


Healthy City Community Space-Oriented Structural Planning and Management Optimization under COVID-19



Abstract
1. Introduction
2. Methods
2.1. Theoretical Sources of Healthy and Smart Cities
2.2. Using Particle Swarm Optimization (PSO) to Evaluate Residents’ Health Status and Infectious Risk in a Healthy City
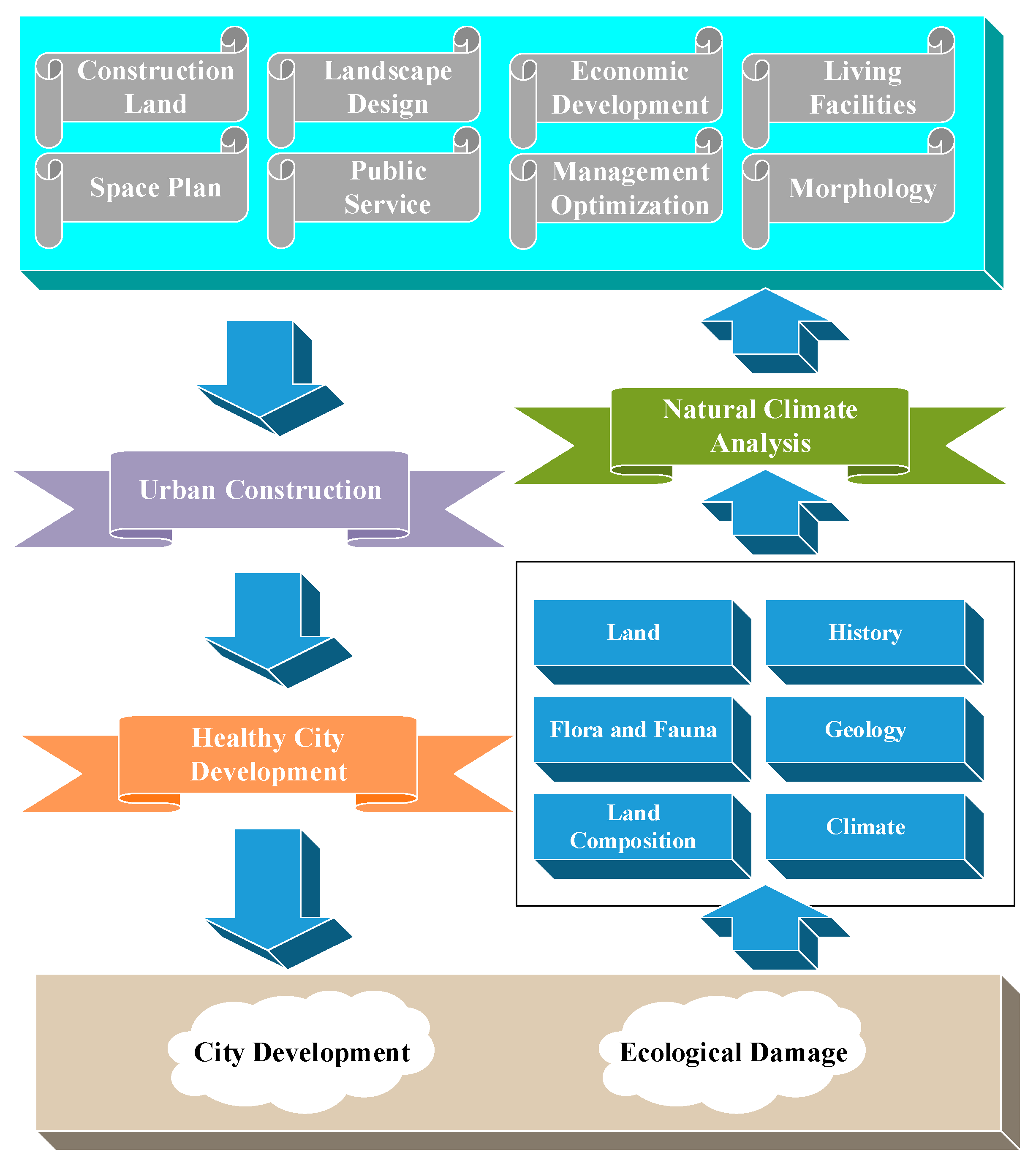
2.3. Community Space Structure Planning for Healthy Cities
- Rational organization of urban road traffic. In particular, the division of arterial roads is often the main factor determining the scale of residential land.
