
Lessons Learned from Natural Disasters around Digital Health Technologies and Delivering Quality Healthcare

 , , , and
, , , and
Abstract
1. Introduction
2. Digital Health
2.1. Telehealth and Telemedicine
2.2. Electronic Health Records
2.3. Electronic Prescribing
2.4. Electronic Referrals
2.5. mHealth
2.6. Artificial (Augmented) Intelligence and Machine Learning

{kind=link}
| Type of Robotics | Definition | Examples of Applications in Healthcare Industry |
|---|---|---|
| Telerobots | Semi-autonomous robots that can be controlled from a distance by human operators using a wireless network, televisions, or tethered connections. | A popular telerobot platform (da Vinci system) has been in use for urological and cardiac surgery since the beginning of the 21st century [35]. Telerobots have great potential for use in locating survivors and human rescue in the aftermath of disasters, as well as delivering short-distance medical services to disaster victims [36]. |
| Collaborative robots | Service robots that can co-exist in close proximity with humans, maintaining/ensuring a high level of human safety during operation. | Collaborative robots are in wide use in healthcare settings for laboratory testing of biological samples [37]. Collaborative multi-robot systems have potential for use in search and rescue operations during disasters [38]. |
| Autonomous robots | Robotic systems capable of independent actions with minimal or no interaction from human operators. | Autonomous robots have been used for various surgical procedures since the mid-1980s [39]. Autonomous robots like flying drones can be used in disaster settings for search or rescue operations, and for delivery of essential medical supplies (e.g., medicines or sterile equipment). |
| Social robots | Artificial intelligence systems that are capable of interaction and communication with humans and their surrounding environment. | Social robots (e.g., PETRA [40]), capable of detecting signs of diabetes and hypothyroidism, have been developed by pharmaceutical companies to support pre-screening for these diseases. In disaster settings, social robots can be used to provide mental health support to victims undergoing rehabilitation [41]. |
| Wearable robots | Human-worn smart electronic devices that provide information about body signals, such as vital signs or physical activity, to support or reinforce capabilities of the users. | Surface electromyography is in use for limb assessments, rehabilitation, and assistance [42]. Wearable robots can be used for triaging disaster causalities in low-resource settings [43]. |
2.7. Internet of Things
2.8. Robotics
2.9. Wearables (Trackers and Monitors)
2.10. Digital Markers and Sensors
2.11. Cloud Computing
2.12. Social Media and Internet
| Technology | Uptake | Advantages | Vulnerabilities | References |
|---|---|---|---|---|
| Mobile phones and devices | Widespread use | Rapid, wide-area communications; efficient individual tracking and identification. | Expensive equipment required. Battery storage limits may impair use over time. Partially dependent on access to electricity. Vulnerable to scams/privacy invasion. | [74] [75] [76] |
| Electronic health records | Increasing | Highly portable. Provides critical clinical history for displaced/non-communicative patients. | Privacy concerns. Dependent on network availability and electrical power. Identification/documentation information may be unavailable to displaced persons. Requires advance implementation for utility in disaster situations. | [77] [78] |
| Telehealth; Electronic prescribing; Electronic consultation | Widespread use | Proven effectiveness in COVID-19 pandemic. Usable across multiple platforms (mobile devices, landlines, teleconferencing, internet). Greatly expands healthcare workforce effectiveness, especially in understaffed situations. Highly flexible. Demonstrated clinical utility and good evidence base. Use of radio frequency identification (RFID), barcodes, quick response (QR) codes. Limits errors and improves security and traceability. | Dependent on intact communications infrastructure. Privacy concerns. Subtle clinical details may be obscured. Patient unfamiliarity/digital literacy may compromise effectiveness. | [79] [80] [81] |
| Artificial Intelligence | Limited at present | Facilitates planning and logistics. Likely to aid diagnosis and care delivery in underserved areas in future. Greatest potential may be in training/simulation/situation analysis. | Susceptible to input bias (i.e., data used for training algorithms may not be applicable to all populations). Concerns about “black box” decision making in clinical situations. Requires extensive advance planning/training/infrastructure for use. | [82] [83] [32] |
| Robotics | Limited at present | Stand-off operation allows for access to dangerous/confined/inhospitable areas. Facilitates search and rescue. Dedicated clinical/surgical systems can deliver remote care. Can be combined with sensor networks and other technologies. Telemonitoring can augment reach of human carers in understaffed/underserved areas. | Expensive equipment. Infrastructure dependent. Requires highly skilled operators and secure communications. Clinical/surgical robots confined to limited procedures. May not be relevant for post-disaster care. | [54] [55] |
| Wireless Sensor Networks | Limited at present | Facilitate terrain/environmental monitoring. Can provide critical information for public health decision making. Synergistic with other DHTs (e.g., AI; robotics). Potential for supply chain/logistical monitoring in affected areas. | Limited direct clinical utility for healthcare delivery. May require centralized monitoring networks. | [84] |
| Drones/Uncrewed vehicles | Increasing | Strong potential for use in monitoring, search and rescue, and supply/logistics in affected areas. | May not be a core DHT component. High skill/training requirement at present. Limited power/battery life. | [57] [56] [58] |
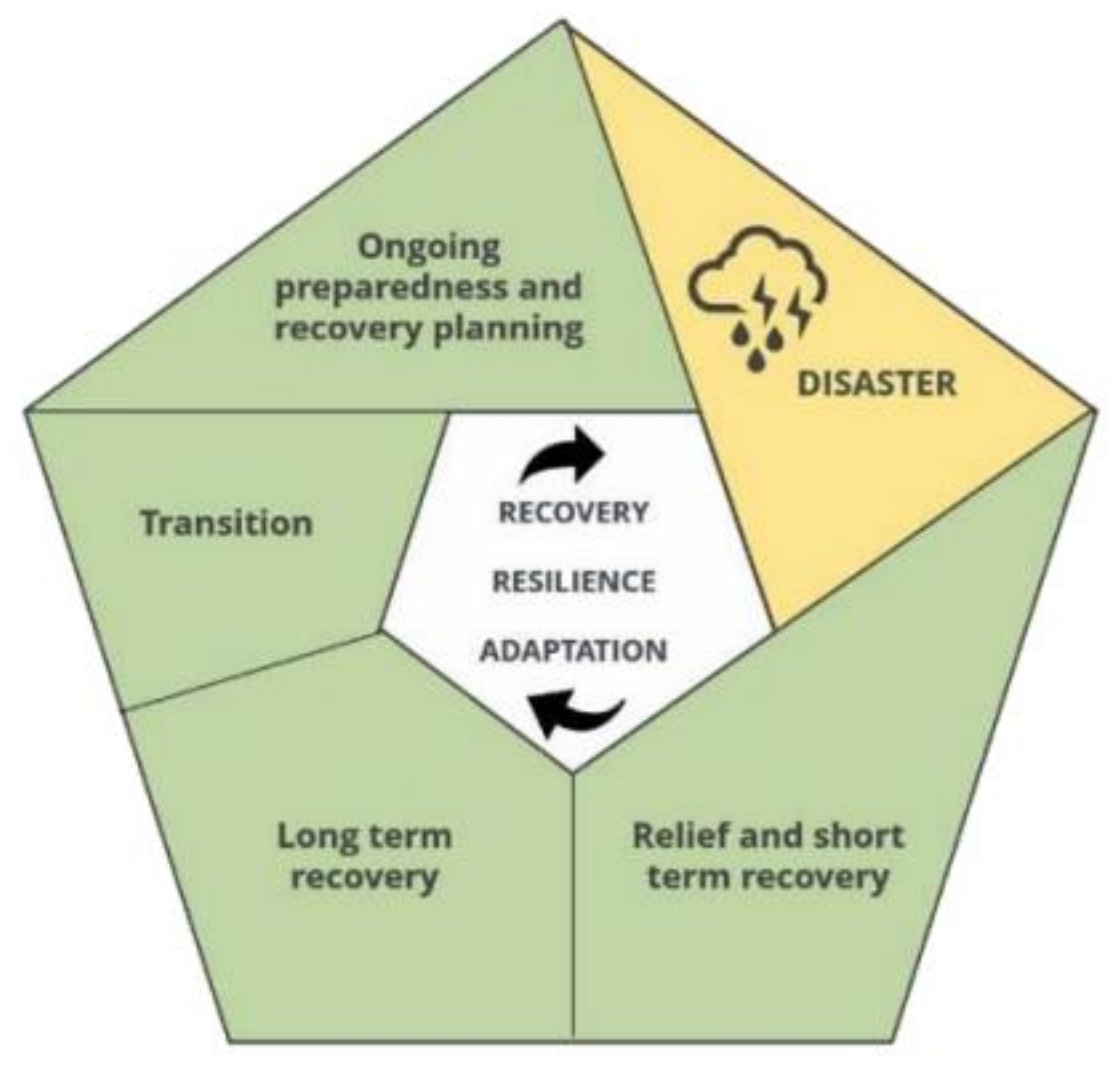
3. Disaster- and Climate-Resilient Healthcare Systems in the Context of Digital Health
Disaster Recovery Frameworks
4. Natural Disasters
5. Lessons from the Impacts of Natural Disasters on Digital Health Technology to Deliver Quality Healthcare
5.1. Study Methods and Analysis
5.2. Lessons Learned
5.2.1. Infrastructure
5.2.2. Vulnerabilities and Risks to Delivering Quality Healthcare in Disaster Settings
Experience of Using DHTs in the Aftermath of the 2015 Nepal Earthquake
Australian 2019–2020 Bushfires and 2022 Floods
Hurricane Florence, 2018, North Carolina, USA
| Study/Study Site | Natural Disaster | DHT Type | Equipment Required | Disaster Stage | DHT Application | DHT Strengths | Implementation Challenges | Lessons Learned |
