
Threat through the Screen? Association between Proximity and/or Watching Media Coverage of a Terrorist Attack and Health

 ,
,  ,
,
Abstract
:1. Introduction
- The relation between media watching and mental health outcomes, namely anxiety and depressive symptoms.
- The relation between media watching and physical health outcomes.
- The role of proximity in relation to media watching in association with health outcomes.
2. Materials and Methods
2.1. Design
2.2. Population and Sample
2.3. Measures
2.3.1. Media-Watching
2.3.2. Proximity
2.3.3. Health Indicators
2.4. Analysis
2.5. Ethics
3. Results
3.1. Characteristics of Sample
3.2. Media-Watching
3.3. Proximity to Attacks
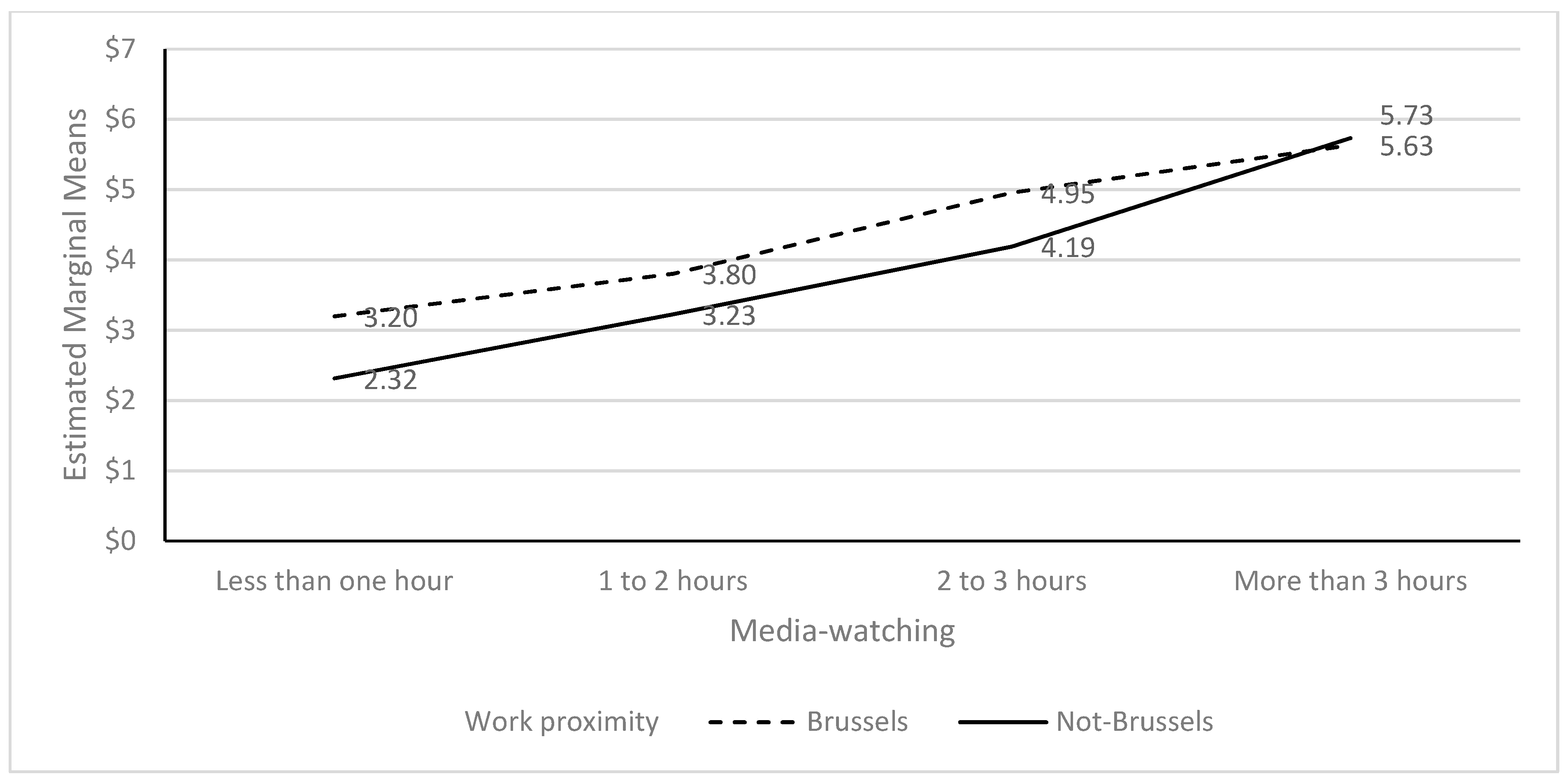
3.4. Proximity and Media-Watching
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, N.M.; Garfin, D.R.; Holman, E.A.; Silver, R.C. Media Use and Exposure to Graphic Content in the Week Following the Boston Marathon Bombings. Am. J. Community Psychol. 2016, 58, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Ahern, J.; Galea, S.; Resnick, H.; Kilpatrick, D.; Bucuvalas, M.; Gold, J.; Vlahov, D. Television Images and Psychological Symptoms after the September 11 Terrorist Attacks. Psychiatry Interpers. Biol. Process. 2002, 65, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.R.; Holman, E.A.; Silver, R.C. Worst Life Events and Media Exposure to Terrorism in a Nationally Representative U.S. Sample. J. Trauma. Stress 2020, 33, 984–993. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.C.; Holman, E.A.; Andersen, J.; Poulin, M.; McIntosh, D.N.; Gil-Rivas, V. Mental- and Physical-Health Effects of Acute Exposure to Media Images of the September 11, 2001, Attacks and the Iraq War. Psychol. Sci. 2013, 24, 1623–1634. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; Palka, J.; North, C.S. Media Contact and Posttraumatic Stress in Employees of New York City Area Businesses after the September 11 Attacks. Disaster Med. Public Health Prep. 2020, 16, 163–169. [Google Scholar] [CrossRef]
- Robert, M.; Stene, L.E.; Garfin, D.R.; Vandentorren, S.; Motreff, Y.; du Roscoat, E.; Pirard, P. Media Exposure and Post-traumatic Stress Symptoms in the Wake of the November 2015 Paris Terrorist Attacks: A Population-Based Study in France. Front. Psychiatry 2021, 12, 509457. [Google Scholar] [CrossRef]
