


Effects of Different Hamstring Eccentric Exercise Programs on Preventing Lower Extremity Injuries: A Systematic Review and Meta-Analysis

Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
2.5. Data Collection Process
2.6. Data Items
2.7. Study Risk of Bias Assessment
2.8. Effect Measures
2.9. Synthesis Methods
2.10. Publication Bias
2.11. Assessment of Certainty of Evidence
3. Results
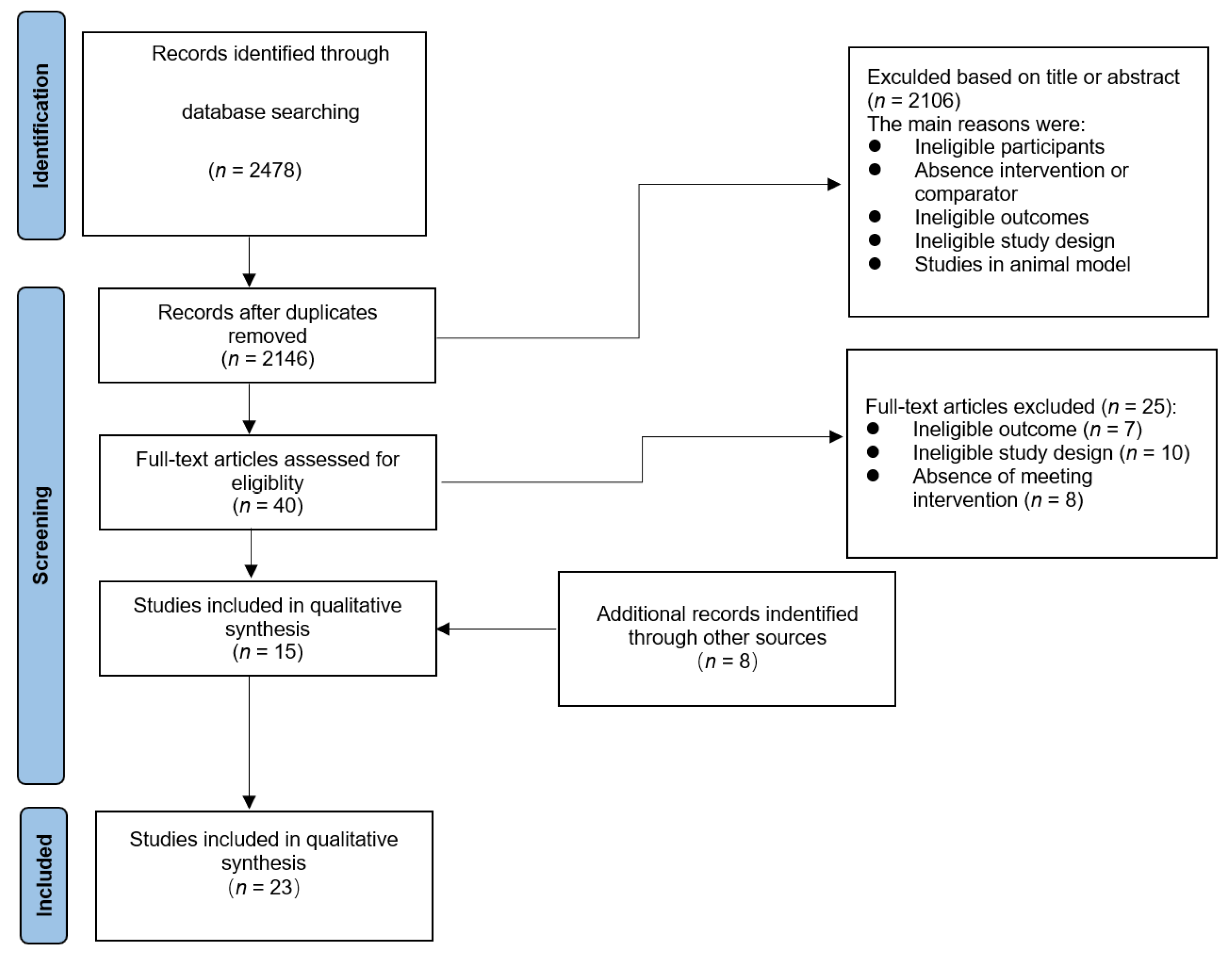
3.1. Study Selection
3.2. Study Characteristics
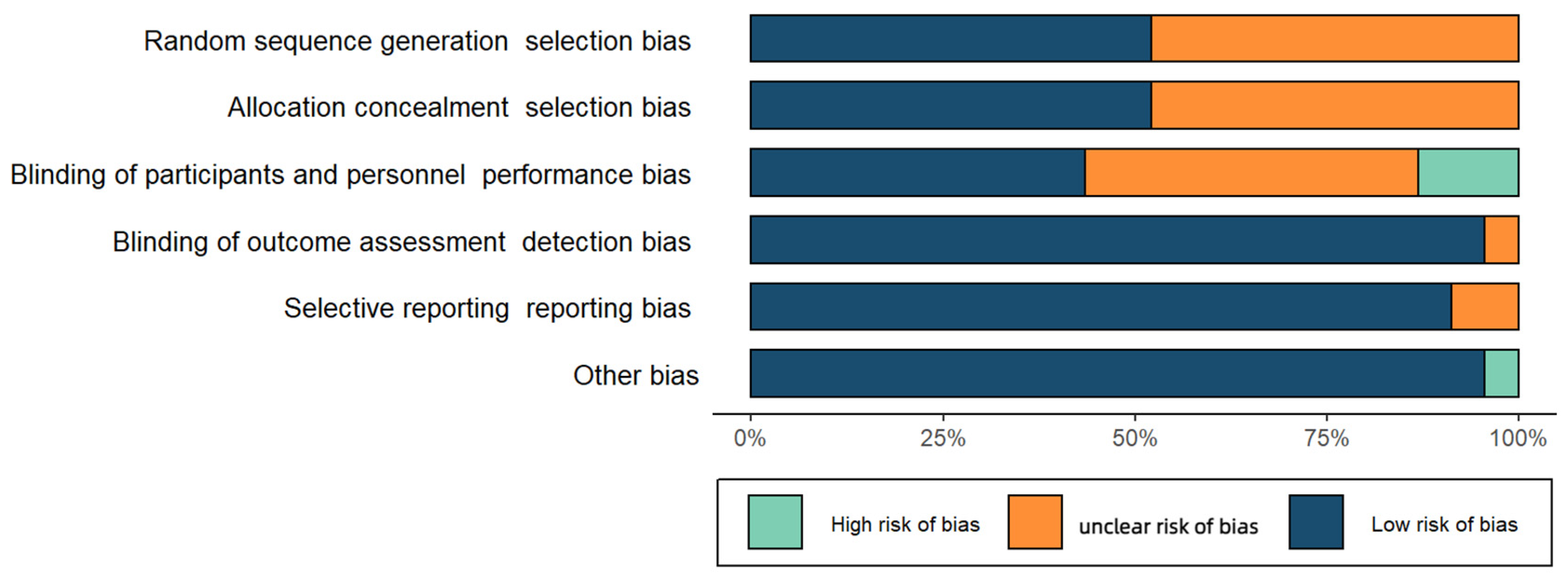
3.3. Risk of Bias in Studies
3.4. Publication Bias Results
3.5. Effect of Hamstring Eccentric Exercise on Preventing Lower Extremity Injuries