- The radius of public facilities for residents living services. Reasonable facility scale (i.e., the economy of operation and management) and service radius (i.e., the walking distance of residents using public buildings) affect the convenience and safety of residents’ lives.
- A unified urban administrative management system. As the basic cell of society, the family is bound to be linked with the administrative organization of society.
- Terrain. The organizational form of residential areas is affected and restricted by topography to a certain extent. It is generally difficult to compactly arrange residential land on undulating terrain [21].
2.4. Reliability and Validity Analysis
2.5. Questionnaire Design of Investigating Healthy City Resident’s Health Status and Public Services
3. Results
3.1. Analysis of the Daily Living Ability of Patients with Respiratory Diseases
3.2. Community Health Services Coverage among Healthy Cities’ Residents
4. Discussion
- The provision of community health and medical personnel should be accelerated. Community health medical personnel are the foundation of the development of community health services. Without excellent personnel, there will be no quality service. General practice and community nursing programs can be established in medical colleges and universities to specifically train professionals suitable for community health [27].
- A sound community health electronic information platform needs to be established. The informatization of community health service has played an important role in promoting the development and mode transformation of community health.
- The income of employees should be increased, and a scientific performance appraisal system should be implemented. While implementing two lines of revenue and expenditure, a positive and effective performance appraisal system should be adopted. Otherwise, the efficiency of community health services will be inevitably affected [28].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ardabili, S.F.; Mosavi, A.; Ghamisi, P.; Ferdinand, F.; Varkonyi-Koczy, A.R.; Reuter, U.; Rabczuk, T.; Atkinson, P.M. COVID-19 outbreak prediction with machine learning. Algorithms 2020, 13, 249. [Google Scholar] [CrossRef]
- Gkiotsalitis, K.; Cats, O. Public transport planning adaption under the COVID-19 pandemic crisis: Literature review of research needs and directions. Transp. Rev. 2021, 41, 374–392. [Google Scholar] [CrossRef]
- Costa, D.G.; Peixoto, J.P.J. COVID-19 pandemic: A review of smart cities initiatives to face new outbreaks. IET Smart Cities 2020, 2, 64–73. [Google Scholar] [CrossRef]
- Louro, A.; Marques da Costa, N.; Marques da Costa, E. Sustainable urban mobility policies as a path to healthy cities—The case study of LMA, Portugal. Sustainability 2019, 11, 2929. [Google Scholar] [CrossRef]
- Yang, J.; Luo, X.; Xiao, Y.; Shen, S.; Su, M.; Bai, Y.; Gong, P. Comparing the Use of Spatially Explicit Indicators and Conventional Indicators in the Evaluation of Healthy Cities: A Case Study in Shenzhen, China. Int. J. Environ. Res. Public Health 2020, 17, 7409. [Google Scholar] [CrossRef]
- Singh, A.K.; Misra, A. Herd mentality, herds of migrants/people, and COVID-19 in India. Diabetes Metab. Syndr. 2020, 14, 497. [Google Scholar] [CrossRef]
- Leporelli, E.; Santi, G. From psychology of sustainability to sustainability of urban spaces: Promoting a primary prevention approach for well-being in the healthy city designing. A waterfront case study in livorno. Sustainability 2019, 11, 760. [Google Scholar] [CrossRef]
- De Jong, M.A.; Wagemakers, A.; Koelen, M.A. “We Don’t Assume That Everyone Has the Same Idea About Health, Do We?” Explorative Study of Citizens’ Perceptions of Health and Participation to Improve Their Health in a Low Socioeconomic City District. Int. J. Environ. Res. Public Health 2020, 17, 4958. [Google Scholar] [CrossRef]
- Vujcic, M.; Tomicevic-Dubljevic, J.; Zivojinovic, I.; Toskovic, O. Connection between urban green areas and visitors’ physical and mental well-being. Urban For. Urban Green. 2019, 40, 299–307. [Google Scholar] [CrossRef]
- Sun, M.; Zhang, J. Research on the application of block chain big data platform in the construction of new smart city for low carbon emission and green environment. Comput. Commun. 2020, 149, 332–342. [Google Scholar] [CrossRef]
