
How Can a Bundled Payment Model Incentivize the Transition from Single-Disease Management to Person-Centred and Integrated Care for Chronic Diseases in the Netherlands?

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Case Example: OPTIMA FORMA
2.2. Incentives in Payment Models
2.3. Design of an Alternative Payment Model
2.4. Expected Impact on Integration of Care
3. Results
3.1. Incentives Induced by Different Payment Models
3.2. Proposed Payment Model for Person-Centred and Integrated Care
3.3. Consequences of the Proposed Payment Model
3.4. Impact on Integration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Target population: The care programme focuses on people with DM2, COPD/asthma, and/or CVRM, and who are subscribed for at least one of these current DMPs at one of the participating GP practices and who is insured at one of the participating health insurers. This was used to delineate the patient population. The patient population is heterogeneous because people with these chronic diseases can be of all ages and can have multiple other chronic diseases. The care plan has the potential to broaden the scope and include other chronic diseases (i.e., people with rheumatological disorders). The payment model could be extended as well.
- Main contractor of the bundled payment: The main contractor is the primary care cooperative. The care group finances all participating healthcare providers participating in the care programme. The primary care cooperative is responsible for a fair allocation. The healthcare providers are subcontracted by the primary care cooperative [i.e., the GP practice, the dietician, the physiotherapist, the foot therapist, the medical specialist, the primary mental health physician, and the district nurse].
- Care coordinator and provider coverage: The general practitioner (GP) is responsible and the practice nurse (POH-S) is the coordinator of care. The POH-S and the patient formulate the care goals, based on the integral health status of the patient. The POH-S coordinates and organizes the chosen health interventions.
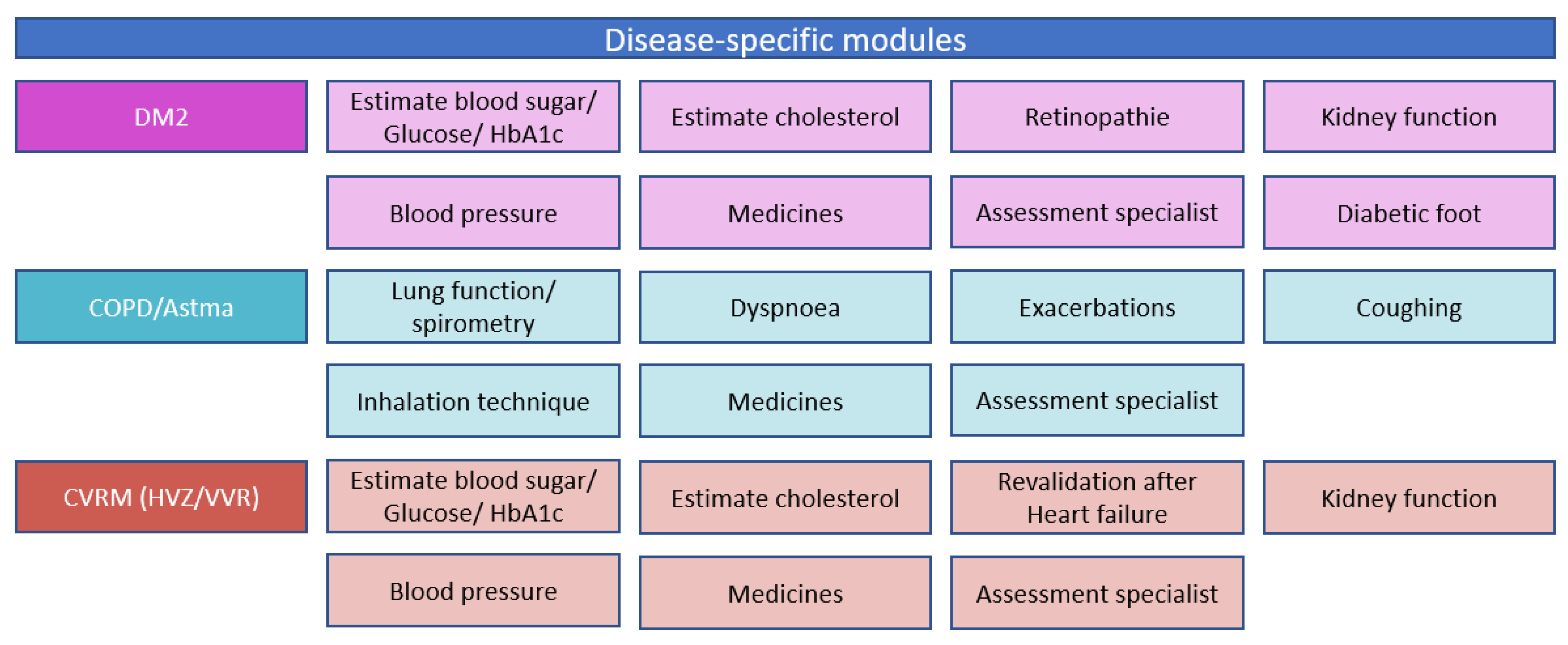
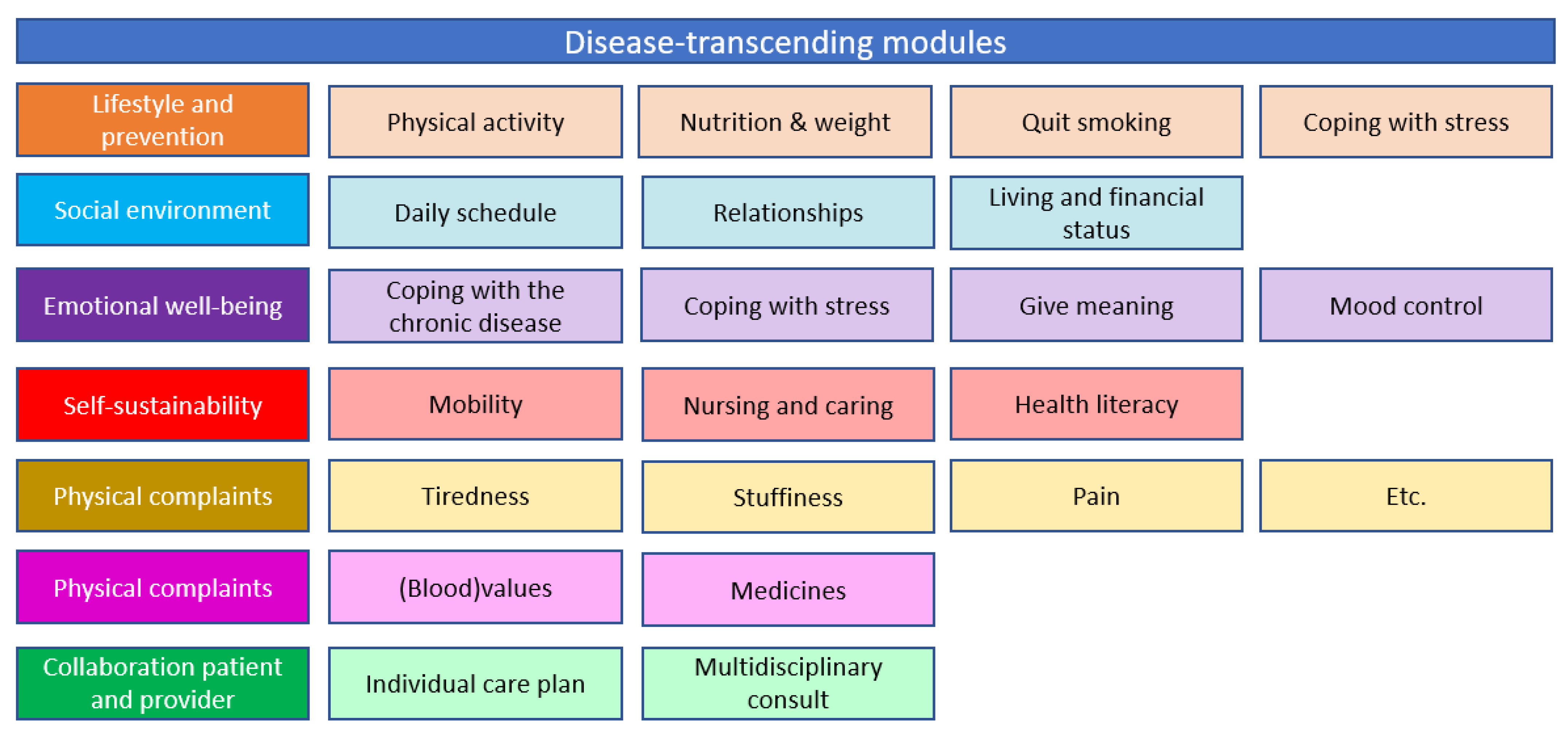
- Provided care through the person-centred care plan: All the interventions provided in the different modules (Figure 1) are covered in either the person-centred bundled payment or included in the virtual budget. The disease-specific and disease-transcending modules focus on (1) lifestyle and prevention, (2) social environment, (3) emotional well-being, (4) self-sustainability, (5) physical complaints, and (6) physical functioning.