3.5.1. Overall Effect Test
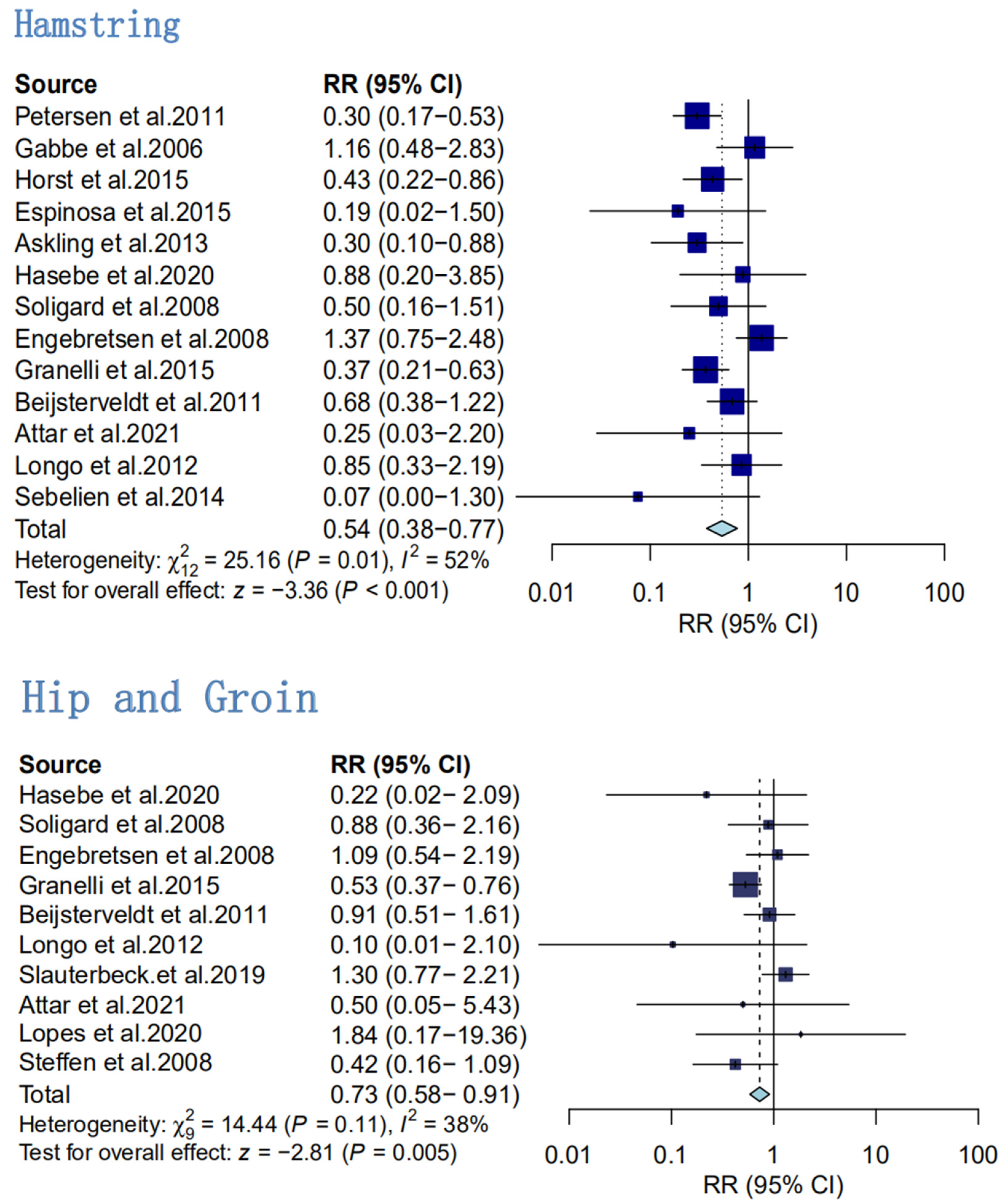
3.5.2. Injury in Different Body Regions
- Secondary analyses of the effect of hamstring sports injury prevention
- 2.
- Secondary analyses of the effect of hip and groin sports injury prevention
- 3.
- Secondary analyses of the effect of knee sports injury prevention
- 4.