- Ghosh, S. Smart homes: Architectural and engineering design imperatives for smart city building codes. In Proceedings of the 2018 Technologies for Smart-City Energy Security and Power (ICSESP), Bhubaneswar, India, 28–30 March 2018; pp. 1–4. [Google Scholar] [CrossRef]
- Camero, A.; Alba, E. Smart City and information technology: A review. Cities 2019, 93, 84–94. [Google Scholar] [CrossRef]
- Pozoukidou, G.; Chatziyiannaki, Z. 15-Minute City: Decomposing the new urban planning eutopia. Sustainability 2021, 13, 928. [Google Scholar] [CrossRef]
- Zeng, C.; Huang, Y.; Yu, L.; Zeng, Q.; Wang, B.; Xu, Y. Long-Term Assessment of Rehabilitation Treatment of Sports through Artificial Intelligence Research. Comput. Math. Methods Med. 2021, 2021, 4980718. [Google Scholar] [CrossRef] [PubMed]
- Zeyu, W.; Jia, L.; Mingyu, L.; Siting, Y.; Yutong, W.; Xin, C. Edge Computing and Blockchain in Enterprise Performance and Venture Capital Management. Comput. Intell. Neurosci. 2022, 2022, 2914936. [Google Scholar] [CrossRef]
- Saini, J.; Dutta, M.; Marques, G. Fuzzy inference system tree with particle swarm optimization and genetic algorithm: A novel approach for PM10 forecasting. Expert Syst. Appl. 2021, 183, 115376. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Dobrzański, L.B. Effect of Biomedical Materials in the implementation of a long and healthy life policy. Processes 2021, 9, 865. [Google Scholar] [CrossRef]
- Zeyu, W.; Yue, D.; Shouan, Z.; Zhongbang, W. Achieving sustainable development goal 9: A study of enterprise resource optimization based on artificial intelligence algorithms. Resour. Policy 2022, 80, 103212. [Google Scholar] [CrossRef]
- Lee, M.; Park, S.; Yoon, K. Does Health Promotion Program Affect Local Resident’ Emotions? Int. J. Environ. Res. Public Health 2019, 16, 549. [Google Scholar] [CrossRef]
- Zeyu, W.; Shuting, Z.; Yuanyuan, Z.; Chuan, C.; Xiufang, D. Risk prediction and credibility detection of network public opinion using blockchain technology. Technol. Forecast. Soc. Chang. 2022, 187, 122177. [Google Scholar] [CrossRef]
- Guo, A.; Yang, J.; Xiao, X.; Xia, J.; Jin, C.; Li, X. Influences of urban spatial form on urban heat island effects at the community level in China. Sustain. Cities Soc. 2020, 53, 101972. [Google Scholar] [CrossRef]
- Bibri, S.E.; Krogstie, J.; Kärrholm, M. Compact city planning and development: Emerging practices and strategies for achieving the goals of sustainability. Dev. Built Environ. 2020, 4, 100021. [Google Scholar] [CrossRef]
- Vieira, J.; Matos, P.; Mexia, T.; Silva, P.; Lopes, N.; Freitas, C.; Correia, O.; Santos-Reis, M.; Branquinho, C.; Pinho, P. Green spaces are not all the same for the provision of air purification and climate regulation services: The case of urban parks. Environ. Res. 2018, 160, 306–313. [Google Scholar] [CrossRef]
- Blay-Palmer, A.; Santini, G.; Dubbeling, M.; Renting, H.; Taguchi, M.; Giordano, T. Validating the city region food system approach: Enacting inclusive, transformational city region food systems. Sustainability 2018, 10, 1680. [Google Scholar] [CrossRef]
- Chetwynd, E. Critical Analysis of Reliability and Validity in Literature Reviews. J. Hum. Lact. 2022, 38, 392–396. [Google Scholar] [CrossRef]
- Wang, S.; Gao, R.C.; Li, R.; Wu, G.C. Psychological status and correlated factors of primary medical staff during the COVID-19 outbreak in Hefei City, China. J. Multidiscip. Healthc. 2021, 14, 751. [Google Scholar] [CrossRef]
- Perry, H.B.; Hodgins, S. Health for the people: Past, current, and future contributions of national community health worker programs to achieving global health goals. Glob. Health Sci. Pract. 2021, 9, 1–9. [Google Scholar] [CrossRef]
- Moher, D.; Naudet, F.; Cristea, I.A.; Miedema, F.; Ioannidis, J.P.; Goodman, S.N. Assessing scientists for hiring, promotion, and tenure. PLoS Biol. 2018, 16, e2004089. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| City Disease | Influence Situation |
|---|---|
| Polluted environment | Residents have low health conditions and poor living conditions. |
| Mass infection | |
