
A Three-Armed Randomized Controlled Trial to Evaluate the Effectiveness, Acceptance, and Negative Effects of StudiCare Mindfulness, an Internet- and Mobile-Based Intervention for College Students with No and “On Demand” Guidance

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
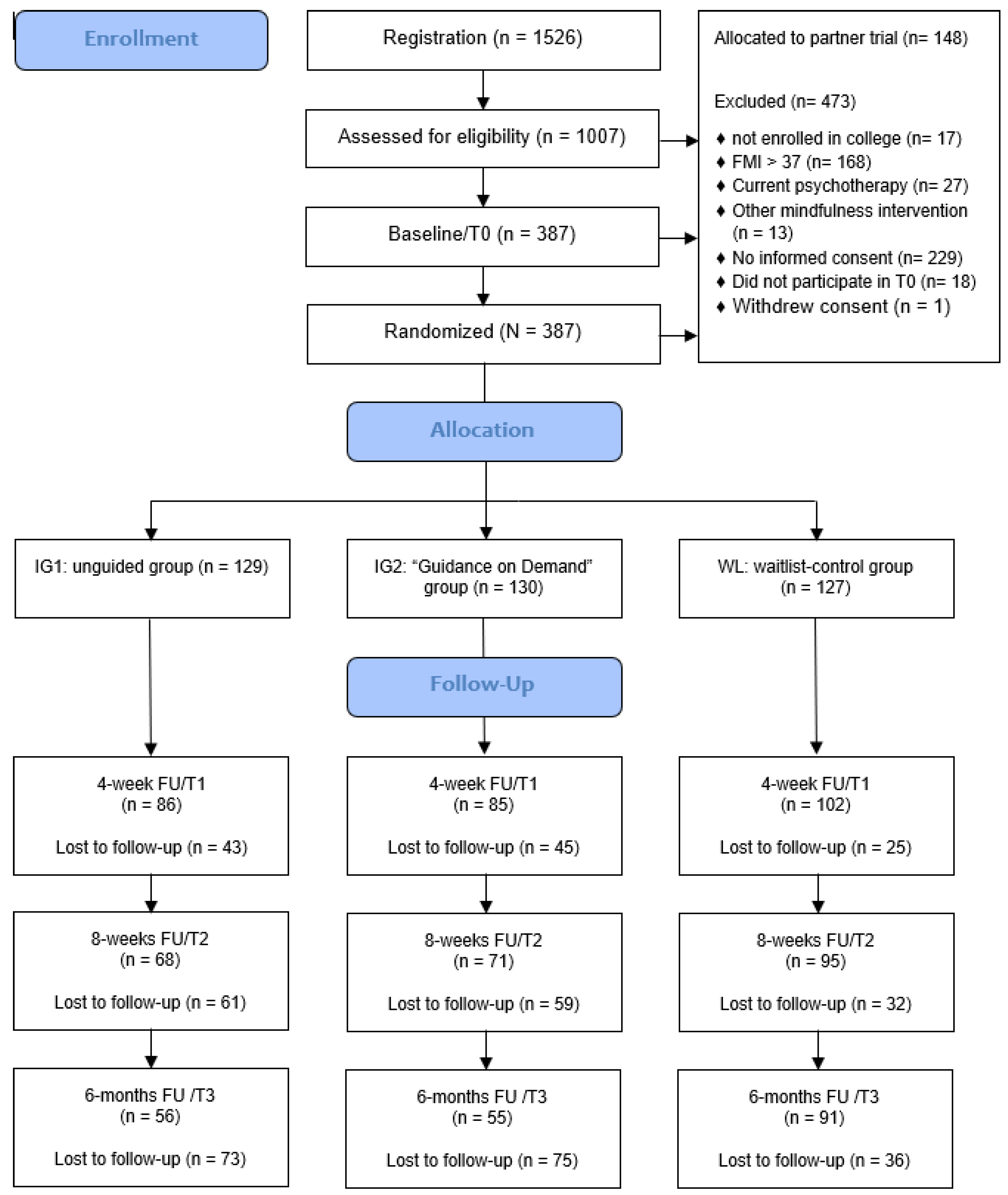
2.1. Study Design
2.2. Eligibility Criteria
2.3. Setting/Recruitment
2.4. Randomization
2.5. Intervention
2.5.1. Guidance and Promotion of Adherence
2.5.2. Control Condition
2.6. Assessments and Outcomes
2.6.1. Primary Outcome
2.6.2. Secondary Outcomes
2.6.3. Covariates
2.7. Statistical Analyses
3. Results
3.1. Participants
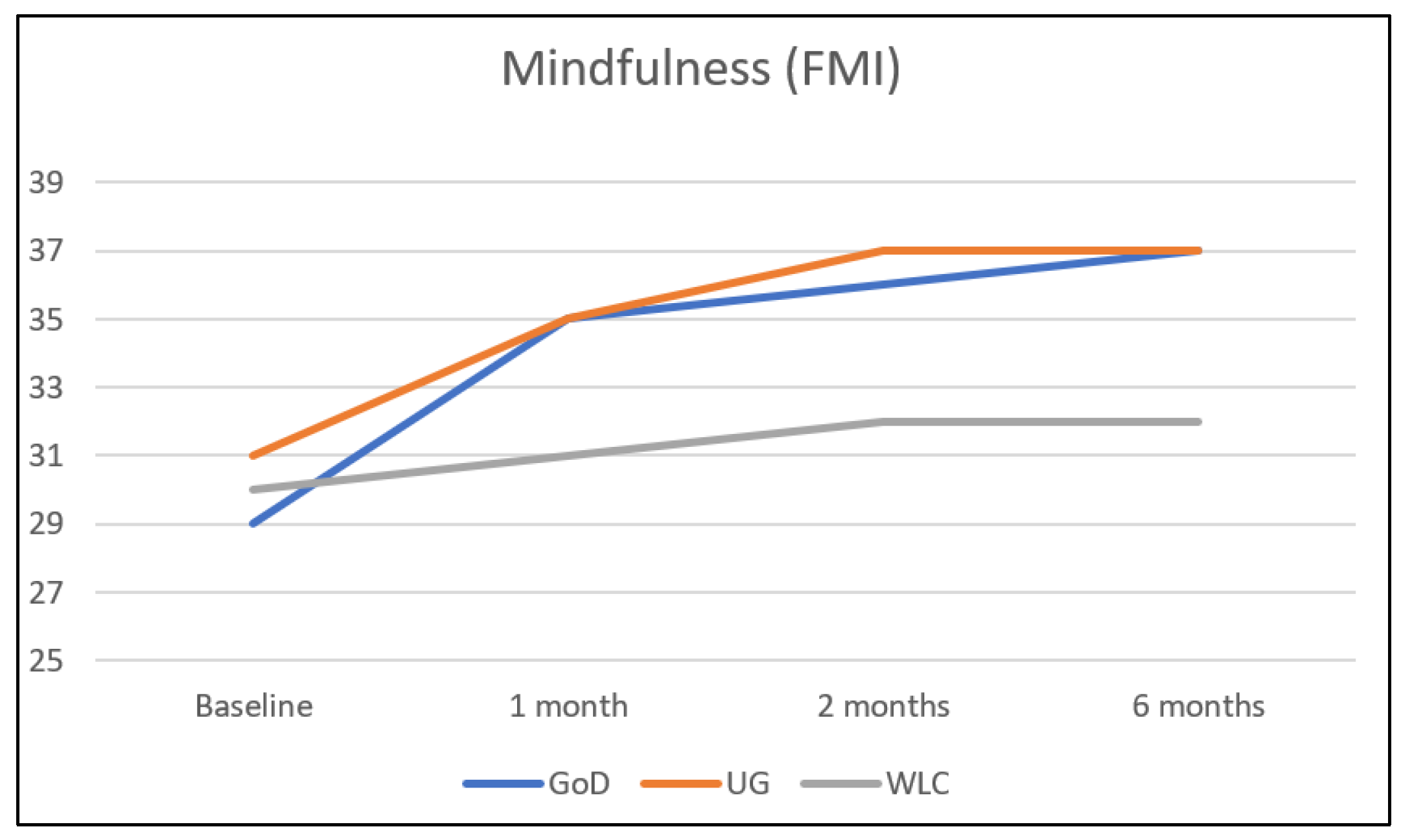
3.2. Primary Outcome Analyses
3.3. Secondary Outcome Analyses

{kind=link}
{kind=link}
| M ± SD | Primary Analyses | Secondary Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|
| UG vs. WL | GoD vs. WL | UG vs. GoD | |||||||
| Variable | UG (n = 129) | GoD (n = 130) | WL (n = 127) | β (95% CI) | p | β (95% CI) | p | β (95% CI) | p |
| Primary Outcome | |||||||||
| Mindfulness (FMI) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 30.56 ± 4.74 34.59 ± 4.75 36.84 ± 4.86 36.49 ± 5.28 | 29.29 ± 4.91 34.45 ± 4.53 36.19 ± 5.10 37.26 ± 5.12 | 29.71 ± 4.71 30.75 ± 5.32 31.50 ± 5.17 31.89 ± 5.29 | 0.65 [0.41; 0.88] 0.88 [0.62; 1.13] 0.73 [0.49; 0.97] | <0.001 <0.001 <0.001 | 0.76 [0.53; 0.99] 0.88 [0.63; 1.13] 0.97 [0.69; 1.25] | <0.001 <0.001 <0.001 | 0.07 [−0.17; 0.31] −0.02 [−0.30; 0.26] 0.22 [−0.03; 0.48] | 0.560 0.898 0.084 |
| Secondary Outcomes | |||||||||
| Depression (PHQ-9) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 9.19 ± 4.41 8.07 ± 3.87 6.94 ± 4.28 6.99 ± 4.15 | 9.34 ± 4.35 7.96 ± 3.88 6.54 ± 4.05 6.67 ± 4.12 | 9.17 ± 4.47 8.99 ± 4.43 8.35 ± 4.26 8.29 ± 4.18 | −0.23 [−0.46; −0.00] −0.33 [−0.62; −0.05] −0.31 [−0.62; −0.01] | 0.048 0.020 0.045 | −0.28 [−0.52; −0.04] −0.44 [−0.68; −0.21] −0.40 [−0.69; −0.12] | 0.025 <0.001 0.007 | −0.05 [−0.28; 0.19] −0.11 [−0.40; 0.18] −0.09 [−0.47; 0.28] | 0.706 0.465 0.620 |
| Anxiety (GAD-7) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 8.35 ± 3.96 7.22 ± 3.73 6.35 ± 4.09 6.37 ± 3.82 | 9.16 ± 4.28 6.69 ± 3.61 5.85 ± 4.14 5.55 ± 3.80 | 8.71 ± 4.34 8.25 ± 4.07 8.18 ± 4.79 8.10 ± 4.60 | −0.22 [−0.46; 0.02] −0.36 [−0.64; −0.08] −0.37 [−0.65; −0.08] | 0.077 0.014 0.012 | −0.46 [−0.70; −0.23] −0.58 [−0.83; −0.33] −0.66 [−0.96; −0.36] | <0.001 <0.001 <0.001 | −0.23 [−0.49; 0.03] −0.20 [−0.48; 0.09] −0.28 [−0.53; −0.03] | 0.082 0.166 0.026 |
| Stress (PSS-4) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 7.71 ± 2.92 6.52 ± 2.84 6.27 ± 3.16 6.02 ± 3.22 | 7.82 ± 3.14 6.21 ± 2.78 5.40 ± 2.81 5.29 ± 3.12 | 7.76 ± 3.01 7.55 ± 2.85 7.27 ± 3.14 6.79 ± 3.13 | −0.35 [−0.60; −0.09] −0.31 [−0.59; −0.03] −0.23 [−0.51; 0.05] | 0.008 0.030 0.102 | −0.47 [−0.73; −0.22] −0.60 [−0.85; −0.35] −0.47 [−0.79; −0.16] | <0.001 <0.001 0.004 | −0.12 [−0.41; 0.16] −0.29 [−0.56; −0.03] −0.24 [−0.58; 0.09] | 0.390 0.031 0.155 |
| Well-being (WHO-5) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 9.64 ± 4.09 11.04 ± 4.57 12.39 ± 5.13 13.19 ± 4.85 | 9.90 ± 4.45 12.65 ± 4.21 13.05 ± 5.13 12.94 ± 4.75 | 9.82 ± 4.36 10.22 ± 4.68 10.41 ± 4.79 11.22 ± 5.05 | 0.20 [−0.07; 0.46] 0.40 [0.13; 0.67] 0.42 [0.09; 0.75] | 0.140 0.004 0.015 | 0.52 [0.27; 0.77] 0.51 [0.24; 0.77] 0.34 [0.06; 0.61] | <0.001 <0.001 0.016 | 0.32 [0.05; 0.60] 0.10 [−0.21; 0.42] −0.08 [−0.37; 0.21] | 0.023 0.508 0.589 |
| Presenteeism (SPS) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 54.73 ± 6.78 - 54.49 ± 7.85 54.81 ± 7.42 | 55.00 ± 6.60 - 55.44 ± 7.62 54.09 ± 8.12 | 55.41 ± 7.36 - 55.20 ± 7.66 55.29 ± 7.84 | - −0.07 [−0.39; 0.25] −0.04 [−0.33; 0.24] | - 0.682 0.774 | - 0.05 [−0.24; 0.33] −0.14 [−0.50; 0.22] | - 0.744 0.436 | - 0.11 [−0.19; 0.42] −0.10 [−0.47; 0.27) | - 0.462 0.588 |
| Work Output | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 63.46 ± 21.25 - 67.60 ± 23.64 69.58 ± 25.07 | 62.98 ± 21.65 - 71.79 ± 22.87 70.56 ± 24.11 | 63.09 ± 22.98 - 66.14 ± 22.61 68.94 ± 23.25 | - 0.06 [−0.26; 0.37] 0.02 [−0.27; 0.31] | - 0.724 0.896 | - 0.25 [−0.01; 0.50] 0.07 [−0.21; 0.35] | - 0.060 0.617 | - 0.19 [−0.13; 0.51] 0.05 [−0.29; 0.39] | - 0.243 0.768 |
