
Cost Sharing and Cost Shifting Mechanisms under a per Diem Payment System in a County of China


Abstract
1. Introduction
2. Institutional Background
3. Data and Methods
3.1. Data
3.2. Methods
4. Results
4.1. Difference-in-Differences Estimates on the Reform Impacts
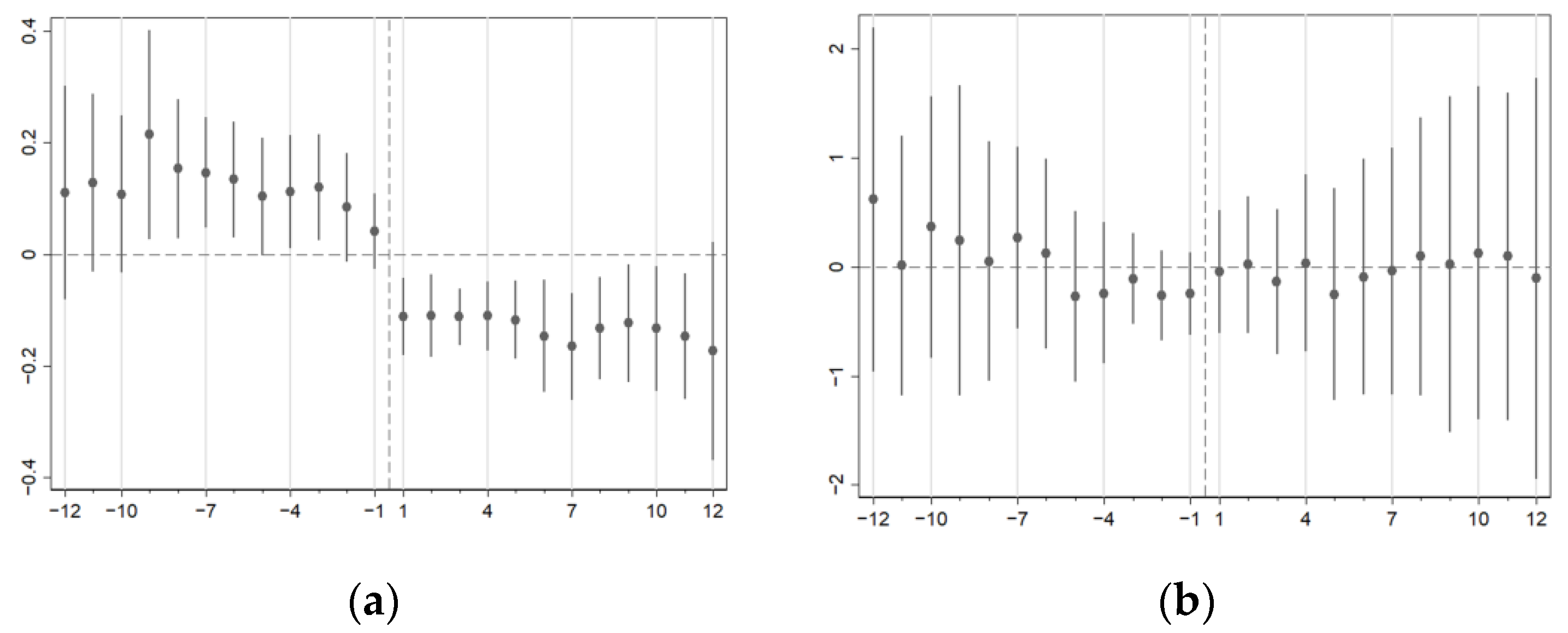
4.2. Robustness Check with Dynamic Estimates
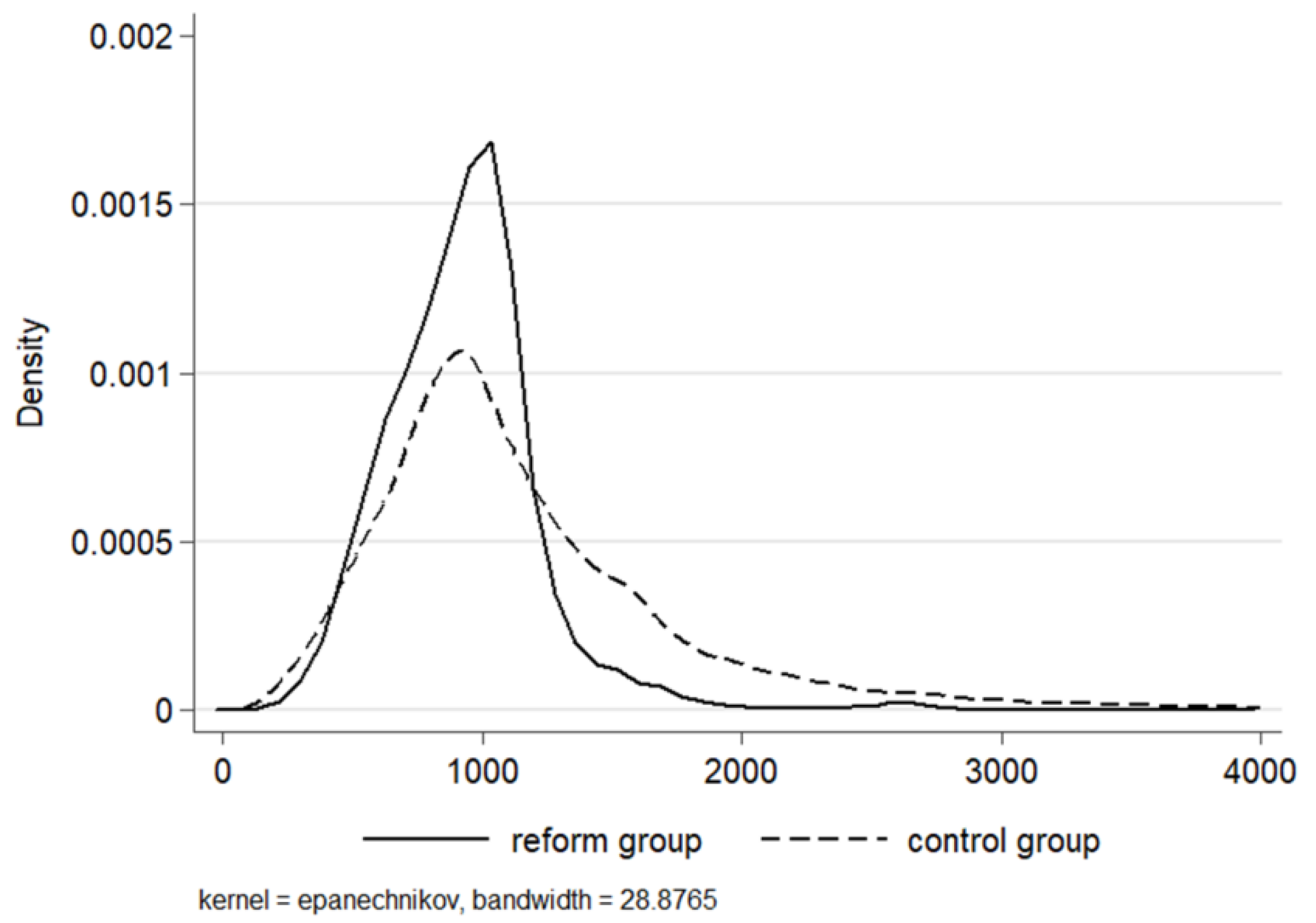
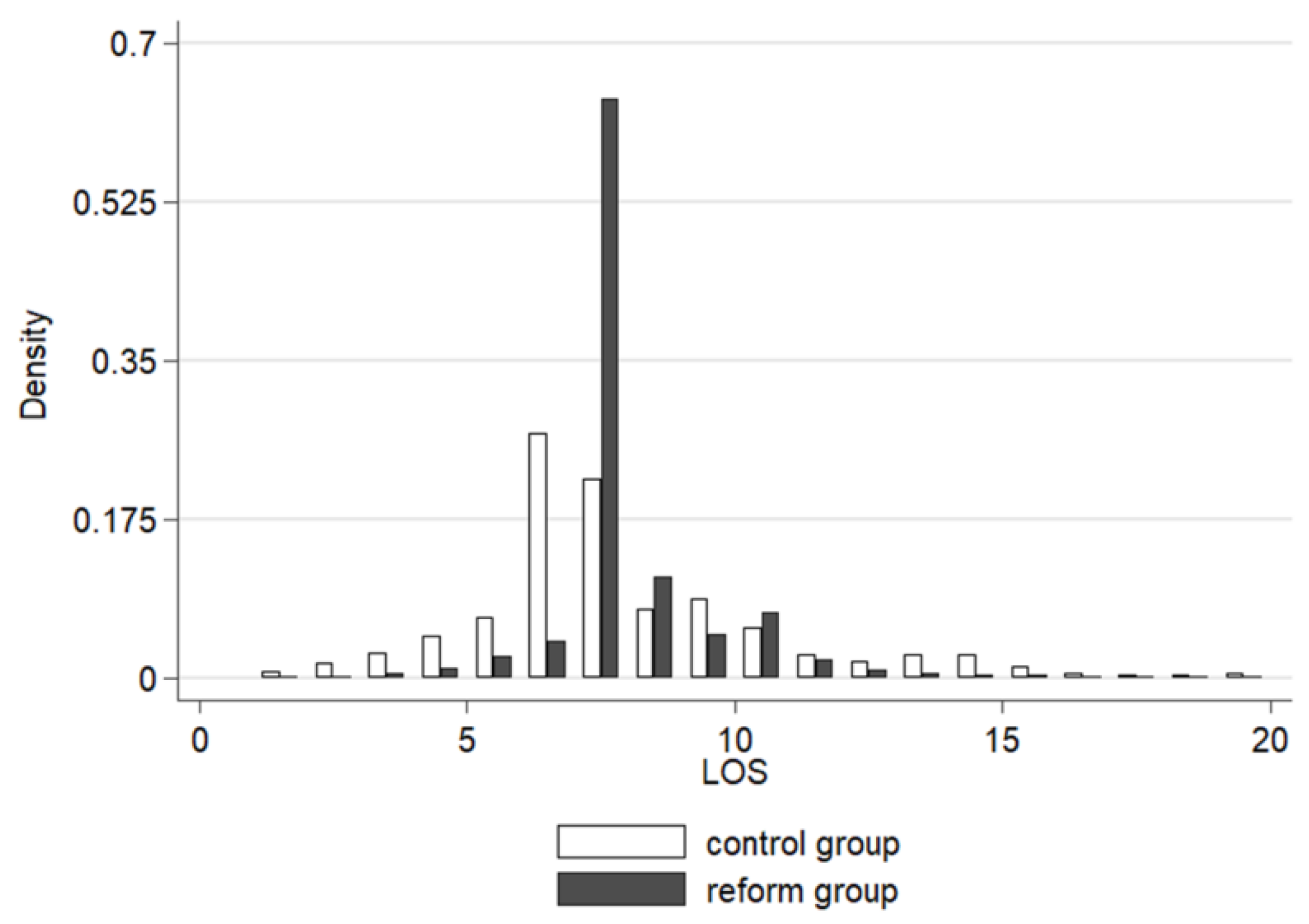
4.3. Heterogeneous Effects on Medical Costs and LOS
5. Discussions
Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medical Costs | |
|---|---|
| Reform | −0.0384 (0.0561) |
| Gender | −0.0198 ** (0.0083) |
| Age | 0.0157 *** (0.0033) |
| Age2 | −0.0001 *** (0.0000) |
| LOS | 0.0888 *** (0.0056) |
| Control variables | Yes |
| Hospital fixed effects | Yes |
| Time fixed effects | Yes |
| N | 28,021 |
| adj. R2 | 0.609 |
References
- McClellan, M. Reforming Payments to Healthcare Providers: The Key to Slowing Healthcare Cost Growth While Improving Quality? J. Econ. Perspect. 2011, 25, 69–92. [Google Scholar] [CrossRef]
- Robinson, J.C. Theory and practice in the design of physician payment incentives. Milbank Q. 2001, 79, 149–177. [Google Scholar] [CrossRef]
- Meng, Z.; Hui, W.; Cai, Y.; Liu, J.; Wu, H. The effects of DRGs-based payment compared with cost-based payment on inpatient healthcare utilization: A systematic review and meta-analysis. Health Policy 2020, 124, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Liu, C. Alternative payment models and physician treatment decisions: Evidence from lower back pain. J. Health Econ. 2021, 80, 102548. