


The Influence of Home-Based Music Therapy Interventions on Relationship Quality in Couples Living with Dementia—An Adapted Convergent Mixed Methods Study

 , , , ,
, , , ,
Abstract
1. Introduction
2. Methods
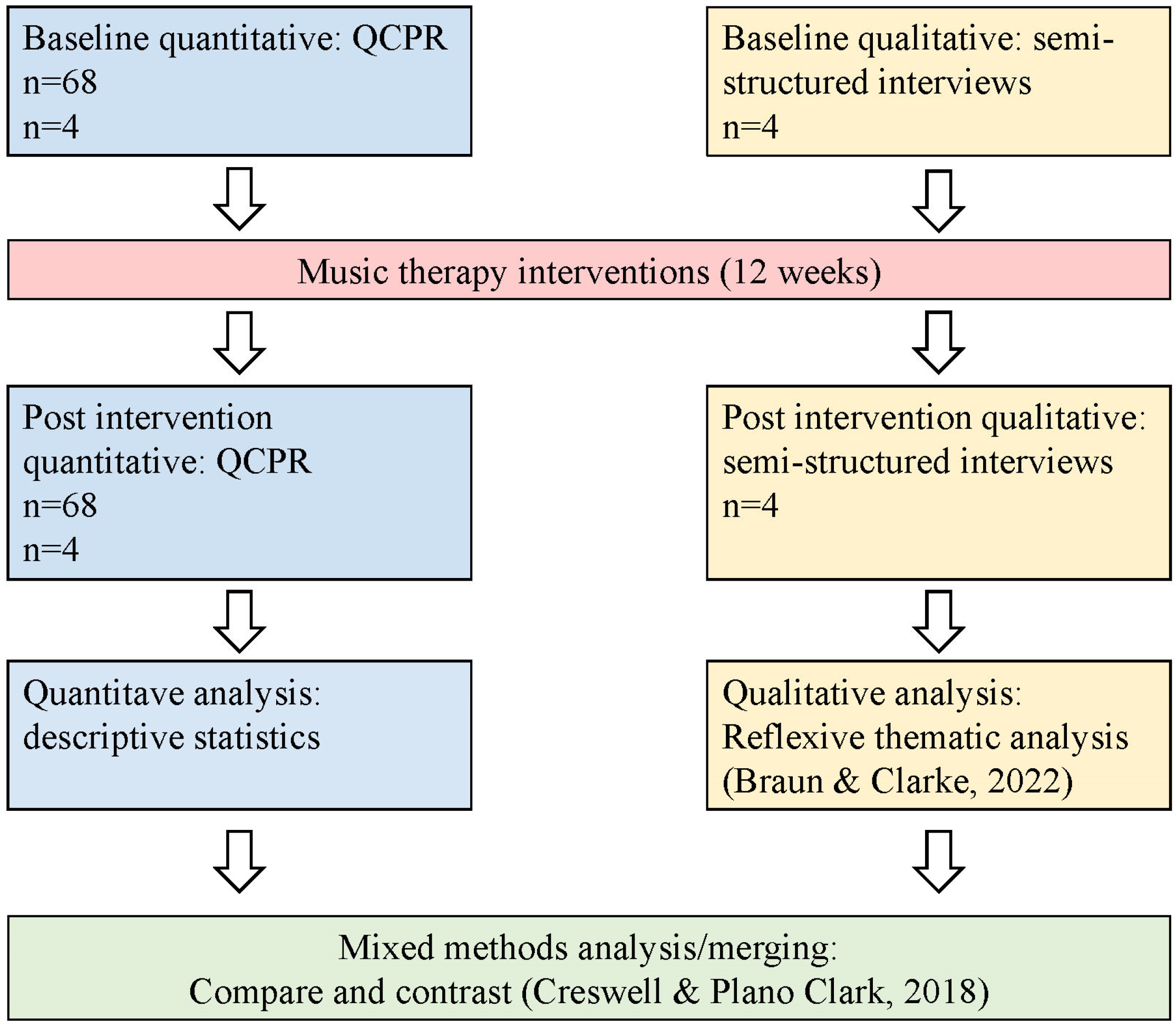
2.1. Study Design
2.2. Inclusion Criteria and Recruitment
- Two persons living together at home, married or in an equivalent significant relationship.
