Benzeval, M.; Campbell, D.; Craig, P.; Demou, E.; Leyland, A.; Pearce, A.; Thomson, R.; Whitley, E.; et al. Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: Longitudinal analyses of the UK Household Longitudinal Study. J. Epidemiol. Community Health 2021, 75, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Peters, A.; Rospleszcz, S.; Greiser, K.H.; Dallavalle, M.; Berger, K. Complete list of authors available under: Collaborators. The impact of the COVID-19 pandemic on self-reported health. Dtsch. Arztebl. Int. 2020, 117, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Tušl, M.; Brauchli, R.; Kerksieck, P.; Bauer, G.F. Impact of the COVID-19 crisis on work and private life, mental well-being and self-rated health in German and Swiss employees: A cross-sectional online survey. BMC Public Health 2021, 21, 741. [Google Scholar] [CrossRef]
- Yarrington, J.S.; Lasser, J.; Garcia, D.; Vargas, J.H.; Couto, D.D.; Marafon, T.; Craske, M.G.; Niles, A.N. Impact of the COVID-19 pandemic on mental health among 157,213 Americans. J. Affect Disord. 2021, 286, 64–70. [Google Scholar] [CrossRef]
- Yamamoto, T.; Uchiumi, C.; Suzuki, N.; Yoshimoto, J.; Murillo-Rodriguez, E. The psychological impact of “mild lockdown” in Japan during the COVID-19 pandemic: A nationwide survey under a declared state of emergency. Int. J. Environ. Res. Public Health 2020, 17, 9382. [Google Scholar] [CrossRef]
- Kim, H.H.; Jung, J.H. Social isolation and psychological distress during the COVID-19 pandemic: A cross-national analysis. Gerontologist 2021, 61, 103–113. [Google Scholar] [CrossRef]
- Kotwal, A.A.; Holt-Lunstad, J.; Newmark, R.L.; Cenzer, I.; Smith, A.K.; Covinsky, K.E.; Escueta, D.P.; Lee, J.M.; Perissinotto, C.M. Social isolation and loneliness among San Francisco Bay area older adults during the COVID-19 shelter-in-place orders. J. Am. Geriatr. Soc. 2021, 69, 20–29. [Google Scholar] [CrossRef]
- Macdonald, B.; Hülür, G. Well-being and loneliness in Swiss older adults during the COVID-19 pandemic: The role of social relationships. Gerontologist 2021, 61, 240–250. [Google Scholar] [CrossRef]
- Müller, F.; Röhr, S.; Reininghaus, U.; Riedel-Heller, S.G. Social isolation and loneliness during COVID-19 lockdown: Associations with depressive symptoms in the German old-age population. Int. J. Environ. Res. Public Health 2021, 18, 3615. [Google Scholar] [CrossRef] [PubMed]