| Traffic congestion | Residents’ simple but basic needs are not always met, such as traveling and some living materials. |
| Stressful life | |
| Frequent disasters | Job opportunities are rare, and defaults on wage payments occur occasionally. |
| Prominent social problems |
| Basic Information | ||||||||
| Age | Do you have a chronic disease? | |||||||
| Gender | Have you been infected with COVID-19? | |||||||
| No. | Content of the questionnaire | Options: A. Strongly agree B. Relatively agree C. Neutral D. Disagree E. Extremely disagree | ||||||
| Respiratory diseases (mainly COVID-19) | ||||||||
| 1 | COVID-19 is extremely contagious. | A | B | C | D | E | ||
| 2 | Maintaining personal and environmental hygiene is an effective measure to prevent COVID-19. | A | B | C | D | E | ||
| 3 | In a crowded environment, I always wear a mask. | A | B | C | D | E | ||
| 4 | I am actively vaccinated against COVID-19. | A | B | C | D | E | ||
| 5 | You are satisfied with your community’s COVID-19 prevention efforts. | A | B | C | D | E | ||
| 6 | Have you recently contracted other respiratory diseases? | A | B | C | D | E | ||
| 7 | Community workers will often visit your home to check on your health. | A | B | C | D | E | ||
| Status of community safety and health services | ||||||||
| 1 | I think my living environment is clean and up to standard regarding hygiene. | A | B | C | D | E | ||
| 2 | I can achieve my goals in my living environment in a healthy state. | A | B | C | D | E | ||
| 3 | My life and activities will not be threatened by environmental sanitation. | A | B | C | D | E | ||
| 4 | Community staff will conduct regular health and hygiene training. | A | B | C | D | E | ||
| 5 | You are satisfied with the health service attitude of the community workers. | A | B | C | D | E | ||
| 6 | Community workers can achieve health protection purposes in a variety of ways. | A | B | C | D | E | ||
| 7 | You are satisfied with the work content of health care in the community. | A | B | C | D | E | ||
| 8 | You think the spread of healthy communities is very important. | A | B | C | D | E | ||
| 9 | The appearance of community workers is decent. | A | B | C | D | E | ||
| 10 | The community environment is quiet, clean, and human-focused. | A | B | C | D | E | ||
| 11 | Community service workers are very concerned about the residents, and they can help answer any concerns in a timely manner. | A | B | C | D | E | ||
| 12 | Community health service centers are generally trustworthy. | A | B | C | D | E | ||
| Other supplements: | ||||||||
| Methods | Statistics | Expert Assess | |
|---|---|---|---|
| Performance | |||
| Initial data | Good | Good | |
| Relevance | Good | Good | |
| The correctness of the question | Good | Better | |
| The appropriateness of the survey time | Good | Good | |
| Judgment Standard | Patient’s Physical Mobility | Daily Activities | |
|---|---|---|---|
| Time of Evaluation | |||
| Before the implementation of the proposed community structure | 17.43 ± 7.28 | 16.57 ± 7.24 | |
| After the implementation of the proposed community structure | 20.18 ± 5.42 | 19.75 ± 5.45 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Jiang, Z.; Hou, Y.; Wang, H.; Wang, Z. Healthy City Community Space-Oriented Structural Planning and Management Optimization under COVID-19. Int. J. Environ. Res. Public Health 2023, 20, 3863. https://doi.org/10.3390/ijerph20053863
Yang Y, Jiang Z, Hou Y, Wang H, Wang Z. Healthy City Community Space-Oriented Structural Planning and Management Optimization under COVID-19. International Journal of Environmental Research and Public Health. 2023; 20(5):3863. https://doi.org/10.3390/ijerph20053863
Chicago/Turabian StyleYang, Ya, Zhengyu Jiang, Yawei Hou, Huaxing Wang, and Zeyu Wang. 2023. "Healthy City Community Space-Oriented Structural Planning and Management Optimization under COVID-19" International Journal of Environmental Research and Public Health 20, no. 5: 3863. https://doi.org/10.3390/ijerph20053863
APA StyleYang, Y., Jiang, Z., Hou, Y., Wang, H., & Wang, Z. (2023). Healthy City Community Space-Oriented Structural Planning and Management Optimization under COVID-19. International Journal of Environmental Research and Public Health, 20(5), 3863. https://doi.org/10.3390/ijerph20053863