
HIV-Exposed Uninfected Children: A Systematic Review on Psychological Well-Being and Association with School Performances in Africa

 , , and
, , and 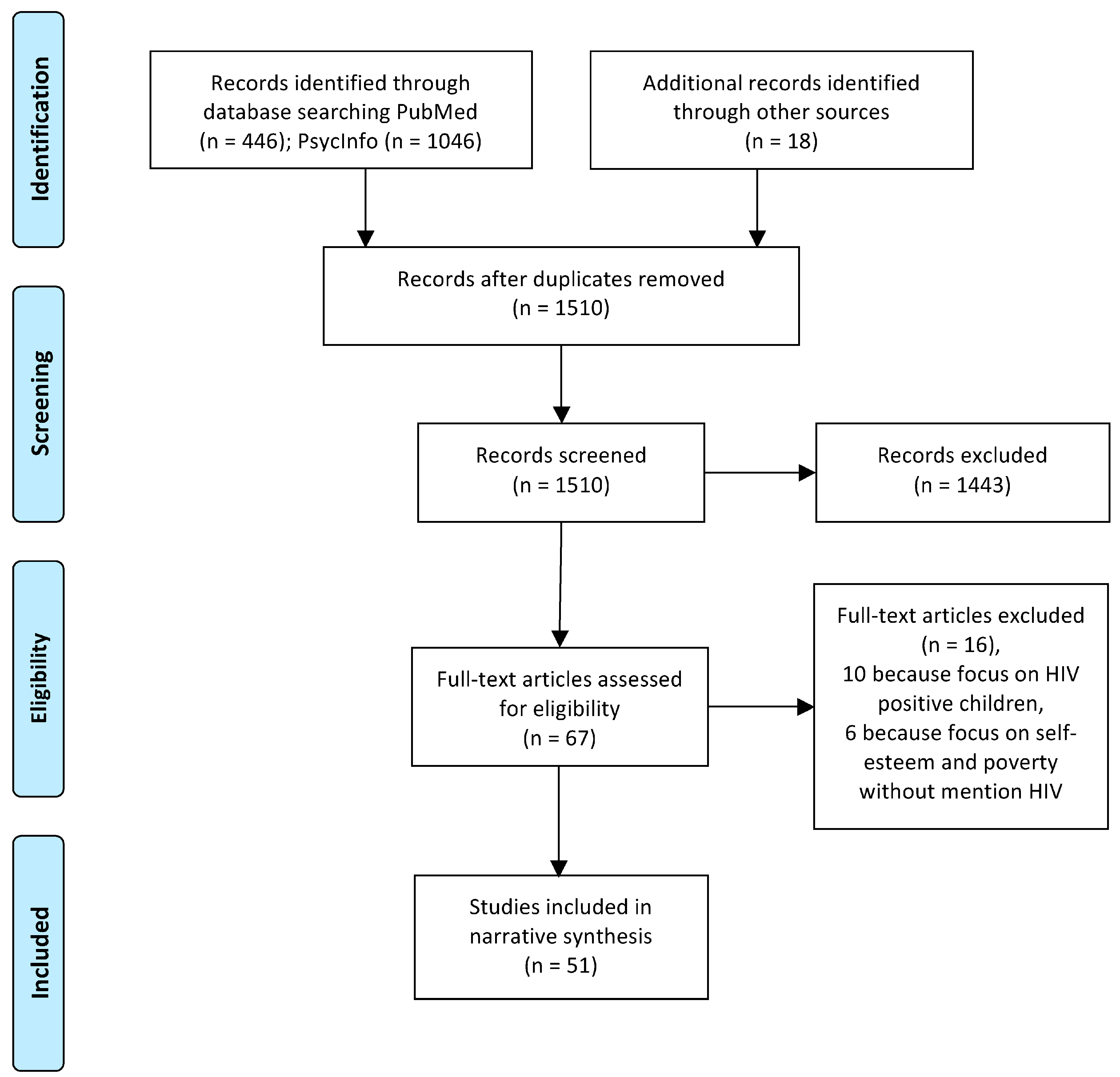{kind=link}
Abstract
1. Introduction
2. Methods
Literature Research
3. Results
3.1. Individual Factors
3.2. Self-Esteem and Resilience
3.3. Depression
3.4. Gender Differences in School Outcomes
3.5. Cognitive Abilities
3.6. Family Factors
Family and Parental Support
3.7. Social Factors and School Environment
Risk and Protective Factors
3.8. Educational Outcomes
3.9. Interventions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Joint Programme on HIV/AIDS (UNAIDS). Global HIV Statistics. Available online: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf (accessed on 26 December 2021).