| Absenteeism | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 5.95 ± 14.33 - 6.81 ± 16.63 6.14 ± 16.27 | 5.46 ± 8.56 - 5.40 ± 13.01 3.59 ± 7.69 | 6.31 ± 11.99 - 6.02 ± 17.56 4.52 ± 10.79 | - 0.07 [−0.21; 0.34] 0.15 [−0.14; 0.44] | - 0.631 0.305 | - −0.01 [−0.27; 0.26] −0.06 [−0.27; 0.15] | - −0.962 0.588 | - −0.07 [−0.35; 0.20] −0.19 [−0.46; 0.09] | - 0.597 0.181 |
| Interoceptive Sensibility (BPQ) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 65.44 ± 18.68 - 66.81 ± 22.73 62.37 ± 22.46 | 60.20 ± 14.55 - 60.00 ± 19.10 61.17 ± 21.37 | 64.74 ± 18.16 - 60.89 ± 20.13 60.75 ± 19.06 | - 0.26 [0.01; 0.51] 0.05 [−0.19; 0.30] | - 0.039 0.666 | - 0.09 [−0.14; 0.33] 0.17 [−0.09; 0.43] | - 0.439 0.203 | - −0.17 [−0.43; 0.09] 0.12 [−0.18; 0.43] | - 0.191 0.424 |
| Self-efficacy (SES) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 26.40 ± 4,00 27.98 ± 3.82 28.81 ± 4.48 29.18 ± 4.90 | 25.67 ± 4.99 27.92 ± 4.17 29.16 ± 4.90 28.99 ± 5.09 | 25.74 ± 4.43 25.65 ± 4.30 25.79 ± 4.82 26.21 ± 5.15 | 0.45 [0.24; 0.66] 0.51 [0.29; 0.73] 0.48 [0.19; 0.76] | <0.001 <0.001 0.002 | 0.55 [0.33; 0.76] 0.69 [0.46; 0.92] 0.54 [0.23; 0.85] | <0.001 <0.001 0.001 | 0.09 [−0.14; 0.31] 0.17 [−0.07; 0.40] 0.05 [−0.27; 0.38] | 0.441 0.156 0.740 |
| Cognitive Fusion (CFQ-D) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 31.67 ± 8.28 28.71 ± 8.24 26.36 ± 8.44 24.69 ± 8.54 | 32.66 ± 7.29 27.89 ± 8.37 26.13 ± 8.43 24.38 ± 8.33 | 31.63 ± 8.20 30.33 ± 8.50 30.58 ± 8.62 29.24 ± 9.34 | −0.20 [−0.42; 0.03] −0.49 [−0.70; −0.28] −0.51 [−0.76; −0.26] | 0.083 <0.001 <0.001 | −0.38 [−0.59; −0.17] −0.60 [−0.81; −0.38] −0.62 [−0.86; −0.39] | <0.001 <0.001 <0.001 | −0.18 [−0.40; 0.04] −0.10 [−0.32; 0.12] −0.11 [−0.39; 0.17] | 0.108 0.376 0.443 |
| Alexithymia (TAS-20) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 49.98 ± 11.20 47.33 ± 10.58 45.70 ± 10.63 44.73 ± 11.47 | 50.67 ± 11.83 46.86 ± 10.22 44.45 ± 10.34 43.77 ± 11.25 | 48.50 ± 11.67 48.16 ± 11.29 47.77 ± 11.30 47.05 ± 11.58 | −0.18 [−0.36; −0.01] −0.30 [−0.47; −0.12] −0.30 [−0.52; −0.08] | 0.043 0.001 0.009 | −0.27 [−0.44; −0.09] −0.45 [−0.63; −0.27] −0.42 [−0.64; −0.20] | 0.003 <0.001 <0.001 | −0.09 [−0.28; 0.11] −0.16 [−0.34; 0.03] −0.13 [−0.36; 0.11] | 0.368 0.094 0.280 |
| Emotion Regulation–Expressive Suppression (ERQ–SP) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 14.95 ± 5.24 14.88 ± 4.76 14.07 ± 5.19 13.65 ± 5.13 | 14.26 ± 4.94 13.92 ± 4.59 13.25 ± 4.65 13.40 ± 4.79 | 14.53 ± 5.34 15.04 5.23 14.94 ± 5.58 14.96 ± 5.52 | −0.08 [−0.31; 0.14] −0.22 [−0.45; 0.01] −0.30 [−0.53; −0.07] | 0.468 0.059 0.012 | −0.19 [−0.41; 0.026] −0.29 [−0.52; −0.09] −0.27 [−0.53; −0.01] | 0.083 0.015 0.044 | −0.12 [−0.33; 0.10] −0.08 [−0.32; 0.15] 0.02 [−0.27; 0.31] | 0.289 0.481 0.894 |
| Emotion Regulation–Cognitive Reappraisal (ERQ–RE) | |||||||||
| Baseline 4 weeks 8 weeks 6 months | 23.98 ± 6.05 25.73 ± 5.67 27.97 ± 5.86 28.19 ± 6.57 | 22.78 ± 7.02 25.18 ± 6.08 26.87 ± 6.34 27.51 ± 7.03 | 27.61 ± 6.07 23.70 ± 6.33 24.19 ± 6.82 24.65 ± 6.69 | 0.33 [0.10; 0.55] 0.57 [0.31; 0.84] 0.51 [0.19; 0.82] | 0.005 <0.001 0.002 | 0.35 [0.12; 0.57] 0.50 [0.23; 0.77] 0.48 [0.15; 0.82] | 0.003 <0.001 0.005 | 0.01 [−0.23; 0.25] −0.09 [−0.40; 0.23] −0.02 [−0.36; 0.32] | 0.943 0.581 0.908 |
3.4. Mindfulness Reliable Improvement
| Variable | UG vs. WL | GoD vs. WL | UG vs. GoD |
|---|---|---|---|
| Mindfulness (FMI) | |||
| 4 weeks 8 weeks 6 months | 0.76 [0.51; 1.02] 1.06 [0.80; 1.32] 0.87 [0.61; 1.13] | 0.75 [0.50; 1.00] 0.91 [0.66; 1.17] 1.03 [0.77; 1.29] | −0.03 [−0.28; 0.21] −0.13 [−0.37; 0.11] 0.15 [−0.09; 0.39] |
| Depression (PHQ-9) | |||
| 4 weeks 8 weeks 6 months | −0.22 [−0.47; 0.02] −0.33 [−0.58; −0.08] −0.31 [−0.56; −0.07] | −0.25 [−0.49; −0.00] −0.44 [−0.68; −0.19] −0.39 [−0.64; −0.14] | −0.03 [−0.27; 0.22] −0.09 [−0.33; 0.15] −0.08 [−0.32; 0.17] |
| Anxiety (GAD-7) | |||
| 4 weeks 8 weeks 6 months | −0.27 [−0.51; −0.02] −0.41 [−0.66; −0.16] −0.41 [−0.66; −0.16] | −0.41 [−0.65; −0.16] −0.52 [−0.77; −0.27] −0.61 [−0.86; −0.36] | −0.14 [−0.39; 0.10] −0.12 [−0.37; 0.12] −0.22 [−0.46; 0.03] |
| Stress (PSS-4) | |||