- Secondary analyses of the preventive effect of ankle sports injuries
3.5.3. Results of Subgroup Analysis (Table 1)

| Subgroup | Heterogeneity Test I²(﹪) P-Value | Group | RR (95%CI) | The Number of Study | Sample Size | |
|---|---|---|---|---|---|---|
| Exercise methods | 37% | 0.19 | Additional hamstring eccentric training | 0.71 (0.59–0.87) | 4 | 4376 |
| 88% | <0.001 | FIFA 11+ | 0.66 (0.48–0.90) | 8 | 6835 | |
| 0% | 0.82 | FIFA11 | 0.94 (0.85–1.05) | 2 | 2548 | |
| - | - | FIFA11+Kids | 0.52 (0.33–0.83) | 1 | 962 | |
| Exercise frequency per week | 0% | 0.38 | Once per week | 1.00 (0.84–1.18) | 2 | 2357 |
| 0% | 0.52 | Twice per week | 0.60 (0.49–0.72) | 5 | 3329 | |
| 89% | <0.01 | More than twice a week | 0.69 (0.53–0.90) | 6 | 5303 | |
| Exercise period | 67% | 0.03 | 10–20weeks | 0.68 (0.54–0.87) | 4 | 2243 |
| 86% | <0.01 | 21–30weeks | 0.62 (0.38–1.01) | 4 | 3334 | |
| 79% | <0.01 | More than 31weeks | 0.77 (0.60–1.00) | 7 | 9144 | |
| Competition level | 84% | <0.01 | Youth | 0.75 (0.56–0.99) | 7 | 9688 |
| 80% | <0.02 | Elite | 0.73 (0.57–0.93) | 6 | 4762 | |
| 0% | 0.41 | Amateur | 0.54 (0.38–0.75) | 2 | 271 | |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Okobi, O.E.; Evbayekha, E.O.; Ilechie, E.; Iroro, J.; Nwafor, J.N.; Gandu, Z.; Shittu, H.O. A meta-analysis of randomized controlled trials on the effectiveness of exercise intervention in preventing sports injuries. Cureus 2022, 14, e26123. [Google Scholar] [CrossRef] [PubMed]
- van Mechelen, W. The severity of sports injuries. Sports Med. 1997, 24, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Emery, C.A.; Pasanen, K. Current trends in sport injury prevention. Best Pract. Res. Clin. Rheumatol. 2019, 33, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Hasebe, Y.; Akasaka, K.; Otsudo, T.; Tachibana, Y.; Hall, T.; Yamamoto, M. Effects of Nordic hamstring exercise on hamstring injuries in high school soccer players: A randomized controlled trial. Int. J. Sports Med. 2020, 41, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, A.H.; Myklebust, G.; Holme, I.; Engebretsen, L.; Bahr, R. Prevention of injuries among male soccer players: A prospective, randomized intervention study targeting players with previous injuries or reduced function. Am. J. Sports Med. 2008, 36, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, L.; Willick, S.; Teramoto, M.; Cushman, D.M. Adaptive sports injury epidemiology. Sports Med. Arthrosc. Rev. 2019, 27, e8–e11. [Google Scholar] [CrossRef]
- Hespanhol, L.C., Jr.; Barboza, S.D.; van Mechelen, W.; Verhagen, E. Measuring sports injuries on the pitch: A guide to use in practice. Braz. J. Phys. Ther. 2015, 19, 369–380. [Google Scholar] [CrossRef]
- Stracciolini, A.; Sugimoto, D.; Howell, D.R. Injury prevention in youth sports. Pediatr. Ann. 2017, 46, e99–e105. [Google Scholar] [CrossRef]
- Conn, J.M.; Annest, J.L.; Gilchrist, J. Sports and recreation related injury episodes in the us population, 1997–1999. Inj. Prev. 2003, 9, 117–123. [Google Scholar] [CrossRef]
- Hickey, J.T.; Opar, D.A.; Weiss, L.J.; Heiderscheit, B.C. Hamstring strain injury rehabilitation. J. Athl. Train. 2022, 57, 125–135. [Google Scholar] [CrossRef]