- Budget for quarterly bundled payment: the bundled payment is a fixed budget which is paid every three months. The budget is based on a weighted average sum of all provided care activities. The weighting is based on the number of patients that use a certain care activity and the price of the intervention. Each goal of the patient can be reached in different ways:
- The patient can do something his/herself.
- The patient could use E-health to reach a goal.
- The patient could receive help from a non-medical caregiver (once, in a group, or long-term individual help).
- The patient could receive help from a GP or a practice nurse (once, in a group, or long-term individual help).
- The patient could receive help from a (specialized) provider outside the GP practice (once, in a group, or long-term individual help).
- 6.
- Retrospective or prospective payment: The average tariff of the person-centred bundled payment will be prospectively determined. The virtual budget will also be prospectively calculated and compared to the real expenditures. These real expenditures will be retrospectively determined and compared with the estimated virtual budget.
- 7.
- Calculation of the virtual budget [38]: The virtual budget will be determined by the average [health]care expenditures of one year. All patients who were included in at least one of the existing DMPs for DM2, CVRM, and or COPD in 2017, will be included in the virtual budget. The average expenditures per patient will be calculated with the following formula [38]:
- 8.
- Usage of a one-sided or two-sided shared savings model and the duration of the contract: We would advise to start with a one-sided shared savings contract. In this case, the primary care cooperative and health insurer only share when the care group achieves to save money. When there are more expenditures in 2021 compared to the virtual budget, these will be paid by the health insurer. It is undesirable to start with a two-sided shared savings model because the care groups need some time to get used to the new delivery model. If the risks are too high for the primary care cooperative, it could induce adverse behaviour and reduce costs by saving on needed care. From the literature, we know that a two-sided shared savings model could eventually increase savings [12,13,76], which could make it desirable to switch to a two-sided contract after some time, for instance, after three years. For this reason, we would advise to sign a contract for at least three to five years, to have enough time to recoup the investments.
- 9.