- The Joint Programme on HIV/AIDS (UNAIDS). Country: Eswatini. Available online: https://www.unaids.org/en/regionscountries/countries/eswatini (accessed on 26 December 2021).
- The Joint Programme on HIV/AIDS (UNAIDS). Country: Lesotho. Available online: https://www.unaids.org/en/regionscountries/countries/lesotho (accessed on 26 December 2021).
- The Joint Programme on HIV/AIDS (UNAIDS). Country: South Africa. Available online: https://www.unaids.org/en/regionscountries/countries/southafrica (accessed on 26 December 2021).
- The Joint Programme on HIV/AIDS (UNAIDS). Country: Botswana. Available online: https://www.unaids.org/en/regionscountries/countries/botswana (accessed on 26 December 2021).
- The Joint Programme on HIV/AIDS (UNAIDS). Country: Nigeria. Available online: https://www.unaids.org/en/regionscountries/countries/nigeria (accessed on 26 December 2021).
- Slogrove, A.L.; Powis, K.M.; Johnson, L.F.; Stover, J.; Mahy, M. Estimates of the global population of children who are HIV-exposed and uninfected, 2000–2018: A modelling study. Lancet Glob. Health 2020, 8, e67–e75. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, C.A.; Marais, B.J.; Abrams, E.J. HIV: Prevention of mother-to-child transmission. BMJ Clin. Evid. 2011, 2011, 0909. [Google Scholar] [PubMed]
- Barron, P.; Pillay, Y.; Doherty, T.; Sherman, G.; Jackson, D.; Bhardwaj, S.; Robinson, P.; Goga, A. Eliminating mother-to-child HIV transmission in South Africa. Bull. World Health Organ. 2013, 91, 70–74. [Google Scholar] [CrossRef]
- Filteau, S. The HIV-exposed, uninfected African child. Trop. Med. Int. Health 2009, 14, 276–287. [Google Scholar] [CrossRef] [PubMed]
- Van Rie, A.; Mupuala, A.; Dow, A. Impact of the HIV/AIDS epidemic on the neurodevelopment of preschool-aged children in Kinshasa, Democratic Republic of the Congo. Pediatrics 2008, 122, e123–e128. [Google Scholar] [CrossRef] [PubMed]
- Boivin, M.J.; Maliwichi-Senganimalunje, L.; Ogwang, L.W.; Kawalazira, R.; Sikorskii, A.; Familiar-Lopez, I.; Kuteesa, A.; Nyakato, M.; Mutebe, A.; Namukooli, J.L.; et al. Neurodevelopmental effects of ante-partum and post-partum antiretroviral exposure in HIV-exposed and uninfected children versus HIV-unexposed and uninfected children in Uganda and Malawi: A prospective cohort study. Lancet HIV 2019, 6, e518–e530. [Google Scholar] [CrossRef]
- Bass, J.K.; Nakasujja, N.; Familiar-Lopez, I.; Sikorskii, A.; Murray, S.M.; Opoka, R.; Augustinavicius, J.; Boivin, M.J. Association of caregiver quality of care with neurocognitive outcomes in HIV-affected children aged 2–5 years in Uganda. AIDS Care 2016, 28, 76–83. [Google Scholar] [CrossRef]
- Wedderburn, C.J.; Evans, C.; Yeung, S.; Gibb, D.M.; Donald, K.A.; Prendergast, A.J. Growth and Neurodevelopment of HIV-Exposed Uninfected Children: A Conceptual Framework. Curr. HIV/AIDS Rep. 2019, 16, 501–513. [Google Scholar] [CrossRef]
- Powis, K.M.; Smeaton, L.; Hughes, M.D.; Tumbare, E.A.; Souda, S.; Jao, J.; Wirth, K.E.; Makhema, J.; Lockman, S.; Fawzi, W.; et al. In-utero triple antiretroviral exposure associated with decreased growth among HIV-exposed uninfected infants in Botswana. AIDS (Lond. Engl.) 2016, 30, 211–220. [Google Scholar] [CrossRef]