- One of the persons had a dementia diagnosis according to the 10th revision of the International Classification of Diseases and Related Health Problems (ICD-10), as determined by a clinician experienced in diagnosing dementia.
- A minimum severity score of 6 on the Neuropsychiatric Inventory-Questionnaire (NPI-Q) [34], which measures the degree of behavioural and psychological symptoms of dementia (BPSD).
- Exclusion criteria were:
- Severe hearing impairment, which could not be resolved through hearing aids.
- No access to technical equipment or internet (HOMESIDE subset only).
2.3. Music Therapy Intervention: Implementation of Music Therapy Activities
2.4. Data Collection and Analysis
2.5. Ethical Considerations and Participant Involvement
3. Results
3.1. Participants
3.2. Quantitative Analysis
3.3. Qualitative Analysis
3.3.1. Contextual Findings: Life, Relationship, and the Caregiver-Spouse Paradox
CG: Anyway, he is still my boyfriend!PwD: I agree with you (laughs)CG: Yes, we are still romantic partnersInterviewer: And [PwD], do you think of [CG] as your girlfriend?PwD: Yes. Absolutely.[Baseline interview: Couple 4, large negative change QCPR]
CG: So, I see the man that I fell in love with and have loved all these years, and still do love. He is [PwD], he can’t do all these things anymore, but he is here. So, I can hold his hand, I can help him and support him, and get gratitude in return. He shows gratitude. He becomes frustrated sometimes, and I do too, but then it’s over. I feel that we have closeness still, but of course there are things … I can’t let the pain take over, it hurts too much. The pain is there. But, I need to think positively. Take care of what we have.[Baseline interview: Couple 3, large positive change QCPR]
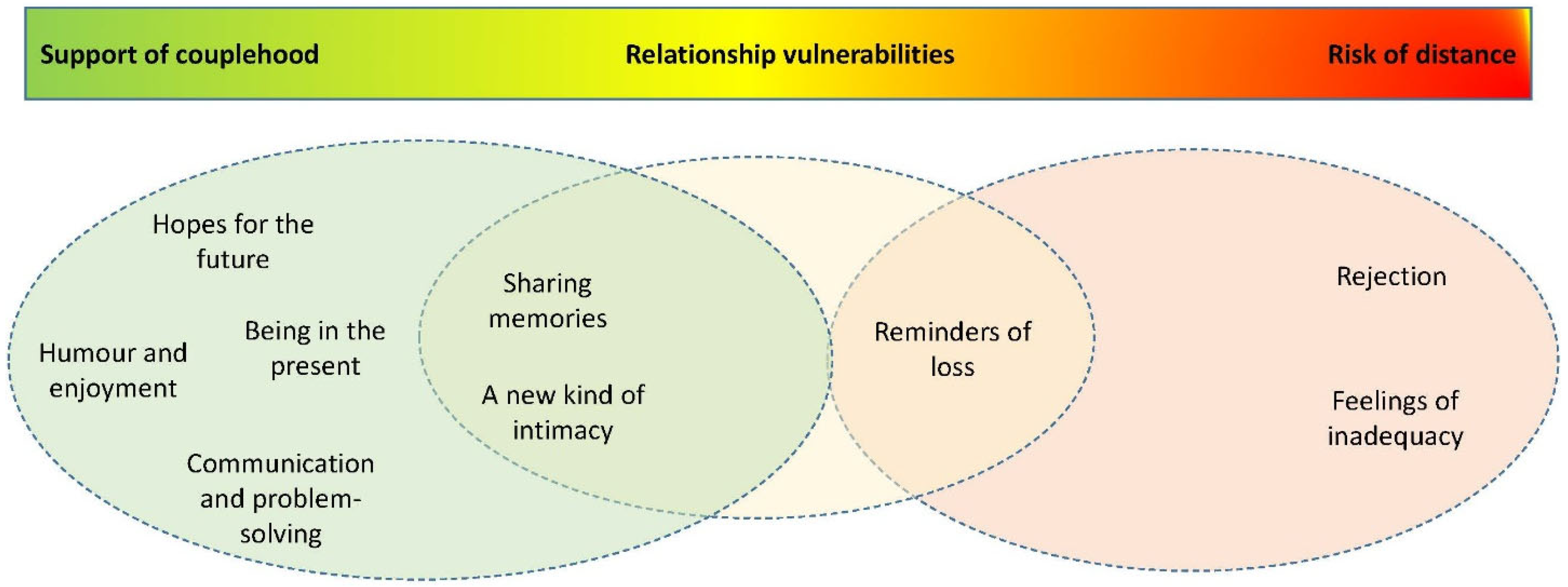
3.3.2. The Influences of the Music Therapy Intervention on Couple Relationship Quality
3.3.3. Overarching Theme 1: Support of Couplehood
Sharing Memories
CG: We reminisce … to music from our youth … I think it makes us both happy and sad.PwD: Yes, I really immerse myself in that music. And I think about everything, the way things were … the way we danced [starts crying].CG: We have so many positive memories. It’s not dangerous to cry a little(both laugh).[Post intervention interview: Couple 4, large negative change QCPR]
Being in the Present
Interviewer: Is music a larger part of your life now?CG: Yes, it is, and I am much more aware that I can use it in different situations. Sometimes it is good to just be in the music, it gives us a rest from everything else, we can just be together in [the music] here and now.[Post intervention interview: Couple 1, small positive change QCPR]
Humour and Enjoyment
CG (turned to PwD): You are more like you used to be before, when we use music. You get cheerful, I never knew you’d get cheerful from Irish music (both laugh) … and I even think you get less nervous when we sing together. That’s new.[Post intervention interview: Couple 2, no change QCPR]
Communication and Problem-Solving
(PwD had fallen asleep at this point of the interview)CG: When he is to sit down in his chair, it’s really hard for him to turn his back to the chair. And he stands like a statue, won’t move. Then one day I thought: what makes him move his legs? Yes, dancing! (laughs). So I held out my hands and asked “do you want to dance?” and started singing something like (sings a short phrase from an up-tempo song), and then he started to move his legs and turned around with me.[Post intervention interview: Couple 3, large positive change in QCPR]