- Murayama, H.; Okubo, R.; Tabuchi, T. Increase in social isolation during the COVID-19 pandemic and its association with mental health: Findings from the JACSIS 2020 Study. Int. J. Environ. Res. Public Health 2021, 18, 8238. [Google Scholar] [CrossRef]
- Yamada, K.; Wakaizumi, K.; Kubota, Y.; Murayama, H.; Tabuchi, T. Loneliness, social isolation, and pain following the COVID-19 outbreak: Data from a nationwide internet survey in Japan. Sci. Rep. 2021, 11, 18643. [Google Scholar] [CrossRef] [PubMed]
- Erzen, E.; Çikrikci, Ö. The effect of loneliness on depression: A meta-analysis. Int. J. Soc. Psychiatry 2018, 64, 427–435. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef]
- van Tilburg, T.G.; Steinmetz, S.; Stolte, E.; van der Roest, H.; de Vries, D.H. Loneliness and mental health during the COVID-19 pandemic: A study among Dutch older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e249–e255. [Google Scholar] [CrossRef]
- Stolz, E.; Mayerl, H.; Freidl, W. The impact of COVID-19 restriction measures on loneliness among older adults in Austria. Eur. J. Public Health 2021, 31, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Mayerl, H.; Stolz, E.; Freidl, W. Trajectories of loneliness, depressive symptoms, and anxiety symptoms during the COVID-19 pandemic in Austria. Public Health 2022, 212, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Oshio, T.; Kimura, H.; Nishizaki, T.; Kuwahara, S. Pre-pandemic social isolation as a predictor of the adverse impact of the pandemic on self-rated health: A longitudinal COVID-19 study in Japan. Prev. Med. 2022, 164, 107329. [Google Scholar] [CrossRef]
- Sato, K.; Kondo, N.; Kondo, K. Pre-pandemic individual- and community-level social capital and depressive symptoms during COVID-19: A longitudinal study of Japanese older adults in 2019–21. Health Place 2022, 74, 102772. [Google Scholar] [CrossRef]
- Li, L.W.; Hu, R.X.; Luo, M.S.; McLaughlin, S. Pre-pandemic social integration: Protection or risk for older adults in the time of COVID-19? J. Gerontol. B Psychol. Sci. Soc. Sci. 2022, 78, gbac177. [Google Scholar] [CrossRef]