| 4 weeks 8 weeks 6 months | −0.36 [−0.61; −0.11] −0.32 [−0.56; −0.07] −0.24 [−0.49; 0.00] | −0.48 [−0.72; −0.23] −0.63 [−0.88; −0.37] −0.48 [−0.73; −0.23] | −0.11 [−0.36; 0.13] −0.29 [−0.54; −0.05] −0.29 [−0.47; 0.02] |
| Well-being (WHO-5) | |||
| 4 weeks 8 weeks 6 months | 0.18; [−0.07; 0.42] 0.40 [0.15; 0.65] 0.40 [0.15; 0.65] | 0.55 [0.30; 0.79] 0.53 [0.28; 0.78] 0.35 [0.10; 0.60] | 0.37 [0.12; 0.61] 0.13 [−0.12; 0.37] −0.05 [−0.30; 0.19] |
| Presenteeism (SPS) | |||
| 4 weeks 8 weeks 6 months | - −0.09 [−0.34; 0.15] −0.06 [−0.31; 0.18] | - 0.03 [−0.21; 0.28] −0.15 [−0.40; 0.10] | - 0.12 [−0.12; 0.37] −0.09 [−0.34; 0.15] |
| Work Output | |||
| 4 weeks 8 weeks 6 months | - −0.06 [0.18; 0.31] 0.03 [−0.22; 0.27] | - 0.25 [0.00; 0.49] 0.07 [−0.18; 0.31] | - −0.18 [−0.42; 0.064] −0.04 [−0.28; 0.20] |
| Absenteeism | |||
| 4 weeks 8 weeks 6 months | - 0.05 [−0.20; 0.29] 0.12 [−0.13; 0.36] | - −0.04 [−0.29; 0.20] −0.10 [−0.35; 0.14] | - 0.10 [−0.15; 0.34] 0.21 [−0.03; 0.46] |
| Interoceptive Sensibility (BPQ) | |||
| 4 weeks 8 weeks 6 months | - 0.28 [0.03; 0.52] 0.08 [−0.17; 0.32] | - −0.05 [−0.29; 0.20] 0.02 [−0.22; 0.27] | - −0.33 [−0.57; −0.08] −0.05 [−0.30; 0.19] |
| Self-efficacy (SES) | |||
| 4 weeks 8 weeks 6 months | 0.57 [0.32; 0.82] 0.65 [0.40; 0.90] 0.59 [0.34; 0.84] | 0.54 [0.29; 0.78] 0.69 [0.44; 0.94] 0.54 [0.29; 0.79] | −0.02 [−0.26; 0.23] 0.07 [−0.17; 0.32] −0.04 [−0.28; 0.21] |
| Cognitive Fusion (CFQ-D) | |||
| 4 weeks 8 weeks 6 months | −0.19 [−0.44; 0.052] −0.49 [−0.74; −0.25] −0.51 [−0.76; −0.26] | −0.29 [−0.54; −0.04] −0.52 [−0.77; −0.27] −0.55 [−0.80; −0.30] | −0.10 [−0.34; 0.14] −0.03 [−0.27; 0.22] −0.04 [−0.28; 0.21] |
| Alexithymia (TAS-20) | |||
| 4 weeks 8 weeks 6 months | −0.08 [−0.32; 0.17] −0.19 [−0.43; 0.06] −0.20 [−0.45; 0.04] | −0.12 [−0.37; 0.12] −0.31 [−0.55; −0.06] −0.29 [−0.53; −0.04] | −0.05 [−0.29; 0.20] −0.12 [−0.36; 0.12] −0.08 [−0.33; 0.16] |
| Emotion Regulation–Expressive Suppression (ERQ–SP) | |||
| 4 weeks 8 weeks 6 months | −0.03 [−0.28; 0.21] −0.16 [−0.41; 0.08] −0.25 [−0.49; 0.00] | −0.23 [−0.47; 0.02] −0.33 [−0.58; −0.08] −0.30 [−0.55; −0.06] | −0.21 [−0.45; 0.04] −0.17 [−0.41; 0.078] −0.05 [−0.29; 0.19] |
| Emotion Regulation–Cognitive Reappraisal (ERQ–RE) | |||
| 4 weeks 8 weeks 6 weeks | 0.34 [0.09; 0.58] 0.60 [0.34; 0.85] 0.53 [0.28; 0.78] | 0.24 [−0.01; 0.48] 0.41 [0.16; 0.65] 0.42 [0.17; 0.66] | −0.09 [−0.34; 0.15] −0.18 [−0.42; 0.06] −0.10 [−0.34; 0.14] |
3.5. Per-Protocol Analyses
3.6. Intervention Adherence and Satisfaction
3.7. Negative Intervention Effects
3.8. Additional Exploratory Analyses
| Variable | n | M (SD) | |
|---|---|---|---|
| Mindfulness practice days per week * | IG1 | 64 | 3.13 (1.77) |
| IG2 | 71 | 3.58 (1.70) | |
| Average minutes per mindfulness practice day * | IG1 | 68 | 9.18 (22.17) |
| IG2 | 71 | 16.41 (25.41) | |
| Number of modules completed | IG1 | 129 | 2.52 (2.09) |
| IG2 | 130 | 3.07 (2.32) | |
| Number of e-coach contacts (all) | IG2 | 130 | 0.28 (0.98) |
| Number of e-coach contacts (at least one e-coach contact) | IG2 | 20 | 1.85 (1.87) |
| n | N (%) | ||
| SMS-coach signup | IG1 | 129 | 49 (38.0) |
| IG2 | 130 | 56 (43.1) | |
| At least one e-Coach contact | IG2 | 130 | 20 (15.4) |
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACT | Acceptance commitment therapy |
| CBT | Cognitive behavioral therapy |
| CONSORT | Consolidated Standards of Reporting Trials |
| GoD | Guidance on demand |
| ICBT | Internet-based cognitive behavioral therapy |
| IMI | Internet- and mobile-based intervention |
| ITT | Intention-to-treat |
| MBSR | Mindfulness-based stress reduction |
| RCT | Randomized controlled trial |
| StudiCare-M | StudiCare Mindfulness |
| TAU | Treatment as usual |
| UG | Unguided |
| WHO | World Health Organization |
| WL | Waitlist control group |
References
- Arnett, J.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef] [PubMed]
- American College Health Association. American College Health Association-National College Health Assessment III: Reference Group Executive Summary Spring 2022; American College Health Association: Silver Spring, MD, USA, 2022. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Auerbach, R.P.; Mortier, P.; Bruffaerts, R.; Alonso, J.; Benjet, C.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; Green, J.G.; Hasking, P.; et al. WHO World Mental Health Surveys International College Student Project: Prevalence and distribution of mental disorders. J. Abnorm. Psychol. 2018, 127, 623–638. [Google Scholar] [CrossRef]
