
Autogenic Training in Mental Disorders: What Can We Expect?



Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Autonomic Dysfunction in Mental Disorders
3.2. The Psychophysiology of Autogenic Training
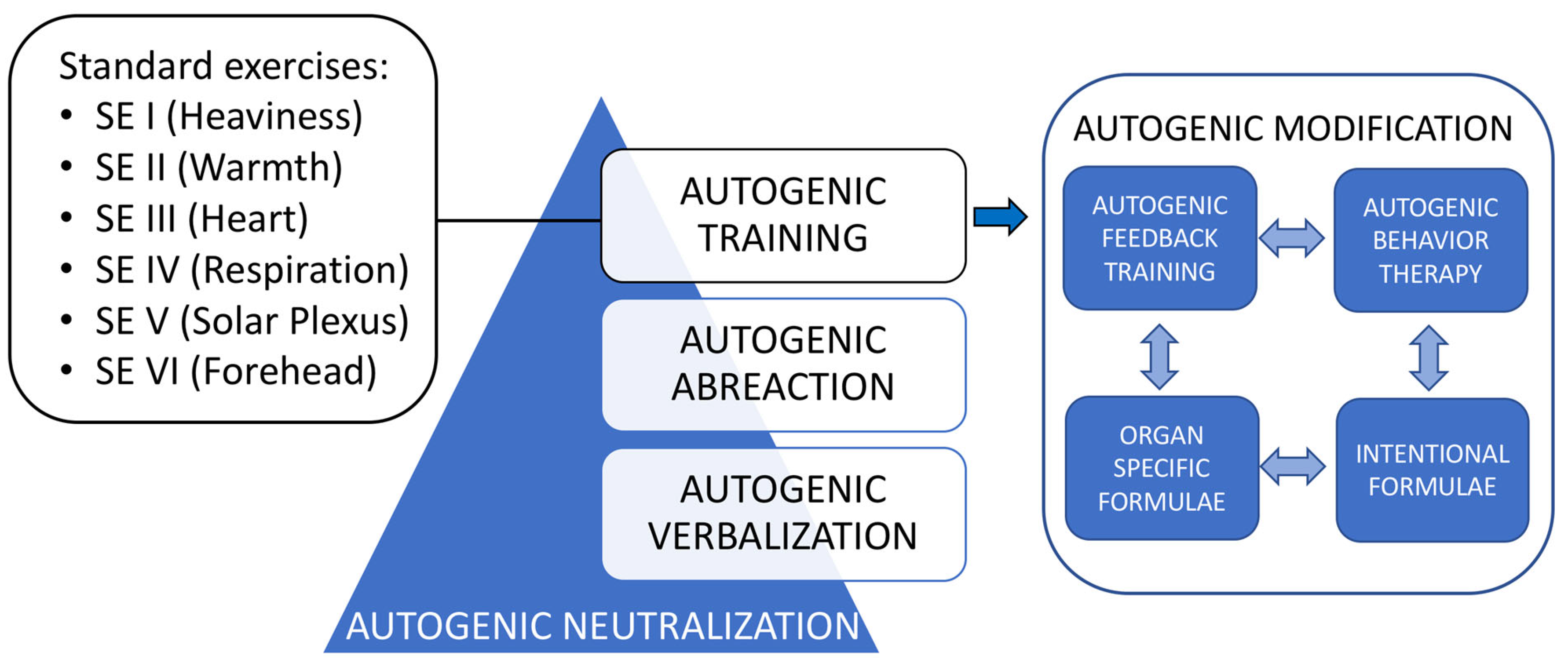
- Heaviness, warmth, breathing, personal formulae (modified Schultz technique);
- Heaviness, warmth, coolness, calmness, and peaceful relaxation (Luthe’s technique);
- Heaviness and warmth (Schultz and Luthe’s technique);
- Heaviness (Budzynski’s technique—taped);
- Heaviness, warmth, breathing patterns, neck and shoulders, mental picture of body alignment (Schultz technique);
- Heaviness and warmth (Luthe’s technique).