- Distribution if there are any savings: the primary care cooperative and preferential health insurer should negotiate about the distribution of any savings. We would advise to let the distribution depend on the quality of the delivered care. Step 10 will describe a pay-for-performance model in more detail. It is important to clarify how possible savings will be spent. The care group is responsible for their part of the savings. The care group could divide all savings equally across participating providers. It is also possible to use any savings to innovate or to use the savings in a region where it is needed the most.
- 10.
- Case-mix adjustment: First, it is important to avoid risk-selection. If the GP practice only selects relatively healthy patients and we would not adjust for case-mix variables, this practice can easily generate savings, because the average costs of a relatively healthy patient population are lower compared to the average costs. The average budget must be adjusted to the included patient population of that region/ practice. It is important to adjust for case-mix differences because the patient population is heterogeneous [patients who are just diagnosed with one chronic disease, or patients with multimorbidity and psychosocial problems].
- 11.
- Pay-for-performance: To keep track of the quality of care, we would advise to implement a form of pay-for-performance. We suggest making the sharing distribution dependent on the quality of care. The bottleneck is selecting which quality indicators to use. It is important that the indicators reflect the care plan and that they can be improved by the new way of working. Care groups, health insurers, and researchers should discuss which indicators would fit this purpose. We would advise to mainly focus on outcome indicators because these are clinically most relevant. The currently used indicators do not seem to fit because these indicators are mainly focused on the process of care instead of outcomes. Actions just need to be ticked off a checklist.
References
- Chen, Y.H.; Karimi, M.; Rutten-Van Mölken, M.P.M.H. The disease burden of multimorbidity and its interaction with educational level. PLoS ONE 2020, 15, e0243275. [Google Scholar] [CrossRef] [PubMed]
- Velek, P.; Luik, A.I.; Brusselle, G.G.O.; Stricker, B.C.; Bindels, P.J.E.; Kavousi, M.; Kieboom, B.C.T.; Voortman, T.; Ruiter, R.; Ikram, M.A.; et al. Sex-specific patterns and lifetime risk of multimorbidity in the general population: A 23-year prospective cohort study. BMC Med. 2022, 20, 304. [Google Scholar] [CrossRef] [PubMed]
- Struckmann, V.; Leijten, F.R.; van Ginneken, E.; Kraus, M.; Reiss, M.; Spranger, A.; Boland, M.R.; Czypionka, T.; Busse, R.; Mölken, M.R.-V. Relevant models and elements of integrated care for multi-morbidity: Results of a scoping review. Health Policy 2017, 122, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Macinko, J.; Starfield, B.; Shi, L. The Contribution of Primary Care Systems to Health Outcomes within Organization for Economic Cooperation and Development (OECD) Countries, 1970–1998. Health Serv. Res. 2003, 38, 831–865. [Google Scholar] [CrossRef]
- NHG-Standaard Diabetes Mellitus Type 2 (M01). 2021. Available online: https://richtlijnen.nhg.org/files/pdf/63_Diabetesmellitustype2_november-2021.pdf (accessed on 11 November 2021).
- Platform Vitale Vaten. Zorgstandaard Vasculair Risicomanagement Deel I (Voor Zorgverleners). 2009. pp. 1–27. Available online: http://www.vitalevaten.nl/uploads/media/Zorgstandaard_deel_I_voor_zorgverleners.pdf (accessed on 11 November 2021).
- Long Alliantie Nederland. Zorgstandaard COPD. 1991. pp. 1–30. Available online: https://www.longalliantie.nl/content/LAN_Zorgstandaard_COPD-2016-2.pdf (accessed on 11 November 2021).
- Out, K.E.M.; de Jong, J.D. Het Perspectief van Zorggroepen en Gezondheidscentra op Onderhandelingen en Contracten Met Zorgverzekeraars. Nivel. 2016. Available online: https://www.nivel.nl/sites/default/files/bestanden/Rapport_Contractering_van_zorggroepen_en_gezondheidscentra.pdf (accessed on 8 November 2021).
- van den Berg, M.; de Bakker, D. Meta-Analyse Introductie: Introductie Praktijkondersteuning op HBO-Niveau in de Huisartsenpraktijk in Nederland. Nivel. 2003. Available online: https://www.nivel.nl/sites/default/files/bestanden/LINH-praktijkondersteuning-hbo-huisartsenpraktijk.pdf (accessed on 8 November 2021).
- de Bakker, D.; Raams, J.; Schut, E.; Vrijhoef, B.; de Wildt, J. Eindrapport van de Evaluatiecommissie—Integrale Bekostiging Integrale bekostiging van zorg: Werk in uitvoering. Nivel. 2012. Available online: https://www.nivel.nl/sites/default/files/bestanden/Eindrapport-integrale-bekostiging-zorg.pdf (accessed on 10 December 2021).