A New Kind of Intimacy
CG (turned to PwD) There is no one I feel as close with, as you. Sometimes, when we go to a concert, maybe together with friends, our eyes meet and we look at each other, we share memories and feelings without using words. That’s bringing us even closer, I think.[Post intervention interview: Couple 4, large negative change QCPR]
Hopes for the Future
Interviewer: Do you think music is something you can share in the future also, even though you will live in different places?CG: Yes, I think so. I think maybe our music can keep us together in the future.[Post intervention interview: Couple 1, small positive change QCPR]
3.3.4. Overarching Theme 2: Risk of Distance
Rejection
PwD: I had hoped we could dance more.CG: But you are tired all the time, you have been tired for weeks!PwD: Yes…CG: you asked me about dancing, but there is not that much we can do with your body, you know?[Post intervention interview: Couple 4, large negative change QCPR]
Feelings of Inadequacy
CG: Sometimes I don’t feel comfortable singing. Once you [PwD] told me I sang out of tune, that made me insecure. I don’t know, it depends on the day. Sometimes listening is better.[Post intervention interview: Couple 2, no change QCPR]
Reminders of Loss
CG: He is very rigid now, also when it comes to music. It’s because of his illness. He used to love so many types of music. Sometimes now we can’t listen to music, because he only wants one artist, and the same song over and over again. It’s too much for me when it’s like that. The music and his way of being.[Post intervention interview: Couple 1, small positive change QCPR]
3.3.5. Merging of Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Rippon, I.; Quinn, C.; Martyr, A.; Morris, R.; Nelis, S.M.; Jones, I.R.; Victor, C.R.; Clare, L. The impact of relationship quality on life satisfaction and well-being in dementia caregiving dyads: Findings from the IDEAL study. Aging Ment. Health 2020, 24, 1411–1420. [Google Scholar] [CrossRef] [PubMed]
- Curnow, E.; Rush, R.; Maciver, D.; Górska, S.; Forsyth, K. Exploring the needs of people with dementia living at home reported by people with dementia and informal caregivers: A systematic review and Meta-analysis. Aging Ment. Health 2021, 25, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Stedje, K.; Kvamme, T.K.; Johansson, K.; Stensæth, K.A.; Odell-Miller, H.; Bukowska, A.; Tamplin, J.; Wosch, T.; Baker, F.A. Influential factors of spousal relationship quality in couples living with dementia-A narrative synthesis systematic review. Dementia 2022, 22, 14713012221137280. [Google Scholar] [CrossRef] [PubMed]
- Feast, A.; Orrell, M.; Charlesworth, G.; Melunsky, N.; Poland, F.; Moniz-Cook, E. Behavioural and psychological symptoms in dementia and the challenges for family carers: Systematic review. Br. J. Psychiatry 2016, 208, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Bruinsma, J.; Peetoom, K.; Millenaar, J.; Köhler, S.; Bakker, C.; Koopmans, R.; Pijnenburg, Y.; Verhey, F.; de Vugt, M. The quality of the relationship perceived by spouses of people with young-onset dementia. Int. Psychogeriatr. 2020, 1–10. [Google Scholar] [CrossRef]