- Oshio, T.; Kan, M. Does social participation accelerate psychological adaptation to health shocks? Evidence from a national longitudinal survey in Japan. Qual. Life Res. 2019, 28, 2125–2133. [Google Scholar] [CrossRef]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef]
- Jylhä, M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef]
- Battey, H.S.; Cox, D.R.; Jackson, M.V. On the linear in probability model for binary data. R. Soc. Open Sci. 2019, 6, 190067. [Google Scholar] [CrossRef]
- Guimarães, P.; Portugal, P. A simple feasible procedure to fit models with high-dimensional fixed effects. Stata J. 2010, 10, 628–649. [Google Scholar] [CrossRef]
- Wooldridge, J.M. Econometric Analysis of Cross Section and Panel Data; MIT Press: Boston, MA, USA, 2010. [Google Scholar]
- Kahneman, D.; Tversky, A. Prospect theory: An analysis of decision under risk. Econometrica 1979, 47, 263–292. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Oshio, T.; Kimura, H.; Nishizaki, T.; Kuwahara, S. At Which area level does COVID-19 infection matter most for an individual’s self-rated health? A Multilevel fixed-effects model analysis in Japan. Int. J. Environ. Res. Public Health 2022, 19, 8918. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Interaction with Others | Interaction | No Interaction | All | |
|---|---|---|---|---|
| Proportion (%) | ||||
| Sex | ||||
| Men | 46.9 | 63.3 | 49.2 | |
| Women | 53.1 | 36.7 | 50.8 | |
| Occupational status | ||||
| Regularly employed | 41.6 | 34.9 | 40.7 | |
| Non-regularly employed | 22.7 | 27.7 | 23.4 | |
| Self-employed | 7.5 | 7.8 | 7.6 | |
| Unemployed | 2.9 | 7.0 | 3.5 | |
| Not working | 20.9 | 21.1 | 20.9 | |
| Student | 4.4 | 1.5 | 4.0 | |
| Educational attainment | ||||
| Junior high school | 1.8 | 6.0 | 2.4 | |
| High school | 40.9 | 52.4 | 42.5 | |
| Junior college | 13.1 | 8.3 | 12.4 | |
| College or above | 44.2 | 33.3 | 42.6 | |
| Married | 59.8 | 42.9 | 57.5 | |
| Lived in emergency-state areas | 23.1 | 21.6 | 22.9 | |
| Age (years) | ||||
| M | 48.5 | 48.5 | 48.4 | |
| SD | (15.6) | (15.2) | (15.4) | |
| Household income (annual, million JPY) | ||||
| M | 6.21 | 4.92 | 6.03 | |
| SD | (6.64) | (7.73) | (6.82) | |
| N | 3589 (85.9%) | 588 (14.1%) | 4177 (100%) | |
| Prevalence (%) | Pairwise Correlation Coefficient | |||
|---|---|---|---|---|