- Bruffaerts, R.; Mortier, P.; Kiekens, G.; Auerbach, R.P.; Cuijpers, P.; Demyttenaere, K.; Green, J.G.; Nock, M.K.; Kessler, R.C. Mental health problems in college freshmen: Prevalence and academic functioning. J. Affect Disord. 2018, 225, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Mortier, P.; Kaehlke, F.; Bruffaerts, R.; Baumeister, H.; Auerbach, R.P.; Alonso, J.; Vilagut, G.; Martínez, K.U.; Lochner, C.; et al. Barriers of mental health treatment utilization among first-year college students: First cross-national results from the WHO World Mental Health International College Student Initiative. Int. J. Methods Psychiatr Res. 2019, 28, e1782. [Google Scholar] [CrossRef] [PubMed]
- Bruffaerts, R.; Mortier, P.; Auerbach, R.P.; Alonso, J.; Hermosillo De la Torre, A.E.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; Green, J.G.; Hasking, P.; et al. Lifetime and 12-month treatment for mental disorders and suicidal thoughts and behaviors among first year college students. Int. J. Methods Psychiatr. Res. 2019, 28, e1764. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Cuijpers, P.; Muñoz, R.F.; Baumeister, H. Prevention of mental health disorders using internet- and mobile-based interventions: A narrative review and recommendations for future research. Front. Psychiatry 2017, 8, 1–16. [Google Scholar] [CrossRef]
- Pedrelli, P.; Nyer, M.; Yeung, A.; Zulauf, C.; Wilens, T. College students: Mental health problems and treatment considerations. Acad. Psychiatry 2015, 39, 503–511. [Google Scholar] [CrossRef]
- Ryan, M.L.; Shochet, I.M.; Stallman, H.M. Universal online interventions might engage psychologically distressed university students who are unlikely to seek formal help. Adv. Ment. Health 2010, 9, 73–83. [Google Scholar] [CrossRef]
- Harrer, M.; Adam, S.H.; Baumeister, H.; Cuijpers, P.; Karyotaki, E.; Auerbach, R.P.; Kessler, R.C.; Bruffaerts, R.; Berking, M.; Ebert, D.D. Internet interventions for mental health in university students: A systematic review and meta-analysis. Int. J. Methods Psychiatr. Res. 2019, 28, e1759. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen Hosp Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Hayes, S.C. Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behav. Ther. 2004, 35, 639–665. [Google Scholar] [CrossRef]
- Jayewardene, W.P.; Lohrmann, D.K.; Erbe, R.G.; Torabi, M.R. Effects of preventive online mindfulness interventions on stress and mindfulness: A meta-analysis of randomized controlled trials. Prev. Med. Rep. 2017, 5, 150–159. [Google Scholar] [CrossRef]
- Sommers-Spijkerman, M.; Austin, J.; Bohlmeijer, E.; Pots, W. New evidence in the booming field of online mindfulness: An updated meta-analysis of randomized controlled trials. JMIR Ment. Health 2021, 8, e28168. [Google Scholar] [CrossRef]
- Dawson, A.F.; Brown, W.W.; Anderson, J.; Datta, B.; Donald, J.N.; Hong, K.; Allan, S.; Mole, T.B.; Jones, P.B.; Galante, J. Mindfulness-Based Interventions for University Students: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Appl. Psychol. Health Well-Being. 2020, 12, 384–410. [Google Scholar] [CrossRef]
- Küchler, A.M.; Kählke, F.; Vollbrecht, D.; Peip, K.; Ebert, D.D.; Baumeister, H. Effectiveness, acceptability, and mechanisms of change of the internet-based intervention StudiCare Mindfulness for college students: A randomized controlled trial. Mindfulness 2022, 13, 2140–2154. [Google Scholar] [CrossRef]
- Baumeister, H.; Reichler, L.; Munzinger, M.; Lin, J. The impact of guidance on internet-based mental health interventions—A systematic review. Internet Interv. 2014, 1, 205–215. [Google Scholar] [CrossRef]
- Spijkerman, M.P.J.; Pots, W.T.M.; Bohlmeijer, E.T. Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clin. Psychol. Rev. 2016, 45, 102–114. [Google Scholar] [CrossRef]