- Clare, L.; Nelis, S.M.; Whitaker, C.J.; Martyr, A.; Markova, I.S.; Roth, I.; Woods, R.T.; Morris, R.G. Marital relationship quality in early-stage dementia: Perspectives from people with dementia and their spouses. Alzheimer Dis. Assoc. Disord. 2012, 26, 148–158. [Google Scholar] [CrossRef]
- De Vugt, M.E.; Stevens, F.; Aalten, P.; Lousberg, R.; Jaspers, N.; Winkens, I.; Jolles, J.; Verhey, F.R.J. Behavioural disturbances in dementia patients and quality of the marital relationship. Int. J. Geriatr. Psychiatry 2003, 18, 149–154. [Google Scholar] [CrossRef]
- Colquhoun, A.; Moses, J.; Offord, R. Experiences of loss and relationship quality in couples living with dementia. Dementia 2019, 18, 2158–2172. [Google Scholar] [CrossRef]
- Garand, L.; Dew, M.A.; Urda, B.; Lingler, J.H.; DeKosky, S.T.; Reynolds, C.F. Marital Quality in the Context of Mild Cognitive Impairment. West. J. Nurs. Res. 2007, 29, 976–992. [Google Scholar] [CrossRef]
- Robinson, L.; Clare, L.; Evans, K. Making sense of dementia and adjusting to loss: Psychological reactions to a diagnosis of dementia in couples. Aging Ment. Health 2005, 9, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Daley, R.T.; O’Connor, M.K.; Shirk, S.D.; Beard, R.L. ‘In this together’ or ‘Going it alone’: Spousal dyad approaches to Alzheimer’s. J. Aging Stud. 2017, 40, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Hellström, I.; Nolan, M.; Lundh, U. ‘We do things together’: A case study of ‘couplehood’ in dementia. Dementia 2005, 4, 7–22. [Google Scholar] [CrossRef]
- Hellström, I.; Nolan, M.; Lundh, U. Sustaining ‘couplehood’: Spouses’ strategies for living positively with dementia. Dementia 2007, 6, 383–409. [Google Scholar] [CrossRef]
- Molyneaux, V.J.; Butchard, S.; Simpson, J.; Murray, C. The co-construction of couplehood in dementia. Dementia 2012, 11, 483–502. [Google Scholar] [CrossRef]
- Shavit, O.; Ben-Ze’Ev, A.; Doron, I. Love between couples living with Alzheimer’s disease: Narratives of spouse care-givers. Ageing Soc. 2019, 39, 488–517. [Google Scholar] [CrossRef]
- Swall, A.; Williams, C.; Marmstål Hammar, L. The value of “us”-Expressions of togetherness in couples where one spouse has dementia. Int. J. Older People Nurs. 2020, 15, e12299. [Google Scholar] [CrossRef]
- Gallagher, E.; Beard, R.L. Buffer or Blade: Perceived relationship closeness in couples navigating Alzheimer’s. J. Aging Stud. 2020, 52, 100832. [Google Scholar] [CrossRef]
- Hickman, H.; Clarke, C.; Wolverson, E. A qualitative study of the shared experience of humour between people living with dementia and their partners. Dementia 2018, 19, 1794–1810. [Google Scholar] [CrossRef]
- Vikström, S.; Josephsson, S.; Stigsdotter-Neely, A.; Nygård, L. Engagement in activities: Experiences of persons with dementia and their caregiving spouses. Dementia 2008, 7, 251–270. [Google Scholar] [CrossRef]
- Elliott, M.; Gardner, P. The role of music in the lives of older adults with dementia ageing in place: A scoping review. Dementia 2018, 17, 199–213. [Google Scholar] [CrossRef] [PubMed]