| Poor self-Rated Health | Interaction with Others | Receiving Social Support | ||
| Poor self-rated health | 20.4 | |||
| Interaction with others | 79.2 | –0.094 *** | ||
| Receiving social support | 88.0 | –0.120 *** | 0.306 *** | |
| SNS use | 66.5 | –0.026 ** | 0.163 *** | 0.107 *** |
| Probability (%) | Change from Wave 1 (Percentage Points) | |||||||
|---|---|---|---|---|---|---|---|---|
| Interaction with others in Wave 1 | No | Yes | No | Yes | ||||
| State of emergency in Wave 2 | Yes | No | Yes | No | Yes | No | Yes | No |
| Poor self-rated health | ||||||||
| Wave 1 | 18.9 | 20.9 | 37.0 | 34.9 | ||||
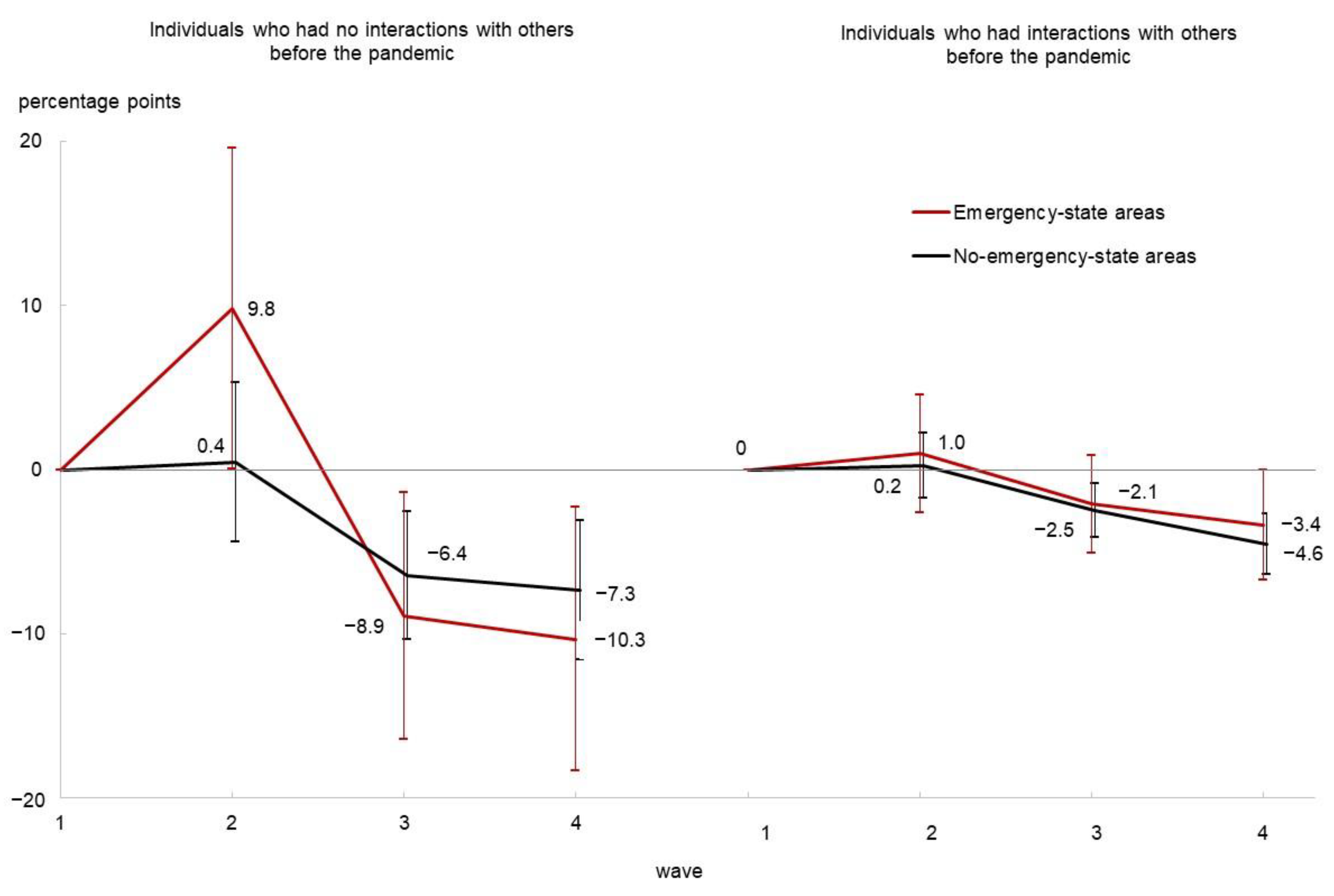
| Wave 2 | 19.7 | 20.1 | 46.7 | 32.9 | 0.8 | −0.8 | 9.7 | −2.0 |
| Wave 3 | 17.5 | 18.4 | 29.1 | 28.4 | −1.4 | −2.5 | −7.9 | −6.5 |
| Wave 4 | 16.1 | 15.9 | 27.8 | 27.5 | −2.8 | −5.1 | −9.2 | −7.5 |
| Interaction with others | ||||||||
| Wave 1 | 100.0 | 100.0 | 0.0 | 0.0 | ||||
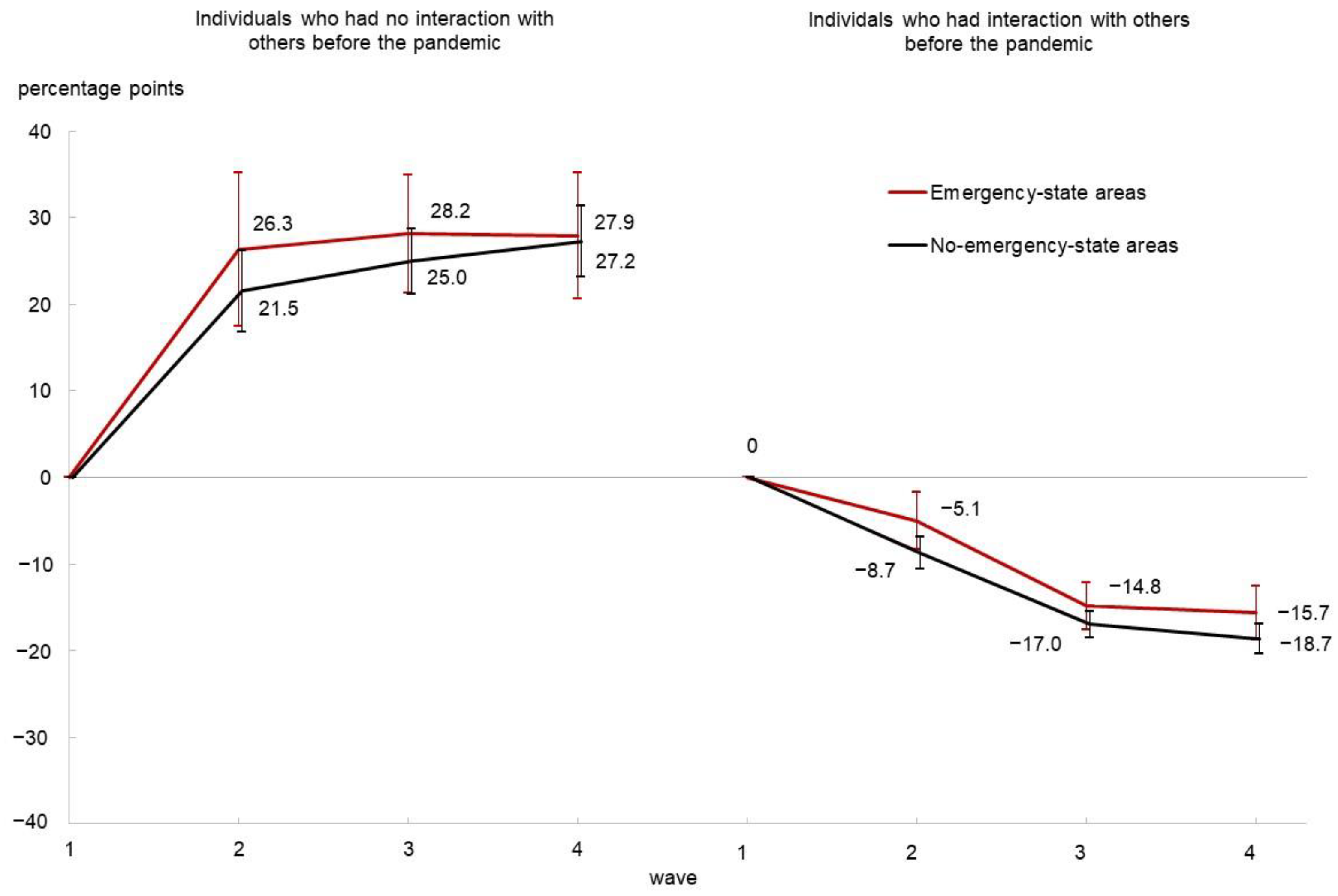
| Wave 2 | 94.3 | 90.9 | 23.3 | 20.9 | −5.7 | −9.1 | 23.3 | 20.9 |
| Wave 3 | 84.5 | 83.0 | 26.8 | 24.9 | −15.5 | −17.0 | 26.8 | 24.9 |
| Wave 4 | 84.0 | 81.0 | 26.9 | 27.2 | −16.0 | −19.0 | 26.9 | 27.2 |
| Receiving social support | ||||||||
| Wave 1 | 95.1 | 93.1 | 59.8 | 61.8 | ||||
| Wave 2 | 93.4 | 92.1 | 66.7 | 69.9 | −1.7 | −0.9 | 6.8 | 8.1 |
| Wave 3 | 91.2 | 90.9 | 68.5 | 63.8 | −3.9 | −2.1 | 8.7 | 2.0 |
| Wave 4 | 91.7 | 90.1 | 63.0 | 66.4 | −3.4 | −3.0 | 3.1 | 4.6 |
| SNS use | ||||||||
| Wave 1 | 69.8 | 67.6 | 44.1 | 47.3 | ||||
| Wave 2 | 74.4 | 72.3 | 70.0 | 49.8 | 4.6 | 4.7 | 25.9 | 2.5 |
| Wave 3 | 69.4 | 70.8 | 49.6 | 49.2 | −0.4 | 3.1 | 5.5 | 2.0 |
| Wave 4 | 68.4 | 67.3 | 51.9 | 46.7 | −1.4 | −0.3 | 7.8 | −0.6 |
| Poor Self-Rated Health | Interaction with Others | Receiving Social Support | SNS Use | |||||
|---|---|---|---|---|---|---|---|---|
| Coef. × 100 | 95% CI 1 | Coef. × 100 | 95% CI | Coef. × 100 | 95% CI | Coef. × 100 | 95% CI | |
| Emergency-state areas (N = 3146) | ||||||||
| β2 | 1.0 | (−2.6, 4.5) | −5.1 | (−8.3, −1.8) | −1.3 | (−4.2, 1.6) | 1.4 | (−2.5, 5.2) |
| β3 | −2.1 | (−5.1, 0.9) | −14.8 | (−17.6, −12.1) | −4.1 | (−6.5, −1.7) | −0.2 | (−3.4, 3.0) |
| β4 | −3.4 | (−6.7, 0.0) | −15.7 | (−18.7, −12.6) | −4.1 | (−6.8, −1.4) | −0.3 | (−3.9, 3.3) |