|---|---|---|---|---|---|---|---|---|
| Vo A.H et al., 2010 [124] USA | Hurricane Ike | Telemedicine | Broadband computer networks, video monitors, cell phones. | Post-disaster response phase. | Provide a continuum of care and consultation services to those in need. | Telephone-based service with a greater outreach. | Disaster-related impacts. The long sustainability of the technology requires a secure, web-accessible file server system and the development of network hubs. | Flexibility of data networks is essential for resuming operation. Mobile phones can be used to facilitate healthcare but require ‘how to’ protocols. EMR notes in simple text are transferable between systems. Advance planning to secure critical data ahead of disasters by developing web-accessible file server systems. Develop fault-tolerant networks. |
| Nicogossian et al., 2011 [125] Armenia | 1988 earthquake | Telemedicine | Space Bridge communication infrastructure, video monitors, video recording. | Post-disaster response phase. | Provision of healthcare services to earthquake victims. | Well-established guidelines and protocols. | Safeguarding patient privacy, effective connectivity through telecommunications and internet. | A pre-existing system and connectivity are essential for rapid DHT implementation to meet the needs of disaster victims. The system must be staffed with trained personnel for effective consultation and services. |
| Callaway et al., 2012 [126] Haiti | 2010 earthquake | Mobile Health (iChart mHealth) | Gas-powered generator for electricity, satellite antenna for wireless network, cellular phones. | Post-disaster response phase. | Patient tracking, triage, postoperative care, protection of unaccompanied minors, patient handovers. | Reduced workload, improved patient care, adequate patient triage, and improved patient tracking. | No significant challenges reported. | iChart functioned with or without internet connectivity. Improved service delivery using scalable mobile technology. |
| Kim et al., 2013 [127] USA | Hurricanes, storms, typhoons and other disasters hitting the US gulf coast | Telehealth | Not reported. | Post-disaster recovery phase. | Provide telehealth services to a disaster-affected population across various health specialties. | Multiple shared challenges and recommendations were identified to support the scalable sustainability of telehealth programs. | Inadequate funding impacted the engagement and implementation. Regulatory challenges (i.e., reimbursement for the uninsured). Lack of guidance on establishment of telehealth policies and procedures. User’s confidentiality. Inadequately trained workforce. | Lack of IT support impacts DHT implementation. Adequate bandwidth and network architecture are essential to good connection. Strong vendor support and equipment testing essential for effective response. The framework is adaptable to future telehealth programs for high service needs with limited resources. |
| Nagata et al., 2013 [128] Japan (Fukushima) | 2011 earthquake | Cloud-based Electronic Health Record (EHR) | Low-bandwidth computer networks, laptops, and portable internet Wi-Fi devices. | Post-disaster response phase. | Increase coordination and communication to enhance medical response in the aftermath of the earthquake and subsequent nuclear disaster. | Low-bandwidth internet was sufficient for EHR implementation. Low-cost intervention. | Internet services required for implementation, data security, and privacy. | Low-bandwidth, low-cost cloud-hosted EHR could perform functions needed to provide safe and quality care. Hospital EHRs need to be connected to a national EHR to permit access to patient data during disasters. Benefits of EHR data accessibility during disasters are likely to outweigh the risks concerning privacy issues. Guidelines to manage privacy concerns regarding a national EHR system need to be developed. |
| Qadir et al., 2016 [129] Pakistan | 2015 flood and earthquake | Telepsychiatry | Not described. | Post-disaster response phase. | Treatment of post-traumatic stress disorder (PTSD). | Active community engagement in the telepsychiatry module. | Not reported | Outcome not assessed. Telepsychiatry could deliver effective services where regular services are interrupted. |
| Taylor et al., 2017 [130] USA | Hurricane Katrina and Hurricane Harvey | EHR | Laptop | Pre-disaster preparedness and post-disaster response phase. | Safe continuum of care in the face of disasters. | EHR was already set up following Hurricane Katrina, which facilitated service continuation during Hurricane Harvey. | Not reported | High-quality healthcare services were achievable amidst the disaster. Patient portals available to access blood test results and medication prescriptions remotely. |
| Stasiak et al., 2018 [131] New Zealand | 2011 Canterbury earthquake | Computerized cognitive behavioural therapy (BRAVE-ONLINE) | Computer with internet services, telephone. | Post-disaster recovery phase. | Cognitive behavioural therapy for anxiety and PTSD. | The DHT (BRAVE-ONLINE) was a validated tool. | Participants were required to be competent technology (computer and internet) users. | With uninterrupted telecommunication services and electricity supply, DHTs can be successfully implemented to provide remote behavioural therapy services. |
| French et al., 2019 [132] USA | Hurricane Florence | Telehealth | Devices to support video assessment (video monitors and low-bandwidth connection), and cellular phones. | Pre-disaster preparedness and post-disaster response phase. | Test the applicability of telehealth support to evacuation shelters and emergency medical services. | Could operate in settings with low internet bandwidth. Real-time patient assessment and treatment. | Cellular towers can be oversubscribed, limiting the connectivity. | Effective implementation and testing of DHTs before the storm were achieved with minimal changes to existing infrastructures. Was not used in response phase. |
| Pasipanodya et al., 2020 [133] USA | 2015 California fire | Telemedicine | Tablet with internet connectivity, home blood pressure machine. | Pre-disaster period and immediate response period following the disaster. | Management of spinal cord injury. | Cheap and effective. | Not described | Uninterrupted quality of care was possible amidst the California wildfire and its aftermath. Changes to reimbursement structure is necessary. |
| Grover et al., 2020 [123] USA | Hurricane Florence | Telemedicine (RelyMD) | Tablet | Pre-disaster preparedness and post-disaster response phase. | Reduction in unnecessary emergency medical service utilization and emergency department visits. | The DHT in existence before the disaster. | Not described | Telemedicine limitations were not reported. |