- Tsiachristas, A.; Hipple-Walters, B.; Lemmens, K.M.; Nieboer, A.P.; Rutten-van Mölken, M.P. Towards integrated care for chronic conditions: Dutch policy developments to overcome the (financial) barriers. Health Policy 2011, 101, 122–132. [Google Scholar] [CrossRef]
- McWilliams, J.M.; Chernew, M.E.; Landon, B.E.; Schwartz, A.L. Performance Differences in Year 1 of Pioneer Accountable Care Organizations. N. Engl. J. Med. 2015, 372, 1927–1936. [Google Scholar] [CrossRef]
- Song, Z.; Ji, Y.; Safran, D.G.; Chernew, M.E. Health Care Spending, Utilization, and Quality 8 Years into Global Payment. N. Engl. J. Med. 2019, 381, 252–263. [Google Scholar] [CrossRef]
- Busse, R.; Stahl, J. Integrated Care Experiences And Outcomes In Germany, The Netherlands, and England. Health Aff. 2014, 33, 1549–1558. [Google Scholar] [CrossRef]
- Hildebrandt, H.; Hermann, C.; Knittel, R.; Richter-Reichhelm, M.; Siegel, A.; Witzenrath, W. Gesundes Kinzigtal Integrated Care: Improving population health by a shared health gain approach and a shared savings contract. Int. J. Integr. Care 2010, 10, e046. [Google Scholar] [CrossRef]
- Coulter, A. Evaluating general practice fundholding in the United Kingdom. Eur. J. Public Health 1995, 5, 233–239. [Google Scholar] [CrossRef]
- Gosden, T.; Torgerson, D.J. The effect of fundholding on prescribing and referral costs: A review of the evidence. Health Policy 1997, 40, 103–114. [Google Scholar] [CrossRef]
- Where next for Integrated Care Organisations in the English NHS? Available online: https://www.nuffieldtrust.org.uk/files/2017-01/where-next-integrated-care-english-nhs-web-final.pdf%0Ahttp://nuffield.dh.bytemark.co.uk/sites/files/nuffield/publication/where_next_for_integrated_care_organisations_in_the_english_nhs_230310.pdf%0Ahttp://ww (accessed on 15 March 2022).
- Transparante Ketenzorg. 2021. pp. 4–7. Available online: https://ineen.nl/wp-content/uploads/2021/06/Benchmark-Transparante-Ketenzorg-2020.pdf (accessed on 14 September 2022).
- Struijs, J.N.; de Jong-van Til, J.T.; Lemmens, L.C.; Drewes, H.W.; de Bruin, S.R.; Baan, C.A. Drie Jaar Integrale Bekostiging van Diabeteszorg. Effecten Op Zorgproces En Kwaliteit van Zorg. RIVM. 2017. Available online: http://www.narcis.nl/publication/RecordID/oai%3Arivm.openrepository.com%3A10029%2F257271 (accessed on 14 March 2022).
- Murtagh, S.; McCombe, G.; Broughan, J.; Carroll, Á.; Casey, M.; Harrold, Á.; Dennehy, T.; Fawsitt, R.; Cullen, W. Integrating Primary and Secondary Care to Enhance Chronic Disease Management: A Scoping Review. Int. J. Integr. Care 2021, 21, 4. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M.; Soubhi, H.; Fortin, M.; Hudon, C.; O’Dowd, T. Managing patients with multimorbidity: Systematic review of interventions in primary care and community settings. BMJ 2012, 345, e5205. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.; Knottnerus, J.A.; Green, L.; van der Horst, H.; Jadad, A.R.; Kromhout, D.; Leonard, B.; Lorig, K.; Loureiro, M.I.; van der Meer, J.W.M.; et al. How should we define health? BMJ 2011, 343, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.; van Vliet, M.; Giezenberg, M.; Winkens, B.; Heerkens, Y.; Dagnelie, P.C.; Knottnerus, J.A. Towards a ‘patient-centred’ operationalisation of the new dynamic concept of health: A mixed methods study. BMJ Open 2016, 6, e010091. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, B.; Payne, K.; Alderson, P.; McMurdo, M.E.T.; Mercer, S. Adapting clinical guidelines to take account of multimorbidity. BMJ 2012, 345, e6341. [Google Scholar] [CrossRef]
- Wallace, E.; Salisbury, C.; Guthrie, B.; Lewis, C.; Fahey, T.; Smith, S.M. Managing patients with multimorbidity in primary care. BMJ 2015, 350, 6–11. [Google Scholar] [CrossRef]
- Tsiachristas, A.; Dikkers, C.; Boland, M.R.; Mölken, M.P.R.-V. Exploring payment schemes used to promote integrated chronic care in Europe. Health Policy 2013, 113, 296–304. [Google Scholar] [CrossRef]
- Karimi, M.; Tsiachristas, A.; Looman, W.; Stokes, J.; van Galen, M.; Rutten-van Mölken, M. Bundled payments for chronic diseases increased health care expenditure in the Netherlands, especially for multimorbid patients. Health Policy 2021, 125, 751–759. [Google Scholar] [CrossRef]
- Looman, W.; Struckmann, V.; Köppen, J.; Baltaxe, E.; Czypionka, T.; Huic, M.; Pitter, J.; Ruths, S.; Stokes, J.; Bal, R.; et al. Drivers of successful implementation of integrated care for multi-morbidity: Mechanisms identified in 17 case studies from 8 European countries. Soc. Sci. Med. 2021, 277, 113728. [Google Scholar] [CrossRef]
- Denkraam Integratie Zorgprogramma’s Voor Chronische Aandoeningen. 2019. pp. 1–17. Available online: https://ineen.nl/wp-content/uploads/2020/06/200528-05-01-denkraam-integratie-zorgprogrammas.pdf (accessed on 18 January 2022).
- Bodenheimer, T.; Sinsky, C. From Triple to Quadruple Aim: Care of the Patient Requires Care of the Provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef]
- Vercoulen, J.H. A simple method to enable patient-tailored treatment and to motivate the patient to change behaviour. Chronic Respir. Dis. 2012, 9, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, E.; Vercoulen, J.; Elbers, L.; Behr, R.; Schermer, T. De NCSI-Methode: Maatwerk Voor COPD-Zorg. Huisarts-en Wet. 2016, 59, 242–247. [Google Scholar] [CrossRef]
- Raaijmakers, L.H.A.; Schermer, T.R.; Wijnen, M.; Van Bommel, H.E.; Michielsen, L.; Boone, F.; Vercoulen, J.H.; Bischoff, E.W.M.A. Development of a person-centred integrated care approach for chronic disease management in Dutch primary care: A mixed-method study. Int. J. Environ. Res. Public Health, 2023; in press. [Google Scholar]
- Quinn, K. The 8 Basic Payment Methods in Health Care. Ann. Intern. Med. 2015, 163, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Alternative Payment Model: APM Framework Refreshed for 2017. Available online: https://hcp-lan.org/workproducts/apm-refresh-whitepaper-final.pdf (accessed on 16 September 2021).