3.2.1. Effects of Autogenic Training on Autonomic Nervous System
3.2.2. Effects of Autogenic Training on Central Nervous System
3.2.3. Effects of Autogenic Training on Psychological Outputs
3.3. Clinical Evidence
3.3.1. Effects of Autogenic Training on Anxiety Disorders
3.3.2. Effects of Autogenic Training on Mood Disorders
3.3.3. Effects of Autogenic Training on Schizophrenia and Psychotic Disorders
3.3.4. Effects of Autogenic Training on Trauma- and Stressor-Related Disorders
3.3.5. Effects of Autogenic Training on Other Mental Disorders
4. Discussion
4.1. Clinical Gaps
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stetter, F.; Kupper, S. Autogenic training: A meta-analysis of clinical outcome studies. Appl. Psychophysiol. Biofeedback 2002, 27, 45–98. [Google Scholar] [CrossRef] [PubMed]
- Schultz, J.H. Das Autogene Training (Konzentrative Selbstentspannung); Georg Thieme Verlag Leipzig: Leipzig, Germany, 1932; p. 305. [Google Scholar]
- Litwic-Kaminska, K.; Kotyśko, M.; Pracki, T.; Wiłkość-Dębczyńska, M.; Stankiewicz, B. The Effect of Autogenic Training in a Form of Audio Recording on Sleep Quality and Physiological Stress Reactions of University Athletes-Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 16043. [Google Scholar] [CrossRef] [PubMed]
- Luthe, W.; Schultz, J.H. Autogenic Therapy: Medical Applications; Grune and Stratton: New York, NY, USA, 1970. [Google Scholar]
- Luthe, W. About the Methods of Autogenic Therapy. In Mind/Body Integration; Peper, E., Ancoli, S., Quinn, M., Eds.; Springer: Boston, MA, USA, 1979. [Google Scholar]
- Luthe, W. The dream formula. In Autogenic Methods; Luthe, W., Antonelli, F., Eds.; Edizioni Luigi Pozzi: Rome, Italy, 1977. [Google Scholar]
- Kanji, N. Autogenic training. Complement. Ther. Med. 1997, 5, 162–167. [Google Scholar] [CrossRef]
- Caponnetto, P.; Magro, R.; Inguscio, L.; Cannella, M.C. Quality of life, work motivation, burn-out and stress perceptions benefits of a stress management program by autogenic training for emergency room staff: A pilot study. Ment. Illnes 2018, 10, 7913. [Google Scholar] [CrossRef]
- Kohlert, A.; Wick, K.; Rosendahl, J. Autogenic Training for Reducing Chronic Pain: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Int. J. Behav. Med. 2022, 29, 531–542. [Google Scholar] [CrossRef]
- Awad, M.A.; Hasanin, M.E.; Taha, M.M.; Gabr, A.A. Effect of stretching exercises versus autogenic training on preeclampsia. J. Exerc. Rehabil. 2019, 15, 109–113. [Google Scholar] [CrossRef]
- Ozamiz-Etxebarria, N.; Santa María, M.D.; Munitis, A.E.; Gorrotxategi, M.P. Reduction of COVID-19 Anxiety Levels Through Relaxation Techniques: A Study Carried Out in Northern Spain on a Sample of Young University Students. Front. Psychol. 2020, 11, 2038. [Google Scholar] [CrossRef]
- de Rivera, L.; Ozamiz-Etxebarria, N.; Dosil-Santamaría, M.; de Rivera-Monterrey, L. Autogenic Training Improves the Subjective Perception of Physical and Psychological Health and of Interpersonal Relational Abilities: An Electronic Field Survey During the COVID-19 Crisis in Spain. Front. Psychol. 2021, 12, 616426. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Ramirez-Garcia, M.P.; Leclerc-Loiselle, J.; Genest, C.; Lussier, R.; Dehghan, G. Effectiveness of autogenic training on psychological well-being and quality of life in adults living with chronic physical health problems: A protocol for a systematic review of RCT. Syst. Rev. 2020, 9, 74. [Google Scholar] [CrossRef]
