
Driving Time to the Nearest Percutaneous Coronary Intervention-Capable Hospital and the Risk of Case Fatality in Patients with Acute Myocardial Infarction in Beijing

 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Population
2.3. Study Outcomes
2.4. Driving Time to the Nearest PCI-Capable Hospital
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
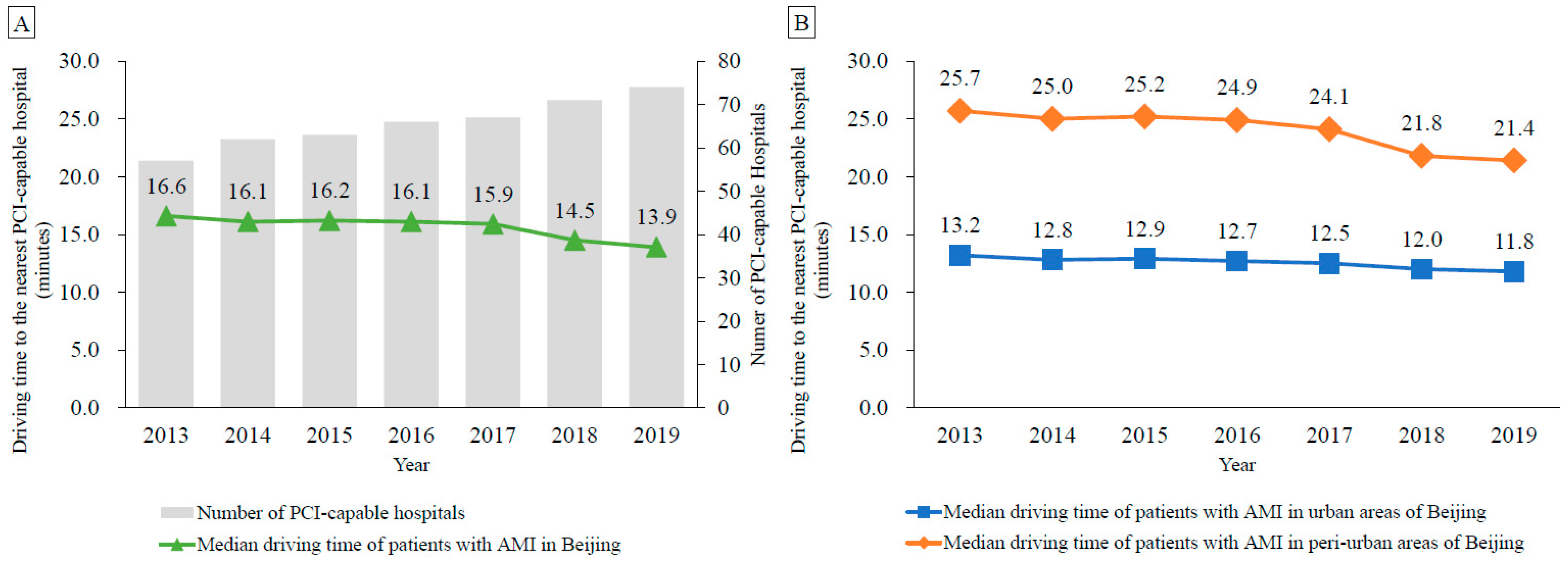
3.2. Driving Time to the Nearest PCI-Capable Hospital
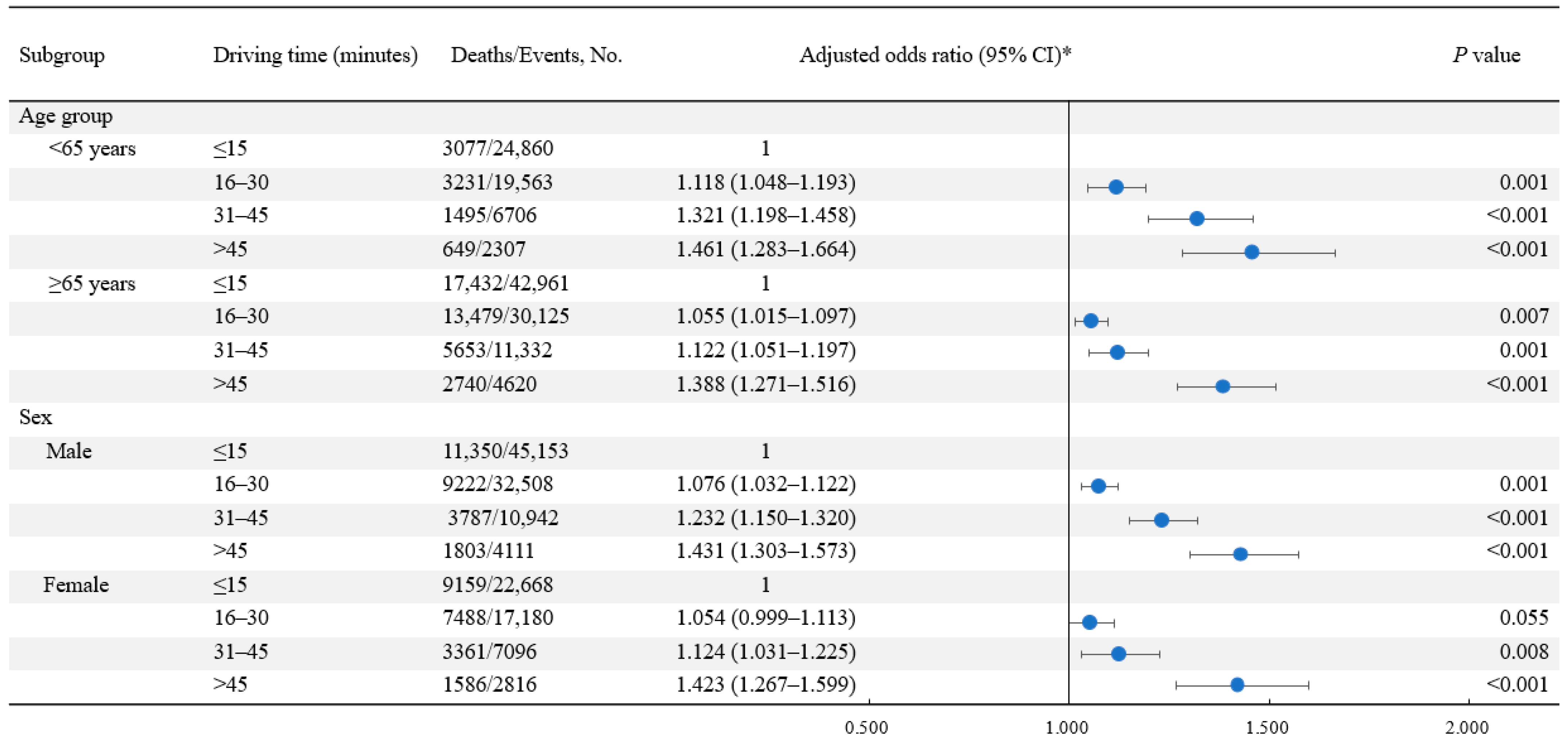
3.3. Association between Driving Time and the Risk of AMI Fatality
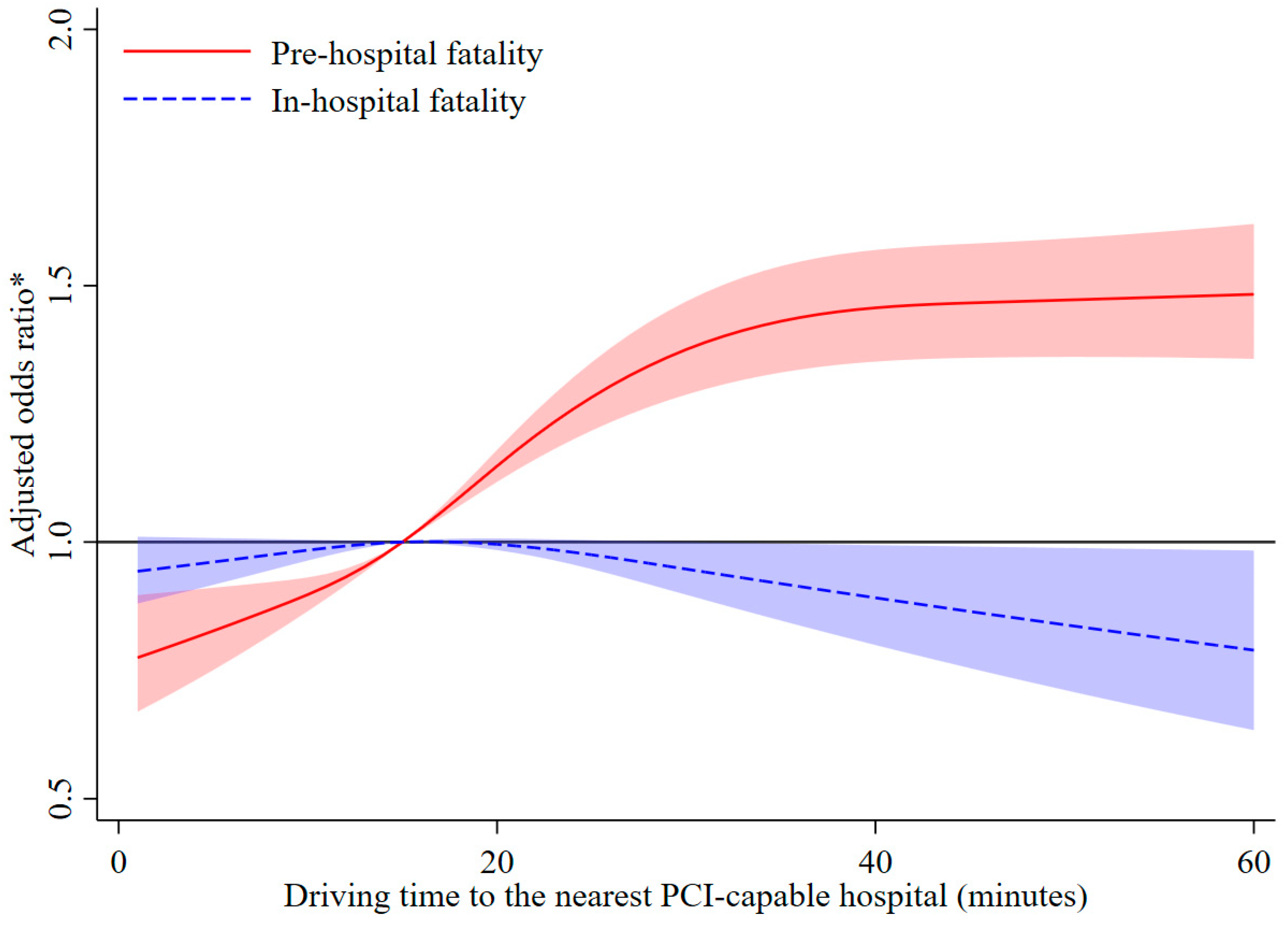
3.4. Association between Driving Time and the Risk of Pre-Hospital and In-Hospital AMI Fatality
3.5. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: A report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation 2022, 145, e18–e114. [Google Scholar] [CrossRef]
- De Luca, G.; Suryapranata, H.; Ottervanger, J.P.; Antman, E.M. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: Every minute of delay counts. Circulation 2004, 109, 1223–1225. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.Q.; Hao, Y.C.; Liu, J.; Yang, N.; Yang, Y.Q.; Sun, Z.Q.; Zhao, D.; Liu, J. Pre-hospital delay in patients with acute myocardial infarction in China: Findings from the Improving Care for Cardiovascular Disease in China-Acute Coronary Syndrome (CCC-ACS) project. J. Geriatr. Cardiol. 2022, 19, 276–283. [Google Scholar] [PubMed]