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, E.J.; Mostashari, F.; Navathe, A.S. Designing a Successful Primary Care Physician Capitation Model. JAMA 2021, 325, 2043–2044. [Google Scholar] [CrossRef] [PubMed]
- Dowling, W.L. Prospective reimbursement of hospitals. Inquiry 1974, 11, 163–180. [Google Scholar]
- Mayes, R. The origins, development, and passage of Medicare’s revolutionary prospective payment system. J. Hist. Med. Allied Sci. 2007, 62, 21–55. [Google Scholar] [CrossRef]
- Brekke, K.R.; Holmås, T.H.; Monstad, K.; Straume, O.R. Do treatment decisions depend on physicians’ financial incentives? J. Public Econ. 2017, 155, 74–92. [Google Scholar] [CrossRef]
- Ellis, R.P.; McGuire, T.G. Provider behavior under prospective reimbursement: Cost sharing and supply. J. Health Econ. 1986, 5, 129–151. [Google Scholar] [CrossRef]
- Albert Ma, C.T.; Riordan, M.H. Health insurance, moral hazard, and managed care. J. Econ. Manag. Strategy 2002, 11, 81–107. [Google Scholar] [CrossRef]
- Sülzle, K.; Wambach, A. Insurance in a market for credence goods. J. Risk Insur. 2005, 72, 159–176. [Google Scholar] [CrossRef]
- Ma, C.-T.A.; McGuire, T.G. Optimal health insurance and provider payment. Am. Econ. Rev. 1997, 87, 685–704. [Google Scholar]