- Coelho, A.V.; Tricarico, P.M.; Celsi, F.; Crovella, S. Antiretroviral Treatment in HIV-1-Positive Mothers: Neurological Implications in Virus-Free Children. Int. J. Mol. Sci. 2017, 18, 423. [Google Scholar] [CrossRef]
- McCoy, D.C.; Peet, E.D.; Ezzati, M.; Danaei, G.; Black, M.M.; Sudfeld, C.R.; Fawzi, W.; Fink, G. Early Childhood Developmental Status in Low- and Middle-Income Countries: National, Regional, and Global Prevalence Estimates Using Predictive Modeling. PLoS Med. 2016, 13, e1002034. [Google Scholar] [CrossRef]
- Nordtveit, B.H. Schools as agencies of protection in Namibia and Swaziland: Can they prevent dropout and child labour in the context of HIV/AIDS and poverty? Comp. Educ. Rev. 2010, 54, 223–242. [Google Scholar] [CrossRef][Green Version]
- Cluver, L.; Gardner, F.; Operario, D. Poverty and psychological health among AIDS-orphaned children in Cape Town, South Africa. AIDS Care 2009, 21, 732–741. [Google Scholar] [CrossRef] [PubMed]
- Han, C.K.; Ssewamala, F.M.; Wang, J.S. Family economic empowerment and mental health among AIDS-affected children living in AIDS-impacted communities: Evidence from a randomised evaluation in southwestern Uganda. J. Epidemiol. Community Health 2013, 67, 225–230. [Google Scholar] [CrossRef]
- Betancourt, T.S.; Ng, L.C.; Kirk, C.M.; Munyanah, M.; Mushashi, C.; Ingabire, C.; Teta, S.; Beardslee, W.R.; Brennan, R.T.; Zahn, I.; et al. Family-based prevention of mental health problems in children affected by HIV and AIDS: An open trial. AIDS (Lond. Engl.) 2014, 28, S359–S368. [Google Scholar] [CrossRef]
- Govender, K.; Reardon, C.; Quinlan, T.; George, G. Children’s psychosocial wellbeing in the context of HIV/AIDS and poverty: A comparative investigation of orphaned and non-orphaned children living in South Africa. BMC Public Health 2014, 14, 615. [Google Scholar] [CrossRef] [PubMed]
- Skovdal, M. “It’s because they care”: Understanding pathways to classroom concentration problems among HIV-affected children and youth in Western Kenya. AIDS Care 2016, 28, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Li, X.; Sherr, L. The impact of HIV/AIDS on children’s educational outcome: A critical review of global literature. AIDS Care 2012, 24, 993–1012. [Google Scholar] [CrossRef]
- Adler, A. Teaching Well-Being Increases Academic Performance: Evidence from Bhutan, Mexico, and Peru. University of Pennsylvania Dissertation. 2016. Available online: https://repository.upenn.edu/edissertations/1572/ (accessed on 17 October 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Betancourt, T.; Scorza, P.; Kanyanganzi, F.; Fawzi, M.C.; Sezibera, V.; Cyamatare, F.; Beardslee, W.; Stulac, S.; Bizimana, J.I.; Stevenson, A.; et al. HIV and Child Mental Health: A Case-Control Study in Rwanda. Pediatrics 2014, 134, e464–e472. [Google Scholar] [CrossRef]
