
Present and Future Drinking Water Security and Its Impacts on Maternities: A Multi-Scale Assessment of Sudan




Abstract
1. Introduction
2. Methods
2.1. Study Area—Sudan
2.2. Composite Drinking Water Security Index (DWSI)
2.3. Sources and Preparation of DWSI Variables
2.3.1. Water Supply Statistics at the State Level
- 1.
- Drinking water source: percentage of the population with access to an improved water source (i.e., designed to be protected from outside contamination, especially fecal contamination). The types of improved water sources are piped water (into dwelling, compound, yard, or plot, to neighbor, public tap/standpipe), tube well/borehole, protected well, protected spring, and rainwater collection.
- 2.
- Water treatment: percentage of the population using an unimproved water source but using adequate water treatment.
- 3.
- Water fetching time: percentage of the population with water fetching time of less than 30 min. Water fetching time includes waiting in line and can be from either an improved or unimproved water source.
2.3.2. Maternities and Primary Water Source
2.3.3. Groundwater Dataset
2.3.4. Climate Data
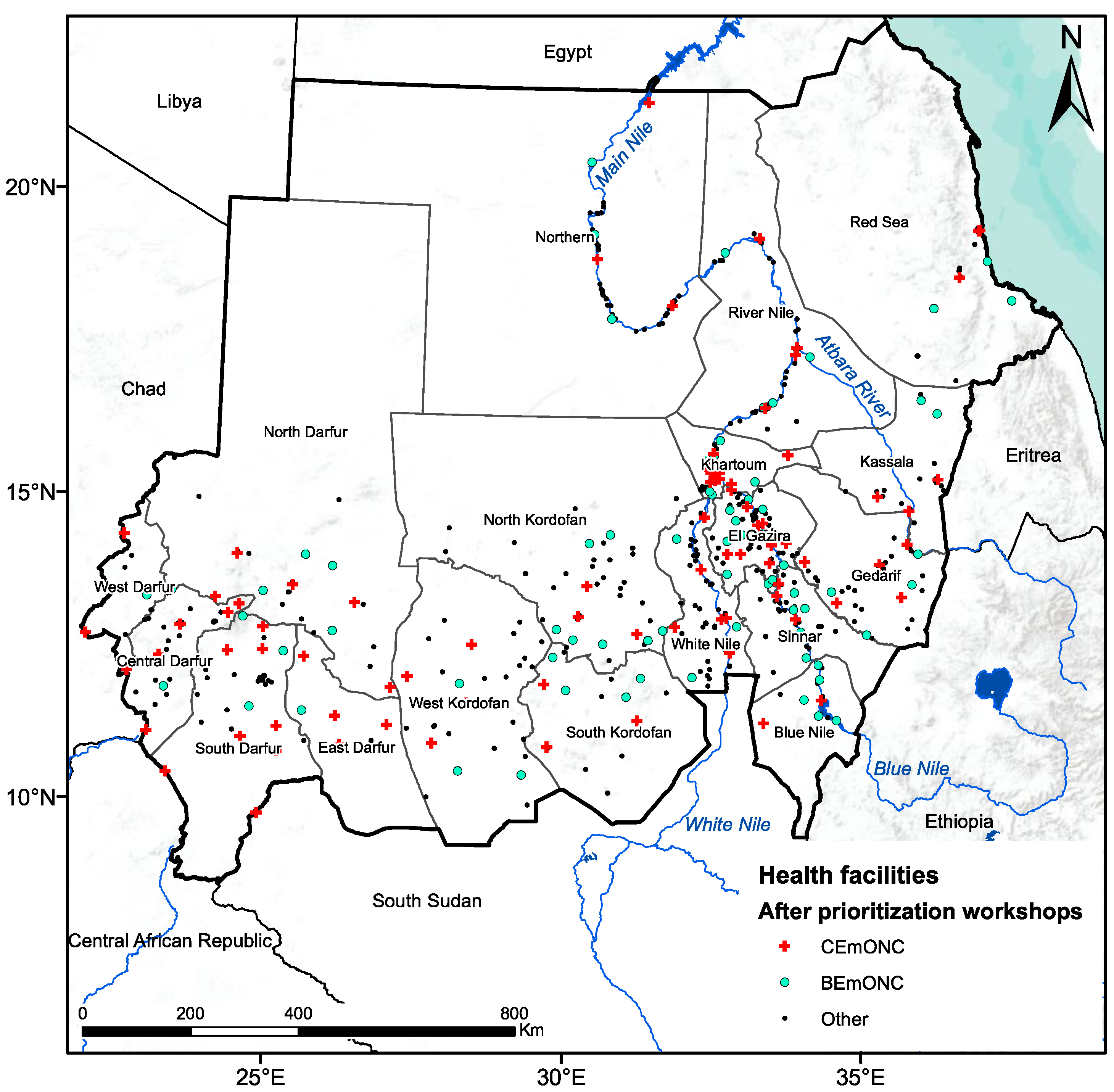
2.4. Geographic Accessibility and Population Coverage of EmONC Facilities
3. Results
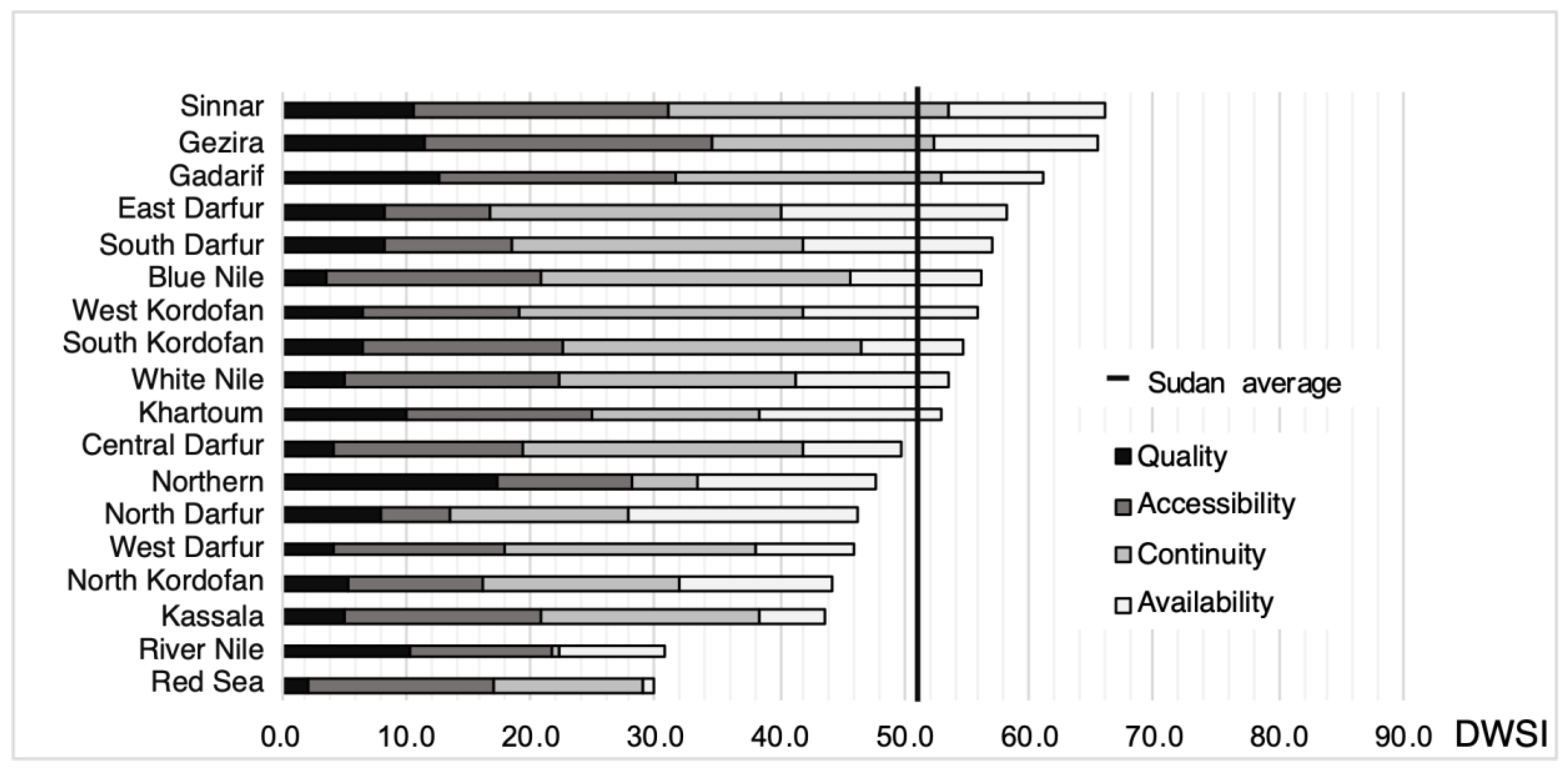
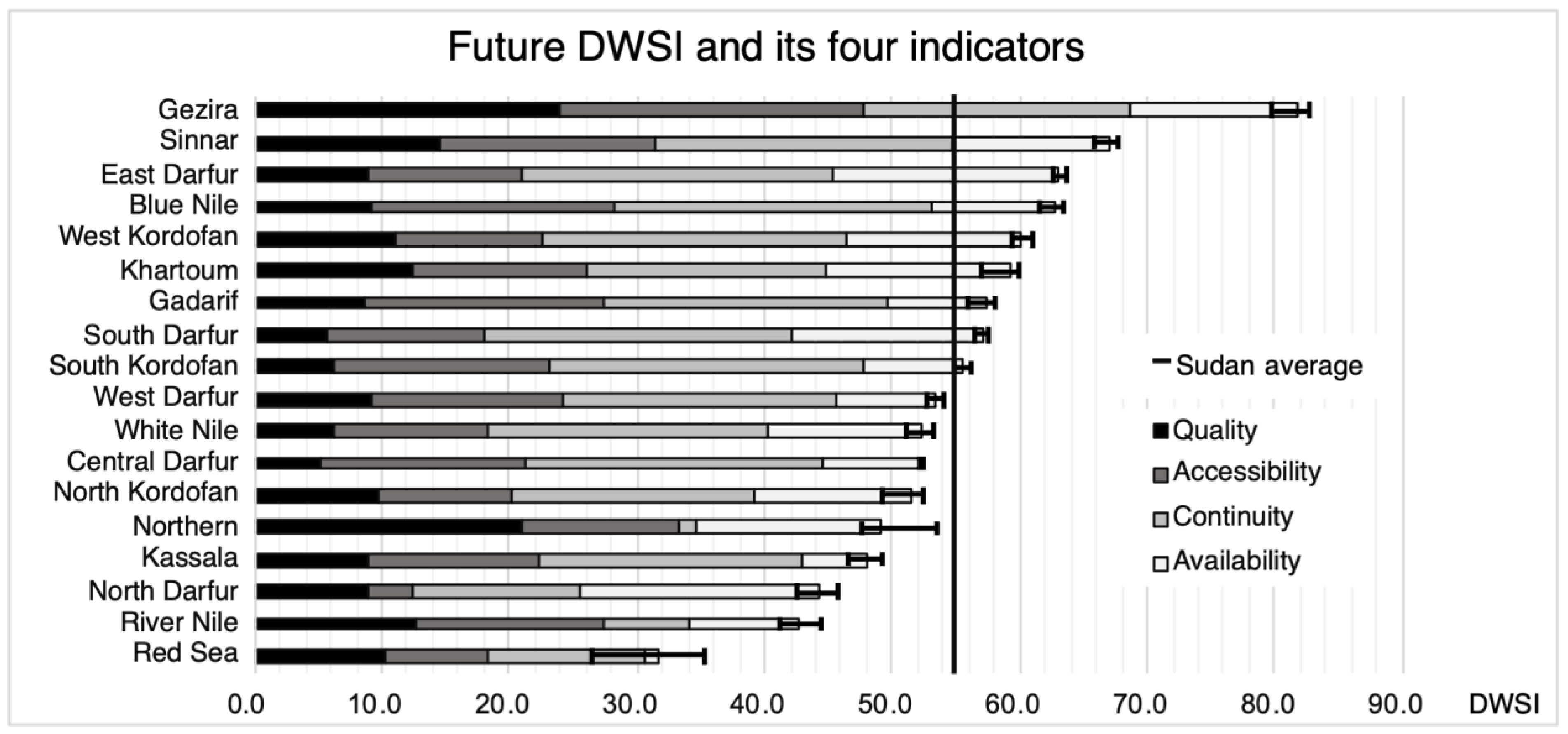
3.1. Assessment of DWSI at State Level
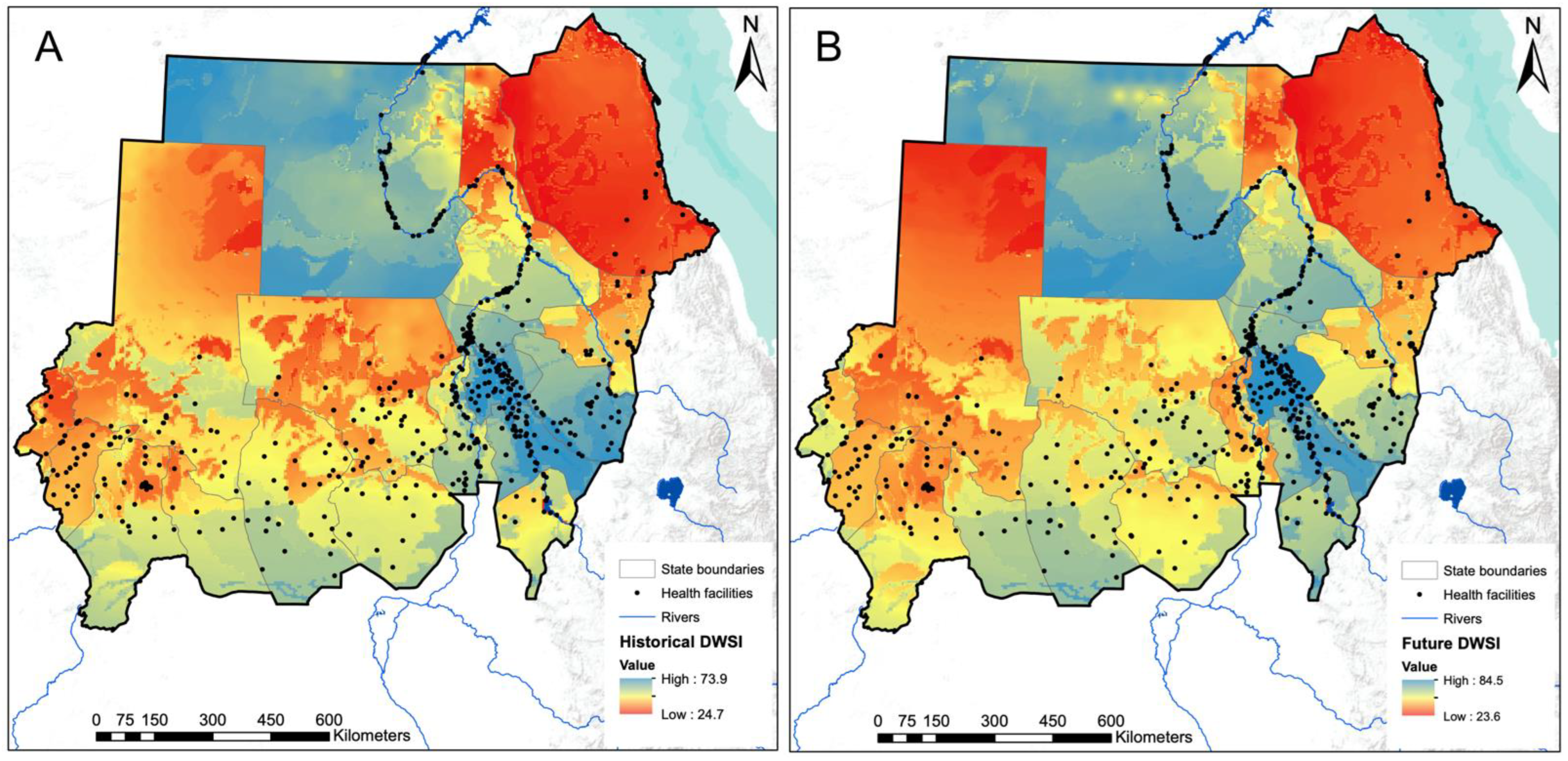
3.2. Assessment of DWSI at 1 km2 Pixel Level
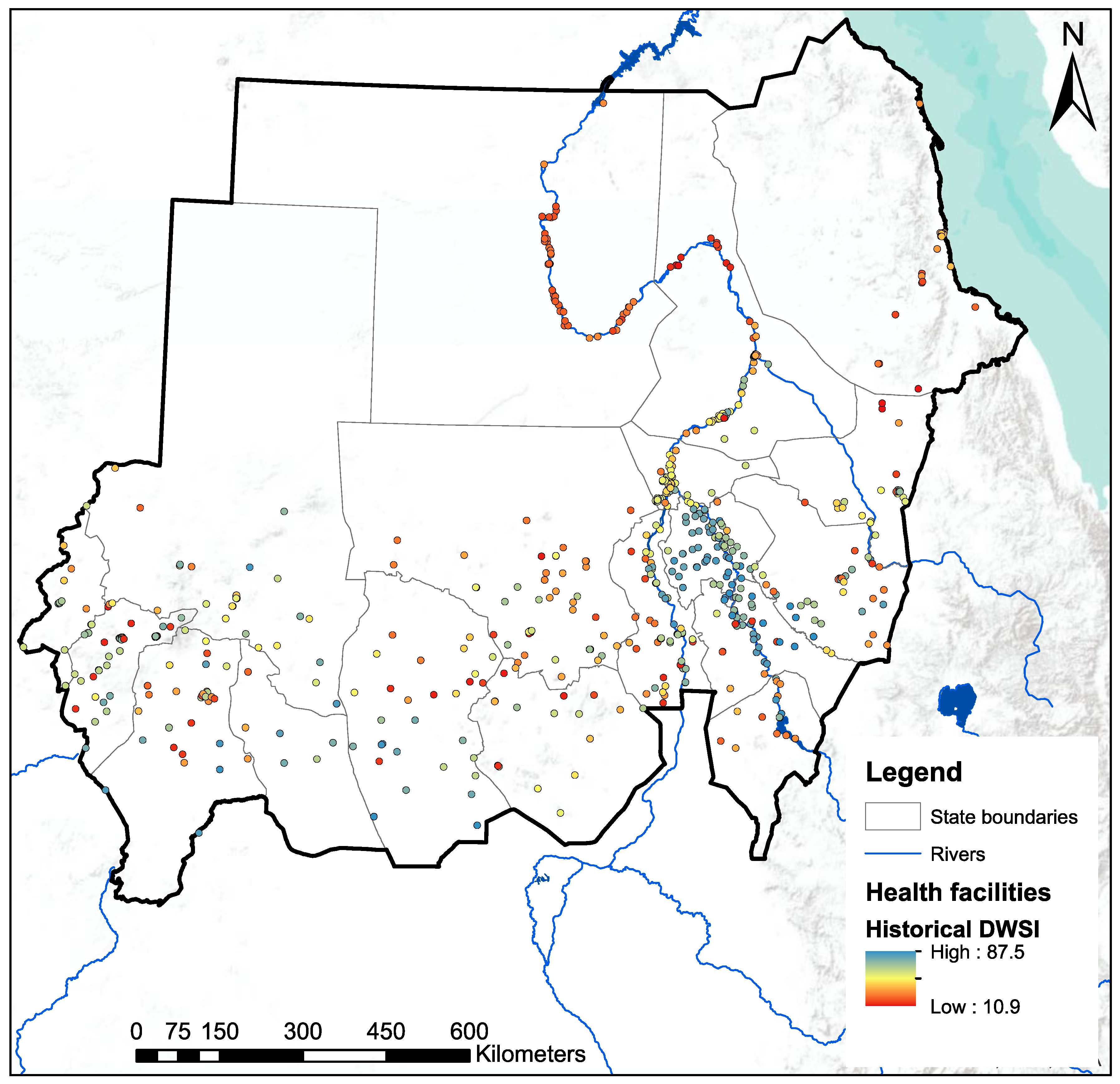
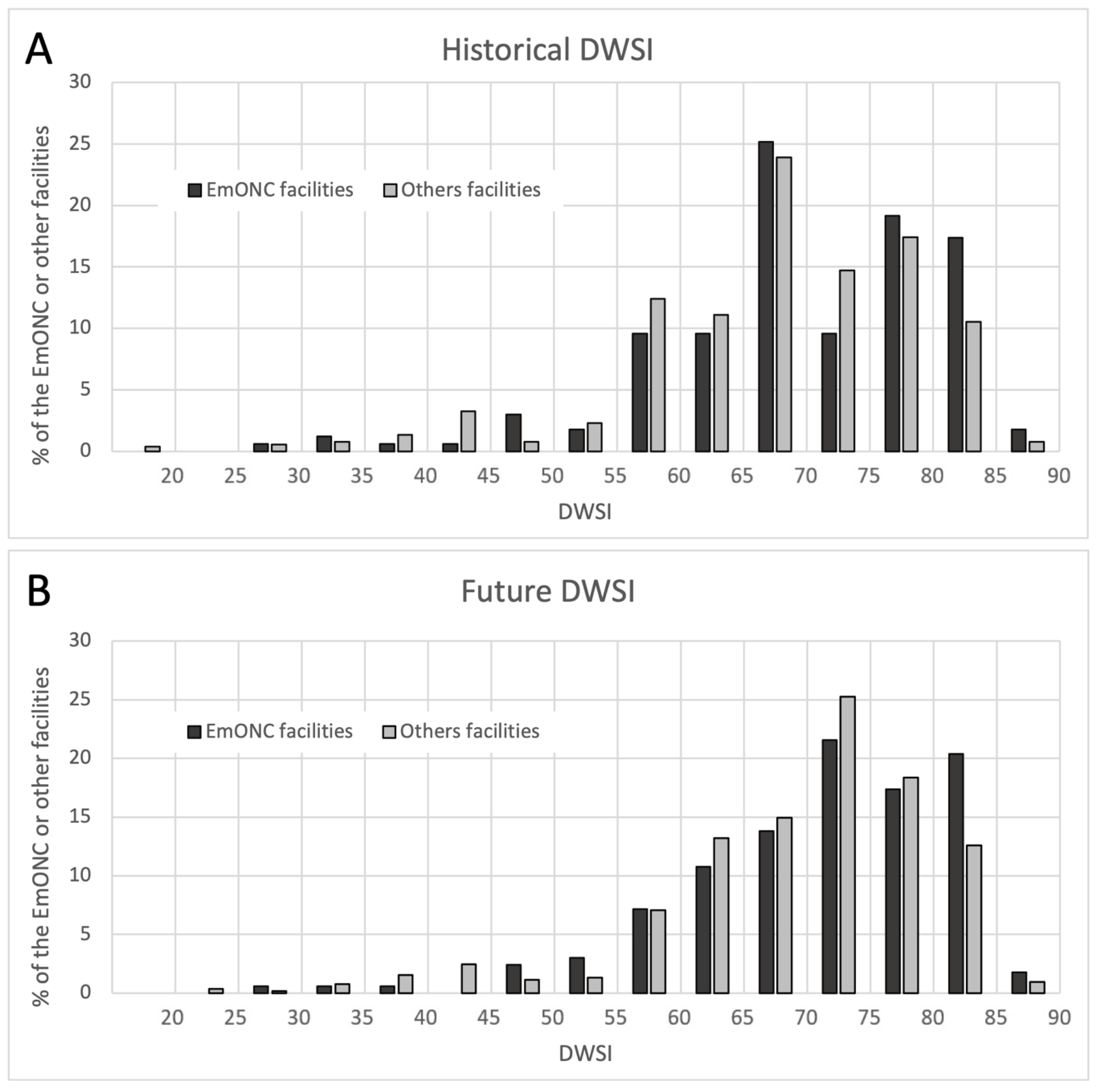
3.3. Assessment of DWSI at Health Facility Level
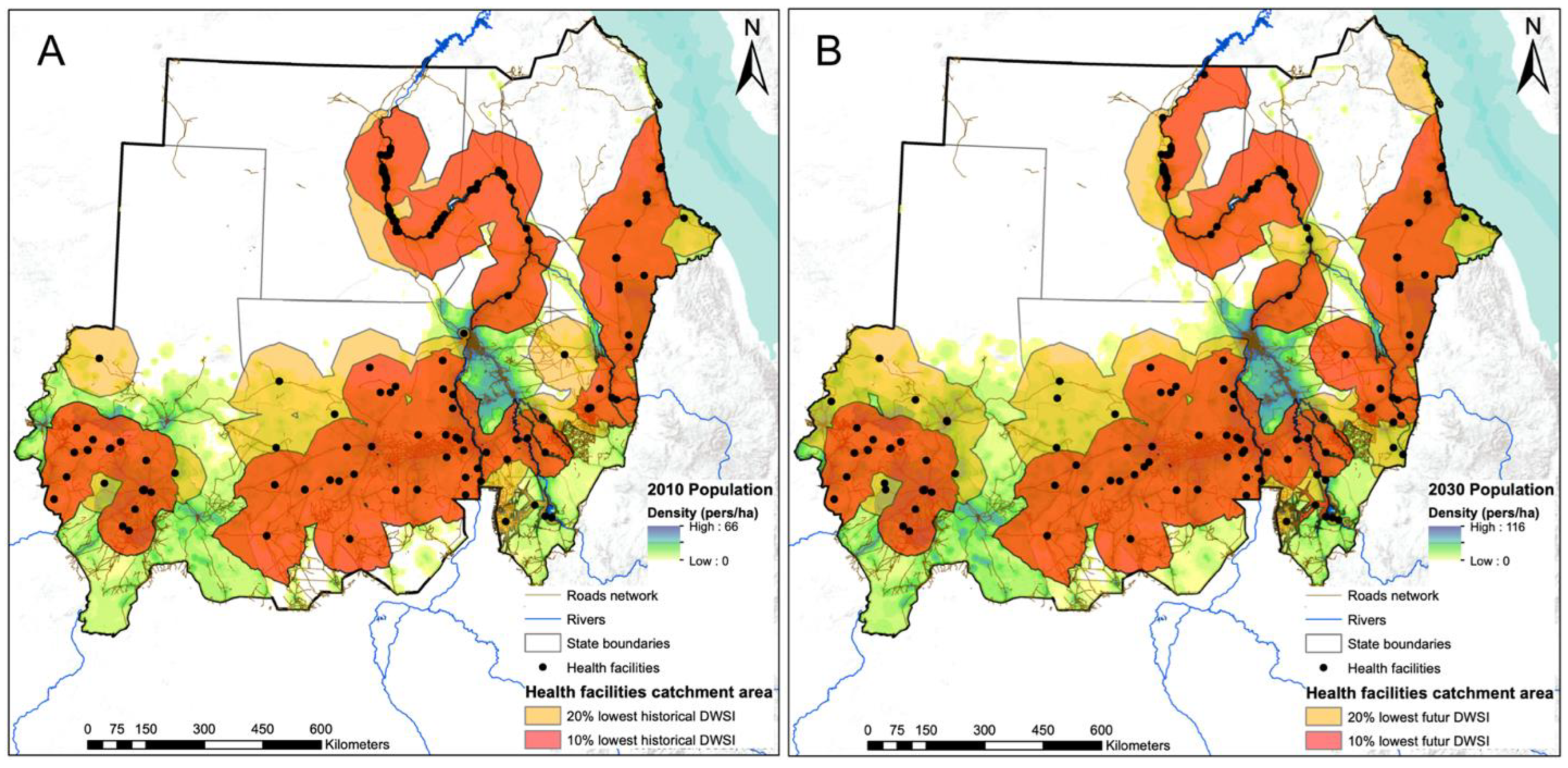
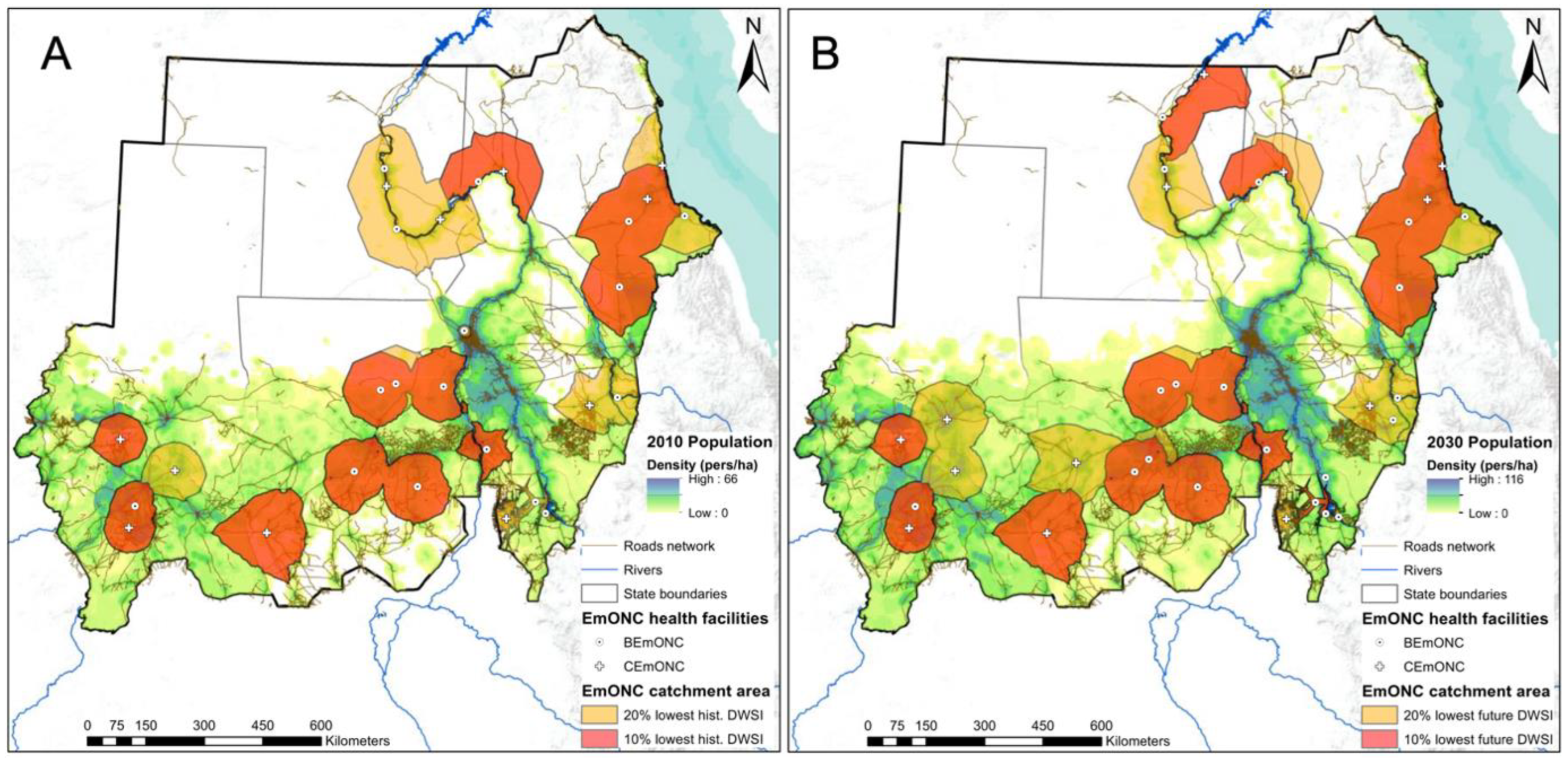
3.4. Population Coverage of Facilities with Low DWSI
4. Discussion