| Sago et al., 2020 [134] Croatia | Earthquake following the COVID pandemic | Telepsychiatry | Telephone, computers with internet connections for Skype consultations, headphones, smartphones. | Post-disaster early response phase during the COVID-19 pandemic. | Psychological counselling and psychotherapy. | Participants’ compliance and active engagement during the telepsychiatry sessions. | Management of social and interpersonal aspects of participants in the group counselling sessions. Use of technology by the service seekers and service providers. Burnout during long sessions of artificial/remote contact. | DHT limitations were not reported. |
| Paratz et al., 2022 [135] Timor-Leste | Flood and population dislocation | Cardiac telehealth service | Video monitor, handheld echocardiograms, mobile phones, and landline phones. | Post-disaster response phase during the COVID-19 pandemic. | Management of cardiac care services. | An effective strategy of critical care service delivery amidst the disaster. | Poor internet connection and less coverage. Repeated cycles of disaster during telemedicine services’ reduced efficiency of service delivery. Difficulty in establishing contacts with service seekers. Financial barriers. | Unreliable internet connection and fixed broadband impacted transmission of echocardiographic images. Zoom link used for clinic appointments. Echocardiographic images shared via email and WhatsApp. Recommend cloud-based system for in-time image optimisation |
6. Future Directions
6.1. Citizen Science
6.2. Climate-Resilient Digital Healthcare
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tilahun, B.; Gashu, K.D.; Mekonnen, Z.A.; Endehabtu, B.F.; Angaw, D.A. Mapping the Role of Digital Health Technologies in Prevention and Control of COVID-19 Pandemic: Review of the Literature. Yearb. Med. Inform. 2021, 30, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.; Yeganeh, L.; Cook, O.; Crawford, K.; Wong, P.; Allen, J. Using telehealth consultations for healthcare provision to patients from non-Indigenous racial/ethnic minorities: A systematic review. J. Am. Med. Inform. Assoc. 2022, 29, 970–982. [Google Scholar] [CrossRef]
- Volkmer, I. Social Media and COVID-19: A Global Study of Digital Crisis Interaction among Gen Z and Millennials; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Chandra, M.; Kumar, K.; Thakur, P.; Chattopadhyaya, S.; Alam, F.; Kumar, S. Digital technologies, healthcare and COVID-19: Insights from developing and emerging nations. Health Technol. 2022, 12, 547–568. [Google Scholar] [CrossRef] [PubMed]
- Gambo, N.; Perry, M.; Kashefi, A.; Ayoung, D.A. Harnessing social and collaborative tools in digital disaster response work: Implications for design and practice. Inf. Dev. 2021, 37, 525–537. [Google Scholar] [CrossRef]
- Lai, J.; Widmar, N.O. Revisiting the Digital Divide in the COVID-19 Era. Appl. Econ. Perspect. Policy 2021, 43, 458–464. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare Digital Health. Available online: https://www.aihw.gov.au/reports/australias-health/digital-health (accessed on 21 November 2022).
- Soobiah, C.; Cooper, M.; Kishimoto, V.; Bhatia, R.S.; Scott, T.; Maloney, S.; Larsen, D.; Wijeysundera, H.C.; Zelmer, J.; Gray, C.S.; et al. Identifying optimal frameworks to implement or evaluate digital health interventions: A scoping review protocol. BMJ Open 2020, 10, e037643. [Google Scholar] [CrossRef] [PubMed]
- United States Food and Drug Administration Digital Health. Available online: https://www.fda.gov/medical-devices/digital-health-center-excellence/what-digital-health (accessed on 21 November 2022).
- Holmner, A.; Ebi, K.L.; Lazuardi, L.; Nilsson, M. Carbon footprint of telemedicine solutions--unexplored opportunity for reducing carbon emissions in the health sector. PLoS ONE 2014, 9, e105040. [Google Scholar] [CrossRef]
- Watts, N.; Amann, M.; Ayeb-Karlsson, S.; Belesova, K.; Bouley, T.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; Chambers, J.; et al. The Lancet Countdown on health and climate change: From 25 years of inaction to a global transformation for public health. Lancet 2018, 391, 581–630. [Google Scholar] [CrossRef]
- Rahimi-Ardabili, H.; Magrabi, F.; Coiera, E. Digital health for climate change mitigation and response: A scoping review. J. Am. Med. Inform. Assoc. 2022, 29, 2140–2152. [Google Scholar] [CrossRef] [PubMed]
- Lokmic-Tomkins, Z.; Davies, S.; Block, L.J.; Cochrane, L.; Dorin, A.; von Gerich, H.; Lozada-Perezmitre, E.; Reid, L.; Peltonen, L.M. Assessing the carbon footprint of digital health interventions: A scoping review. J. Am. Med. Inform. Assoc. 2022, 29, 2128–2139. [Google Scholar] [CrossRef]
- Lokmic-Tomkins, Z.; Borda, A.; Humphrey, K. Designing digital health applications for climate change mitigation and adaptation. Med. J. Aust. 2023, 218, 106–110. [Google Scholar] [CrossRef]
- Abalansa, S.; El Mahrad, B.; Icely, J.; Newton, A. Electronic Waste, an Environmental Problem Exported to Developing Countries: The GOOD, the BAD and the UGLY. Sustainability 2021, 13, 5302. [Google Scholar] [CrossRef]
- World Health Organization Soaring E-Waste Affects the Health of Millions of Children, WHO Warns. Available online: https://www.who.int/news/item/15-06-2021-soaring-e-waste-affects-the-health-of-millions-of-children-who-warns#:~:text=Other%20adverse%20child%20health%20impacts,as%20cancer%20and%20cardiovascular%20disease.&text=%E2%80%9CImproper%20e%2Dwaste%20management%20is%20the%20cause (accessed on 21 November 2022).
- NEJM Catalyst, What is telehealth? NEJM Catal. 2018, 4.
- Shah, B.R.; Schulman, K. Do not let a good crisis go to waste: Health care’s path forward with virtual care. NEJM Catal. Innov. Care Deliv. 2021, 2. [Google Scholar]
- Delaigue, S.; Bonnardot, L.; Steichen, O.; Garcia, D.M.; Venugopal, R.; Saint-Sauveur, J.F.; Wootton, R. Seven years of telemedicine in Médecins Sans Frontières demonstrate that offering direct specialist expertise in the frontline brings clinical and educational value. J. Glob. Health 2018, 8, 020414. [Google Scholar] [CrossRef] [PubMed]
- The National Alliance for Health Information Technology. Defining Key Health Information Technology Terms; The Office of the National Coordinator for Health Information Technology: Washington, DC, USA, 2008.
- Australian Government Department of Health and Aged Care Electronic Health Records. Available online: https://www.health.gov.au/topics/health-technologies-and-digital-health/about/electronic-health-records (accessed on 30 November 2022).