- van Mechelen, W. Sports injury surveillance systems. ‘One size fits all’? Sports Med. 1997, 24, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Sadigursky, D.; Braid, J.A.; Lemos De Lira, D.N.; Barreto Machado, B.A.; Fernandes Carneiro, R.J.; Colavolpe, P.O. The FIFA 11+ injury prevention program for soccer players: A systematic review. BMC Sports Sci. Med. Rehabil. 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Rössler, R.; Donath, L.; Verhagen, E.; Junge, A.; Schweizer, T.; Faude, O. Exercise-based injury prevention in child and adolescent sport: A systematic review and meta-analysis. Sports Med. 2014, 44, 1733–1748. [Google Scholar] [CrossRef] [PubMed]
- Grimm, N.L.; Jacobs, J.C., Jr.; Kim, J.; Amendola, A.; Shea, K.G. Ankle injury prevention programs for soccer athletes are protective a level-i meta-analysis. J. Bone Joint Surg. Am. 2016, 98, 1436–1443. [Google Scholar] [CrossRef] [PubMed]
- Barboza, S.D.; Joseph, C.; Nauta, J.; van Mechelen, W.; Verhagen, E. Injuries in field hockey players: A systematic review. Sports Med. 2018, 48, 849–866. [Google Scholar] [CrossRef] [PubMed]
- Bizzini, M.; Dvorak, J. FIFA 11+: An effective programme to prevent football injuries in various player groups worldwide-a narrative review. Br. J. Sports Med. 2015, 49, 577–579. [Google Scholar] [CrossRef]
- Elerian, A.E.; El-Sayyad, M.M.; Dorgham, H.A.A. Effect of pre-training and post-training Nordic exercise on hamstring injury prevention, recurrence, and severity in soccer players. Ann. Rehabil. Med. 2019, 43, 465–473. [Google Scholar] [CrossRef]
- Owoeye, O.B.A.; Akinbo, S.R.A.; Tella, B.A.; Olawale, O.A. Efficacy of the FIFA 11+warm-up programme in male youth football: A cluster randomised controlled trial. J. Sports Sci. Med. 2014, 13, 321–328. [Google Scholar]
- Nuhu, A.; Jelsma, J.; Dunleavy, K.; Burgess, T. Effect of the FIFA 11+ soccer specific warm up programme on the incidence of injuries: A cluster-randomised controlled trial. PLoS ONE 2021, 16, e0251839. [Google Scholar] [CrossRef]
- Achenbach, L.; Krutsch, V.; Weber, J.; Nerlich, M.; Luig, P.; Loose, O.; Angele, P.; Krutsch, W. Neuromuscular exercises prevent severe knee injury in adolescent team handball players. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1901–1908. [Google Scholar] [CrossRef]
- Emery, C.A.; Owoeye, O.B.A.; Raisanen, A.M.; Befus, K.; Hubkarao, T.; Palacios-Derflingher, L.; Pasanen, K. The “shred injuries basketball” neuromuscular training warm-up program reduces ankle and knee injury rates by 36% in youth basketball. J. Orthop. Sports Phys. Ther. 2022, 52, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Zarei, M.; Abbasi, H.; Namazi, P.; Asgari, M.; Rommers, N.; Rössler, R. The 11+ kids warm-up programme to prevent injuries in young iranian male high-level football (soccer) players: A cluster-randomised controlled trial. J. Sci. Med. Sport 2020, 23, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Bourne, M.N.; Williams, M.D.; Opar, D.A.; Al Najjar, A.; Kerr, G.K.; Shield, A.J. Impact of exercise selection on hamstring muscle activation. Br. J. Sports Med. 2017, 51, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.S.; Kayani, B.; Plastow, R.; Singh, S.; Magan, A.; Haddad, F.S. Management of hamstring injuries: Current concepts review. Bone Joint J. 2020, 102-b, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Hamstring strain injury in athletes: A summary of clinical practice guideline recommendations: Using the evidence to guide physical therapist practice. J. Orthop. Sport. Phys. Ther. 2022, 52, 127–128. [CrossRef]
- Freckleton, G.; Pizzari, T. Risk factors for hamstring muscle strain injury in sport: A systematic review and meta-analysis. Br. J. Sports Med. 2013, 47, 351–358. [Google Scholar] [CrossRef]