- Kelders, S.M.; Kok, R.N.; Ossebaard, H.C.; van Gemert-Pijnen, J.E.W.C. Persuasive system design does matter: A systematic review of adherence to web-based interventions. J. Med. Internet Res. 2012, 14, e152. [Google Scholar] [CrossRef]
- Winter, N.; Russell, L.; Ugalde, A.; White, V.; Livingston, P. Engagement strategies to improve adherence and retention in web-based mindfulness programs: Systematic review. J. Med. Internet Res. 2022, 24, e30026. [Google Scholar] [CrossRef]
- Berger, T.; Caspar, F.; Richardson, R.; Kneubühler, B.; Sutter, D.; Andersson, G. Internet-based treatment of social phobia: A randomized controlled trial comparing unguided with two types of guided self-help. Behav. Res. Ther. 2011, 49, 158–169. [Google Scholar] [CrossRef]
- Rheker, J.; Andersson, G.; Weise, C. The role of “on demand” therapist guidance vs. no support in the treatment of tinnitus via the internet: A randomized controlled trial. Internet Interv. 2015, 2, 189–199. [Google Scholar] [CrossRef]
- Hennemann, S.; Böhme, K.; Baumeister, H.; Bendig, E.; Kleinstäuber, M.; Ebert, D.D.; Witthöft, M. Efficacy of a guided internet-based intervention (iSOMA) for somatic symptoms and related distress in university students: Study protocol of a randomised controlled trial. BMJ Open 2018, 8, e024929. [Google Scholar] [CrossRef] [PubMed]
- Rozental, A.; Andersson, G.; Boettcher, J.; Ebert, D.D.; Cuijpers, P.; Knaevelsrud, C.; Ljótsson, B.; Kaldo, V.; Titov, N.; Carlbring, P. Consensus statement on defining and measuring negative effects of Internet interventions. Internet Interv. 2014, 1, 12–19. [Google Scholar] [CrossRef]
- van Dam, N.T.; van Vugt, M.K.; Vago, D.R.; Schmalzl, L.; Saron, C.D.; Olendzki, A.; Meissner, T.; Lazar, S.W.; Kerr, C.E.; Gorchov, J.; et al. Mind the hype: A critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspect. Psychol. Sci. 2018, 13, 36–61. [Google Scholar] [CrossRef]
- Britton, W.B.; Lindahl, J.R.; Cooper, D.J.; Canby, N.K.; Palitsky, R. Defining and measuring meditation-related adverse effects in mindfulness-based programs. Clin. Psychol. Sci. 2021, 9, 1185–1204. [Google Scholar] [CrossRef]
- Harrer, M.; Adam, S.H.; Fleischmann, R.J.; Baumeister, H.; Auerbach, R.; Bruffaerts, R.; Cuijpers, P.; Kessler, R.C.; Berking, M.; Lehr, D.; et al. Effectiveness of an internet- and app-based intervention for college students with elevated stress: Randomized controlled trial. J. Med. Internet Res. 2018, 20, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, R.J.; Harrer, M.; Zarski, A.C.; Baumeister, H.; Lehr, D.; Ebert, D.D. Patients’ experiences in a guided internet- and app-based stress intervention for college students: A qualitative study. Internet Interv. 2018, 12, 130–140. [Google Scholar] [CrossRef]
- Kählke, F.; Berger, T.; Schulz, A.; Baumeister, H.; Berking, M.; Auerbach, R.P.; Bruffaerts, R.; Cuijpers, P.; Kessler, R.C.; Ebert, D.D. Efficacy of an unguided internet-based self-help intervention for social anxiety disorder in university students: A randomized controlled trial. Int. J. Methods Psychiatr. Res. 2019, 28, e1766. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, 698–702. [Google Scholar] [CrossRef]
- Küchler, A.M.; Schultchen, D.; Pollatos, O.; Moshagen, M.; Ebert, D.D.; Baumeister, H. StudiCare mindfulness—Study protocol of a randomized controlled trial evaluating an internet- and mobile-based intervention for college students with no and “on demand” guidance. Trials 2020, 21, 975. [Google Scholar] [CrossRef] [PubMed]
- Walach, H.; Buchheld, N.; Buttenmüller, V.; Kleinknecht, N.; Schmidt, S. Measuring mindfulness—The Freiburg Mindfulness Inventory (FMI). Pers. Individ. Dif. 2006, 40, 1543–1555. [Google Scholar] [CrossRef]
- Schultchen, D.; Küchler, A.M.; Schillings, C.; Weineck, F.; Karabatsiakis, A.; Ebert, D.D.; Baumeister, H.; Pollatos, O. Effectiveness of a guided online mindfulness-focused intervention in a student population: Study protocol for a randomised control trial. BMJ Open 2020, 10, e032775. [Google Scholar] [CrossRef] [PubMed]
- Sealed Envelope Ltd. Create a Blocked Randomisation List. 2019. Available online: https://www.sealedenvelope.com/ (accessed on 6 June 2019).