- Nilsson, G.; Mooe, T.; Söderström, L.; Samuelsson, E. Pre-hospital delay in patients with first time myocardial infarction: An observational study in a northern Swedish population. BMC Cardiovasc. Disord. 2016, 16, 93. [Google Scholar] [CrossRef]
- Alexandrescu, R.; Bottle, A.; Jarman, B.; Aylin, P. Impact of transfer for angioplasty and distance on AMI in-hospital mortality. Acute Card Care 2012, 14, 5–12. [Google Scholar] [CrossRef]
- Gregory, P.M.; Malka, E.S.; Kostis, J.B.; Wilson, A.C.; Arora, J.K.; Rhoads, G.G. Impact of geographic proximity to cardiac revascularization services on service utilization. Med. Care 2000, 38, 45–57. [Google Scholar] [CrossRef]
- Rhudy JPJr Alexandrov, A.W.; Hyrkäs, K.E.; Jablonski-Jaudon, R.A.; Pryor, E.R.; Wang, H.E.; Bakitas, M.A. Geographic access to interventional cardiology services in one rural state. Heart Lung 2016, 45, 434–440. [Google Scholar] [CrossRef]
- Graves, B.A. Access to cardiac interventional services in Alabama and Mississippi: A geographical information system analysis. Perspect. Health Inf. Manag. 2010, 7, 1b. [Google Scholar]
- Balamurugan, A.; Delongchamp, R.; Im, L.; Bates, J.; Mehta, J.L. Neighborhood and acute myocardial infarction mortality as related to the driving time to percutaneous coronary intervention-capable hospital. J. Am. Heart Assoc. 2016, 5, e002378. [Google Scholar] [CrossRef]