- McMahon, K.; Clark, I.N.; Stensæth, K.; Wosch, T.; Odell Miller, H.; Bukowska, A.; Baker, F.A. A qualitative systematic review of the experiences of sharing music for people living with dementia and their family care partners: The thread of connection. Arts Health 2022, 1–28. [Google Scholar] [CrossRef]
- Tamplin, J.; Clark, I. Therapeutic Music Interventions to Support People with Dementia Living at Home with Their Family Caregivers. In Music and Dementia. From Cognition to Therapy; Baird, A., Garrido, S., Tamplin, J., Eds.; Oxford University Press: New York, NY, USA, 2020. [Google Scholar]
- Baker, F.A.; Grocke, D.; Pachana, N.A. Connecting through music: A study of a spousal caregiver-directed music intervention designed to prolong fulfilling relationships in couples where one person has dementia. Aust. J. Music. Ther. 2012, 23, 4–19. [Google Scholar]
- Thurn, T.; Voigt, M.; Wosch, T. Pilot study of a modular music intervention: A first evaluation of the use of basic elements of music to support interaction between family caregivers and their relatives with dementia. Aust. J. Music. Ther. 2021, 32, 1–25. [Google Scholar]
- Odell-Miller, H.; Blauth, L.; Bloska, J.; Bukowska, A.A.; Clark, I.N.; Crabtree, S.; Engen, R.B.; Knardal, S.; Kvamme, T.K.; McMahon, K.; et al. The HOMESIDE music Intervention: A training protocol for family carers of people living with dementia. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1812–1832. [Google Scholar] [CrossRef]
- Dassa, A. “Opening Our Time Capsule”—Creating an individualized music and other memory cues database to promote communication between spouses and people with dementia during visits to a nursing home. Front. Med. 2018, 5, 215. [Google Scholar] [CrossRef]
- Allan, M. Community music therapy to support the relationship between family carers and people living with dementia: A pilot project. N. Z. J. Music Ther. 2018, 16, 31–53. [Google Scholar]
- Clark, I.N.; Stretton-Smith, P.A.; Baker, F.A.; Lee, Y.-E.C.; Tamplin, J. “It’s feasible to write a song”: A feasibility study examining group therapeutic songwriting for people living with dementia and their family caregivers. Front. Psychol. 2020, 11, 1951. [Google Scholar] [CrossRef] [PubMed]
- Clark, I.N.; Baker, F.A.; Tamplin, J.; Lee, Y.-E.C.; Cotton, A.; Stretton-Smith, P.A. “Doing things together is what it’s about”: An interpretative phenomenological analysis of the experience of group therapeutic songwriting from the perspectives of people with dementia and their family caregivers. Front. Psychol. 2021, 12, 598979. [Google Scholar] [CrossRef] [PubMed]
- Spruytte, N.; Van Audenhove, C.; Lammertyn, F.; Storms, G. The quality of the caregiving relationship in informal care for older adults with dementia and chronic psychiatric patients. Psychol. Psychother. Theory Res. Pract. 2002, 75, 295–311. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.A.; Bloska, J.; Braat, S.; Bukowska, A.; Clark, I.; Hsu, M.H.; Kvamme, T.; Lautenschlager, N.; Lee, Y.E.C.; Smrokowska-Reichmann, A.; et al. HOMESIDE: Home-based family caregiver-delivered music and reading interventions for people living with dementia: Protocol of a randomised controlled trial. BMJ Open 2019, 9, e031332. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage: Los Angeles, CA, USA, 2018. [Google Scholar]