- Brown, S.H.; Fischetti, L.F.; Graham, G.; Bates, J.; Lancaster, A.E.; McDaniel, D.; Gillon, J.; Darbe, M.; Kolodner, R.M. Use of Electronic Health Records in Disaster Response: The Experience of Department of Veterans Affairs After Hurricane Katrina. Am. J. Public Health 2007, 97 (Suppl. 1), S136–S141. [Google Scholar] [CrossRef] [PubMed]
- Mohsin-Shaikh, S.; Furniss, D.; Blandford, A.; McLeod, M.; Ma, T.; Beykloo, M.Y.; Franklin, B.D. The impact of electronic prescribing systems on healthcare professionals’ working practices in the hospital setting: A systematic review and narrative synthesis. BMC Health Serv. Res. 2019, 19, 742. [Google Scholar] [CrossRef]
- Australian Government Department of Health Fact Sheet—National Health Plan A Guide for Pharmacists. Available online: https://www.health.gov.au/sites/default/files/documents/2022/03/covid-19-national-health-plan-prescriptions-via-telehealth-a-guide-for-pharmacists.pdf (accessed on 30 November 2022).
- Naseriasl, M.; Adham, D.; Janati, A. E-referral Solutions: Successful Experiences, Key Features and Challenges—a Systematic Review. Mater Sociomed 2015, 27, 195. [Google Scholar] [CrossRef]
- Azamar-Alonso, A.; Costa, A.P.; Huebner, L.A.; Tarride, J.E. Electronic referral systems in health care: A scoping review. Clin. Outcomes Res. 2019, 11, 325–333. [Google Scholar] [CrossRef]
- World Health Organization. Executive Board, mHealth: Use of Appropriate Digital Technologies for Public Health: Report by the Director-General; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Rowland, S.P.; Fitzgerald, J.E.; Holme, T.; Powell, J.; McGregor, A. What is the clinical value of mHealth for patients? NPJ Digit. Med. 2020, 3, 4. [Google Scholar] [CrossRef]
- Head, K.J.; Noar, S.M.; Iannarino, N.T.; Grant Harrington, N. Efficacy of text messaging-based interventions for health promotion: A meta-analysis. Soc. Sci. Med. 2013, 97, 41–48. [Google Scholar] [CrossRef]
- Nunes, A.; Limpo, T.; Castro, S.L. Acceptance of Mobile Health Applications: Examining Key Determinants and Moderators. Front. Psychol. 2019, 10, 2791. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J. Mathematical logic in artificial intelligence. Daedalus 1988, 117, 297–311. [Google Scholar]
- Arora, A. Conceptualising artificial intelligence as a digital healthcare innovation: An introductory review. Med. Devices 2020, 13, 223. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Kamboj, S.; Bag, S. Role of risks in the development of responsible artificial intelligence in the digital healthcare domain. Inf. Syst. Front. 2021, 1–18. [Google Scholar] [CrossRef]
- Gunasekeran, D.V.; Tseng, R.M.W.W.; Tham, Y.-C.; Wong, T.Y. Applications of digital health for public health responses to COVID-19: A systematic scoping review of artificial intelligence, telehealth and related technologies. NPJ Digit. Med. 2021, 4, 40. [Google Scholar] [CrossRef]
- Lendvay, T.S.; Rosen, J.; Hannaford, B. Telerobotics: Its Future in Clinical Application. In Pediatric Robotic and Reconstructive Urology; Wiley Online Library: Hoboken, NJ, USA, 2011; pp. 314–327. [Google Scholar] [CrossRef]
- Avgousti, S.; Christoforou, E.G.; Panayides, A.S.; Voskarides, S.; Novales, C.; Nouaille, L.; Pattichis, C.S.; Vieyres, P. Medical telerobotic systems: Current status and future trends. BioMedical Eng. OnLine 2016, 15, 96. [Google Scholar] [CrossRef]
- Zanchettin, A.M.; Facciotti, F. A collaborative robotic solution to partly automate SARS-CoV-2 serological tests in small facilities. SLAS Technol. 2022, 27, 100–106. [Google Scholar] [CrossRef]
- Queralta, J.P.; Taipalmaa, J.; Pullinen, B.C.; Sarker, V.K.; Gia, T.N.; Tenhunen, H.; Gabbouj, M.; Raitoharju, J.; Westerlund, T. Collaborative multi-robot systems for search and rescue: Coordination and perception. arXiv 2020, arXiv:2008.12610. [Google Scholar]
- Camarillo, D.B.; Krummel, T.M.; Salisbury, J.K., Jr. Robotic technology in surgery: Past, present, and future. Am. J. Surg. 2004, 188, 2–15. [Google Scholar] [CrossRef]
- Merck. Petra: The Potential of Medical Robots. Available online: https://www.merckgroup.com/en/research/science-space/envisioning-tomorrow/precision-medicine/petra.html (accessed on 22 November 2022).
- Scoglio, A.A.J.; Reilly, E.D.; Gorman, J.A.; Drebing, C.E. Use of Social Robots in Mental Health and Well-Being Research: Systematic Review. J. Med. Internet Res. 2019, 21, e13322. [Google Scholar] [CrossRef]
- Guo, J.; Yu, S.; Li, Y.; Huang, T.H.; Wang, J.; Lynn, B.; Fidock, J.; Shen, C.L.; Edwards, D.; Su, H. A soft robotic exo-sheath using fabric EMG sensing for hand rehabilitation and assistance. Proceedings of 2018 IEEE International Conference on Soft Robotics (RoboSoft), Livorno, Italy, 24–28 April 2018; pp. 497–503. [Google Scholar]
- Niswar, M.; Wijaya, A.S.; Ridwan, M.; Adnan; Ilham, A.A.; Sadjad, R.S.; Vogel, A. The design of wearable medical device for triaging disaster casualties in developing countries. Proceedings of 2015 Fifth International Conference on Digital Information Processing and Communications (ICDIPC), Sierre, Switzerland, 7–9 October 2015; pp. 207–212. [Google Scholar]
- Sadoughi, F.; Behmanesh, A.; Sayfouri, N. Internet of things in medicine: A systematic mapping study. J. Biomed. Inform. 2020, 103, 103383. [Google Scholar] [CrossRef] [PubMed]
- Vijayan, V.; Connolly, J.P.; Condell, J.; McKelvey, N.; Gardiner, P. Review of wearable devices and data collection considerations for connected health. Sensors 2021, 21, 5589. [Google Scholar] [CrossRef] [PubMed]
- Shang, T.; Zhang, J.Y.; Thomas, A.; Arnold, M.A.; Vetter, B.N.; Heinemann, L.; Klonoff, D.C. Products for monitoring glucose levels in the human body with noninvasive optical, noninvasive fluid sampling, or minimally invasive technologies. J. Diabetes Sci. Technol. 2022, 16, 168–214. [Google Scholar] [CrossRef] [PubMed]
- Brinkmann, B.H.; Karoly, P.J.; Nurse, E.S.; Dumanis, S.B.; Nasseri, M.; Viana, P.F.; Schulze-Bonhage, A.; Freestone, D.R.; Worrell, G.; Richardson, M.P. Seizure diaries and forecasting with wearables: Epilepsy monitoring outside the clinic. Front. Neurol. 2021, 12, 690404. [Google Scholar] [CrossRef] [PubMed]
- Bayoumy, K.; Gaber, M.; Elshafeey, A.; Mhaimeed, O.; Dineen, E.H.; Marvel, F.A.; Martin, S.S.; Muse, E.D.; Turakhia, M.P.; Tarakji, K.G. Smart wearable devices in cardiovascular care: Where we are and how to move forward. Nat. Rev. Cardiol. 2021, 18, 581–599. [Google Scholar] [CrossRef] [PubMed]
- Korostynska, O. Sensors for Smart Packaging in Healthcare and Food Industry. In Proceedings of the 2021 IEEE Sensors, Sydney, Australia, 31 October–3 November 2021; p. 1. [Google Scholar]
- Tosh, P.K.; Feldman, H.; Christian, M.D.; Devereaux, A.V.; Kissoon, N.; Dichter, J.R. Business and continuity of operations: Care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest 2014, 146, e103S–e117S. [Google Scholar] [CrossRef]
- Farsi, M.; Elhosseini, M.A.; Badawy, M.; Ali, H.A.; Eldin, H.Z. Deployment techniques in wireless sensor networks, coverage and connectivity: A survey. IEEE Access 2019, 7, 28940–28954. [Google Scholar] [CrossRef]
- Sumartojo, S.; Lugli, D. Lively robots: Robotic technologies in COVID-19. Soc. Cult. Geogr. 2021, 23, 1220–1237. [Google Scholar] [CrossRef]
- Amin, R.; Islam, S.H.; Biswas, G.; Khan, M.K.; Kumar, N. A robust and anonymous patient monitoring system using wireless medical sensor networks. Future Gener. Comput. Syst. 2018, 80, 483–495. [Google Scholar] [CrossRef]
- Martinello, N.; Loshak, H. Experiences with and expectations of robotic surgical systems: A rapid qualitative review. 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK562938/ (accessed on 21 November 2022).