- Mueller, J.; Alie, C.; Jonas, B.; Brown, E.; Sherr, L. A quasi-experimental evaluation of a community-based art therapy intervention exploring the psychosocial health of children affected by HIV in South Africa. Trop. Med. Int. Health 2011, 16, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Skeen, S.; Macedo, A.; Tomlinson, M.; Hensels, I.S.; Sherr, L. Exposure to violence and psychological well-being over time in children affected by HIV/AIDS in South Africa and Malawi. AIDS Care 2016, 28, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Okawa, S.; Yasuoka, J.; Ishikawa, N.; Poudel, K.C.; Ragi, A.; Jimba, M. Perceived social support and the psychological well-being of AIDS orphans in urban Kenya. AIDS Care 2011, 23, 1177–1185. [Google Scholar] [CrossRef]
- Collishaw, S.; Gardner, F.; Lawrence Aber, J.; Cluver, L. Predictors of Mental Health Resilience in Children who Have Been Parentally Bereaved by AIDS in Urban South Africa. J. Abnorm. Child Psychol. 2016, 44, 719–730. [Google Scholar] [CrossRef]
- Small, L.A.; Parchment, T.M.; Bahar, O.S.; Osuji, H.L.; Chomanczuk, A.H.; Bhana, A. South African adult caregivers as “protective shields”: Serving as a buffer between stressful neighborhood conditions and youth risk behaviors. J. Community Psychol. 2019, 47, 1850–1864. [Google Scholar] [CrossRef]
- Ashry, M.; Ziady, H.; Hameed, M.; Mohammed, F. Health-related quality of life in healthy children and adolescents of HIV-infected parents in Alexandria, Egypt. J. Egypt. Public Health Assoc. 2017, 92, 212–219. [Google Scholar] [CrossRef]
- Sherr, L.; Croome, N.; Clucas, C.; Brown, E. Differential effects of single and double parental death on child emotional functioning and daily life in South Africa. Child Welf. 2014, 93, 149–172. [Google Scholar]
- Sipsma, H.; Eloff, I.; Makin, J.; Finestone, M.; Ebersohn, L.; Visser, M.J.; Sikkema, K.J.; Allen, C.A.; Ferreira, R.; Forsyth, B. Behavior and psychological functioning of young children of HIV-positive mothers in South Africa. AIDS Care 2013, 25, 721–725. [Google Scholar] [CrossRef] [PubMed]
- Cluver, L.; Gardner, F.; Operario, D. Psychological distress amongst AIDS-orphaned children in urban South Africa. J. Child Psychol. Psychiatry 2007, 48, 755–763. [Google Scholar] [CrossRef]
- Cluver, L.; Gardner, F.; Operario, D. Effects of stigma on the mental health of adolescents orphaned by AIDS. J. Adolesc. Health 2008, 42, 410–417. [Google Scholar] [CrossRef]
- Cluver, L.; Orkin, M. Cumulative risk and AIDS-orphanhood: Interactions of stigma, bullying and poverty on child mental health in South Africa. Soc. Sci. Med. 2009, 69, 1186–1193. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, T.S.; Rubin-Smith, J.E.; Beardslee, W.R.; Stulac, S.N.; Fayida, I.; Safren, S. Understanding locally, culturally, and contextually relevant mental health problems among Rwandan children and adolescents affected by HIV/AIDS. AIDS Care 2011, 23, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Thurman, T.R.; Kidman, R.; Taylor, T.M. Does investment in home visitors lead to better psychological health for HIV-affected families? Results from a quasi-experimental evaluation in South Africa. AIDS Care 2014, 26, S2–S10. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hensels, I.S.; Sherr, L.; Skeen, S.; Macedo, A.; Roberts, K.J.; Tomlinson, M. Do not forget the boys-gender differences in children living in high HIV-affected communities in South Africa and Malawi in a longitudinal, community-based study. AIDS Care 2016, 28, 100–109. [Google Scholar] [CrossRef]