- Grey, C.; Jackson, R.; Schmidt, M.; Ezzati, M.; Asaria, P.; Exeter, D.J.; Kerr, A.J. One in four major ischaemic heart disease events are fatal and 60% are pre-hospital deaths: A national data-linkage study (ANZACS-QI 8). Eur. Heart J. 2017, 38, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Beijing Municipal Science & Technology Commission, Administration Commission of Zhongguancun Science Park. Beijing Technology Market Statistical Annual Report in 2019. Available online: http://kw.beijing.gov.cn/art/2020/12/8/art_6656_578808.html (accessed on 21 November 2022).
- Xie, W.; Li, G.; Zhao, D.; Xie, X.; Wei, Z.; Wang, W.; Wang, M.; Li, G.; Liu, W.; Sun, J.; et al. Relationship between fine particulate air pollution and is chaemic heart disease morbidity and mortality. Heart 2015, 101, 257–263. [Google Scholar] [CrossRef]
- Asaria, P.; Bennett, J.E.; Elliott, P.; Rashid, T.; Iyathooray Daby, H.; Douglass, M.; Francis, D.P.; Fecht, D.; Ezzati, M. Contributions of event rates, pre-hospital deaths, and deaths following hospitalisation to variations in myocardial infarction mortality in 326 districts in England: A spatial analysis of linked hospitalisation and mortality data. Lancet Public Health 2022, 7, e813–e824. [Google Scholar] [CrossRef]
- Liu, R.; Liu, X.; Yang, P.; Du, X.; He, L.; Chen, T.; Li, X.; Xie, G.; Wu, S.; Su, J.; et al. Influenza-associated cardiovascular mortality in older adults in Beijing, China: A population-based time-series study. BMJ Open 2020, 10, e042487. [Google Scholar] [CrossRef]