- Trottmann, M.; Zweifel, P.; Beck, K. Supply-side and demand-side cost sharing in deregulated social health insurance: Which is more effective? J. Health Econ. 2012, 31, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Ellis, R.P. Creaming, skimping and dumping: Provider competition on the intensive and extensive margins. J. Health Econ. 1998, 17, 537–555. [Google Scholar] [CrossRef]
- Ellis, R.P.; McGuire, T.G. Supply-side and demand-side cost sharing in health care. J. Econ. Perspect. 1993, 7, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Kahn, K.L.; Keeler, E.B.; Sherwood, M.J.; Rogers, W.H.; Draper, D.; Bentow, S.S.; Reinisch, E.J.; Rubenstein, L.V.; Kosecoff, J.; Brook, R.H. Comparing outcomes of care before and after implementation of the DRG-based prospective payment system. Jama 1990, 264, 1984–1988. [Google Scholar] [CrossRef]
- Mayes, R.; Berenson, R.A. Medicare Prospective Payment and the Shaping of US Health Care; JHU Press: Baltimore, MD, USA, 2006. [Google Scholar]
- Jegers, M.; Kesteloot, K.; De Graeve, D.; Gilles, W. A typology for provider payment systems in health care. Health Policy 2002, 60, 255–273. [Google Scholar] [CrossRef]
- Ruggie, M. Health Care Systems: Comparative. In International Encyclopedia of the Social & Behavioral Sciences; Smelser, N.J., Baltes, P.B., Eds.; Pergamon: Oxford, UK, 2001; pp. 6537–6544. [Google Scholar]
- Busse, R.; Schwartz, F.W. Financing reforms in the German hospital sector - From full cost cover principle to prospective case fees. Med. Care 1997, 35, Os40–Os49. [Google Scholar] [CrossRef]