- Kaluza, G. Stressbewältigung; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Heidenreich, T.; Ströhle, G.; Michalak, J. Achtsamkeit: Konzeptuelle Aspekte und Ergebnisse zum Freiburger Achtsamkeitsfragebogen. Verhaltenstherapie 2006, 16, 33–40. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef]
- Cohen, S.; Williamson, G. Perceived stress in a probability sample of the United States. In The Social Psychology of Health; Spacapan, S., Oskamp, S., Eds.; Sage Publications: Newbury Park, CA, USA, 1988; pp. 31–68. [Google Scholar]
- Warttig, S.L.; Forshaw, M.J.; South, J.; White, A.K. New, normative, English-sample data for the Short Form Perceived Stress Scale (PSS-4). J. Health Psychol. 2013, 18, 1617–1628. [Google Scholar] [CrossRef]
- World Health Organization, Regional Office for Europe P, Unit R. World Health Organization info Package: Mastering Depression in Primary Care; Frederiksborg: Hillerod, DK, USA, 1998.
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, M.; Adachi, H.; Arakida, M.; Namura, I.; Takahashi, Y.; Miyata, M.; Kumano-go, T.; Yamamura, S.; Shigedo, Y.; Suganuma, N.; et al. Presenteeism in college students: Reliability and validity of the presenteeism scale for students. Qual. Life Res. 2011, 20, 439–446. [Google Scholar] [CrossRef]
- Porges, S. Body Perception Questionnaire; Laboratory of Development Assessment, University of Maryland: College Park, MD, USA, 1993. [Google Scholar]
- Cabrera, A.; Kolacz, J.; Pailhez, G.; Bulbena-Cabre, A.; Bulbena, A.; Porges, S.W. Assessing body awareness and autonomic reactivity: Factor structure and psychometric properties of the Body Perception Questionnaire-Short Form (BPQ-SF). Int. J. Methods Psychiatr. Res. 2018, 27, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Jerusalem, M. Generalized Self-Efficacy scale. In Measures in Health Psychology: A User’s Portfolio Causal and Control Beliefs; Weinman, J., Wright, S., Johnston, M., Eds.; NFER-Nelson: London, UK, 1995; pp. 35–37. [Google Scholar]
- Schwarzer, R.; Mueller, J.; Greenglass, E. Assessment of perceived general self-efficacy on the internet: Data collection in cyberspace. Anxiety Stress Coping 1999, 12, 145–161. [Google Scholar] [CrossRef]
- China, C.; Hansen, L.B.; Gillanders, D.T.; Benninghoven, D. Concept and validation of the german version of the Cognitive Fusion Questionnaire (CFQ-D). J. Contextual Behav. Sci. 2018, 9, 30–35. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Pers. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef]
- Abler, B.; Kessler, H. Emotion Regulation Questionnaire—Eine deutschsprachige Fassung des ERQ von Gross und John. Diagnostica 2009, 55, 144–152. [Google Scholar] [CrossRef]
- Bagby, R.M.; Parker, J.D.A.; Taylor, G.J. The twenty-item Toronto Alexithymia scale—I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Kupfer, J.; Brosig, B.; Brähler, E. Toronto-Alexithymie-Skala-20 (TAS-20); Hogrefe: Göttingen, Germany, 2001. [Google Scholar]
- Parker, J.D.A.; Taylor, G.J.; Bagby, R.M. The 20-Item Toronto Alexithymia Scale: III. Reliability and factorial validity in a community population. J. Psychosom. Res. 2003, 55, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Ladwig, I.; Rief, W.; Nestoriuc, Y. Welche Risiken und Nebenwirkungen hat Psychotherapie?—Entwicklung des Inventars zur Erfassung Negativer Effekte von Psychotherapie (INEP). Verhaltenstherapie 2014, 24, 252–263. [Google Scholar] [CrossRef]
- Boß, L.; Lehr, D.; Reis, D.; Vis, C.; Riper, H.; Berking, M.; Ebert, D.D. Reliability and validity of assessing user satisfaction with web-based health interventions. J. Med. Internet Res. 2016, 18, 1–13. [Google Scholar] [CrossRef]
- Kriz, D.; Nübling, R.; Steffanowski, A.; Rieger, J.; Schmidt, J. Patientenzufriedenheit: Psychometrische Reanalyse des ZUF-8. DRV-Schriften 2008, 77, 84–85. [Google Scholar]
- Devilly, G.J.; Borkovec, T.D. Psychometric properties of the credibility/expectancy questionnaire. J. Behav. Ther. Exp. Psychiatry 2000, 31, 73–86. [Google Scholar] [CrossRef]
- Kazdin, A.E. Therapy outcome questions requiring control of credibility and treatment-generated expectancies. Behav. Ther. 1979, 10, 81–93. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 28.0; IBM Corp: Armonk, NY, USA, 2022.