- Seo, E.; Kim, S. Effect of Autogenic Training for Stress Response: A Systematic Review and Meta-Analysis. J. Korean Acad. Nurs. 2019, 49, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Aivazyan, T.A.; Zaitsev, V.P. The effectiveness of autogenic training in the psycho-corrective treatment of the patients presenting with chronic somatic diseases. Vopr. Kurortol. Fizioter. I Lech. Fiz. Kult. 2018, 95, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Bowden, A.; Lorenc, A.; Robinson, N. Autogenic Training as a behavioural approach to insomnia: A prospective cohort study. Prim. Health Care Res. Dev. 2012, 13, 175–185. [Google Scholar] [CrossRef]
- Yurdakul, L.; Holttum, S.; Bowden, A. Perceived changes associated with autogenic training for anxiety: A grounded theory study. Psychol. Psychother. 2009, 82 Pt 4, 403–419. [Google Scholar] [CrossRef]
- Manzoni, G.M.; Pagnini, F.; Castelnuovo, G.; Molinari, E. Relaxation training for anxiety: A ten-years systematic review with meta-analysis. BMC Psychiatry 2008, 8, 41. [Google Scholar] [CrossRef]
- Kircher, T.; Teutsch, E.; Wormstall, H.; Buchkremer, G.; Thimm, E. Effects of autogenic training in elderly patients. Z. Gerontol. Geriatr. 2002, 35, 157–165. [Google Scholar] [CrossRef]
- Ernst, E.; Kanji, N. Autogenic training for stress and anxiety: A systematic review. Complement. Ther. Med. 2000, 8, 106–110. [Google Scholar] [CrossRef]
- Sakai, M. Application of autogenic training for anxiety disorders: A clinical study in a psychiatric setting. Fukuoka Igaku Zasshi = Hukuoka Acta Med. 1997, 88, 56–64. [Google Scholar]
- Feruglio, S.; Pascut, S.; Matiz, A.; Paschetto, A.; Crescentini, C. Effects of Mind-Body Interventions on Adolescents’ Cooperativeness and Emotional Symptoms. Behav. Sci. 2022, 12, 33. [Google Scholar] [CrossRef] [PubMed]
- Rucka, K.; Talarowska, M. The Impact of One-Time Relaxation Training on Attention Efficiency Measured by Continuous Performance Test in Depressive Disorders. Int. J. Environ. Res. Public Health 2022, 19, 6473. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Garcia, M.P.; Leclerc-Loiselle, J.; Gagnon, M.P.; Côté, J.; Brouillette, M.J.; Thomas, R. A mixed-method randomized feasibility trial evaluating progressive muscle relaxation or autogenic training on depressive symptoms and quality of life in people living with human immunodeficiency virus (HIV) who have depressive symptoms. J. Complement. Integr. Med. 2020, 18, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Goto, F.; Nakai, K.; Murakami, M.; Ogawa, K. Intractable depression successfully treated with a combination of autogenic training and high-dose antidepressant in department of otorhinolaryngology: A case report. Cases J. 2009, 2, 6908. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A.F.; Morgan, A.J.; Hetrick, S.E. Relaxation for depression. Cochrane Database Syst. Rev. 2008, 4, Cd007142. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.J.; Jorm, A.F. Self-help interventions for depressive disorders and depressive symptoms: A systematic review. Ann. Gen. Psychiatry 2008, 7, 13. [Google Scholar] [CrossRef]
- Kircher, T.; Stetter, F.; Wormstall, H. Use of supportive autogenic training in multiple morbidity in geriatric psychiatry patients. Z. Gerontol. Geriatr. 1997, 30, 348–353. [Google Scholar]
- Motoda, K.; Shibata, J.I.; Inanaga, K.; Isozaki, H. Visual evoked responses in schizophrenics during autogenic training. Am. J. Clin. Hypn. 1969, 12, 67–74. [Google Scholar] [CrossRef]
- Shibata, J.I. Limits of Application of Autogenic Training to Schizophrenia and Selection of the Patients. Am. J. Clin. Hypn. 1968, 11, 99–100. [Google Scholar] [CrossRef]