- Chen, J.; Normand, S.L.; Wang, Y.; Drye, E.E.; Schreiner, G.C.; Krumholz, H.M. Recent declines in hospitalizations for acute myocardial infarction for Medicare fee-for-service beneficiaries: Progress and continuing challenges. Circulation 2010, 121, 1322–1328. [Google Scholar] [CrossRef]
- Kulkarni, V.T.; Ross, J.S.; Wang, Y.; Nallamothu, B.K.; Spertus, J.A.; Normand, S.L.; Masoudi, F.A.; Krumholz, H.M. Regional density of cardiologists and rates of mortality for acute myocardial infarction and heart failure. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 352–359. [Google Scholar] [CrossRef]
- Nallamothu, B.K.; Bates, E.R.; Wang, Y.; Bradley, E.H.; Krumholz, H.M. Driving times and distances to hospitals with percutaneous coronary intervention in the United States: Implications for prehospital triage of patients with ST-elevation myocardial infarction. Circulation 2006, 113, 1189–1195. [Google Scholar] [CrossRef]
- Niu, Q.; Wang, Y.; Xia, Y.; Wu, H.; Tang, X. Detailed assessment of the spatial distribution of urban parks according to day and travel mode based on Web Mapping API: A case study of main parks in Wuhan. Int. J. Environ. Res. Public Health 2018, 15, 1725. [Google Scholar] [CrossRef]
- Amap. WebService API. Available online: https://lbs.amap.com/api/webservice/guide/api/georegeo#geo (accessed on 21 November 2022).