- Meyer, S. Payment schemes and cost efficiency: Evidence from Swiss public hospitals. Int. J. Health Econ. Manag. 2015, 15, 73–97. [Google Scholar] [CrossRef]
- Hamada, H.; Sekimoto, M.; Imanaka, Y. Effects of the per diem prospective payment system with DRG-like grouping system (DPC/PDPS) on resource usage and healthcare quality in Japan. Health Policy 2012, 107, 194–201. [Google Scholar] [CrossRef]
- W T Hanning, B. Combining DRGs and per diem payments in the private sector: The Equitable Payment Model. Aust. Health Rev. 2005, 29, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Okamura, S.; Kobayashi, R.; Sakamaki, T. Case-mix payment in Japanese medical care. Health Policy 2005, 74, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Aas, I.M. Incentives and financing methods. Health Policy 1995, 34, 205–220. [Google Scholar]
- Besstremyannaya, G. Differential Effects of Declining Rates in a Per Diem Payment System. Health Econ. 2016, 25, 1599–1618. [Google Scholar] [CrossRef]
- Nawata, K.; Kawabuchi, K. Evaluation of the DPC-based inclusive payment system in Japan for cataract operations by a new model. Math. Comput. Simul. 2013, 93, 76–85. [Google Scholar] [CrossRef]
- Ministry of Human Resources and Social Security of the People’s Republic of China; Ministry of Finance of the People’s Republic of China. The Notice of Public Institution Salary System Reform; Ministry of Human Resources and Social Security of the People’s Republic of China: Beijing, China, 2006.