- De’Angelis, N.; Khan, J.; Marchegiani, F.; Bianchi, G.; Aisoni, F.; Alberti, D.; Ansaloni, L.; Biffl, W.; Chiara, O.; Ceccarelli, G. Robotic surgery in emergency setting: 2021 WSES position paper. World J. Emerg. Surg. 2022, 17, 4. [Google Scholar] [CrossRef] [PubMed]
- Surmann, H.; Slomma, D.; Grafe, R.; Grobelny, S. Deployment of Aerial Robots During the Flood Disaster in Erftstadt/Blessem in July 2021. In Proceedings of the 2022 8th International Conference on Automation, Robotics and Applications (ICARA), Prague, Czech Republic, 18–20 February 2022; pp. 97–102. [Google Scholar]
- Daud, S.M.S.M.; Yusof, M.Y.P.M.; Heo, C.C.; Khoo, L.S.; Singh, M.K.C.; Mahmood, M.S.; Nawawi, H. Applications of drone in disaster management: A scoping review. Sci. Justice 2022, 62, 30–42. [Google Scholar] [CrossRef]
- Johnson, A.M.; Cunningham, C.J.; Arnold, E.; Rosamond, W.D.; Zègre-Hemsey, J.K. Impact of using drones in emergency medicine: What does the future hold? Open Access Emerg. Med. OAEM 2021, 13, 487. [Google Scholar] [CrossRef]
- Ates, H.C.; Yetisen, A.K.; Güder, F.; Dincer, C. Wearable devices for the detection of COVID-19. Nat. Electron. 2021, 4, 13–14. [Google Scholar] [CrossRef]
- Surantha, N.; Atmaja, P.; Wicaksono, M. A review of wearable internet-of-things device for healthcare. Procedia Comput. Sci. 2021, 179, 936–943. [Google Scholar] [CrossRef]
- Royea, R.; Buckman, K.J.; Benardis, M.; Holmes, J.; Fletcher, R.L.; Eyk, N.; Rajendra Acharya, U.; Ellenhorn, J.D.I. An introduction to the Cyrcadia Breast Monitor: A wearable breast health monitoring device. Comput. Methods Programs Biomed. 2020, 197, 105758. [Google Scholar]
- Piwek, L.; Ellis, D.A.; Andrews, S.; Joinson, A. The Rise of Consumer Health Wearables: Promises and Barriers. PLOS Med. 2016, 13, e1001953. [Google Scholar] [CrossRef] [PubMed]
- Ben, L. Earthquake Warning app Sends First ever Alert to Users in California. Available online: https://9to5mac.com/2019/12/19/earthquake-warning-app/ (accessed on 25 November 2022).
- Tai, Y.; Yu, T.-T. Using smartphones to locate trapped victims in disasters. Sensors 2022, 22, 7502. [Google Scholar] [CrossRef]
- Dillon, T.; Wu, C.; Chang, E. Cloud Computing: Issues and Challenges. In Proceedings of the 2010 24th IEEE International Conference on Advanced Information Networking and Applications, Perth, WA, Australia, 20–23 April 2010; pp. 27–33. [Google Scholar]
- Cheikhrouhou, O.; Koubaa, A.; Zarrad, A. A Cloud Based Disaster Management System. J. Sens. Actuator Netw. 2020, 9, 6. [Google Scholar] [CrossRef]
- Loeza-Mejía, C.I.; Sánchez-DelaCruz, E.; Pozos-Parra, P.; Landero-Hernández, L.A. The potential and challenges of Health 4.0 to face COVID-19 pandemic: A rapid review. Health Technol. 2021, 11, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Madanian, S.; Parry, D. IoT, cloud computing and big data: Integrated framework for healthcare in disasters. Stud. Health Technol. Inform. 2019, 998–1002. [Google Scholar]
- Lokmic, Z.; Hallenstein, L.; Penington, A. Parental experience of prenatal diagnosis of lymphatic malformation. Lymphology 2017, 50, 16–26. [Google Scholar] [PubMed]
- World Health Organization. WHO Guidance on Research Methods for Health Emergency and Disaster Risk Management; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Sylvia Chou, W.-Y.; Gaysynsky, A.; Cappella, J.N. Where We Go from Here: Health Misinformation on Social Media; American Public Health Association: Washington, DC, USA, 2020; Volume 110, pp. S273–S275. [Google Scholar]
- Anikeeva, O.; Steenkamp, M.; Arbon, P. The future of social media use during emergencies in Australia: Insights from the 2014 Australian and New Zealand disaster and emergency management conference social media workshop. In Effective Communication During Disasters; Apple Academic Press: Palm Bay, FL, USA, 2016; pp. 151–162. [Google Scholar]
- Good Karma Networks. Available online: https://www.goodkarmaeffect.com/networks/networks (accessed on 30 November 2022).
- Tangari, G.; Ikram, M.; Ijaz, K.; Kaafar, M.A.; Berkovsky, S. Mobile health and privacy: Cross sectional study. BMJ 2021, 373, n1248. [Google Scholar] [CrossRef] [PubMed]
- Gething, P.W.; Tatem, A.J. Can mobile phone data improve emergency response to natural disasters? PLoS Med. 2011, 8, e1001085. [Google Scholar] [CrossRef] [PubMed]
- Kongsiriwattana, W.; Gardner-Stephen, P. Smart-phone battery-life short-fall in disaster response: Quantifying the gap. Proceedings of 2016 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 13–16 October 2016; pp. 220–225. [Google Scholar]
- Ahmad, G.I.; Singla, J.; Giri, K.J. Security and Privacy of E-health Data. In Multimedia Security: Algorithm Development, Analysis and Applications; Giri, K.J., Parah, S.A., Bashir, R., Muhammad, K., Eds.; Springer: Singapore, 2021; pp. 199–214. [Google Scholar] [CrossRef]
- Balsari, S.; Kiang, M.; Buckee, C. Data in crisis—Rethinking disaster preparedness in the United States. New Engl. J. Med. 2021, 385, 1526–1530. [Google Scholar] [CrossRef] [PubMed]
- Doarn, C.R.; Merrell, R.C. Telemedicine and e-Health in Disaster Response; Mary Ann Liebert, Inc.: New Rochelle, NY, USA, 2014; Volume 20, pp. 605–606. [Google Scholar]
- Litvak, M.; Miller, K.; Boyle, T.; Bedenbaugh, R.; Smith, C.; Meguerdichian, D.; Reisman, D.; Biddinger, P.; Licurse, A.; Goralnick, E. Telemedicine use in disasters: A scoping review. Disaster Med. Public Health Prep. 2021, 1–10. [Google Scholar] [CrossRef]
- Baek, J.; Simon-Friedt, B.; Lopez, A.; Kolman, J.M.; Nicolas, J.; Jones, S.L.; Phillips, R.A.; Menser, T. Assessing patient needs during natural disasters: Mixed methods analysis of portal messages sent during Hurricane Harvey. J. Med. Internet Res. 2021, 23, e31264. [Google Scholar] [CrossRef]
- Lu, S.; Christie, G.A.; Nguyen, T.T.; Freeman, J.D.; Hsu, E.B. Applications of artificial intelligence and machine learning in disasters and public health emergencies. Disaster Med. Public Health Prep. 2022, 16, 1674–1681. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Bocchini, P.; Davison, B.D. Applications of artificial intelligence for disaster management. Nat. Hazards 2020, 103, 2631–2689. [Google Scholar] [CrossRef]
- Prasad, D.; Hassan, A.; Verma, D.K.; Sarangi, P.; Singh, S. Disaster Management System using Wireless Sensor Network: A Review. Proceedings of 2021 International Conference on Computational Intelligence and Computing Applications (ICCICA), Nagpur, India, 26–27 November 2021; pp. 1–6. [Google Scholar]
- Al Knawy, B.; Adil, M.; Crooks, G.; Rhee, K.; Bates, D.; Jokhdar, H.; Klag, M.; Lee, U.; Mokdad, A.H.; Schaper, L.; et al. The Riyadh Declaration: The role of digital health in fighting pandemics. Lancet 2020, 396, 1537–1539. [Google Scholar] [CrossRef]
- World Health Organization. WHO Technical Guidance Notes on Sendai Framework Reporting for Ministries of Health; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Global Strategy on Digital Health 2020–2025; World Health Organization: Geneva, Switzerland, 2021.