4.1. Drinking Water Security at State and Pixel Levels
4.2. Drinking Water Security at Facility Level
4.3. Limitations
4.3.1. Availability and Temporality of MICS Data
4.3.2. Health Facility Data
4.3.3. DWSI Calculation
4.3.4. Population Coverage
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Esrey, S.A.; Potash, J.B.; Roberts, L.; Shiff, C. Effects of improved water supply and sanitation on ascariasis, diarrhoea, dracunculiasis, hookworm infection, schistosomiasis, and trachoma. Bull. World Health Organ. 1991, 69, 609. [Google Scholar] [PubMed]
- UNICEF. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines; 924151289X; World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 2017. [Google Scholar]
- Prüss, A.; Kay, D.; Fewtrell, L.; Bartram, J. Estimating the burden of disease from water, sanitation, and hygiene at a global level. Environ. Health Perspect. 2002, 110, 537–542. [Google Scholar] [PubMed]
- Victora, C.G.; Smith, P.G.; Vaughan, J.P.; Nobre, L.C.; Lombard, C.; Teixeira, A.M.B.; Fuchs, S.C.; Moreira, L.; Gigante, L.; Barros, F.C. Water supply, sanitation and housing in relation to the risk of infant mortality from diarrhoea. Int. J. Epidemiol. 1988, 17, 651–654. [Google Scholar] [CrossRef] [PubMed]
- Campbell, O.M.; Benova, L.; Gon, G.; Afsana, K.; Cumming, O. Getting the basic rights–the role of water, sanitation and hygiene in maternal and reproductive health: A conceptual framework. Trop. Med. Int. Health 2015, 20, 252–267. [Google Scholar] [CrossRef]
- Benova, L.; Cumming, O.; Campbell, O.M. Systematic review and meta-analysis: Association between water and sanitation environment and maternal mortality. Trop. Med. Int. Health 2014, 19, 368–387. [Google Scholar] [CrossRef]
- Songa, J.; Machine, M.; Rakuom, C. Maternal child health through water, sanitation and hygiene. Sky J. Med. Med. Sci. 2015, 3, 94–104. [Google Scholar]
- Kayser, G.L.; Moriarty, P.; Fonseca, C.; Bartram, J. Domestic water service delivery indicators and frameworks for monitoring, evaluation, policy and planning: A review. Int. J. Environ. Res. Public Health 2013, 10, 4812–4835. [Google Scholar] [CrossRef]
- UN Water. Water Security and the Global Water Agenda: A UN-Water Analytical Brief; United Nations University: Hamilton, ON, Canada, 2013. [Google Scholar]
- Zakieldeen, S.A. Adaptation to Climate Change: A Vulnerability Assessment for Sudan; Gatekeeper Series, International Institute for Environment and Development, Sustainable Agriculture and Rural Livelihoods Programme; Gatekeeper: London, UK, 2009; Volume 142. [Google Scholar]
- World Bank Database. Available online: https://data.worldbank.org/country (accessed on 21 February 2019).