- Shibata, J.I.; Motoda, K. The Application of Autogenic Training to a Group of Schizophrenic Patients. Am. J. Clin. Hypn. 1967, 10, 15–19. [Google Scholar] [CrossRef]
- Louvardi, M.; Chrousos, G.P.; Darviri, C. The Effect of Stress Management Techniques on Persons with Addictive Behaviors: A Systematic Review. Mater. Socio-Med. 2021, 33, 213–218. [Google Scholar] [CrossRef]
- Gordon, J.S.; Staples, J.K.; Blyta, A.; Bytyqi, M.; Wilson, A.T. Treatment of posttraumatic stress disorder in postwar Kosovar adolescents using mind-body skills groups: A randomized controlled trial. J. Clin. Psychiatry 2008, 69, 1469–1476. [Google Scholar] [CrossRef]
- Mitani, S.; Fujita, M.; Sakamoto, S.; Shirakawa, T. Effect of autogenic training on cardiac autonomic nervous activity in high-risk fire service workers for posttraumatic stress disorder. J. Psychosom. Res. 2006, 60, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Jojic, B.R.; Leposavic, L.M. Autogenic training as a therapy for adjustment disorder in adolescents. Srp. Arh. Celok. Lek. 2005, 133, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Jojic, B.R.; Leposavic, L.M. Autogenic training as a therapy for adjustment disorder in adults. Srp. Arh. Celok. Lek. 2005, 133, 505–509. [Google Scholar] [CrossRef]
- Stanton, A.M.; Hixon, J.G.; Nichols, L.M.; Meston, C.M. One Session of Autogenic Training Increases Acute Subjective Sexual Arousal in Premenopausal Women Reporting Sexual Arousal Problems. J. Sex. Med. 2018, 15, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Arango, C.; Dragioti, E.; Solmi, M.; Cortese, S.; Domschke, K.; Murray, R.M.; Jones, P.B.; Uher, R.; Carvalho, A.F.; Reichenberg, A.; et al. Risk and protective factors for mental disorders beyond genetics: An evidence-based atlas. World Psychiatry Off. J. World Psychiatr. Assoc. 2021, 20, 417–436. [Google Scholar] [CrossRef] [PubMed]
- Alvares, G.A.; Quintana, D.S.; Hickie, I.B.; Guastella, A.J. Autonomic nervous system dysfunction in psychiatric disorders and the impact of psychotropic medications: A systematic review and meta-analysis. J. Psychiatry Neurosci. 2016, 41, 89–104. [Google Scholar] [CrossRef]
- Schiweck, C.; Piette, D.; Berckmans, D.; Claes, S.; Vrieze, E. Heart rate and high frequency heart rate variability during stress as biomarker for clinical depression. A systematic review. Psychol. Med. 2019, 49, 200–211. [Google Scholar] [CrossRef]
- Faurholt-Jepsen, M.; Kessing, L.V.; Munkholm, K. Heart rate variability in bipolar disorder: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2017, 73, 68–80. [Google Scholar] [CrossRef]
- Miu, A.C.; Heilman, R.M.; Miclea, M. Reduced heart rate variability and vagal tone in anxiety: Trait versus state, and the effects of autogenic training. Auton. Neurosci. Basic Clin. 2009, 145, 99–103. [Google Scholar] [CrossRef]
- de Faria Cardoso, C.; Ohe, N.T.; Bader, Y.; Afify, N.; Al-Homedi, Z.; Alwedami, S.M.; O’Sullivan, S.; Campos, L.A.; Baltatu, O.C. Heart Rate Variability Indices as Possible Biomarkers for the Severity of Post-traumatic Stress Disorder Following Pregnancy Loss. Front. Psychiatry 2021, 12, 700920. [Google Scholar] [CrossRef]