- FHIR. Available online: http://hl7.org/fhir/ (accessed on 30 November 2022).
- Queensland Fire and Emergency Services. Queensland Prevention Preparedness, Response and Recovery Disaster Management Guideline; Queensland Fire and Emergency Services: Caboolture, QLD, Australia, 2022. [Google Scholar]
- Kariotis, T. Digital Government and Disaster Responses: Empowering Community-Led Recovery. 2022. Available online: https://apo.org.au/node/317945 (accessed on 30 November 2022).
- Binskin, M.; Bennett, A.; Macintosh, A. Royal Commission into National Natural Disaster Arrangements Report; Commonwealth of Australia: Canberra, Australia, 2020. [Google Scholar]
- United Nations Framework Convention on Climate Change Zimbabwe and the United Nations Framework Convention on Climate Change. Available online: https://unfccc.int/resource/ccsites/zimbab/conven/text/art01.htm (accessed on 8 October 2022).
- World Health Organization. Community Emergency Preparedness: A Manual for Managers and Policy-Makers; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Allan, R.P.; Barlow, M.; Byrne, M.P.; Cherchi, A.; Douville, H.; Fowler, H.J.; Gan, T.Y.; Pendergrass, A.G.; Rosenfeld, D.; Swann, A.L. Advances in understanding large-scale responses of the water cycle to climate change. Ann. New York Acad. Sci. 2020, 1472, 49–75. [Google Scholar] [CrossRef] [PubMed]
- Kraaijenbrink, P.D.; Stigter, E.E.; Yao, T.; Immerzeel, W.W. Climate change decisive for Asia’s snow meltwater supply. Nat. Clim. Change 2021, 11, 591–597. [Google Scholar] [CrossRef]
- Mukhopadhyay, R.; Sarkar, B.; Jat, H.S.; Sharma, P.C.; Bolan, N.S. Soil salinity under climate change: Challenges for sustainable agriculture and food security. J. Environ. Manag. 2021, 280, 111736. [Google Scholar] [CrossRef] [PubMed]
- Van Aalst, M.K. The impacts of climate change on the risk of natural disasters. Disasters 2006, 30, 5–18. [Google Scholar] [CrossRef]
- Rousi, E.; Kornhuber, K.; Beobide-Arsuaga, G.; Luo, F.; Coumou, D. Accelerated western European heatwave trends linked to more-persistent double jets over Eurasia. Nat. Commun. 2022, 13, 3851. [Google Scholar] [CrossRef]
- Moreau, P.; Ismael, S.; Masadeh, H.; Katib, E.A.; Viaud, L.; Nordon, C.; Herfat, S. 3D technology and telemedicine in humanitarian settings. Lancet Digit. Health 2020, 2, e108–e110. [Google Scholar] [CrossRef]
- Morchel, H.; Raheem, M.; Stevens, L. Electronic health records access during a disaster. Online J Public Health Inf. 2014, 5, 232. [Google Scholar]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- United Nations Office for Disaster Risk Reduction; International Science Council. Hazard Definition & Classification Review: Technical Report; UNDRR: Geneva, Switzerland, 2020. [Google Scholar]
- UNDRR; International Science Council. Hazard Information Profiles-Supplement to UNDRR-ISC Hazard Definiton and Classification Review-Technical Report; United Nations Office for Disaster Risk Reduction (UNDRR): Geneva, Switzerland, 2021. [Google Scholar]
- Jonathan, W.; Dickon, P.; Hamid, S.; Hauke, E.; Mekala, K.; Brodie, B.; Peter, C.; Byron, R. Will Infrastructure Bend or Break under Climate Stress? Available online: https://www.mckinsey.com/capabilities/sustainability/our-insights/will-infrastructure-bend-or-break-under-climate-stress (accessed on 25 November 2022).
- Federal Communications Commission. FCC Chairman Genachowski Announces Post-Superstorm Sandy Field Hearings to Examine New Challenges to Resiliency of U.S. Communications Networks during Natural Disasters and Other Times of Crisis In Public Safety and Homeland Security; Office of Former Chairman Genachowski, Media Relations: Washington, DC, USA, 2012.
- GSMA. The 2017 Atlantic Hurricane Season: Mobile Industry Impact and Response in the Caribbean. Available online: https://www.gsma.com/mobilefordevelopment/resources/the-2017-atlantic-hurricane-season-mobile-industry-impact-and-response-in-the-caribbean/ (accessed on 25 November 2022).
- Lal, A.; Patel, M.; Hunter, A.; Phillips, C. Towards resilient health systems for increasing climate extremes: Insights from the 2019–20 Australian bushfire season. Int. J. Wildland Fire 2020, 30, 1–5. [Google Scholar] [CrossRef]
- Lokmic-Tomkins, Z.; Choo, D.; Foley, P.; Dix, S.; Wong, P.; Brand, G. Pre-registration nursing students’ perceptions of their baseline digital literacy and what it means for education: A prospective COHORT survey study. Nurse Educ. Today 2022, 111, 105308. [Google Scholar] [CrossRef]
- Lokmic-Tomkins, Z.; Nayna Schwerdtle, P.; Armstrong, F. Engaging with our responsibility to protect health from climate change. J. Adv. Nurs. 2022. [Google Scholar] [CrossRef] [PubMed]
- Pezard, S.; Thaler, D.E.; Grill, B.; Klein, A.; Robson, S. Nepal Disaster Management and Reference Handbook; Center for Excellence in Disaster Management & Humanitarian Assistance: Joint Base Pearl Harbor–Hickam, HI, USA, 2017. [Google Scholar]
- Nepal Disaster Risk Reduction Portal. Nepal Earthquake 2015: Country Profile; Ministry of Home Affairs, Nepal: Kathmandu, Nepal, 2015. [Google Scholar]
- Basu, M.; Ghosh, S.; Jana, A.; Bandyopadhyay, S.; Singh, R. Medical Requirements During a Natural Disaster: A Case Study on WhatsApp Chats Among Medical Personnel During the 2015 Nepal Earthquake. Disaster Med. Public Health Prep. 2017, 11, 652–655. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Crane, O.; Balen, J.; Devkota, B.; Ghimire, S.; Rushton, S. Use of information and communication technologies in the formal and informal health system responses to the 2015 Nepal earthquakes. Health Policy Plan. 2017, 32 (Suppl. 3), iii48–iii58. [Google Scholar] [CrossRef] [PubMed]
- CoastAdapt Australia’s Climate-Drivers, Variability and Extremes. Available online: https://coastadapt.com.au/australias-climate-drivers-variability-and-extremes (accessed on 25 November 2022).