- Xu, G.; Zhou, Z.; Zhu, N.; Chen, C. The analysis of doctors’ salary structure and its improving strategy: Based on Hospital A. Accountant 2021, 117–118. [Google Scholar]
- Zhang, H. The system and the problem of salary alloction in a tertiary hospital. Jiangsu Health Syst. Manag. 2022, 33, 1155–1158. [Google Scholar]
- The National Bureau of Statistics of the People’s Republic of China. Consumer Price Index for Health Care. Available online: https://data.stats.gov.cn/easyquery.htm?cn=C01 (accessed on 1 October 2022).
- Stabile, M.; Thomson, S.; Allin, S.; Boyle, S.; Busse, R.; Chevreul, K.; Marchildon, G.; Mossialos, E. Health care cost containment strategies used in four other high-income countries hold lessons for the United States. Health Aff. 2013, 32, 643–652. [Google Scholar] [CrossRef]
- Qian, M.; Zhang, X.; Chen, Y.; Xu, S.; Ying, X. The pilot of a new patient classification-based payment system in China: The impact on costs, length of stay and quality. Soc. Sci. Med. 2021, 289, 114415. [Google Scholar] [CrossRef]
- Lai, Y.; Fu, H.Q.; Li, L.; Yip, W. Hospital response to a case-based payment scheme under regional global budget: The case of Guangzhou in China. Soc. Sci. Med. 2022, 292, 114601. [Google Scholar] [CrossRef]
- Goodman-Bacon, A. Difference-in-differences with variation in treatment timing. J. Econom. 2021, 225, 254–277. [Google Scholar] [CrossRef]
- Wooldridge, J. What’s New in Econometrics? Lecture 10 Difference-in-Differences Estimation. NBER Summer Institute. Volume 9, p. 85. Available online: www.nber.org/WNE/Slides7–31–07/slides_10_diffindiffs.pdf (accessed on 11 July 2022).