- Orkin, M.; Boyes, M.E.; Cluver, L.D.; Zhang, Y. Pathways to poor educational outcomes for HIV/AIDS-affected youth in South Africa. AIDS Care 2014, 26, 343–350. [Google Scholar] [CrossRef]
- Sharp, C.; Penner, F.; Marais, L.; Skinner, D. School connectedness as psychological resilience factor in children affected by HIV/AIDS. AIDS Care 2018, 30, 34–41. [Google Scholar] [CrossRef]
- Sherr, L.; Macedo, A.; Tomlinson, M.; Skeen, S.; Cluver, L.D. Could cash and good parenting affect child cognitive development? A cross-sectional study in South Africa and Malawi. BMC Pediatr. 2017, 17, 123. [Google Scholar] [CrossRef]
- Nabunya, P.; Ssewamala, F.M. The Effects of Parental Loss on the Psychosocial Wellbeing of AIDS-Orphaned Children Living in AIDS-Impacted Communities: Does Gender Matter? Child. Youth Serv. Rev. 2014, 43, 131–137. [Google Scholar] [CrossRef]
- Milligan, R.; Cockcroft, K. Working Memory Profiles in HIV-Exposed, Uninfected and HIV-Infected Children: A Comparison with Neurotypical Controls. Front. Hum. Neurosci. 2017, 11, 348. [Google Scholar] [CrossRef]
- Ezeamama, A.E.; Kizza, F.N.; Zalwango, S.K.; Nkwata, A.K.; Zhang, M.; Rivera, M.L.; Sekandi, J.N.; Kakaire, R.; Kiwanuka, N.; Whalen, C.C. Perinatal HIV Status and Executive Function During School-Age and Adolescence: A Comparative Study of Long-Term Cognitive Capacity Among Children From a High HIV Prevalence Setting. Med. (Baltim.) 2016, 95, e3438. [Google Scholar] [CrossRef]
- Nkwata, A.K.; Zalwango, S.K.; Kizza, F.N.; Sekandi, J.N.; Mutanga, J.; Zhang, M.; Musoke, P.M.; Ezeamama, A.E. Quality of life among perinatally HIV-affected and HIV-unaffected school-aged and adolescent Ugandan children: A multi-dimensional assessment of wellbeing in the post-HAART era. Qual. Life Res. 2017, 26, 2397–2408. [Google Scholar] [CrossRef] [PubMed]
- Boivin, M.J. Culture–specific neurodevelopmental assessment of HIV-affected children. NIH RePORTER, 2019; work in progress. [Google Scholar]
- Lowenthal, E.D.; Scott, J.C. A computerized neurocognitive battery for use in youth affected by HIV in resource-limited settings. NIH RePORTER, 2018; work in progress. [Google Scholar]
- Robb, M.L. Determinants of resilience in youth with HIV infection and youth affected by HIV. NIH RePORTER, 2018; work in progress. [Google Scholar]
- Cluver, L.; Operario, D.; Lane, T.; Kganakga, M. “I Can’t Go to School and Leave Her in So Much Pain”: Educational Shortfalls Among Adolescent ‘Young Carers’ in the South African AIDS Epidemic. J. Adolesc. Res. 2012, 27, 581–586. [Google Scholar] [CrossRef]
- Kagotho, N.; Ssewamala, F.M. Correlates of depression among caregivers of children affected by HIV/AIDS in Uganda: Findings from the Suubi-Maka family study. AIDS Care 2012, 24, 1226–1232. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lachman, J.M.; Cluver, L.D.; Boyes, M.E.; Kuo, C.; Casale, M. Positive parenting for positive parents: HIV/AIDS, poverty, caregiver depression, child behavior, and parenting in South Africa. AIDS Care 2014, 26, 304–313. [Google Scholar] [CrossRef]