- Schlenger, W.E.; Caddell, J.M.; Ebert, L.; Jordan, B.K.; Rourke, K.M.; Wilson, D.; Thalji, L.; Dennis, J.M.; Fairbank, J.A.; Kulka, R.A. Psychological reactions to terrorist attacks: Findings from the National Study of Americans’ Reactions to September 11. JAMA 2002, 288, 581–588. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Palka, J.; North, C. Associations between News Media Coverage of the 11 September Attacks and Depression in Employees of New York City Area Businesses. Behav. Sci. 2021, 11, 29. [Google Scholar] [CrossRef]
- American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders 5; APA: Washington, DC, USA, 2013. [Google Scholar]
- Rigutto, C.; Sapara, A.O.; Agyapong, V.I.O. Anxiety, Depression and Posttraumatic Stress Disorder after Terrorist Attacks: A General Review of the Literature. Behav. Sci. 2021, 11, 140. [Google Scholar] [CrossRef]
- de Wit, L.; van Straten, A.; Lamers, F.; Cuijpers, P.; Penninx, B. Are sedentary television watching and computer use behaviors associated with anxiety and depressive disorders? Psychiatry Res. 2011, 186, 239–243. [Google Scholar] [CrossRef]
- Holman, E.A.; Silver, R.C.; Poulin, M.; Andersen, J.; Gil-Rivas, V.; McIntosh, D.N. Terrorism, acute stress, and cardiovascular health: A 3-year national study following the September 11th attacks. Arch. Gen. Psychiatry 2008, 65, 73–80. [Google Scholar] [CrossRef]
- Strand, L.B.; Mukamal, K.J.; Halasz, J.; Vatten, L.J.; Janszky, I. Short-Term Public Health Impact of the July 22, 2011, Terrorist Attacks in Norway: A Nationwide Register-Based Study. Psychosom. Med. 2016, 78, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Chatignoux, E.; Gabet, A.; Moutengou, E.; Pirard, P.; Motreff, Y.; Bonaldi, C.; Olié, V. The 2015 and 2016 terrorist attacks in France: Was there a short-term impact on hospitalizations for cardiovascular disease? Clin. Epidemiol. 2018, 10, 413–419. [Google Scholar] [CrossRef]
- Stene, L.E.; Vuillermoz, C.; Van Overmeire, R.; Bilsen, J.; Dückers, M.; Nilsen, L.G.; Vandentorren, S. Psychosocial care responses to terrorist attacks: A country case study of Norway, France and Belgium. BMC Health Serv. Res. 2022, 22, 390. [Google Scholar] [CrossRef]