- Beck, T.; Levine, R.; Levkov, A. Big Bad Banks? The Winners and Losers from Bank Deregulation in the United States. J. Financ. 2010, 65, 1637–1667. [Google Scholar] [CrossRef]
- Bronzini, R.; Piselli, P. The impact of R&D subsidies on firm innovation. Res. Policy 2016, 45, 442–457. [Google Scholar] [CrossRef]
- Arrow, K.J. Uncertainty and the welfare economics of medical care. In Uncertainty in Economics; Elsevier: Amsterdam, The Netherlands, 1978; pp. 345–375. [Google Scholar]
- Chen, A.; Lakdawalla, D.N. Saving Lives Or Saving Money?: Understanding the Dual Nature of Physician Preferences; National Bureau of Economic Research: Cambridge, MA, USA, 2016. [Google Scholar]
- Ellis, R.P.; McGuire, T.G. Hospital response to prospective payment: Moral hazard, selection, and practice-style effects. J. Health Econ. 1996, 15, 257–277. [Google Scholar] [CrossRef]
- Yip, W.C.-M.; Hsiao, W.; Meng, Q.; Chen, W.; Sun, X. Realignment of incentives for health-care providers in China. Lancet 2010, 375, 1120–1130. [Google Scholar] [CrossRef]




| Whole | Control Group | Reform Group | ||||
|---|---|---|---|---|---|---|
| Mean | S.D. | Mean | S.D. | Mean | S.D. | |
| Gender | 0.55 | 0.50 | 0.54 | 0.50 | 0.57 | 0.50 |
| Age | 58.74 | 14.12 | 56.89 | 15.38 | 61.05 | 11.97 |
| LOS | 7.56 | 2.72 | 7.60 | 3.34 | 7.53 | 1.64 |
| Medical costs | 1078.04 | 688.37 | 1187.79 | 815.71 | 940.19 | 446.30 |
| Medical Costs | LOS | |
|---|---|---|
| Reform | −0.1759 *** (0.0186) | 0.0249 (0.0448) |
| Gender | −0.0135 *** (0.0050) | −0.0300 *** (0.0069) |
| Age | 0.0138 *** (0.026) | −0.0061 *** (0.0019) |
| Age2 | −0.0001 *** (0.0000) | −0.0001 *** (0.0000) |
| LOS | −0.0915 *** (0.0049) | |
| Disease variables | Yes | Yes |
| Hospital fixed effects | Yes | Yes |
| Time fixed effects | Yes | Yes |
| n | 69,480 | 69,480 |
| adj. R2 | 0.582 |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| OLS | Q10 | Q20 | Q30 | Q40 | Q50 | Q60 | Q70 | Q80 | Q90 | |
| Reform | −0.1759 *** | −0.1072 *** | −0.1359 *** | −0.1500 *** | −0.1667 *** | −0.1814 *** | −0.1975 *** | −0.2114 *** | −0.2250 *** | −0.2287 *** |
| (0.0135) | (0.0109) | (0.0089) | (0.0079) | (0.0073) | (0.0068) | (0.0070) | (0.0070) | (0.0070) | (0.0091) | |
| Control variables | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES |
| Hospital fixed effects | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES |
| Time fixed effects | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES |
| N | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Poisson | Q10 | Q20 | Q30 | Q40 | Q50 | Q60 | Q70 | Q80 | Q90 | |
| Reform | 0.0249 | 0.1795 *** | 0.1458 *** | 0.1246 *** | 0.1038 *** | 0.0866 *** | 0.0670 *** | 0.0318 *** | −0.0339 *** | −0.1050 *** |
| (0.0448) | (0.0060) | (0.0035) | (0.0037) | (0.0040) | (0.0049) | (0.0045) | (0.0059) | (0.0086) | (0.0120) | |
| Control variables | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES |
| Hospital fixed effects | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES |
| Time fixed effects | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES |
| N | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 | 69,480 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, F.; Chen, J.; Li, C.; Xu, F. Cost Sharing and Cost Shifting Mechanisms under a per Diem Payment System in a County of China. Int. J. Environ. Res. Public Health 2023, 20, 2522. https://doi.org/10.3390/ijerph20032522
Liu F, Chen J, Li C, Xu F. Cost Sharing and Cost Shifting Mechanisms under a per Diem Payment System in a County of China. International Journal of Environmental Research and Public Health. 2023; 20(3):2522. https://doi.org/10.3390/ijerph20032522
Chicago/Turabian StyleLiu, Fengrong, Jiayu Chen, Chaozhu Li, and Fenghui Xu. 2023. "Cost Sharing and Cost Shifting Mechanisms under a per Diem Payment System in a County of China" International Journal of Environmental Research and Public Health 20, no. 3: 2522. https://doi.org/10.3390/ijerph20032522
APA StyleLiu, F., Chen, J., Li, C., & Xu, F. (2023). Cost Sharing and Cost Shifting Mechanisms under a per Diem Payment System in a County of China. International Journal of Environmental Research and Public Health, 20(3), 2522. https://doi.org/10.3390/ijerph20032522