- Casale, M.; Cluver, L.; Crankshaw, T.; Kuo, C.; Lachman, J.M.; Wild, L.G. Direct and Indirect Effects of Caregiver Social Support on Adolescent Psychological Outcomes in Two South African AIDS-Affected Communities. Am. J. Community Psychol. 2015, 55, 336–346. [Google Scholar] [CrossRef]
- Nalugya, R.; Russell, S.; Zalwango, F.; Seeley, J. The role of children in their HIV-positive parents’ management of antiretroviral therapy in Uganda. Afr. J. AIDS Res. 2018, 17, 37–46. [Google Scholar] [CrossRef]
- Webster, K.D.; de Bruyn, M.M.; Zalwango, S.K.; Sikorskii, A.; Barkin, J.L.; Familiar-Lopez, I.; Musoke, P.; Giordani, B.; Boivin, M.J.; Ezeamama, A.E. Caregiver socioemotional health as a determinant of child well-being in school-aged and adolescent Ugandan children with and without perinatal HIV exposure. Trop. Med. Int. Health 2019, 24, 608–619. [Google Scholar] [CrossRef]
- Barenbaum, E.; Smith, T. Social support as a protective factor for children impacted by HIV/AIDS across varying living environments in southern Africa. AIDS Care 2016, 28, 92–99. [Google Scholar] [CrossRef]
- UNICEF. Life Skills: Child Friendly Schools. Available online: http://www.unicef.org/lifeskills/index_7260.html (accessed on 18 November 2021).
- Watkins, J.A.; Sello, M.; Cluver, L.; Boyes, M.; Kaplan, L. ‘At school I got myself a certificate’: HIV/AIDS Orphanhood and Secondary Education: A Qualitative Study of Risk and Protective Factors. Glob. Soc. Welf. 2014, 1, 111–121. [Google Scholar] [CrossRef][Green Version]
- Scorza, P.; Duarte, C.S.; Stevenson, A.; Mushashi, C.; Kanyanganzi, F.; Munyana, M.; Betancourt, T.S. Individual-level factors associated with mental health in Rwandan youth affected by HIV/AIDS. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 867–875. [Google Scholar] [CrossRef]
- Campbell, C.; Andersen, L.; Mutsikiwa, A.; Madanhire, C.; Skovdal, M.; Nyamukapa, C.; Gregson, S. Children’s representations of school support for HIV-affected peers in rural Zimbabwe. BMC Public Health 2014, 14, 402. [Google Scholar] [CrossRef] [PubMed]
- Anabwni, G.; Karugaba, G.; Gabaitiri, L. Health, schooling, needs, perspectives and aspirations of HIV infected and affected children in Botswana: A cross-sectional survey. BMC Pediatr. 2016, 16, 106. [Google Scholar] [CrossRef]
- Visser, M.; Finestone, M.; Sikkema, K.; Boeving-Allen, A.; Ferreira, R.; Eloff, I.; Forsyth, B. Development and piloting of a mother and child intervention to promote resilience in young children of HIV-infected mothers in South Africa. Eval. Program Plan. 2012, 35, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Pufall, E.L.; Gregson, S.; Eaton, J.W.; Masoka, T.; Mpandaguta, E.; Andersen, L.; Skovdal, M.; Nyamukapa, C.; Campbell, C. The contribution of schools to supporting the well being of children affected by HIV in eastern Zimbabwe. AIDS 2014, 28, S379–S387. [Google Scholar] [CrossRef]
- Nicholson, L.; Chisenga, M.; Siame, J.; Kasonka, L.; Filteau, S. Growth and health outcomes at school age in HIV-exposed, uninfected Zambian children: Follow-up of two cohorts studied in infancy. BMC Pediatr. 2015, 15, 66. [Google Scholar] [CrossRef]
- Phaladze, N.A.; Ngwenya, B.N.; Gabaitiri, L. Orphans’ perspectives on grief and loss in Botswana. AIDS Care 2018, 30, 506–510. [Google Scholar] [CrossRef]