| β2 + γ2 | 9.8 | (0.1, 19.5) | 26.3 | (17.4, 35.2) | 8.0 | (0.1, 16.0) | 19.4 | (8.9, 29.9) |
| β3 + γ3 | −8.9 | (−16.4, −1.4) | 28.2 | (21.3, 35.0) | 8.6 | (2.5, 14.6) | 5.1 | (−3.0, 13.1) |
| β4 + γ4 | −10.3 | (−18.3, −2.3) | 27.9 | (20.6, 35.3) | 2.0 | (−4.5, 8.5) | 9.8 | (1.1, 18.4) |
| No-emergency-state areas (N = 10,727) | ||||||||
| β2 | 0.2 | (−1.7, 2.2) | −8.7 | (−10.6, −6.8) | −0.1 | (−1.7, 1.5) | 2.5 | (0.4, 4.6) |
| β3 | −2.5 | (−4.1, −0.9) | −17.0 | (−18.6, −15.4) | −2.1 | (−3.4, −0.8) | 3.3 | (1.6, 5.0) |
| β4 | −4.6 | (−6.4, −2.7) | −18.7 | (−20.4, −16.9) | −2.5 | (−4.0, −1.0) | 1.8 | (−0.1, 3.8) |
| β2 + γ2 | 0.4 | (−4.4, 5.3) | 21.5 | (16.9, 26.2) | 7.2 | (3.2, 11.2) | −1.4 | (−6.5, 3.8) |
| β3 + γ3 | −6.4 | (−10.3, −2.5) | 25.0 | (21.2, 28.7) | 1.9 | (−1.3, 5.1) | 1.9 | (−2.2, 6.1) |
| β4 + γ4 | −7.3 | (−11.5, −3.1) | 27.2 | (23.2, 31.3) | 3.7 | (0.2, 7.1) | 0.8 | (−3.7, 5.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oshio, T.; Kimura, H.; Nakazawa, S.; Kuwahara, S. Evolutions of Self-Rated Health and Social Interactions during the COVID-19 Pandemic Affected by Pre-Pandemic Conditions: Evidence from a Four-Wave Survey. Int. J. Environ. Res. Public Health 2023, 20, 4594. https://doi.org/10.3390/ijerph20054594
Oshio T, Kimura H, Nakazawa S, Kuwahara S. Evolutions of Self-Rated Health and Social Interactions during the COVID-19 Pandemic Affected by Pre-Pandemic Conditions: Evidence from a Four-Wave Survey. International Journal of Environmental Research and Public Health. 2023; 20(5):4594. https://doi.org/10.3390/ijerph20054594
Chicago/Turabian StyleOshio, Takashi, Hiromi Kimura, Shingo Nakazawa, and Susumu Kuwahara. 2023. "Evolutions of Self-Rated Health and Social Interactions during the COVID-19 Pandemic Affected by Pre-Pandemic Conditions: Evidence from a Four-Wave Survey" International Journal of Environmental Research and Public Health 20, no. 5: 4594. https://doi.org/10.3390/ijerph20054594
APA StyleOshio, T., Kimura, H., Nakazawa, S., & Kuwahara, S. (2023). Evolutions of Self-Rated Health and Social Interactions during the COVID-19 Pandemic Affected by Pre-Pandemic Conditions: Evidence from a Four-Wave Survey. International Journal of Environmental Research and Public Health, 20(5), 4594. https://doi.org/10.3390/ijerph20054594