- Kaufer, D.I.; Cummings, J.L.; Christine, D.; Bray, T.; Castellon, S.; Masterman, D.; MacMillan, A.; Ketchel, P.; DeKosky, S.T. Assessing the impact of neuropsychiatric symptoms in Alzheimer’s disease: The Neuropsychiatric Inventory Caregiver Distress Scale. J. Am. Geriatr. Soc. 1998, 46, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Kitwood, T. Dementia Reconsidered: The Person Comes First; Open University Press: London, UK, 1997. [Google Scholar]
- Ridder, H.M. Singing Dialogue: Music Therapy with Persons in Advanced Stages of Dementia. A Case Study Design. Ph.D. Thesis, Aalborg University, Aalborg, Denmark, 2003. [Google Scholar]
- Pangman, V.C.; Sloan, J.; Guse, L. An examination of psychometric properties of the Mini-Mental State Examination and the Standardized Mini-Mental State Examination: Implications for clinical practice. Appl. Nurs. Res. 2000, 13, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)–A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Thompson, Z.; Baker, F.; Clark, I.; Tamplin, J. Making qualitative interviews in music therapy research more accessible for participants living with dementia–Reflections on development and implementation of interview guidelines. Int. J. Qual. Methods 2021, 20, 1–12. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Thematic Analysis. A Practical Guide; Sage: London, UK, 2022. [Google Scholar]
- Bauer, M.J.; Maddox, M.K.; Kirk, L.N.; Burns, T.; Kuskowski, M.A. Progressive dementia: Personal and relational impact on caregiving wives. Am. J. Alzheimer’s Dis. Other Dement. 2001, 16, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, L. A Couplehood Typology for spouses of institutionalized persons with Alzheimer’s disease: Perceptions of “we”–“I”. Fam. Relat. 2001, 50, 87–98. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| HOMESIDE Subset | Individually Recruited Subset |
|---|---|
| n = 68 couples/136 individuals | n = 4 couples/8 individuals |
| Nationality: Australian (n = 19), German (n = 14), Norwegian (n = 14), Polish (n = 1), British (n = 20) | Nationality: Norwegian (n = 4) |
| Clinical intervention: 12-week online home-based music therapy intervention with music therapist | Clinical intervention: 12-week face-to-face home-based music therapy intervention with music therapist |
| Data collection: quantitative, at baseline and post intervention | Data collection: quantitative and qualitative, at baseline and post intervention |
| Week | |
|---|---|
| 1 | Music training session with music therapist and the couple together |
| 1–3 | Couple experiencing music together, by themselves. Phone call from music therapist. |
| 3 | Music training session with music therapist and the couple together |
| 3–6 | Couple experiencing music together, by themselves. Phone calls from music therapist. |
| 6 | Music training session with music therapist and the couple together |
| 7–12 | Couple experiencing music together, by themselves. Fortnightly phone calls from music therapist |
| HOMESIDE Subset Total | Individually Recruited Participants Subset | |
|---|---|---|
| N | n = 68 couples/136 individuals | n = 4 couples/8 individuals |
| Diagnosis | Alzheimer’s dementia(31), Vascular dementia,(15), Memory problems(8), Mixed dementias(4), Lewy Body dementia(3), Frontotemporal dementia(2), Semantic dementia(2), Parkinson’s dementia(1), Mild cognitive impairment(1) | Alzheimer’s dementia(2), Frontotemporal dementia(1), Parkinson’s dementia(1) |