- Cattel, D.; Eijkenaar, F. Value-Based Provider Payment Initiatives Combining Global Payments With Explicit Quality Incentives: A Systematic Review. Med Care Res. Rev. 2019, 77, 511–537. [Google Scholar] [CrossRef] [PubMed]
- Hayen, A.P.; van den Berg, M.J.; Meijboom, B.R.; Struijs, J.N.; Westert, G.P. Incorporating shared savings programs into primary care: From theory to practice. BMC Health Serv. Res. 2015, 15, 580. [Google Scholar] [CrossRef] [PubMed]
- Steenhuis, S.; Struijs, J.; Koolman, X.; Ket, J.; van der Hijden, E. Unraveling the Complexity in the Design and Implementation of Bundled Payments: A Scoping Review of Key Elements From a Payer’s Perspective. Milbank Q. 2020, 98, 197–222. [Google Scholar] [CrossRef]
- Eijkenaar, F.; Emmert, M.; Scheppach, M.; Schöffski, O. Effects of pay for performance in health care: A systematic review of systematic reviews. Health Policy 2013, 110, 115–130. [Google Scholar] [CrossRef]
- Mendelson, A.; Kondo, K.; Damberg, C.; Low, A.; Motúapuaka, M.; Freeman, M.; O’Neil, M.; Relevo, R.; Kansagara, D. The Effects of Pay-for-Performance Programs on Health, Health Care Use, and Processes of Care: A systematic review. Ann. Intern. Med. 2017, 166, 341–353. [Google Scholar] [CrossRef]
- Hayen, A. Shared Savings and Patient Cost Sharing in the Dutch Health Care System. Ph.D. Thesis, Tilburg University, Tilburg, The Netherlands, 30 November 2018. [Google Scholar]
- McWilliams, J.M.; Hatfield, L.A.; Landon, B.E.; Hamed, P.; Chernew, M.E. Medicare Spending after 3 Years of the Medicare Shared Savings Program. N. Engl. J. Med. 2018, 379, 1139–1149. [Google Scholar] [CrossRef]
- Agarwal, R.; Liao, J.M.; Gupta, A.; Navathe, A.S. The Impact Of Bundled Payment On Health Care Spending, Utilization, And Quality: A Systematic Review. Health Aff. 2020, 39, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Struijs, J.N.; de Vries, E.F.; van Dorst, H.D.C.A.; Over, E.A.B.; Baan, C.A. Geboortezorg in Beeld—Een Nulmeting En Eerste Ervaringen Met Het Werken Met Integrale Bekostiging. RIVM. 2018. Available online: https://www.rivm.nl/bibliotheek/rapporten/2018-0109.pdf (accessed on 8 February 2023).
- Stokes, J.; Struckmann, V.; Kristensen, S.R.; Fuchs, S.; van Ginneken, E.; Tsiachristas, A.; van Mölken, M.R.; Sutton, M. Towards incentivising integration: A typology of payments for integrated care. Health Policy 2018, 122, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Kralj, B.; Kantarevic, J. Quality and quantity in primary care mixed-payment models: Evidence from family health organizations in Ontario. Can. J. Econ./Rev. Can. D’économique 2013, 46, 208–238. [Google Scholar] [CrossRef]
- Krasnik, A.; Groenewegen, P.P.; Pedersen, P.A.; von Scholten, P.; Mooney, G.; Gottschau, A.; Flierman, H.A.; Damsgaard, M.T. Changing remuneration systems: Effects on activity in general practice. BMJ 1990, 300, 1698–1701. [Google Scholar] [CrossRef] [PubMed]
- Iversen, T.; Luras, H. The effect of capitation on GPs’ referral decisions. Health Econ. 2000, 9, 199–210. [Google Scholar] [CrossRef]
- van der Hijden, E.; Steenhuis, S.; Hofstra, G.; van der Wolk, J.; Bijlsma, W.; Struijs, J.; Koolman, X. Ontwikkelingen in zorginkoop: Van inkoop van verrichtingen naar inkoop van zorgbundels. Maandbl. Voor Account. en Bedrijfsecon. 2019, 93, 223–239. [Google Scholar] [CrossRef]
- Tsiachristas, A. Payment and economic evaluation of integrated care. Int. J. Integr. Care 2015, 15, e013. [Google Scholar] [CrossRef]
- Gosden, T.; Forland, F.; Kristiansen, I.; Sutton, M.; Leese, B.; Giuffrida, A.; Sergison, M.; Pedersen, L. Capitation, salary, fee-for-service and mixed systems of payment: Effects on the behaviour of primary care physicians. Cochrane Database Syst. Rev. 2000, 2000, CD002215. [Google Scholar] [CrossRef]
- Gosden, T.; Forland, F.; Kristiansen, I.S.; Sutton, M.; Leese, B.; Giuffrida, A.; Sergison, M.; Pedersen, L. Impact of payment method on behaviour of primary care physicians: A systematic review. J. Health Serv. Res. Policy 2001, 6, 44–55. [Google Scholar] [CrossRef]
- Simoens, S.; Giuffrida, A. The Impact of Physician Payment Methods on Raising the Efficiency of the Healthcare System: An international comparison. Appl. Health Econ. Health Policy 2004, 3, 39–46. [Google Scholar] [CrossRef]
- Barros, P.P. Cream-skimming, incentives for efficiency and payment system. J. Health Econ. 2003, 22, 419–443. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.C. Theory and Practice in the Design of Physician Payment Incentives. Milbank Q. 2001, 79, 149–177. [Google Scholar] [CrossRef] [PubMed]
- Andrawis, J.P.; Koenig, K.M.; Bozic, K.J. Bundled payment care initiative: How this all started. Semin. Arthroplast. JSES 2016, 27, 188–192. [Google Scholar] [CrossRef]
- Cutler, D.M.; Ghosh, K. The Potential for Cost Savings through Bundled Episode Payments. N. Engl. J. Med. 2012, 366, 1075–1077. [Google Scholar] [CrossRef]
- Weeks, W.B.; Rauh, S.S.; Wadsworth, E.B.; Weinstein, J.N. The Unintended Consequences of Bundled Payments. Ann. Intern. Med. 2013, 158, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Struijs, J.N.; Mohnen, S.M.; Molema, C.C.M.; de Jong-van Til, J.T.; Baan, C.A. Effect van Integrale Bekostiging Op Curatieve. RIVM. 2010. Available online: https://www.rivm.nl/bibliotheek/rapporten/260131005.pdf (accessed on 16 September 2021).