- Sandhya, M.; Mittal, S.; Kathrotia, R.; Rawat, V.S.; Singh, Y.; Srikant, S.; Agrawal, M.; Mohan, L. Cardiovascular Autonomic Function Tests in Patients of Obsessive-Compulsive Disorder: A Cross-Sectional Study. Indian J. Psychol. Med. 2022, 44, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Licht, C.M.; de Geus, E.J.; van Dyck, R.; Penninx, B.W. Association between anxiety disorders and heart rate variability in The Netherlands Study of Depression and Anxiety (NESDA). Psychosom. Med. 2009, 71, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Kemp, A.H.; Quintana, D.S.; Gray, M.A.; Felmingham, K.L.; Brown, K.; Gatt, J.M. Impact of depression and antidepressant treatment on heart rate variability: A review and meta-analysis. Biol. Psychiatry 2010, 67, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.Y.; Barr, A.M.; Procyshyn, R.M.; Honer, W.G.; Pang, C.C. Cardiovascular side-effects of antipsychotic drugs: The role of the autonomic nervous system. Pharmacol. Ther. 2012, 135, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Licht, C.M.; de Geus, E.J.; van Dyck, R.; Penninx, B.W. Longitudinal evidence for unfavorable effects of antidepressants on heart rate variability. Biol. Psychiatry 2010, 68, 861–868. [Google Scholar] [CrossRef]
- Schultz, J.H.; Luthe, W. Autogenic Therapy Volume 1 Autogenic Methods, 1st ed.; Grune & Stratton, Inc.: New York, NY, USA, 1969. [Google Scholar]
- Hall, J.E.; Hall, M.E. Guyton and Hall Textbook of Medical Physiology, 14th ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Zaccaro, A.; Piarulli, A.; Laurino, M.; Garbella, E.; Menicucci, D.; Neri, B.; Gemignani, A. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Front. Hum. Neurosci. 2018, 12, 353. [Google Scholar] [CrossRef]
- Park, Y.J.; Park, Y.B. Clinical utility of paced breathing as a concentration meditation practice. Complement. Ther. Med. 2012, 20, 393–399. [Google Scholar] [CrossRef]
- Luthe, W.; Schultz, J.H. Autogenic Therapy, Volume 1: Autogenic Methods; Original work published 1969; British Autogenic Society: London, UK, 2001. [Google Scholar]
- Teasdale, J.D.; Barnard, P.J. Affect, Cognition and Change: Re-Modelling Depressive Thought; Lawrence Erlbaum Associates: Hove, UK, 1993. [Google Scholar]
- Teasdale, J.D. The transformation of meaning: The interacting cognitive subsystems approach. In The Transformation of Meaning in Psychological Therapies: Integrating Theory and Practice; Power, M., Brewin, C., Eds.; Wiley: Chichester, UK, 1997. [Google Scholar]
- Teasdale, J.D. Metacognition, mindfulness and the modification of mood disorders. Clin. Psychol. Psychother. 1999, 6, 146–155. [Google Scholar] [CrossRef]
- Wells, A.; King, P. Metacognitive therapy for generalized anxiety disorder: An open trial. J. Behav. Ther. Exp. Psychiatry 2006, 37, 206–212. [Google Scholar] [CrossRef]
- Farne, M.A.; Jimenez-Munoz, N. Personality changes induced by autogenic training practice. Stress Med. 2000, 16, 263–268. [Google Scholar] [CrossRef]
- Helgason, C.; Sarris, J. Mind-body medicine for schizophrenia and psychotic disorders: A review of the evidence. Clin. Schizophr. Relat. Psychoses 2013, 7, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Rudisch, B.; Nemeroff, C.B. Epidemiology of comorbid coronary artery disease and depression. Biol. Psychiatry 2003, 54, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Taylor, V.; McKinnon, M.C.; Macdonald, K.; Jaswal, G.; Macqueen, G.M. Adults with mood disorders have an increased risk profile for cardiovascular disease within the first 2 years of treatment. Can. J. Psychiatry. Rev. Can. Psychiatr. 2010, 55, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Rosengren, A.; Hawken, S.; Ounpuu, S.; Sliwa, K.; Zubaid, M.; Almahmeed, W.A.; Blackett, K.N.; Sitthi-amorn, C.; Sato, H.; Yusuf, S. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 953–962. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Lawrence, D. Revascularisation and mortality rates following acute coronary syndromes in people with severe mental illness: Comparative meta-analysis. Br. J. Psychiatry J. Ment. Sci. 2011, 198, 434–441. [Google Scholar] [CrossRef]