- Australian Government Bureau of Meteorology. The Recent Climate–News, Reports and Summaries. Available online: http://www.bom.gov.au/climate/current/ (accessed on 25 November 2022).
- Commonwealth Scientific and Industrial Research Organisation Climate Change in Australia. Available online: https://www.csiro.au/en/research/environmental-impacts/climate-change/climate-change-information (accessed on 25 November 2022).
- Clarke, H.; Cirulis, B.; Penman, T.; Price, O.; Boer, M.M.; Bradstock, R. The 2019–2020 Australian forest fires are a harbinger of decreased prescribed burning effectiveness under rising extreme conditions. Sci. Rep. 2022, 12, 1–10. [Google Scholar] [CrossRef]
- NASA Earth Observatory Flooding in Eastern Australia. Available online: https://earthobservatory.nasa.gov/images/150542/flooding-in-eastern-australia#:~:text=Waves%20of%20heavy%20rainfall%20left,South%20Wales%20to%20northern%20Victoria (accessed on 25 November 2022).
- Senate Public Administration References Committee. Lessons to be Learned in Relation to the Australian Bushfire Season 2019–20; 2021. Available online: https://www.aph.gov.au/Parliamentary_Business/Committees/Senate/Finance_and_Public_Administration/Bushfirerecovery (accessed on 25 November 2022).
- Brooker, C. Review bushfire response: A nation in flames. AJP: Aust. J. Pharm. 2020, 101, 20–22. [Google Scholar]
- Australian Digital Health Agency. Increased Use of My Health Record by Healthcare Providers; Australian Government: Sydney, NSW, Australia, 2020.
- Australian Digital Health Agency. Help Is at Hand Information for Those Flooded, Stranded-My Health Record, Electronic Prescriptions and Telehealth Can Help; Government of Australia: Sydney, NSW, Australia, 2022.
- Grover, J.M.; Smith, B.; Williams, J.G.; Patel, M.D.; Cabanas, J.G.; Brice, J.H. Novel Use of Telemedicine by Hurricane Evacuation Shelters. Prehosp Emerg. Care 2020, 24, 804–812. [Google Scholar] [CrossRef]
- Vo, A.H.; Brooks, G.B.; Bourdeau, M.; Farr, R.; Raimer, B.G. University of Texas Medical Branch telemedicine disaster response and recovery: Lessons learned from hurricane Ike. Telemed. J. E-Health 2010, 16, 627–633. [Google Scholar] [CrossRef]
- Nicogossian, A.E.; Doarn, C.R. Armenia 1988 earthquake and telemedicine: Lessons learned and forgotten. Telemed. J. E-Health 2011, 17, 741–745. [Google Scholar] [CrossRef]
- Callaway, D.W.; Peabody, C.R.; Hoffman, A.; Cote, E.; Moulton, S.; Baez, A.A.; Nathanson, L. Disaster Mobile Health Technology: Lessons from Haiti. Prehospital Disaster Med. 2012, 27, 148–152. [Google Scholar] [CrossRef]
- Kim, T.J.; Arrieta, M.I.; Eastburn, S.L.; Icenogle, M.L.; Slagle, M.; Nuriddin, A.H.; Brantley, K.M.; Foreman, R.D.; Buckner, A.V. Post-disaster Gulf Coast recovery using telehealth. Telemed. J. E-Health 2013, 19, 200–210. [Google Scholar] [CrossRef]
- Nagata, T.; Halamka, J.; Himeno, S.; Himeno, A.; Kennochi, H.; Hashizume, M. Using a cloud-based electronic health record during disaster response: A case study in Fukushima, March 2011. Prehospital Disaster Med. 2013, 28, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Qadir, T.F.; Fatima, H.; Usmani, M.H.; Hussain, S.A. Telepsychiatry in Pakistan after natural disasters. Lancet Psychiatry 2016, 3, 1016. [Google Scholar] [CrossRef]
- Taylor, S.S.; Ehrenfeld, J.M. Electronic Health Records and Preparedness: Lessons from Hurricanes Katrina and Harvey. J. Med. Syst 2017, 41, 173. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stasiak, K.; Merry, S.N.; Frampton, C.; Moor, S. Delivering solid treatments on shaky ground: Feasibility study of an online therapy for child anxiety in the aftermath of a natural disaster. Psychother. Res. 2018, 28, 643–653. [Google Scholar] [CrossRef]
- French, D.M.; Hall, G.A.; McGeorge, T.; Haschker, M.; Brazeal, J.G.; Dubose-Morris, R. Hurricane Impact on Emergency Services and Use of Telehealth to Support Prehospital Care. Disaster Med. Public Health Prep. 2020, 14, 39–43. [Google Scholar] [CrossRef]
- Pasipanodya, E.C.; Shem, K. Provision of care through telemedicine during a natural disaster: A case study. Spinal Cord Ser. Cases 2020, 6, 60. [Google Scholar] [PubMed]
- Šago, D.; Martić, V.; Šmida, D.; Mayer, N.; Lovretić, V.; Filipčić, I. Telepsychiatry in the Time of the COVID-19 and Earthquake in Zagreb as Odysseus between Scylla and Charybdis. Psychiatr. Danub. 2020, 32, 478–481. [Google Scholar] [CrossRef]
- Paratz, E.D.; Mock, N.; Marques, D.; Wilson, W.; Kushwaha, V.; Eggleton, S.; Harries, J.; da Silva, S.; Dos Santos da Silva, A.; Saramento, J.; et al. Telemedicine to Timor-Leste: Implementing an international cardiac telehealth service during population dislocation, floods and COVID-19. Intern. Med. J. 2022, 52, 2076–2085. [Google Scholar] [CrossRef]
- Haklay, M.; Fraisl, D.; Greshake Tzovaras, B.; Hecker, S.; Gold, M.; Hager, G.; Ceccaroni, L.; Kieslinger, B.; Wehn, U.; Woods, S.; et al. Contours of citizen science: A vignette study. R. Soc. Open Sci. 2021, 8, 202108. [Google Scholar] [CrossRef]
- Heigl, F.; Kieslinger, B.; Paul, K.T.; Uhlik, J.; Dörler, D. Toward an international definition of citizen science. Proc. Natl. Acad. Sci. USA 2019, 116, 8089–8092. [Google Scholar] [CrossRef]
- Jørgensen, F.A.; Jørgensen, D. Citizen science for environmental citizenship. Conserv. Biol. 2021, 35, 1344–1347. [Google Scholar]
- Ceccaroni, L.; Woods, S.M.; Sprinks, J.; Wilson, S.; Faustman, E.M.; Bonn, A.; Greshake Tzovaras, B.; Subirats, L.; Kimura, A.H. Citizen Science, Health, and Environmental Justice. In The Science of Citizen Science; Vohland, K., Land-Zandstra, A., Ceccaroni, L., Lemmens, R., Perelló, J., Ponti, M., Samson, R., Wagenknecht, K., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 219–239. [Google Scholar]
- Fraisl, D.; Hager, G.; Bedessem, B.; Gold, M.; Hsing, P.-Y.; Danielsen, F.; Hitchcock, C.B.; Hulbert, J.M.; Piera, J.; Spiers, H.; et al. Citizen science in environmental and ecological sciences. Nat. Rev. Methods Prim. 2022, 2, 64. [Google Scholar]
- English, P.B.; Richardson, M.J.; Garzón-Galvis, C. From Crowdsourcing to Extreme Citizen Science: Participatory Research for Environmental Health. Annu. Rev. Public Health 2018, 39, 335–350. [Google Scholar] [CrossRef]
- Wiggins, A.; Wilbanks, J. The Rise of Citizen Science in Health and Biomedical Research. Am. J. Bioeth. 2019, 19, 3–14. [Google Scholar] [CrossRef]
- Colovic, A.; Caloffi, A.; Rossi, F. Crowdsourcing and COVID-19: How Public Administrations Mobilize Crowds to Find Solutions to Problems Posed by the Pandemic. Public Adm. Rev. 2022, 82, 756–763. [Google Scholar] [PubMed]
- Davis, S.; Button-Simons, K.; Bensellak, T.; Ahsen, E.M.; Checkley, L.; Foster, G.J.; Su, X.; Moussa, A.; Mapiye, D.; Khoo, S.K. Leveraging crowdsourcing to accelerate global health solutions. Nat. Biotechnol. 2019, 37, 848–850. [Google Scholar]
- Hislop, M. When the Floods Hit Lismore, Sally Flannery’s Team Coordination Efforts Saved Lives. Available online: https://womensagenda.com.au/latest/when-the-floods-hit-lismore-sally-flannerys-massive-coordination-efforts-saved-lives/ (accessed on 25 November 2022).