- Fabbian, F.; Bhatia, S.; De Giorgi, A.; Maietti, E.; Bhatia, S.; Shanbhag, A.; Deshmukh, A. Circadian periodicity of ischemic heart disease: A systematic review of the literature. Heart Fail. Clin. 2017, 13, 673–680. [Google Scholar] [CrossRef]
- Beijing Transport Institute. Beijing Transport Development Annual Report in 2021. Available online: https://www.bjtrc.org.cn/List/index/cid/7.html (accessed on 21 November 2022).
- Beijing Municipal Bureau of Statistics. Tabulation on the 2010 Population Census of Beijing Municipality. Available online: http://tjj.beijing.gov.cn/tjsj_31433/tjsk_31457/202003/t20200327_1740183.html (accessed on 21 November 2022).
- Beijing Municipal Bureau of Statistics. Beijing Regional Statistical Yearbook. Available online: http://nj.tjj.beijing.gov.cn/nj/qxnj/2021/zk/indexch.htm (accessed on 21 November 2022).
- Sun, J.W.; Wang, R.; Li, D.; Toh, S. Use of linked databases for improved confounding control: Considerations for potential selection bias. Am. J. Epidemiol. 2022, 191, 711–723. [Google Scholar] [CrossRef]
- Denktas, A.E.; Anderson, H.V.; McCarthy, J.; Smalling, R.W. Total ischemic time: The correct focus of attention for optimal ST-segment elevation myocardial infarction care. JACC Cardiovasc. Interv. 2011, 4, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Mathews, R.; Peterson, E.D.; Li, S.; Roe, M.T.; Glickman, S.W.; Wiviott, S.D.; Saucedo, J.F.; Antman, E.M.; Jacobs, A.K.; Wang, T.Y. Use of emergency medical service transport among patients with ST-segment-elevation myocardial infarction: Findings from the National Cardiovascular Data Registry Acute Coronary Treatment Intervention Outcomes Network Registry-Get with The Guidelines. Circulation 2011, 124, 154–163. [Google Scholar] [CrossRef]
- Mahajan, S.; Valero-Elizondo, J.; Khera, R.; Desai, N.R.; Blankstein, R.; Blaha, M.J.; Virani, S.S.; Kash, B.A.; Zoghbi, W.A.; Krumholz, H.M.; et al. Variation and disparities in awareness of myocardial infarction symptoms among adults in the United States. JAMA Netw. Open 2019, 2, e1917885. [Google Scholar] [CrossRef]
- Chang, J.; Deng, Q.; Guo, M.; Ezzati, M.; Baumgartner, J.; Bixby, H.; Chan, Q.; Zhao, D.; Lu, F.; Hu, P.; et al. Trends and inequalities in the incidence of acute myocardial infarction among Beijing townships, 2007–2018. Int. J. Environ. Res. Public Health 2021, 18, 12276. [Google Scholar] [CrossRef]
- Beijing Municipal Health Commission. Beijing Health Facilities Special Plan (2020–2035). Available online: http://wjw.beijing.gov.cn/zwgk_20040/ghjh1/202109/t20210910_2490429.html (accessed on 21 November 2022).