- Deschepper, R.; Six, S.; Gidron, Y.; Depoorter, A.-M.; Vandekerckhove, M.; Gheysens, N.; Van Overmeire, R.; Bilsen, J. Association between feeling threatened by a terrorist attack and subjective health: A web survey a week after the attacks of 22 March 2016 in Belgium. Eur. J. Psychotraumatol. 2018, 9, 1500821. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Lowe, B. An ultra-brief screening scale for anxiety and depression: The PHQ-4. Psychosomatics 2009, 50, 613–621. [Google Scholar] [PubMed]
- Kocalevent, R.-D.; Hinz, A.; Brähler, E. Standardization of a screening instrument (PHQ-15) for somatization syndromes in the general population. BMC Psychiatry 2013, 13, 91. [Google Scholar] [CrossRef]
- Holman, E.A.; Garfin, D.R.; Silver, R.C. Media’s role in broadcasting acute stress following the Boston Marathon bombings. Proc. Natl. Acad. Sci. USA 2013, 111, 93–98. [Google Scholar] [CrossRef]
- Thompson, R.R.; Jones, N.M.; Holman, E.A.; Silver, R.C. Media exposure to mass violence events can fuel a cycle of distress. Sci. Adv. 2019, 5, eaav3502. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Nitiéma, P.; Pfefferbaum, R.L.; Houston, J.B.; Tucker, P.; Jeon-Slaughter, H.; North, C.S. Reactions of Oklahoma City bombing survivors to media coverage of the September 11, 2001, attacks. Compr. Psychiatry 2015, 65, 70–78. [Google Scholar] [CrossRef]
- Van Overmeire, R.; Gidron, Y.; Six, S.; Deschepper, R.; Vandekerckhove, M.; Bilsen, J. Suicide in Flanders, Belgium, after terrorist attacks. Psychol. Health Med. 2022, 27, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Van Overmeire, R.; Six, S.; Deschepper, R.; Vandekerckhove, M.; Bilsen, J. Association Between Feeling Threatened, Behaviour and Symptoms of Anxiety and Depression: Two and a Half Years After the Terrorist Attacks in Belgium. Community Ment Health J. 2022, 58, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Durodie, B.; Wainwright, D. Terrorism and post-traumatic stress disorder: A historical review. Lancet Psychiatry 2019, 6, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Government Belgium. Werkloosheidsgraad 2023: Belgian Government. 2023. Available online: https://indicators.be/nl/i/G08_UNE/Werkloosheidsgraad (accessed on 12 December 2022).