- De Invloed van Financiele Prikkels op de Behandeltijd in de GGZ. Me Judice. 2015. Available online: https://www.mejudice.nl/artikelen/detail/de-invloed-van-financiele-prikkels-op-de-behandeltijd-in-de-ggz (accessed on 16 September 2021).
- Advies Zorgprestatiemodel Ggz en, fz. Advies Zorgprestatiemodel Ggz en fz. 2019. pp. 1–60. Available online: https://www.vgn.nl/system/files/article/file/Advies%2Bzorgprestatiemodel%2Bggz%2Ben%2Bfz%2B-%2BDEFINITIEF.pdf (accessed on 16 September 2021).
- Belonen van Zorg Die Waarde Toevoegt Inhoud. 2018. Available online: https://puc.overheid.nl/nza/doc/PUC_252732_22/1/ (accessed on 16 September 2021).
- Invoering Abonnementstarief in de Wmo per 2020 Uitvoeringstoets naar de Gemeenten. 2018. Available online: https://www.eerstekamer.nl/overig/20181219/invoering_abonnementstarief_in_de/document (accessed on 16 September 2021).
- Doorontwikkeling Bekostiging Wlz. 2017. Available online: https://puc.overheid.nl/nza/doc/PUC_3566_22/1/ (accessed on 16 September 2021).
- Eijkenaar, F.; Schut, E. Uitkomstbekostiging in de Zorg: Een (on) Begaanbare Weg? 2015. pp. 1–126. Available online: https://www.eur.nl/sites/corporate/files/Onderzoeksrapport_uitkomstbekostiging_in_de_zorg_def_24032015__FE3__0.pdf (accessed on 6 December 2021).
- Holmstrom, B.; Milgrom, P. Multitask Principal-Agent Analyses: Incentive Contracts, Asset Ownership, and Job Design. J. Law, Econ. Organ. 1991, 7, 24–52. [Google Scholar] [CrossRef]
- Smith, P.C.; York, N. Quality incentives: The case of U.K. general practitioners—An ambitious U.K. quality improvement initiative offers the potential for enormous gains in the quality of primary health care. Health Aff. 2004, 23, 112–118. [Google Scholar] [CrossRef][Green Version]
- Kirschner, K.; Braspenning, J.; Akkermans, R.P.; Jacobs, J.E.A.; Grol, R. Assessment of a pay-for-performance program in primary care designed by target users. Fam. Pract 2013, 30, 161–171. [Google Scholar] [CrossRef]
- Campbell, S.M.; Reeves, D.; Kontopantelis, E.; Sibbald, B.; Roland, M. Effects of Pay for Performance on the Quality of Primary Care in England. N. Engl. J. Med. 2009, 361, 368–378. [Google Scholar] [CrossRef]
- Longzorg Gestuurd op Uitkomsten. 2018. pp. 24–25. Available online: https://www.gc-nijkerk.nl/wp-content/uploads/2018/02/longzorg-eerstelijns.pdf (accessed on 12 April 2022).
- LongZorg Nijkerk Doelstelling. 2018. Available online: https://www.rug.nl/cpheb/docs/jurriaanpropper.pdf (accessed on 12 April 2022).
- McWilliams, J.M.; Hatfield, L.A.; Chernew, M.E.; Landon, B.E.; Schwartz, A.L. Early Performance of Accountable Care Organizations in Medicare. N. Engl. J. Med. 2016, 374, 2357–2366. [Google Scholar] [CrossRef]
- Song, Z.; Rose, S.; Safran, D.G.; Landon, B.E.; Day, M.P.; Chernew, M.E. Changes in Health Care Spending and Quality 4 Years into Global Payment. N. Engl. J. Med. 2014, 371, 1704–1714. [Google Scholar] [CrossRef]
- Ouayogodé, M.H.; Colla, C.H.; Lewis, V.A. Determinants of success in Shared Savings Programs: An analysis of ACO and market characteristics. Healthcare 2016, 5, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Nyweide, D.J.; Lee, W.; Cuerdon, T.T.; Pham, H.H.; Cox, M.; Rajkumar, R.; Conway, P.H. Association of Pioneer Accountable Care Organizations vs Traditional Medicare Fee for Service With Spending, Utilization, and Patient Experience. JAMA—J. Am. Med. Assoc. 2015, 313, 2152–2161. [Google Scholar] [CrossRef] [PubMed]
- Cattel, D.; Eijkenaar, F.; Schut, F.T. Value-based provider payment: Towards a theoretically preferred design. Health Econ. Policy Law 2018, 15, 94–112. [Google Scholar] [CrossRef]
- Berwick, D.M. Launching Accountable Care Organizations—The Proposed Rule for the Medicare Shared Savings Program. N. Engl. J. Med. 2011, 364, e32. [Google Scholar] [CrossRef]
- Overheveling van Zorg? Of Overheveling van Problemen? 2020. pp. 34–36. Available online: https://www.medischcontact.nl/nieuws/laatste-nieuws/artikel/overheveling-van-zorg-of-overheveling-van-problemen.htm (accessed on 15 June 2022).