- Mckenna, K.; Broome, K.; Liddle, J. What older people do: Time use and exploring the link between role participation and life satisfaction in people aged 65 years and over. Aust. Occup. Ther. J. 2007, 54, 273–284. [Google Scholar] [CrossRef]
- Bu, J.; Yin, J.; Yu, Y.; Zhan, Y. Identifying the daily activity spaces of older adults living in a high-density urban area: A study using the smartphone-based Global Positioning System trajectory in Shanghai. Sustainability 2021, 13, 5003. [Google Scholar] [CrossRef]
- Zhang, Q.; Zhao, D.; Xie, W.; Xie, X.; Guo, M.; Wang, M.; Wang, W.; Liu, W.; Liu, J. Recent trends in hospitalization for acute myocardial infarction in Beijing: Increasing overall burden and a transition from ST-segment elevation to non-ST-segment elevation myocardial infarction in a population-based study. Medicine 2016, 95, e2677. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 142,474) | Driving Time to the Nearest PCI-Capable Hospital (minutes) | p Value | |||
|---|---|---|---|---|---|---|
| Driving Time: ≤15 (n = 67,821) | Driving Time: 16–30 (n = 49,688) | Driving Time: 31–45 (n = 18,038) | Driving Time: >45 (n = 6927) | |||
| Patient-level characteristics | ||||||
| Age, mean (SD), years | 69.3 (13.6) | 69.9 (13.7) | 68.6 (13.7) | 68.8 (13.4) | 70.1 (13.3) | <0.001 |
| Age groups, n (%) | <0.001 | |||||
| <65 years | 53,436 (37.5) | 24,860 (36.7) | 19,563 (39.4) | 6706 (37.2) | 2307 (33.3) | |
| ≥65 years | 89,038 (62.5) | 42,961 (63.3) | 30,125 (60.6) | 11,332 (62.8) | 4620 (66.7) | |
| Male, n (%) | 92,714 (65.1) | 45,153 (66.6) | 32,508 (65.4) | 10,942 (60.7) | 4111 (59.4) | <0.001 |
| Marital status, n (%) | <0.001 | |||||
| Married | 116,611 (81.9) | 57,318 (84.5) | 40,321 (81.2) | 13,974 (77.5) | 4998 (72.2) | |
| Not married | 25,863 (18.1) | 10,503 (15.5) | 9367 (18.8) | 4064 (22.5) | 1929 (27.8) | |
| Comorbidity, n (%) | ||||||
| Heart failure | 46,068 (32.3) | 24,057 (35.5) | 15,531 (31.3) | 4830 (26.8) | 1650 (23.8) | <0.001 |
| Stroke | 8387 (5.9) | 4603 (6.8) | 2779 (5.6) | 744 (4.1) | 261 (3.8) | <0.001 |
| Day of the week, n (%) | <0.001 | |||||
| Weekday | 107,218 (75.3) | 51,757 (76.3) | 37,227 (74.9) | 13,234 (73.4) | 5000 (72.2) | |
| Weekend | 35,256 (24.7) | 16,064 (23.7) | 12,461 (25.1) | 4804 (26.6) | 1927 (27.8) | |
| Region, n (%) | <0.001 | |||||
| Urban | 78,394 (55.0) | 50,871 (75.0) | 26,061 (52.5) | 1462 (8.1) | 0 | |
| Peri-urban | 64,080 (45.0) | 16,950 (25.0) | 23,627 (47.5) | 16,576 (91.9) | 6927 (100.0) | |
| Years of education | 11.3 (1.6) | 12.1 (1.0) | 11.2 (1.6) | 9.5 (1.0) | 8.7 (0.8) | <0.001 |
| District-level characteristics | ||||||
| Per capita disposable income, n (%) | <0.001 | |||||
| Quartile 1 (31,611–33,936) | 21,454 (15.1) | 4202 (6.2) | 8515 (17.1) | 7162 (39.7) | 1575 (22.7) | |
| Quartile 2 (33,937–41,168) | 32,769 (23.0) | 8742 (12.9) | 11,170 (22.5) | 8108 (45.0) | 4749 (68.6) | |