- Chauvet-Gelinier, J.C.; Trojak, B.; Verges-Patois, B.; Cottin, Y.; Bonin, B. Review on depression and coronary heart disease. Arch. Cardiovasc. Dis. 2013, 106, 103–110. [Google Scholar] [CrossRef]
- Clamor, A.; Lincoln, T.M.; Thayer, J.F.; Koenig, J. Resting vagal activity in schizophrenia: Meta-analysis of heart rate variability as a potential endophenotype. Br. J. Psychiatry J. Ment. Sci. 2016, 208, 9–16. [Google Scholar] [CrossRef]
- Weber, C.S.; Thayer, J.F.; Rudat, M.; Wirtz, P.H.; Zimmermann-Viehoff, F.; Thomas, A.; Perschel, F.H.; Arck, P.C.; Deter, H.C. Low vagal tone is associated with impaired post stress recovery of cardiovascular, endocrine, and immune markers. Eur. J. Appl. Physiol. 2010, 109, 201–211. [Google Scholar] [CrossRef]
- Sgoifo, A.; Carnevali, L.; Alfonso Mde, L.; Amore, M. Autonomic dysfunction and heart rate variability in depression. Stress 2015, 18, 343–352. [Google Scholar] [CrossRef]


{kind=link}
| Reported Study | Number of Studies | Number of Participants | Outcomes | Results |
|---|---|---|---|---|
| Anxiety disorders | ||||
| de Rivera et al., 2021 [12] | 1 | 75 | The effectiveness of autogenic training (AT) | There was an increase in the practice of AT during the COVID-19 pandemic. Autogenic training was very useful for physical and psychological health and for a better understanding of others. |
| Ramirez-Garcia et al., 2020 [14] | A protocol for a systematic review | Randomized controlled trials to be identified | The efficacy of AT on psychological wellbeing (anxiety, distress, depression) in people with chronic physical health problems | Pending results. |
| Ozamiz-Etxebarria et al., 2020 [11] | 1 | 44 | Generalized anxiety disorder-7 (GAD-7) scale | Jacobson’s progressive relaxation techniques, Schultz’s AT, abdominal relaxations, and visualizations were effective in lowering the COVID-19 anxiety levels of university students as an alternative to pharmacotherapy. |
| Seo and Kim, 2019 [15] | Systematic review: 21 meta-analysis: 11 | 85–327 | Anxiety score | Autogenic training decreased anxiety score. |
| Aivazyan and Zaitsev, 2018 [16] | 1 | 325 | The effectiveness of AT | Autogenic training reduced anxiety, tension, negative feelings, stress sensitivity, and improved mood and activity levels in patients affected by chronic somatic diseases. |
| Bowden et al., 2012 [17] | 1 | 153 | “Measure Yourself Medical Outcome Profile” and hospital anxiety and depression scale | Autogenic training reduced anxiety. |
| Yurdakul et al., 2009 [18] | 1 | 12 | Autogenic training experience in anxiety | The cognitive changes reported have implications for anxiety treatments. |
| Manzoni et al., 2008 [19] | 27 | 1014 | Anxiety, psychometric questionnaires | There was consistent and significant efficacy of relaxation training in reducing anxiety. |
| Kircher et al., 2002 [20] | 1 | 16 | Effectiveness of the AT in cognitively impaired, frail elderly | Mentally impaired, frail elderly participants were able to learn the AT. Cognitive impairment was disadvantageous for successful participation. |
| Stetter and Kupper, 2002 [1] | 60 | >1500 | Anxiety | Medium range positive effects of AT were found for anxiety disorders. |