- Falkenmark, M.; Lundqvist, J.; Widstrand, C. Macro-scale water scarcity requires micro-scale approaches: Aspects of vulnerability in semi-arid development. Nat. Resour. Forum 1989, 13, 258–267. [Google Scholar] [CrossRef]
- Falkenmark, M.; Widstrand, C. Population and water resources: A delicate balance. Popul. Bull. 1992, 47, 1–36. [Google Scholar]
- Central Bureau of Statistics, UNICEF. Multiple Indicator Cluster Survey 2014 of Sudan, Final Report; UNICEF and Central Bureau of Statistics: Khartoum, Sudan, 2016. [Google Scholar]
- Sayed, M.A.; Abdala, B. Sudan Environmental and Climate Change Assessment; International Fund for Agricultural Development: Rome, Italy, 2013. [Google Scholar]
- Elagib, N. Changing rainfall, seasonality and erosivity in the hyper-arid zone of Sudan. Land Degrad. Dev. 2011, 22, 505–512. [Google Scholar] [CrossRef]
- WHO. Trends in Maternal Mortality 2000 to 2017: Estimates from WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division; World Health Organization (WHO): Geneva, Switzerland, 2019. [Google Scholar]
- Brun, M.; Monet, J.P.; Agbigbi, Y.; Lysias, J.; Moreira, I.; Schaaf, M.; Ray, N. Implementation Manual for Developing a National Network of Maternity Units: Improving Emergency Obstetric and Newborn Care (EmONC); United Nations Population Fund (UNFPA): New York, NY, USA, 2020. [Google Scholar]
- FMoH, UNFPA, UNICEF. Mapping and Assessment of Maternal, Neonatal and Child Emergencies and Rehabilitation Services; UNICEF-SoP: Jerusalem, Palestine, 2018. [Google Scholar]
- Jepson, W.E.; Wutich, A.; Colllins, S.M.; Boateng, G.O.; Young, S.L. Progress in household water insecurity metrics: A cross-disciplinary approach. Wiley Interdiscip. Rev. Water 2017, 4, e1214. [Google Scholar] [CrossRef]
- Norman, E.S.; Dunn, G.; Bakker, K.; Allen, D.M.; De Albuquerque, R.C. Water security assessment: Integrating governance and freshwater indicators. Water Resour. Manag. 2013, 27, 535–551. [Google Scholar] [CrossRef]
- Lawrence, P.R.; Meigh, J.; Sullivan, C. The Water Poverty Index: An International Comparison; Citeseer: Princeton, NJ, USA, 2002. [Google Scholar]
- Aggarwal, S.; Punhani, G.; Kher, J. Hotspots of household water insecurity in India’s current and future climates: Association with gender inequalities. wH2O J. Gend. Water 2014, 3, 34–41. [Google Scholar]
- Aayog, N. Composite Water Management Index: A Tool for Water Management; National nstitution for Transforming India: New Delhi, India, 2018; p. 239. [Google Scholar]
- Lautze, J.; Manthrithilake, H. Water security: Old concepts, new package, what value? Nat. Resour. Forum 2012, 36, 76–87. [Google Scholar] [CrossRef]
- Assefa, Y.T.; Babel, M.S.; Susnik, J.; Shinde, V.R. Development of a Generic Domestic Water Security Index, and Its Application in Addis Ababa, Ethiopia. Water 2019, 11, 37. [Google Scholar] [CrossRef]
- Jemmali, H. Mesures de la pauvreté en eau: Analyse comparative et développement de l‘indice de pauvreté en eau. VertigO 2013, 13, 1–10. [Google Scholar] [CrossRef]
- Mahgoub, F. Current Status of Agriculture and Future Challenges in Sudan; Nordiska Afrikainstitutet: Uppsala, Sweden, 2014. [Google Scholar]
- Hamad, O.E.-T.; El-Battahani, A. Sudan and the Nile basin. Aquat. Sci. 2005, 67, 28–41. [Google Scholar] [CrossRef]
- Fanack Water Water Resources in Sudan. Available online: https://water.fanack.com/sudan/water-resources-in-sudan/ (accessed on 24 February 2019).
- Omer, A.M. Water resources and freshwater ecosystems in Sudan. Renew. Sustain. Energy Rev. 2008, 12, 2066–2091. [Google Scholar] [CrossRef]
- Elamin, A.W.M. Water Resources in Sudan. In Agriculture Mechanization and Information Technologies; IARTC: Izmir, Turkey, 2013. [Google Scholar]
- Sullivan, C. Calculating a water poverty index. World Dev. 2002, 30, 1195–1210. [Google Scholar] [CrossRef]
- FMoH, Central Bureau of Statistics, UNICEF. Sudan Household Health Survey 2010; National Ministry of Health: Khartoum, Sudan, 2012. [Google Scholar]
- UNFPA. Identifying the National Network of Health Facilities Providing EmONC in the REPUBLIC of SUDAN—Technical Report; UNFPA: Geneva, Switzerland, 2021; p. 223. Available online: https://sudan.unfpa.org/en/node/103301 (accessed on 27 October 2022).