| Quartile 3 (41,169–65,966) | 48,057 (33.7) | 26,359 (38.9) | 18,961 (38.2) | 2134 (11.8) | 603 (8.7) | |
| Quartile 4 (65,967–77,167) | 40,194 (28.2) | 28,518 (42.0) | 11,042 (22.2) | 634 (3.5) | 0 | |
| The proportion of unemployed, n (%) | <0.001 | |||||
| Quartile 1 (3.1–3.9) | 37,020 (26.0) | 17,975 (26.5) | 12,723 (25.6) | 3987 (22.1) | 2335 (33.7) | |
| Quartile 2 (4.0–4.3) | 44,359 (31.1) | 26,292 (38.8) | 15,028 (30.2) | 2542 (14.1) | 497 (7.2) | |
| Quartile 3 (4.4–4.7) | 33,103 (23.2) | 13,514 (19.9) | 12,489 (25.1) | 6324 (35.1) | 776 (11.2) | |
| Quartile 4 (4.8–9.5) | 27,992 (19.7) | 10,040 (14.8) | 9448 (19.1) | 5185 (28.7) | 3319 (47.9) | |
| Driving Time (minutes) | Deaths/Events, No. | Model 1 * | Model 2 † | Model 3 ‡ | Model 4 § | ||||
|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | ||
| ≤15 | 20,509/67,821 | 1 | 1 | 1 | 1 | ||||
| 16–30 | 16,710/49,688 | 1.210 (1.177–1.243) | <0.001 | 1.291 (1.253–1.329) | <0.001 | 1.071 (1.037–1.106) | <0.001 | 1.068 (1.033–1.104) | <0.001 |
| 31–45 | 7148/18,038 | 1.703 (1.635–1.774) | <0.001 | 1.759 (1.683–1.838) | <0.001 | 1.211 (1.149–1.277) | <0.001 | 1.189 (1.127–1.255) | <0.001 |
| >45 | 3389/6927 | 2.566 (2.428–2.713) | <0.001 | 2.467 (2.322–2.620) | <0.001 | 1.501 (1.399–1.611) | <0.001 | 1.436 (1.334–1.544) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, J.; Deng, Q.; Hu, P.; Yang, Z.; Guo, M.; Lu, F.; Su, Y.; Sun, J.; Qi, Y.; Long, Y.; et al. Driving Time to the Nearest Percutaneous Coronary Intervention-Capable Hospital and the Risk of Case Fatality in Patients with Acute Myocardial Infarction in Beijing. Int. J. Environ. Res. Public Health 2023, 20, 3166. https://doi.org/10.3390/ijerph20043166
Chang J, Deng Q, Hu P, Yang Z, Guo M, Lu F, Su Y, Sun J, Qi Y, Long Y, et al. Driving Time to the Nearest Percutaneous Coronary Intervention-Capable Hospital and the Risk of Case Fatality in Patients with Acute Myocardial Infarction in Beijing. International Journal of Environmental Research and Public Health. 2023; 20(4):3166. https://doi.org/10.3390/ijerph20043166
Chicago/Turabian StyleChang, Jie, Qiuju Deng, Piaopiao Hu, Zhao Yang, Moning Guo, Feng Lu, Yuwei Su, Jiayi Sun, Yue Qi, Ying Long, and et al. 2023. "Driving Time to the Nearest Percutaneous Coronary Intervention-Capable Hospital and the Risk of Case Fatality in Patients with Acute Myocardial Infarction in Beijing" International Journal of Environmental Research and Public Health 20, no. 4: 3166. https://doi.org/10.3390/ijerph20043166
APA StyleChang, J., Deng, Q., Hu, P., Yang, Z., Guo, M., Lu, F., Su, Y., Sun, J., Qi, Y., Long, Y., & Liu, J. (2023). Driving Time to the Nearest Percutaneous Coronary Intervention-Capable Hospital and the Risk of Case Fatality in Patients with Acute Myocardial Infarction in Beijing. International Journal of Environmental Research and Public Health, 20(4), 3166. https://doi.org/10.3390/ijerph20043166