| Ernst and Kanji, 2000 [21] | 8 | 245 | Anxiety, Spielberger’s state–Trait anxiety inventory | Autogenic training reduced stress and anxiety. |
| Sakai, 1997 [22] | 1 | 55 | The impact of AT on anxiety disorders | Twenty-eight patients with anxiety disorders (51%) were cured, fourteen (25%) much improved, eight (15%) improved, and five (9%) unchanged at the end of the treatment. Forty-two patients (76%) were assessed as having had successful treatment. |
| Mood disorders | ||||
| Feruglio et al., 2022 [23] | 1 | 72 | Cooperativeness and emotional symptoms (self-reported temperament and character inventory; strengths and difficulties questionnaire for adolescents) | Both mindfulness-oriented meditation training and AT enhanced a cooperative attitude in adolescents and helped reduce their emotional problems. |
| Rucka and Talarowska, 2022 [24] | 1 | 42 | Attention efficiency determined by the perceptual speed index measured using the attention and perceptiveness test | A 15-min-long, one-time AT session improved the efficiency of attention and perceptiveness in people with depression. |
| Ramirez-Garcia et al., 2020 [25] | 1 | 42 | Emotion management, depressive symptoms, and quality of life | Adults living with human immunodeficiency virus reported better emotion management and improvements in depressive symptoms and quality of life following the AT intervention. |
| Seo and Kim, 2019 [15] | systematic review: 21 meta-analysis: 11 | 85–327 | Depression score | Autogenic training decreased depression score. |
| Bowden et al., 2012 [17] | 1 | 153 | “Measure Your Medical Outcome Profile” and hospital anxiety and depression scale | Autogenic training reduced depression. |
| Goto et al., 2009 [26] | 1 | 1 | Self-rating depression scale, manifested anxiety scale | Depressive state was markedly alleviated following the AT. |
| Jorm et al., 2008 [27] | systematic review: 15 meta-analysis: 11 | 48–286 | Depressive symptoms | Relaxation techniques (including the AT) were more effective at reducing self-rated depressive symptoms than no or minimal treatment. |
| Morgan and Jorm, 2008 [28] | 2 | 189 | Depressive symptoms | Depression symptoms in the AT group improved significantly more than in the control group, but significantly less than in the psychotherapy group. |
| Stetter and Kupper, 2002 [1] | 60 | >1500 | Depression/dysthymia | Medium range positive effects of AT were found for mild-to-moderate depression/dysthymia. |
| Kircher et al., 1997 [29] | 1 | 23 | Psychopathological status: brief psychiatric rating scale, geriatric depression scale, the cognitive state (a mini-mental state examination) | Autogenic training was a useful component in psychotherapeutic and psychiatric therapy for elderly multimorbid in- and outpatients. |
| Schizophrenia and psychotic disorders | ||||
| Motoda et al., 1969 [30] | 1 | 30 | Visually evoked responses | Recordings of electrical signals generated by the visual cortex in response to visual stimulation suggest the brain activity in schizophrenia may be stabilized by practicing AT. |
| Shibata, 1968 [31] | 1 | 1 | Limits of AT application to schizophrenia | The limits of AT application depend on the selection of schizophrenic patients. The patients in remission should be selected for AT. |
| Shibata and Motoda, 1967 [32] | 1 | 65 | Rehabilitation effects of AT on schizophrenic convalescent patients | All study participants progressed favorably during the SE. After proceeding on to meditation exercises, symptoms aggravated in several patients. |
| Trauma- and stressor-related disorders | ||||