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- van Buuren, S.; Groothuis-Oudshoorn, K. MICE: Multivariate imputation by chained equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Enders, C.K. Applied Missing Data Analysis; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Little, R.J.A. Missing-data adjustments in large surveys. J. Bus. Econ. Stat. 1988, 6, 287–296. [Google Scholar]
- Rubin, D.B. Multiple imputation after 18+ years. J. Am. Stat. Assoc. 1996, 91, 473–489. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum: Mahwah, NJ, USA, 1988. [Google Scholar]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; van Daele, T.; Nordgreen, T.; Karekla, M.; Compare, A.; Zarbo, C.; Brugnera, A.; Øverland, S.; Trebbi, G.; Jensen, K.; et al. Internet- and mobile-based psychological interventions: Applications, efficacy, and potential for improving mental health: A report of the EFPA e-health taskforce. Eur. Psychol. 2018, 23, 167–187. [Google Scholar] [CrossRef]
- Lamers, S.M.A.; Westerhof, G.J.; Glas, C.A.W.; Bohlmeijer, E.T. The bidirectional relation between positive mental health and psychopathology in a longitudinal representative panel study. J. Posit. Psychol. 2015, 10, 553–560. [Google Scholar] [CrossRef]
- Wood, A.M.; Joseph, S. The absence of positive psychological (eudemonic) well-being as a risk factor for depression: A ten year cohort study. J. Affect Disord. 2010, 122, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L.M.; Dhingra, S.S.; Simoes, E.J. Change in level of positive mental health as a predictor of future risk of mental illness. Am. J. Public Health 2010, 100, 2366–2371. [Google Scholar] [CrossRef]
- Saddichha, S.; Al-Desouki, M.; Lamia, A.; Linden, I.A.; Krausz, M. Online interventions for depression and anxiety—A systematic review. Health Psychol. Behav. Med. 2014, 2, 841–881. [Google Scholar] [CrossRef]
- Dour, H.J.; Wiley, J.F.; Roy-Byrne, P.; Stein, M.B.; Sullivan, G.; Sherbourne, C.D.; Bystritsky, A.; Rose, R.D.; Craske, M.G. Perceived social support mediates anxiety and depressive symptom changes following primaray care intervention. Depress. Anxiety 2014, 31, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Baier, A.L.; Kline, A.C.; Feeny, N.C. Therapeutic alliance as a mediator of change: A systematic review and evaluation of research. Clin. Psychol.Rev. 2020, 82, 101921. [Google Scholar] [CrossRef]
- Domhardt, M.; Cuijpers, P.; Ebert, D.D.; Baumeister, H. More Light? Opportunities and Pitfalls in Digitalized Psychotherapy Process Research. Front. Psychol. 2021, 19, 544129. [Google Scholar] [CrossRef]
- Räsänen, P.; Lappalainen, P.; Muotka, J.; Tolvanen, A.; Lappalainen, R. An online guided ACT intervention for enhancing the psychological wellbeing of university students: A randomized controlled clinical trial. Behav. Res. Ther. 2016, 78, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Simon, G.E.; Imel, Z.E.; Ludman, E.J.; Steinfeld, B.J. Is dropout after a first psychotherapy visit always a bad outcome? Psychiatr. Serv. 2012, 63, 705–707. [Google Scholar] [CrossRef] [PubMed]
- Beintner, I.; Vollert, B.; Zarski, A.C.; Bolinski, F.; Musiat, P.; Görlich, D.; Ebert, D.D.; Jacobi, C. Adherence reporting in randomized controlled trials examining manualized multisession online interventions: Systematic review of practices and proposal for reporting standards. J. Med. Internet Res. 2019, 21, e14181. [Google Scholar] [CrossRef]
- Papa, A.; Follette, W.C. Dismantling studies of psychotherapy. In The Encyclopedia of Clinical Psychology, 1st ed.; Cautin, R.L., Lilienfeld, S.O., Eds.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2015; pp. 1–6. [Google Scholar]
- Domhardt, M.; Steubl, L.; Boettcher, J.; Buntrock, C.; Karyotaki, E.; Ebert, D.D.; Cuijpers, P.; Baumeister, H. Mediators and mechanisms of change in internet- and mobile-based interventions for depression: A systematic review. Clin. Psychol. Rev. 2021, 83, 101953. [Google Scholar] [CrossRef]
- Bendig, E.; Erb, B.; Meißner, D.; Bauereiß, N.; Baumeister, H. Feasibility of a Software agent providing a brief Intervention for Self-help to Uplift psychological wellbeing (“SISU”). A single-group pretest-posttest trial investigating the potential of SISU to act as therapeutic agent. Internet Interv. 2021, 24, 100377. [Google Scholar] [CrossRef]
- Borghouts, J.; Eikey, E.; Mark, G.; de Leon, C.; Schueller, S.M.; Schneider, M.; Stadnick, N.; Zheng, K.; Mukamel, D.; Sorkin, D. Barriers to and facilitators of user engagement with digital mental health interventions: Systematic review. J. Med. Internet Res. 2021, 23, e24387. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.A.; Noma, H.; Caldwell, D.M.; Honyashiki, M.; Shinohara, K.; Imai, H.; Chen, P.; Hunot, V.; Churchill, R. Waiting list may be a nocebo condition in psychotherapy trials: A contribution from network meta-analysis. Acta Psychiatr. Scand. 2014, 130, 181–192. [Google Scholar] [CrossRef]
- Nederhof, A.J. Methods of coping with social desirability bias: A review. Eur. J. Soc. Psychol. 1985, 15, 263–280. [Google Scholar] [CrossRef]


| Module | Aims and Content | Examples of Exercises and Assignments |
|---|---|---|
| 1. Being in the here and now | Introducing the concept of mindfulness | Reviewing most and least mindful moments of the day; “body scan” meditation; taking a mindful walk |