- Hicks, A.; Barclay, J.; Chilvers, J.; Armijos, M.T.; Oven, K.; Simmons, P.; Haklay, M. Global Mapping of Citizen Science Projects for Disaster Risk Reduction. Front. Earth Sci. 2019, 7, 226. [Google Scholar]
- Ludwig, T.; Siebigteroth, T.; Pipek, V. CrowdMonitor: Monitoring Physical and Digital Activities of Citizens During Emergencies. In Social Informatics; Aiello, L.M., McFarland, D., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 421–428. [Google Scholar]
- Kempf, H. Experience from large-scale crowdsourcing via weather apps. Australas. J. Disaster Trauma Stud. 2021, 25, 87–93. [Google Scholar]
- Blake, D.; Johnston, D.; Leonard, G.; McLaren, L.; Becker, J. A Citizen Science Initiative to Understand Community Response to the Kaikōura Earthquake and Tsunami Warning in Petone and Eastbourne, Wellington, Aotearoa/New ZealandA Citizen Science Initiative to Understand Community Response to the Kaikōura Earthquake. Bull. Seismol. Soc. Am. 2018, 108, 1807–1817. [Google Scholar] [CrossRef]
- Rodney, R.M.; Swaminathan, A.; Calear, A.L.; Christensen, B.K.; Lal, A.; Lane, J.; Leviston, Z.; Reynolds, J.; Trevenar, S.; Vardoulakis, S.; et al. Physical and Mental Health Effects of Bushfire and Smoke in the Australian Capital Territory 2019–20. Front. Public Health 2021, 9, 682402. [Google Scholar]
- Workman, A.; Jones, P.J.; Wheeler, A.J.; Campbell, S.L.; Williamson, G.J.; Lucani, C.; Bowman, D.M.J.S.; Cooling, N.; Johnston, F.H. Environmental Hazards and Behavior Change: User Perspectives on the Usability and Effectiveness of the AirRater Smartphone App. Int. J. Environ. Res. Public Health 2021, 18, 3591. [Google Scholar] [CrossRef] [PubMed]
- Ulpiani, G.; Hart, M.A.; Di Virgilio, G.; Maharaj, A.M.; Lipson, M.J.; Potgieter, J. A citizen centred urban network for weather and air quality in Australian schools. Sci. Data 2022, 9, 129. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, P.; Andamon, M.M.; Paolini, R. Investigating thermal comfort and energy impact through microclimate monitoring-a citizen science approach. Energy Build. 2020, 229, 110526. [Google Scholar] [CrossRef]
- Rieger, C.; Byrne, J.M. The Role of Citizen Science in Risk Mitigation and Disaster Response: A Case Study of 2015 Nepalese Earthquake Using OpenStreetMap. In Proceedings of the AGU Fall Meeting Abstracts, San Francisco, CA, USA; 2015; p. GC33A-1252. [Google Scholar]
- Calyx, C. Sustaining citizen science beyond an emergency. Sustainability 2020, 12, 4522. [Google Scholar] [CrossRef]
- Ottinger, G. Becoming Infrastructure: Integrating Citizen Science into Disaster Response and Prevention. Citiz. Sci. Theory Pract. 2022, 7, 15. [Google Scholar] [CrossRef]
- Calyx, C.; Finlay, S.M. Improving a framework for evaluating participatory science. Evaluation 2022, 28, 150–165. [Google Scholar] [CrossRef]
- Chari, R. Citizen Science for Disasters: A Guide for Community Groups. 2021. Available online: https://www.rand.org/pubs/tools/TLA175-2.html (accessed on 25 November 2022).
- World Health Organization. Operational Framework for Building Climate Resilient Health Systems; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization. WHO Guidance for Climate-Resilient and Environmentally Sustainable Health Care Facilities; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Safe Hospitals in Emergencies and Disasters: Structural, Non-Structural and Functional Indicators; WHO Regional Office for the Western Pacific: Manila, Philippines, 2010. [Google Scholar]
- Robin, M.; James, T. Chaos after Heat Crashes Computers at Leading London Hospitals. Guardian 2022. Available online: https://www.theguardian.com/environment/2022/aug/07/chaos-after-heat-crashes-computers-at-leading-london-hospitals#:~:text=Two%20of%20the%20UK’s%20leading,height%20of%20last%20month’s%20heatwave (accessed on 1 December 2022).
- Australian Medical Association Health Providers Impacted by Disasters Must Be Considered Essential Services. Available online: https://www.ama.com.au/ama-rounds/23-september-2022/articles/health-providers-impacted-disasters-must-be-considered (accessed on 1 December 2022).
- Digital Health Atlas. Available online: https://www.digitalhealthatlas.org/en/-/ (accessed on 1 December 2022).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lokmic-Tomkins, Z.; Bhandari, D.; Bain, C.; Borda, A.; Kariotis, T.C.; Reser, D. Lessons Learned from Natural Disasters around Digital Health Technologies and Delivering Quality Healthcare. Int. J. Environ. Res. Public Health 2023, 20, 4542. https://doi.org/10.3390/ijerph20054542
Lokmic-Tomkins Z, Bhandari D, Bain C, Borda A, Kariotis TC, Reser D. Lessons Learned from Natural Disasters around Digital Health Technologies and Delivering Quality Healthcare. International Journal of Environmental Research and Public Health. 2023; 20(5):4542. https://doi.org/10.3390/ijerph20054542
Chicago/Turabian StyleLokmic-Tomkins, Zerina, Dinesh Bhandari, Chris Bain, Ann Borda, Timothy Charles Kariotis, and David Reser. 2023. "Lessons Learned from Natural Disasters around Digital Health Technologies and Delivering Quality Healthcare" International Journal of Environmental Research and Public Health 20, no. 5: 4542. https://doi.org/10.3390/ijerph20054542
APA StyleLokmic-Tomkins, Z., Bhandari, D., Bain, C., Borda, A., Kariotis, T. C., & Reser, D. (2023). Lessons Learned from Natural Disasters around Digital Health Technologies and Delivering Quality Healthcare. International Journal of Environmental Research and Public Health, 20(5), 4542. https://doi.org/10.3390/ijerph20054542