| Louvardi et al., 2021 [33] | 4 | 188 | The effect of stress management on stress levels measured using instruments or biochemical assessments | Progressive muscle relaxation might lead to a reduction of stress levels in persons with addictive behaviors, while no such evidence was found concerning guided imagery and AT. |
| Gordon et al., 2008 [34] | 1 | 82 | Posttraumatic stress disorder (PTSD) symptom scores (Harvard trauma questionnaire) | Postwar Kosovar adolescents with PTSD undergoing AT experienced a significant decrease in PTSD symptom scores that was maintained at 3-month follow-up. |
| Mitani et al., 2006 [35] | 1 | 22 | PTSD signs and symptoms (cardiac sympathetic and parasympathetic nervous activity, impact of event scale—revised questionnaire) | Autogenic training ameliorated disturbances in cardiac autonomic nervous activity and improved self-reported psychological dysfunction secondary to PTSD (intrusion, avoidance, hyperarousal) in fire service workers with PTSD. |
| Jojic and Leposavic, 2005 [36] | 1 | 31 | Adjustment disorder indicators (arterial blood pressure, pulse rate, concentration of cholesterol and cortisol) | Autogenic training significantly decreased the values of physiological indicators of adjustment disorder and diminished the effects of stress in adolescents with adjustment disorder. |
| Jojic and Leposavic, 2005 [37] | 1 | 35 | Adjustment disorder indicators (arterial blood pressure, pulse rate, concentration of cholesterol and cortisol) | Autogenic training significantly decreased the values of physiological indicators of adjustment disorder and diminished the effects of stress in adults with adjustment disorder. |
| Other mental disorders | ||||
| Litwic-Kaminska et al., 2022 [3] | 1 | 22 | Sleep quality (the Pittsburg sleep quality index), physiological stress reactions | Sleep quality significantly increased after two-week AT usage in experimental group. |
| Stanton et al., 2018 [38] | 1 | 25 | Genital sexual arousal, subjective sexual arousal, and perceived genital sensations | Autogenic training significantly improved acute subjective arousal and increased perceived genital sensations in premenopausal women with self-reported arousal concerns. |
| Bowden et al., 2012 [17] | 1 | 153 | Sleep questionnaires | Autogenic training improved sleep patterns. |
| Stetter and Kupper, 2002 [1] | 60 | >1500 | Functional sleep disorders | Medium range positive effects of AT were found for functional sleep disorders. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Breznoscakova, D.; Kovanicova, M.; Sedlakova, E.; Pallayova, M. Autogenic Training in Mental Disorders: What Can We Expect? Int. J. Environ. Res. Public Health 2023, 20, 4344. https://doi.org/10.3390/ijerph20054344
Breznoscakova D, Kovanicova M, Sedlakova E, Pallayova M. Autogenic Training in Mental Disorders: What Can We Expect? International Journal of Environmental Research and Public Health. 2023; 20(5):4344. https://doi.org/10.3390/ijerph20054344
Chicago/Turabian StyleBreznoscakova, Dagmar, Milana Kovanicova, Eva Sedlakova, and Maria Pallayova. 2023. "Autogenic Training in Mental Disorders: What Can We Expect?" International Journal of Environmental Research and Public Health 20, no. 5: 4344. https://doi.org/10.3390/ijerph20054344
APA StyleBreznoscakova, D., Kovanicova, M., Sedlakova, E., & Pallayova, M. (2023). Autogenic Training in Mental Disorders: What Can We Expect? International Journal of Environmental Research and Public Health, 20(5), 4344. https://doi.org/10.3390/ijerph20054344