| 2. Mindful body perception | Practicing awareness of body signals | Testing one’s heartbeat perception; practicing “heart meditation”; mindful eating and drinking |
| 3. A new perspective on stress | Distancing oneself from stress-inducing thoughts | Identifying former ways of coping with stress; learning techniques to challenge automatic thoughts; “mindful perception of body posture” meditation |
| 4. Developing beneficial thoughts | Getting to know beneficial ways of thinking | Identifying one’s “stress patterns” and developing and internalizing beneficial thoughts; “mindful breathing” meditation |
| 5. What makes your life valuable? | Identifying one’s values and pursuing one’s goals | Writing a speech for one’s 70th birthday; setting and pursuing goals with the SMART technique; variation of “body scan” meditation |
| 6. Being mindful towards yourself | Learning how to appreciatively accept one’s personality traits | Exercise to identify different personality traits and corresponding automatic reactions; learning to accept and appreciate all personality traits; “loving kindness” meditation |
| 7. Training your body and senses | Exercising the ability to enjoy and getting acquainted with the practice of yoga | Mindful chocolate eating exercise; mindful yoga exercises |
| Booster 1 (4 weeks after completion of module 7) | Repeating module 1 to 3 and mindfulness exercises | Choosing favorite mindfulness exercises; setting goals for their implementation in the coming weeks |
| Booster 2 (12 weeks after completion of module 7) | Repeating modules 4 to 7 and ensuring long-term integration of mindfulness into daily life | Reviewing pursuit of goals in the last two months; identifying potential barriers and developing solutions |
| All (N = 386) | UG (n = 129) | GoD (n = 130) | WL (n = 127) | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | n | % | n | % | n | % | |
| Sociodemographic characteristics | ||||||||
| Age (M, SD) | 29.85 | 4.80 | 25.99 | 5.26 | 25.46 | 5.07 | ||
| Female gender | 289 | 74.9 | 92 | 71.3 | 102 | 78.5 | 95 | 74.8 |
| Single | 255 | 66.1 | 85 | 65.9 | 91 | 70.0 | 79 | 62.6 |
| German citizenship | 310 | 80.3 | 102 | 79.1 | 103 | 79.2 | 105 | 82.7 |
| Study characteristics | ||||||||
| Full-time student | 317 | 82.1 | 103 | 79.8 | 113 | 86.9 | 101 | 79.5 |
| Number of total semesters (M, SD) | 9.05 | 5.39 | 9.60 | 5.80 | 8.4 | 4.6 | 9.14 | 5.66 |
| Study subject | ||||||||
| Psychology | 51 | 13.2 | 18 | 14.0 | 18 | 13.8 | 15 | 11.8 |
| Medicine and health | 71 | 18.4 | 20 | 15.5 | 26 | 20.0 | 25 | 19.7 |
| Business and law | 45 | 11.7 | 16 | 12.4 | 14 | 10.8 | 15 | 11.8 |
| Educational sciences | 59 | 15.3 | 19 | 14.7 | 19 | 14.6 | 21 | 16.5 |
| Engineering | 36 | 9.3 | 18 | 14.0 | 11 | 8.5 | 7 | 5.5 |
| Linguistics and culture | 45 | 11.7 | 14 | 10.9 | 16 | 12.3 | 15 | 11.8 |
| Social sciences | 21 | 5.4 | 7 | 5.4 | 4 | 3.1 | 10 | 7.9 |
| Mathematics and other sciences | 56 | 14.5 | 17 | 13.2 | 21 | 16.2 | 18 | 14.2 |
| Others | 2 | 0.5 | 0 | 0 | 1 | 0.8 | 1 | 0.8 |
| Previous help seeking | ||||||||
| Psychotherapy experience | 89 | 23.1 | 23 | 17.8 | 28 | 21.5 | 38 | 30.7 |
| Mindfulness experience | 145 | 37.6 | 52 | 40.3 | 50 | 38.2 | 43 | 33.8 |
| CEQ: Treatment credibility (M, SD) | 20.36 | 3.78 | 20.47 | 3.80 | 20.06 | 3.89 | 20.56 | 3.66 |
| CEQ: Treatment expectancy (M, SD) | 18.15 | 4.04 | 18.24 | 4.27 | 17.98 | 3.69 | 18.24 | 4.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Küchler, A.-M.; Schultchen, D.; Dretzler, T.; Moshagen, M.; Ebert, D.D.; Baumeister, H. A Three-Armed Randomized Controlled Trial to Evaluate the Effectiveness, Acceptance, and Negative Effects of StudiCare Mindfulness, an Internet- and Mobile-Based Intervention for College Students with No and “On Demand” Guidance. Int. J. Environ. Res. Public Health 2023, 20, 3208. https://doi.org/10.3390/ijerph20043208
Küchler A-M, Schultchen D, Dretzler T, Moshagen M, Ebert DD, Baumeister H. A Three-Armed Randomized Controlled Trial to Evaluate the Effectiveness, Acceptance, and Negative Effects of StudiCare Mindfulness, an Internet- and Mobile-Based Intervention for College Students with No and “On Demand” Guidance. International Journal of Environmental Research and Public Health. 2023; 20(4):3208. https://doi.org/10.3390/ijerph20043208
Chicago/Turabian StyleKüchler, Ann-Marie, Dana Schultchen, Tim Dretzler, Morten Moshagen, David D. Ebert, and Harald Baumeister. 2023. "A Three-Armed Randomized Controlled Trial to Evaluate the Effectiveness, Acceptance, and Negative Effects of StudiCare Mindfulness, an Internet- and Mobile-Based Intervention for College Students with No and “On Demand” Guidance" International Journal of Environmental Research and Public Health 20, no. 4: 3208. https://doi.org/10.3390/ijerph20043208
APA StyleKüchler, A.-M., Schultchen, D., Dretzler, T., Moshagen, M., Ebert, D. D., & Baumeister, H. (2023). A Three-Armed Randomized Controlled Trial to Evaluate the Effectiveness, Acceptance, and Negative Effects of StudiCare Mindfulness, an Internet- and Mobile-Based Intervention for College Students with No and “On Demand” Guidance. International Journal of Environmental Research and Public Health, 20(4), 3208. https://doi.org/10.3390/ijerph20043208