- de Vries, E.F.; Drewes, H.W.; Struijs, J.N.; Heijink, R.; Baan, C.A. Barriers to payment reform: Experiences from nine Dutch population health management sites. Health Policy 2019, 123, 1100–1107. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Design Elements | |
|---|---|
| Specify bundle and select provider [s]: characteristics of a contract specified by a health insurer and one contracting entity or multiple healthcare providers | How to delineate the population? |
| Definition of the patient population? | |
| Small or heterogeneous patient populations? | |
| How to attribute patients to a provider group? | |
| Which providers are included? | |
| Mandatory or voluntary bundled payment? | |
| Who is the main contractor? | |
| Are the group members employed or subcontracted? | |
| What care services are included in the bundle? | |
| [Re]Allocation of care delivery among providers? | |
| Prospective or retrospective payment strategy? | |
| Negotiate and sign contract: negotiate about price, volume, weight of case-mix method, quality measurement and quality incentive structure, distribution of savings/losses, and risk-mitigating measures for providers | Is the payment real or virtual? |
| How to set a payment/target? (Calculate the average annualizing expenditures, Weight the expenditures, and Cap expenditures, evaluate expenditures against a benchmark, Trending factor, Risk adjustment) | |
| Allocation of possible savings? | |
| One-sided or two-sided risk? | |
| What is the risk-sharing rate? | |
| Is there a maximum saving rate according to the costs? | |
| Is risk adjustment applied? | |
| Which risk adjustors are used? | |
| What is the contract duration? | |
| What care to carve out? | |
| Are shared savings/losses conditional on quality? | |
| Add-on for quality? | |
| Which quality indicators to use? | |
| What measurement level [individual/group]? | |
| Rewards and/or penalties? | |
| Maximum payment size relative to total payment? | |
| Absolute, relative and/or improvement targets? | |
| How often to pay for performance? |
| Payment Model | Providers | Incentivises | Literature |
|---|---|---|---|
| Combination of contract capitation payment and fee for service | General practitioner | Positive Fewer referrals Adequate provision of care (no under- or overtreatment) Preventive care Negative Collaboration not explicitly addressed | [20,47,48,49] |
| Fee for service (FFS) | Physiotherapist, exercise therapist, speech therapist, dietician, and district nursing | Positive High productivity Transparency of the delivered care Negative Overprovision Unnecessary readmissions and diagnostics Quality of care not explicitly addressed Fragmentation of care Preventive care not stimulated | [50,51,52,53] |
| Per time period | Salary paid health care providers | Positive Cost-conscious behaviour Negative Undertreatment Selection of patients Low productivity which could result in longer waiting lists Quality of care not explicitly addressed Unnecessary referrals | [54,55,56] |
| Per episode (chronic care) | The SDMPs for chronic diseases in primary care | Positive Integrated care (coordination and continuity) Cost-conscious behaviour High quality of care Efficient care Negative Risk selection ‘Over-bundling’ * Double billing Unnecessary referrals Undertreatment within the bundle | [14,50,57,58,59,60] |
| Per episode (1. DTCs in specialist care, 2. Per patient profile and time, and 3. Per treatment activity and time) |
| Positive Less fragmentation of care Efficiency Negative Strategic declaration behaviour Overprovision Upcoding | [61,62,63] |
| Contract capitation in combination with a patient co-payment (€19 per month) | Social care | Positive Wide access because of the low co-payment Flexibility to tailor help to personal circumstances Negative Underuse because of accumulating co-payments | [64,65] |
| Pay for performance | Alternative payment model | Positive Quality of care explicitly addressed Transparency of care Positive spill-over effects ** Negative Negative spill-over effects ** Risk selection Gaming behaviour No incentive if threshold is met Providers held accountable for outcomes they may not be able to influence | [37,40,41,66,67,68,69,70] |
| Shared savings model | Alternative payment model | Positive Cost-conscious behaviour Integrated care (coordination and continuity) Preventive care Quality of care (implicitly and explicitly) Negative Undertreatment To drive the expenditures of the benchmark | [13,14,15,42,43,71,72,73,74] |
| (Sub)population—based bundled payment | Alternative payment model | Positive Integrated care (coordination and continuity) Quality of care Cost-conscious behaviour Preventive care Negative High risk for the contracting entity Reduction of necessary care in the bundle Less freedom of choice Risk selection | [16,17,18,45] |
| Payment Model | Desirable Consequences | Undesirable Consequences |
|---|---|---|
| Person-centred bundled payment | A holistic approach Integration of care More flexibility on how to spend the budget Responsibility of the primary care cooperative and therefore coordination of care Reduction of risk selection | Lowering the threshold to include someone in the person-centred bundled payment Reduction of freedom of choice of the patients because certain physicians are contracted, and others are not Reduction of costs by avoiding necessary care |
| One-sided shared savings | A holistic approach Multidisciplinary collaboration due to mutual responsibility The right care for the right patient at the right place Cost-conscious behaviour Double declaration is unattractive Mitigated risks for the primary care cooperative | Feeling less responsible because the savings partly depend on providers that are not part of the person-centred bundled payment, which makes the coordination difficult Reduction of costs by avoiding necessary care |