- Katisi, M.; Jefferies, P.; Dikolobe, O.; Moeti, O.; Brisson, J.; Ungar, M. Fostering Resilience in Children Who have been Orphaned: Preliminary results from the Botswana Balekane EARTH Program. Child Youth Care Forum 2019, 48, 585–601. [Google Scholar] [CrossRef]
- Ssewamala, F.M.; Karimli, L.; Torsten, N.; Wang, J.S.; Han, C.K.; Ilic, V.; Nabunya, P. Applying a Family-Level Economic Strengthening Intervention to Improve Education and Health-Related Outcomes of School-Going AIDS-Orphaned Children: Lessons from a Randomized Experiment in Southern Uganda. Prev. Sci. 2016, 17, 134–143. [Google Scholar] [CrossRef]
- Sherr, L.; Tomlinson, M.; Macedo, A.; Skeen, S.; Hensels, I.S.; Cluver, L.D. Can cash break the cycle of educational risks for young children in high HIV-affected communities? A cross-sectional study in South Africa and Malawi. J. Glob. Health 2017, 7, 020409. [Google Scholar] [CrossRef]
- Cvencek, D.; Fryberg, S.A.; Covarrubias, R.; Meltzoff, A.N. Self-Concepts, Self-Esteem, and Academic Achievement of Minority and Majority North American Elementary School Children. Child Dev. 2018, 89, 1099–1109. [Google Scholar] [CrossRef]
- Peterson, A.K.; Fox, C.B.; Israelsen, M. A Systematic Review of Academic Discourse Interventions for School-Aged Children With Language-Related Learning Disabilities. Lang. Speech Hear. Serv. Sch. 2020, 51, 866–881. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, T.S.; Meyers-Ohki, S.E.; Charrow, A.; Hansen, N. Annual Research Review: Mental health and resilience in HIV/AIDS-affected children—A review of the literature and recommendations for future research. J. Child Psychol. Psychiatry 2013, 54, 423–444. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mensi, M.; Ahishakiye, A.; Journeay, K.; Baiocco, R.; Betancourt, T.S.; Paganotti, G.M. HIV-Exposed Uninfected Children: A Systematic Review on Psychological Well-Being and Association with School Performances in Africa. Int. J. Environ. Res. Public Health 2023, 20, 2499. https://doi.org/10.3390/ijerph20032499
Mensi M, Ahishakiye A, Journeay K, Baiocco R, Betancourt TS, Paganotti GM. HIV-Exposed Uninfected Children: A Systematic Review on Psychological Well-Being and Association with School Performances in Africa. International Journal of Environmental Research and Public Health. 2023; 20(3):2499. https://doi.org/10.3390/ijerph20032499
Chicago/Turabian StyleMensi, Marina, Alain Ahishakiye, Katharine Journeay, Roberto Baiocco, Theresa Stichick Betancourt, and Giacomo M. Paganotti. 2023. "HIV-Exposed Uninfected Children: A Systematic Review on Psychological Well-Being and Association with School Performances in Africa" International Journal of Environmental Research and Public Health 20, no. 3: 2499. https://doi.org/10.3390/ijerph20032499
APA StyleMensi, M., Ahishakiye, A., Journeay, K., Baiocco, R., Betancourt, T. S., & Paganotti, G. M. (2023). HIV-Exposed Uninfected Children: A Systematic Review on Psychological Well-Being and Association with School Performances in Africa. International Journal of Environmental Research and Public Health, 20(3), 2499. https://doi.org/10.3390/ijerph20032499