{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Gender | ||
| Male | 895 | 30.1 |
| Female | 2077 | 69.9 |
| Education level | ||
| Lower | 255 | 8.6 |
| Middle | 906 | 30.5 |
| Higher | 1811 | 60.9 |
| Professional status | ||
| Wage earners | 1948 | 65.5 |
| Independent | 326 | 11 |
| Students | 361 | 12.1 |
| Unemployed | 129 | 4 |
| Retired | 236 | 7.9 |
| Sick leave | 112 | 3.8 |
| Living situation | ||
| Alone | 603 | 20.3 |
| Together | 2362 | 79.7 |
| Home proximity | ||
| Brussels | 793 | 26.8 |
| Not Brussels | 2171 | 73.2 |
| Work proximity | ||
| Brussels | 1231 | 49.3 |
| Not Brussels | 1266 | 50.7 |
| Overall proximity * | ||
| Brussels | 640 | 34.8 |
| Not Brussels | 1200 | 65.2 |
| Mental symptoms (PHQ-4) | ||
| Normal | 1040 | 35 |
| Mild | 907 | 30.5 |
| Moderate | 544 | 18.3 |
| Severe | 481 | 16.2 |
| Somatic symptoms (PHQ-15) | ||
| Normal | 1500 | 50.5 |
| Mild | 895 | 30.1 |
| Moderate | 390 | 13.1 |
| Severe | 187 | 6.3 |
| Working in Brussels | % | Not Working in Brussels | % | |
|---|---|---|---|---|
| Living in Brussels | 640 | 52.1 | 65 | 5.1 |
| Not living in Brussels | 588 | 47.9 | 1200 | 94.4 |
| Three Hours or Less Watching | % | More than Three Hours Watching | % | p-Value | |
|---|---|---|---|---|---|
| Alone * | 335 | 18.8 | 268 | 22.7 | 0.01 |
| Together | 1149 | 81.2 | 913 | 77.3 | |
| Lower education level | 129 | 7.2 | 126 | 10.6 | 0.003 |
| Middle education level | 544 | 30.4 | 362 | 30.5 | |
| Higher education level | 1114 | 62.3 | 697 | 58.8 | |
| PHQ-4 | <0.001 | ||||
| Normal | 774 | 43.3 | 266 | 35 | |
| Mild | 577 | 31.2 | 350 | 30.5 | |
| Moderate | 274 | 15.3 | 270 | 18.3 | |
| Severe | 182 | 10.2 | 299 | 16.2 | |
| PHQ-15 | <0.001 | ||||
| Normal | 1059 | 59.3 | 441 | 37.2 | |
| Mild | 486 | 27.2 | 409 | 34.5 | |
| Moderate | 175 | 9.8 | 215 | 18.1 | |
| Severe | 67 | 3.7 | 120 | 10.1 |
| PHQ-4 | SD | p-Value | PHQ-15 | SD | p-Value | |
|---|---|---|---|---|---|---|
| Three hours or less watching | 3.7448 | 3.1925 | <0.001 | 4.61 | 4.434 | <0.001 |
| More than three hours watching | 5.692 | 3.6519 | 6.95 | 5.313 | ||
| Living in Brussels | 5.1740 | 3.5869 | <0.001 | 6.0 | 4.881 | 0.002 |
| Not living in Brussels | 4.2736 | 3.4518 | 5.37 | 4.952 | ||
| Working in Brussels | 4.7929 | 3.4406 | <0.001 | 5.70 | 4.830 | 0.035 |
| Not working in Brussels | 4.1927 | 3.4247 | 5.29 | 4.825 | ||
| Overall in Brussels | 5.1813 | 3.5632 | <0.001 | 6.01 | 4.87 | 0.003 |
| Overall not in Brussels | 4.1733 | 3.4207 | 5.29 | 4.869 |
| Three Hours or Less Watching | % | More than Three Hours Watching | % | p-Value | |
|---|---|---|---|---|---|
| Living in Brussels | 423 | 23.7 | 370 | 31.4 | <0.001 |
| Not living in Brussels | 1361 | 76.3 | 810 | 68.6 | |
| Total | 1784 | 100 | 1180 | 100 | |
| Working in Brussels | 732 | 48 | 499 | 51.3 | 0.104 |