- MacDonald, A.M.; Bonsor, H.C.; Dochartaigh, B.É.Ó.; Taylor, R.G. Quantitative maps of groundwater resources in Africa. Environ. Res. Lett. 2012, 7, 024009. [Google Scholar] [CrossRef]
- OCHA. Sudan-Subnational Administrative Boundaries. Available online: https://data.humdata.org/dataset/cod-ab-sdn (accessed on 27 October 2022).
- Schuol, J.; Abbaspour, K.C. Using monthly weather statistics to generate daily data in a SWAT model application to West Africa. Ecol. Model. 2007, 201, 301–311. [Google Scholar] [CrossRef]
- Abbaspour, K.C.; Vaghefi, S.A.S.; Yang, H.; Srinivasan, R. Global soil, landuse, evapotranspiration, historical and future weather databases for SWAT Applications. Sci. Data 2019, 6, 263. [Google Scholar] [CrossRef] [PubMed]
- Vörösmarty, C.J.; Fekete, B.; Tucker, B.A. River Discharge Database, Version 1.1; Institute for the Study of Earth, Oceans, and Space/University of New Hampshire: Durham, NH, USA, 1998. [Google Scholar]
- Ibrahim, A.; Belal, M.; Ahmed, S.A.K. Impact Of Fiscal Policy Shocks On Official Versus Parallel Exchange Rate Of Sudan: Under Long-Term Economic Sanction And South Sudan Reverondum (1997–2017). ABC Res. Alert 2018, 6, 113–127. [Google Scholar]
- Bailey, P.; Lobis, S.; Maine, D.; Fortney, J.A. Monitoring Emergency Obstetric Care: A Handbook; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Omer, A. Focus on groundwater in Sudan. Environ. Geol. 2002, 41, 972–976. [Google Scholar] [CrossRef]
- Selby, J.; Hoffmann, C. Beyond scarcity: Rethinking water, climate change and conflict in the Sudans. Glob. Environ. Chang. 2014, 29, 360–370. [Google Scholar] [CrossRef]
- Kansara, P.; Li, W.; El-Askary, H.; Lakshmi, V.; Piechota, T.; Struppa, D.; Sayed, M.A. An Assessment of the Filling Process of the Grand Ethiopian Renaissance Dam and Its Impact on the Downstream Countries. Remote Sens. 2021, 13, 711. [Google Scholar] [CrossRef]
- Harris, I.; Jones, P.D.; Osborn, T.J.; Lister, D.H. Updated high-resolution grids of monthly climatic observations–The CRU TS3. 10 Dataset. Int. J. Climatol. 2014, 34, 623–642. [Google Scholar] [CrossRef]
- Ray, N.; Ebener, S. AccessMod 3.0: Computing geographic coverage and accessibility to health care services using anisotropic movement of patients. Int. J. Health Geogr. 2008, 7, 63. [Google Scholar] [CrossRef]
- Lloyd, C.T.; Sorichetta, A.; Tatem, A.J. High resolution global gridded data for use in population studies. Sci. Data 2017, 4, 170001. [Google Scholar] [CrossRef]
- UNICEF MICS Survey Status. Available online: https://mics.unicef.org/surveys (accessed on 27 October 2022).
- Keyes, E.B.; Parker, C.; Zissette, S.; Bailey, P.E.; Augusto, O. Geographic access to emergency obstetric services: A model incorporating patient bypassing using data from Mozambique. BMJ Glob. Health 2019, 4, e000772. [Google Scholar] [CrossRef]
- Ocholla, I.A.; Agutu, N.O.; Ouma, P.O.; Gatungu, D.; Makokha, F.O.; Gitaka, J. Geographical accessibility in assessing bypassing behaviour for inpatient neonatal care, Bungoma County-Kenya. BMC Pregnancy Childbirth 2020, 20, 287. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Guidelines for Drinking-Water Quality: Fourth Edition Incorporating the First Addendum; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Trevett, A.F.; Carter, R.C.; Tyrrel, S.F. Water quality deterioration: A study of household drinking water quality in rural Honduras. Int. J. Environ. Health Res. 2004, 14, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Howard, G.; Bartram, J. Domestic Water Quantity, Service Level and Health; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Central Bureau of Statistics. Statistical Year Book for the Year 2016. Available online: https://www.unhcr.org/5a8ee0387.pdf (accessed on 27 October 2022).
- Frich, P.; Alexander, L.V.; Della-Marta, P.; Gleason, B.; Haylock, M.; Tank, A.K.; Peterson, T. Observed coherent changes in climatic extremes during the second half of the twentieth century. Clim. Res. 2002, 19, 193–212. [Google Scholar] [CrossRef]
- Duan, Y.; Ma, Z.; Yang, Q. Characteristics of consecutive dry days variations in China. Theor. Appl. Climatol. 2017, 130, 701–709. [Google Scholar] [CrossRef]
- Hayes, M.; Svoboda, M.; Wall, N.; Widhalm, M. The Lincoln declaration on drought indices: Universal meteorological drought index recommended. Bull. Am. Meteorol. Soc. 2011, 92, 485–488. [Google Scholar] [CrossRef]
- Pattanayak, S.K.; Yang, J.C.; Whittington, D.; Bal Kumar, K. Coping with unreliable public water supplies: Averting expenditures by households in Kathmandu, Nepal. Water Resour. Res. 2005, 41. [Google Scholar] [CrossRef]
- Kundzewicz, Z.W.; Doell, P. Will groundwater ease freshwater stress under climate change? Hydrol. Sci. J. 2009, 54, 665–675. [Google Scholar] [CrossRef]
- FAO. AQUASTAT Database. Available online: http://www.fao.org/nr/water/aquastat/countries_regions/SDN/indexfra.stm (accessed on 19 February 2021).