| MMSE scores * | Mean 14.44 (SD 9.64) Range 29 (0–29) | Range: 4–26 |
| NPI-Q severity scores+ | Mean 11.03 (SD 3.58) Range 16 (6–22) | Range: 6–11 |
| Years since diagnosis | Mean: 2.75 (SD 2.1) Median: 2.0 (IQR 3) | Range: 2–6 |
| Years of relationship | Mean: 41.7 (SD 13.0) Median: 41.0 (IQR 18.5) | Range: 30–53 |
| PwD age | Mean: 73.2 (SD 7.5) Median: 73 (IQR 11) Range: 34 (58–92) | Range: 58–78 |
| CG age | Mean: 69.6 (SD 8.2) Median: 71 (IQR 11.5) Range: 39 (50–89) | Range: 55–78 |
| PwD gender | Male: 50 (73.5%) Female: 18 (26.5%) | Male (4) |
| CG gender | Male: 18 (26.5%) Female: 50 (73.5%) | Female (4) |
| PwD education | Trade/community college(22), Bachelor’s degree(17), Master’s degree(12), Secondary/high school(11), Other(4), Doctor of philosophy(2) | Secondary/high school (2), Bachelor’s degree (1), Master’s degree (1) |
| PwD occupation | Professional(31), Technician(10), Manager(9), Service/sales(7), Clerical(4), Craft/trade(3), Machine operator(2), Armed forces(2) | Manager (2), Service/sales worker (1), Craft worker (1) |
| Baseline | Post Intervention | Difference | p-Value | 95%CI | |
|---|---|---|---|---|---|
| QCPR Score | Mean 54.07 (SD 8.5) Range 33 (37–70) | Mean 54.84 (SD 8.6) Range 32 (36–68) | 0.765 (SD 0.1) | 0.186 | −1.91–0.38 |
| Median 54 (IQR 12) | Median 55.5 (IQR 12.5) | 1.5 (IQR 0.5) |
| Couple 1 | Couple 2 | Couple 3 | Couple 4 | |
|---|---|---|---|---|
| QCPR pre intervention | 50 | 56 | 56 | 66 |
| QCPR post intervention | 52 | 56 | 65 | 55 |
| QCPR difference | 2 | 0 | 9 | −11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stedje, K.; Kvamme, T.S.; Johansson, K.; Sousa, T.V.; Odell-Miller, H.; Stensæth, K.A.; Bukowska, A.A.; Tamplin, J.; Wosch, T.; Baker, F.A. The Influence of Home-Based Music Therapy Interventions on Relationship Quality in Couples Living with Dementia—An Adapted Convergent Mixed Methods Study. Int. J. Environ. Res. Public Health 2023, 20, 2863. https://doi.org/10.3390/ijerph20042863
Stedje K, Kvamme TS, Johansson K, Sousa TV, Odell-Miller H, Stensæth KA, Bukowska AA, Tamplin J, Wosch T, Baker FA. The Influence of Home-Based Music Therapy Interventions on Relationship Quality in Couples Living with Dementia—An Adapted Convergent Mixed Methods Study. International Journal of Environmental Research and Public Health. 2023; 20(4):2863. https://doi.org/10.3390/ijerph20042863
Chicago/Turabian StyleStedje, Kristi, Tone Sæther Kvamme, Kjersti Johansson, Tanara Vieira Sousa, Helen Odell-Miller, Karette Annie Stensæth, Anna A. Bukowska, Jeanette Tamplin, Thomas Wosch, and Felicity Anne Baker. 2023. "The Influence of Home-Based Music Therapy Interventions on Relationship Quality in Couples Living with Dementia—An Adapted Convergent Mixed Methods Study" International Journal of Environmental Research and Public Health 20, no. 4: 2863. https://doi.org/10.3390/ijerph20042863
APA StyleStedje, K., Kvamme, T. S., Johansson, K., Sousa, T. V., Odell-Miller, H., Stensæth, K. A., Bukowska, A. A., Tamplin, J., Wosch, T., & Baker, F. A. (2023). The Influence of Home-Based Music Therapy Interventions on Relationship Quality in Couples Living with Dementia—An Adapted Convergent Mixed Methods Study. International Journal of Environmental Research and Public Health, 20(4), 2863. https://doi.org/10.3390/ijerph20042863