| Not working in Brussels | 793 | 52 | 473 | 48.7 | |
| Total | 1525 | 100 | 972 | 100 | |
| Overall in Brussels | 359 | 32.1 | 281 | 39 | 0.003 |
| Overall not in Brussels | 761 | 67.9 | 439 | 61 | |
| Total | 1120 | 100 | 720 | 100 |
| B | SD | p | R2 | |
|---|---|---|---|---|
| PHQ-4 | ||||
| Step 1 | <0.001 | 0.058 | ||
| Constant | 8.345 | 0.367 | <0.001 | |
| Age | 0.005 | 0.005 | 0.311 | |
| Gender (female ref. cat) | −1.520 | 0.137 | <0.001 | |
| Education level (lower-middle ref. cat) | −0.595 | 0.131 | <0.001 | |
| Home proximity (Brussels. ref. cat) | −0.971 | 0.144 | <0.001 | |
| Step 2 | <0.001 | 0.139 | ||
| Constant | 4.675 | 0.414 | <0.001 | |
| Age | 0.007 | 0.004 | 0.091 | |
| Gender (female ref. cat) | −1.339 | 0.132 | <0.001 | |
| Education level (lower-middle ref. cat) | −0.529 | 0.125 | <0.001 | |
| Home proximity (Brussels. ref. cat) | −0.750 | 0.138 | <0.001 | |
| Media-watching | 0.986 | 0.059 | <0.001 | |
| PHQ-4 | ||||
| Step 1 | <0.001 | 0.049 | ||
| Constant | 7.105 | 0.369 | <0.001 | |
| Age | 0.013 | 0.006 | 0.015 | |
| Gender (female ref. cat) | −1.453 | 0.149 | <0.001 | |
| Education level (lower-middle ref. cat) | −0.472 | 0.142 | <0.001 | |
| Work proximity (Brussels. ref. cat) | −0.641 | 0.137 | <0.001 | |
| Step 2 | <0.001 | 0.132 | ||
| Constant | 3.595 | 0.419 | <0.001 | |
| Age | 0.018 | 0.005 | <0.001 | |
| Gender (female ref. cat) | −1.282 | 0.143 | <0.001 | |
| Education level (lower-middle ref. cat) | −0.445 | 0.136 | 0.001 | |
| Work proximity (Brussels. ref. cat) | −0.502 | 0.131 | <0.001 | |
| Media-watching | 0.985 | 0.064 | <0.001 | |
| PHQ-4 | ||||
| Step 1 | <0.001 | 0.065 | ||
| Constant | 8.044 | 0.46 | <0.001 | |
| Age | 0.017 | 0.007 | 0.009 | |
| Gender (female ref. cat) | −1.403 | 0.174 | <0.001 | |
| Education level (lower-middle ref. cat) | −0.780 | 0.167 | <0.001 | |
| Overall proximity (Brussels. ref. cat) | −0.574 | 0.085 | <0.001 | |
| Step 2 | <0.001 | 0.16 | ||
| Constant | 4.14 | 0.512 | <0.001 | |
| Age | 0.022 | 0.006 | <0.001 | |
| Gender (female ref. cat) | −1.255 | 0.165 | <0.001 | |
| Education level (lower-middle ref. cat) | −0.737 | 0.158 | <0.001 | |
| Overall proximity (Brussels. ref. cat) | −0.454 | 0.081 | <0.001 | |
| Media-watching | 1.065 | 0.074 | <0.001 | |
| PHQ-15 | ||||
| Step 1 | <0.001 | 0.067 | ||
| Constant | 10.941 | 0.514 | <0.001 | |
| Age | −0.008 | 0.006 | 0.193 | |
| Gender (female ref. cat) | −2.545 | 0.192 | <0.001 | |
| Education level (lower-middle ref. cat) | −0.900 | 0.183 | <0.001 | |
| Home proximity (Brussels. ref. cat) | −0.691 | 0.201 | <0.001 | |
| Step 2 | <0.001 | 0.118 | ||
| Constant | 6.82 | 0.589 | <0.001 | |
| Age | −0.005 | 0.006 | 0.401 | |
| Gender (female ref. cat) | −2.342 | 0.188 | <0.001 | |
| Education level (lower-middle ref. cat) | −0.825 | 0.178 | <0.001 | |