- Lanzoni, M.; Darling, W.; Edmunds, W. Groundwater in Sudan: An improved understanding of wadi-directed recharge. Appl. Geochem. 2018, 99, 55–64. [Google Scholar] [CrossRef]
- Thornthwaite, C.W. An approach toward a rational classification of climate. Geogr. Rev. 1948, 38, 55–94. [Google Scholar] [CrossRef]
- Vicente-Serrano, S.M.; Beguería, S.; López-Moreno, J.I. A multiscalar drought index sensitive to global warming: The standardized precipitation evapotranspiration index. J. Clim. 2010, 23, 1696–1718. [Google Scholar] [CrossRef]
- DeGaetano, A.T.; Belcher, B.N.; Noon, W. Temporal and spatial interpolation of the standardized precipitation index for computational efficiency in the dynamic drought index tool. J. Appl. Meteorol. Climatol. 2015, 54, 795–810. [Google Scholar] [CrossRef]
- Camera, C.; Bruggeman, A.; Hadjinicolaou, P.; Pashiardis, S.; Lange, M.A. Evaluation of interpolation techniques for the creation of gridded daily precipitation (1 × 1 km2); Cyprus, 1980–2010. J. Geophys. Res. Atmos. 2014, 119, 693–712. [Google Scholar] [CrossRef]
- Rhee, J.; Carbone, G.J.; Hussey, J. Drought index mapping at different spatial units. J. Hydrometeorol. 2008, 9, 1523–1534. [Google Scholar] [CrossRef]
- Keblouti, M.; Ouerdachi, L.; Boutaghane, H. Spatial interpolation of annual precipitation in Annaba-Algeria-comparison and evaluation of methods. Energy Procedia 2012, 18, 468–475. [Google Scholar] [CrossRef]
- Dobesch, H.; Dumolard, P.; Dyras, I. Spatial Interpolation for Climate Data: The Use of GIS in Climatology and Meteorology; John Wiley & Sons: New York, NY, USA, 2013. [Google Scholar]
- Rhee, J.; Carbone, G.J. Estimating drought conditions for regions with limited precipitation data. J. Appl. Meteorol. Climatol. 2011, 50, 548–559. [Google Scholar] [CrossRef]
- Akhtari, R.; Morid, S.; Mahdian, M.H.; Smakhtin, V. Assessment of areal interpolation methods for spatial analysis of SPI and EDI drought indices. Int. J. Climatol. A J. R. Meteorol. Soc. 2009, 29, 135–145. [Google Scholar] [CrossRef]
- Dyras, I.; Dobesch, H.; Grueter, E.; Perdigao, A.; Tveito, O.E.; Thornes, J.E.; van der Wel, F.; Bottai, L. The use of Geographic Information Systems in climatology and meteorology: COST 719. Meteorol. Appl. 2005, 12, 1–5. [Google Scholar] [CrossRef]
- Shepard, D. A two-dimensional interpolation function for irregularly-spaced data. In Proceedings of the 1968 23rd ACM National Conference, New York, NY, USA, 27–29 August 1968; pp. 517–524. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator | Variable | Measurements | Static (ST) Dynamic (DY) 1 | Positive (+) Negative (−) 2 | |
|---|---|---|---|---|---|
| At State and Pixel Level | At Health Facility (HF) Level | ||||
| Quality (Quali) | Drinking water source | % of population with improved water sources | Type of primary water source (5–1) | state: DY HF: ST | + |
| Water treatment | % of population with unimproved water source but appropriate water treatment | No available measurements | state: DY HF: / | + | |
| Accessibility (Acces) | Water fetching time | % of population at less than 30 min fetching time | Binary value, with (1) or without (0) water source | state: DY HF: ST | + |
| Groundwater depth | Estimated depth to groundwater (m below ground level) | ST | − | ||
| Continuity (Conti) | Droughts | Maximum consecutive dry day (CDD) per year | DY | − | |
| Inter-annual variability | Coefficient of variation (CV) in annual precipitation (%) | DY | − | ||
| Seasonal variability | Coefficient of variation (CV) in monthly precipitation (%) | DY | − | ||
| Availability (Avail) | Water balance ratio | Precipitation / Potential Evapotranspiration (-) | DY | + | |
| Groundwater storage | Water depth (m) | ST | + | ||
| Groundwater productivity | Borehole yields expected (L/s) | ST | + | ||
| DATA TYPE | Source | Data Format | Representative Year | Publication Year |
|---|---|---|---|---|
| Water supply statistics at state level | Multiple Indicator Cluster Survey (MICS) [14,34] | Report and tables | 2010/2014 | 2012/2016 |
| Health facilities location and their primary water source | Sudan EmONC Need Assessment [19] | Vector and table | 2017 | 2018 |
| EmONC facility network | Identifying the national network of health facilities providing EmONC in the Republic of Sudan—Technical report [35] | Report and table | 2019 | 2021 |
| Groundwater resources (depth, storage, productivity) | Quantitative maps of groundwater resources in Africa [36] | Raster (5 × 5 km) | 2011 | 2012 |
| Administrative boundaries | OCHA Regional Office for Southern and Eastern Africa (HDX) [37] | Vector | 2018 | 2018 |
| Global Historical Climate Data | Climatic Research Unit (CRU) and dGen [38] | Tables (0.5° grid points) | 1970–2006 | 2007 |
| Global IPCC Climate Database | 5 GCMs (GFDL, HadGEM, IPSL, MIROC, NoerESM) and 1 RCP (8.5) [39] | Tables (0.5° grid points) | 2006–2099 | 2019 |
| Observed water discharge | Global Runoff Data Centre (GRDC) and the Global River Discharge Database (RivDIS) [40] | Table | 1900–1984 | 2022 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simonin, V.; Vaghefi, S.A.; Abdelgadir, Z.M.; Eltayeb, D.; Sidahmed, M.A.M.; Monet, J.-P.; Ray, N. Present and Future Drinking Water Security and Its Impacts on Maternities: A Multi-Scale Assessment of Sudan. Int. J. Environ. Res. Public Health 2023, 20, 2204. https://doi.org/10.3390/ijerph20032204
Simonin V, Vaghefi SA, Abdelgadir ZM, Eltayeb D, Sidahmed MAM, Monet J-P, Ray N. Present and Future Drinking Water Security and Its Impacts on Maternities: A Multi-Scale Assessment of Sudan. International Journal of Environmental Research and Public Health. 2023; 20(3):2204. https://doi.org/10.3390/ijerph20032204
Chicago/Turabian StyleSimonin, Vincent, Saeid Ashraf Vaghefi, Zeinab M. Abdelgadir, Dalya Eltayeb, Mohammed Ahmed M. Sidahmed, Jean-Pierre Monet, and Nicolas Ray. 2023. "Present and Future Drinking Water Security and Its Impacts on Maternities: A Multi-Scale Assessment of Sudan" International Journal of Environmental Research and Public Health 20, no. 3: 2204. https://doi.org/10.3390/ijerph20032204
APA StyleSimonin, V., Vaghefi, S. A., Abdelgadir, Z. M., Eltayeb, D., Sidahmed, M. A. M., Monet, J.-P., & Ray, N. (2023). Present and Future Drinking Water Security and Its Impacts on Maternities: A Multi-Scale Assessment of Sudan. International Journal of Environmental Research and Public Health, 20(3), 2204. https://doi.org/10.3390/ijerph20032204