| Pay-for-performance | High quality of care | Focus on the measured quality indicators (gaming) |
| Domain (Level) | Explanation |
|---|---|
| Target population (2) | The currently used payment model only focusses on people with either DM2, COPD, or CVRM. The alternative payment model includes care for all three chronic diseases in one bundle and additional disease-transcending care. The alternative payment model focuses on a much wider population; therefore, the level of integration moves from 1 to 2. |
| Time (3) | In the currently used payment model, agreements about the budget are made for one year. We recommend making agreements for multiple years. The collaboration becomes stronger and the mutual trust between primary care cooperative and health insurer increases. Agreements for a longer time span also create more possibilities to innovate and investigate the potentials of the alternative payment model; therefore, the level of integration moves from 2 to 3. |
| Sectors (2.5) | The currently used payment model focusses on primary care. Secondary care is incorporated, but is rather limited and only includes a single consultation by a specialist for a small proportion of the target population. The aim of the alternative payment model is to finance care from all sectors (primary, secondary, tertiary care, and the social domain). The primary care cooperative is a coordinating organ, so also non-financial agreements could be made with, for instance, the municipality about the social care domain. Both the SDMP and the PC-IC programme include preventive interventions like smoking cessation support and lifestyle interventions, but so far these have not been covered by the bundled payment for SDMP. Therefore, the level of integration moves from 1.5 to 2.5. |
| Provider coverage (2.5) | The providers covered by the currently used payment model are the practical nurse, the GP, the dietician, the foot therapist, the physiotherapist, and a consultation with a medical specialist. In the alternative bundled payment, we propose to expand the scope to include all services that are part of the personal care plan (Figure 3). All other healthcare utilization is included in the virtual budget (Figure 2); therefore, the level of integration moves from 1.5 to 2.5. |
| Financial pooling/sharing (2) | In the currently used payment model, the primary care cooperative and health insurer do not usually have agreements about sharing savings or losses. These savings or losses are estimated by comparing a virtual budget (i.e., the expected expenditures) to the real expenditures. We advise to start with a one-sided shared savings model, and therefore, the level of integration moves from 1 to 2. |
| Income (1) | The alternative payment model for PC-IC will not drastically change the income of the individual health care provider. The budget for chronic care of the GP practice increases as the target population increases, but at the same time less care will be financed through FFS. The net result depends on the details of the contract. |
| Multiple diseases/needs focus (2.5) | The currently used payment model finances disease-specific care. The alternative payment model includes all services that are part of the personal care plan (Figure 3). At the start, the model will pertain to people with DM2, CVRM, and/or COPD, but once a patient is incorporated into the PC-IC programme, the patient will be fully assessed on six domains (Figure 1). Therefore, the level of integration moves from 1 to 2.5. |
| Quality measurement (2.5) | In the currently used SDMP, the quality of care is assessed by InEeN, which delivers an annual report about the quality of chronic care. The quality indicators are determined by the Dutch GP society (NHG) and mostly include process indicators (e.g., if the smoking status is registered). The currently used bundled payment is not related to performance on these indicators. In the alternative payment model, we aim to measure quality of care on outcome indicators (e.g., health-related quality of life) and patient satisfaction. The ratio that is used to share savings between the health insurer and the primary care cooperative will depend on the delivered quality of care. Therefore, the level of integration moves from 1 to 2.5. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bour, S.S.; Raaijmakers, L.H.A.; Bischoff, E.W.M.A.; Goossens, L.M.A.; Rutten-van Mölken, M.P.M.H. How Can a Bundled Payment Model Incentivize the Transition from Single-Disease Management to Person-Centred and Integrated Care for Chronic Diseases in the Netherlands? Int. J. Environ. Res. Public Health 2023, 20, 3857. https://doi.org/10.3390/ijerph20053857
Bour SS, Raaijmakers LHA, Bischoff EWMA, Goossens LMA, Rutten-van Mölken MPMH. How Can a Bundled Payment Model Incentivize the Transition from Single-Disease Management to Person-Centred and Integrated Care for Chronic Diseases in the Netherlands? International Journal of Environmental Research and Public Health. 2023; 20(5):3857. https://doi.org/10.3390/ijerph20053857
Chicago/Turabian StyleBour, Sterre S., Lena H. A. Raaijmakers, Erik W. M. A. Bischoff, Lucas M. A. Goossens, and Maureen P. M. H. Rutten-van Mölken. 2023. "How Can a Bundled Payment Model Incentivize the Transition from Single-Disease Management to Person-Centred and Integrated Care for Chronic Diseases in the Netherlands?" International Journal of Environmental Research and Public Health 20, no. 5: 3857. https://doi.org/10.3390/ijerph20053857
APA StyleBour, S. S., Raaijmakers, L. H. A., Bischoff, E. W. M. A., Goossens, L. M. A., & Rutten-van Mölken, M. P. M. H. (2023). How Can a Bundled Payment Model Incentivize the Transition from Single-Disease Management to Person-Centred and Integrated Care for Chronic Diseases in the Netherlands? International Journal of Environmental Research and Public Health, 20(5), 3857. https://doi.org/10.3390/ijerph20053857