| Home proximity (Brussels. ref. cat) | −0.442 | 0.197 | 0.025 | |
| Media-watching | 1.108 | 0.084 | <0.001 | |
| PHQ-15 | ||||
| Step 1 | <0.001 | 0.059 | ||
| Constant | 9.77 | 0.514 | <0.001 | |
| Age | 0.001 | 0.008 | 0.855 | |
| Gender (female ref. cat) | −2.448 | 0.207 | <0.001 | |
| Education level (lower-middle ref. cat) | −0.776 | 0.198 | <0.001 | |
| Work proximity (Brussels. ref. cat) | −0.454 | 0.191 | 0.017 | |
| Step 2 | <0.001 | 0.114 | ||
| Constant | 5.785 | 0.593 | <0.001 | |
| Age | 0.007 | 0.007 | 0.37 | |
| Gender (female ref. cat) | −2.254 | 0.202 | <0.001 | |
| Education level (lower-middle ref. cat) | −0.745 | 0.192 | <0.001 | |
| Work proximity (Brussels. ref. cat) | −0.297 | 0.185 | 0.11 | |
| Media-watching | 1.118 | 0.09 | <0.001 | |
| PHQ-15 | ||||
| Step 1 | <0.001 | 0.057 | ||
| Constant | 10.459 | 0.642 | <0.001 | |
| Age | 0.001 | 0.009 | 0.877 | |
| Gender (female ref. cat) | −2.238 | 0.243 | <0.001 | |
| Education level (lower-middle ref. cat) | −1.051 | 0.233 | <0.001 | |
| Overall proximity (Brussels. ref. cat) | −0.433 | 0.119 | <0.001 | |
| Step 2 | <0.001 | 0.117 | ||
| Constant | 6.174 | 0.731 | <0.001 | |
| Age | 0.006 | 0.009 | 0.468 | |
| Gender (female ref. cat) | −2.076 | 0.236 | <0.001 | |
| Education level (lower-middle ref. cat) | −1.004 | 0.226 | <0.001 | |
| Overall proximity (Brussels. ref. cat) | −0.301 | 0.116 | 0.009 | |
| Media-watching | 1.169 | 0.105 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Overmeire, R.; Stene, L.E.; Vandekerckhove, M.; Six, S.; Deschepper, R.; Bilsen, J. Threat through the Screen? Association between Proximity and/or Watching Media Coverage of a Terrorist Attack and Health. Int. J. Environ. Res. Public Health 2023, 20, 2876. https://doi.org/10.3390/ijerph20042876
Van Overmeire R, Stene LE, Vandekerckhove M, Six S, Deschepper R, Bilsen J. Threat through the Screen? Association between Proximity and/or Watching Media Coverage of a Terrorist Attack and Health. International Journal of Environmental Research and Public Health. 2023; 20(4):2876. https://doi.org/10.3390/ijerph20042876
Chicago/Turabian StyleVan Overmeire, Roel, Lise Eilin Stene, Marie Vandekerckhove, Stefaan Six, Reginald Deschepper, and Johan Bilsen. 2023. "Threat through the Screen? Association between Proximity and/or Watching Media Coverage of a Terrorist Attack and Health" International Journal of Environmental Research and Public Health 20, no. 4: 2876. https://doi.org/10.3390/ijerph20042876
APA StyleVan Overmeire, R., Stene, L. E., Vandekerckhove, M., Six, S., Deschepper, R., & Bilsen, J. (2023). Threat through the Screen? Association between Proximity and/or Watching Media Coverage of a Terrorist Attack and Health. International Journal of Environmental Research and Public Health, 20(4), 2876. https://doi.org/10.3390/ijerph20042876