- Silvers-Granelli, H.; Mandelbaum, B.; Adeniji, O.; Insler, S.; Bizzini, M.; Pohlig, R.; Junge, A.; Snyder-Mackler, L.; Dvorak, J. Efficacy of the FIFA 11+ injury prevention program in the collegiate male soccer player. Am. J. Sports Med. 2015, 43, 2628–2637. [Google Scholar] [CrossRef]
- Al Attar, W.S.A.; Soomro, N.; Pappas, E.; Sinclair, P.J.; Sanders, R.H. How effective are F-MARC injury prevention programs for soccer players? A systematic review and meta-analysis. Sports Med. 2016, 46, 205–217. [Google Scholar] [CrossRef]
- Almeida, M.O.; Maher, C.G.; Saragiotto, B.T. Prevention programmes including Nordic exercises to prevent hamstring injuries in football players (pedro synthesis). Br. J. Sports Med. 2018, 52, 877–878. [Google Scholar] [CrossRef]
- Hilska, M.; Leppaenen, M.; Vasankari, T.; Aaltonen, S.; Kannus, P.; Parkkari, J.; Steffen, K.; Kujala, U.M.; Konttinen, N.; Raeisaenen, A.M.; et al. Neuromuscular training warm-up prevents acute noncontact lower extremity injuries in children’s soccer: A cluster randomized controlled trial. Orthop. J. Sports Med. 2021, 9, 23259671211005769. [Google Scholar] [CrossRef]
- Hilska, M.; Leppänen, M.; Vasankari, T.; Aaltonen, S.; Raitanen, J.; Räisänen, A.M.; Steffen, K.; Forsman, H.; Konttinen, N.; Kujala, U.M.; et al. Adherence to an injury prevention warm-up program in children’s soccer—a secondary analysis of a randomized controlled trial. Int. J. Environ. Res. Public Health 2021, 18, 13134. [Google Scholar] [CrossRef] [PubMed]
- van Dyk, N.; Behan, F.P.; Whiteley, R. Including the nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: A systematic review and meta-analysis of 8459 athletes. Br. J. Sports Med. 2019, 53, 1362–1370. [Google Scholar] [CrossRef] [PubMed]
- Gomes Neto, M.; Conceicao, C.S.; de Lima Brasileiro, A.J.A.; de Sousa, C.S.; Carvalho, V.O.; de Jesus, F.L.A. Effects of the FIFA 11 training program on injury prevention and performance in football players: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Thorborg, K.; Krommes, K.K.; Esteve, E.; Clausen, M.B.; Bartels, E.M.; Rathleff, M.S. Effect of specific exercise-based football injury prevention programmes on the overall injury rate in football: A systematic review and meta-analysis of the FIFA 11 and 11+programmes. Br. J. Sports Med. 2017, 51, 562–571. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Nicoletti, P.; Baldin, G.; Bragazzi, N.L.; Crimì, A.; Ruggieri, P. Hamstring strain injury (hsi) prevention in professional and semi-professional football teams: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 8272. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The prisma 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef]
- Soligard, T.; Myklebust, G.; Steffen, K.; Holme, I.; Silvers, H.; Bizzini, M.; Junge, A.; Dvorak, J.; Bahr, R.; Andersen, T.E. Comprehensive warm-up programme to prevent injuries in young female footballers: Cluster randomised controlled trial. BMJ 2008, 337, a2469. [Google Scholar] [CrossRef]
- Slauterbeck, J.R.; Choquette, R.; Tourville, T.W.; Krug, M.; Mandelbaum, B.R.; Vacek, P.; Beynnon, B.D. Implementation of the FIFA 11+ injury prevention program by high school athletic teams did not reduce lower extremity injuries: A cluster randomized controlled trial. Am. J. Sports Med. 2019, 47, 2844–2852. [Google Scholar] [CrossRef]
- Al Attar, W.S.A.; Bizzini, M.; Alkabkabi, F.; Alshamrani, N.; Alarifi, S.; Alzahrani, H.; Ghulam, H.; Aljedaani, E.; Sanders, R.H. Effectiveness of the FIFA 11+ referees injury prevention program in reducing injury rates in male amateur soccer referees. Scand. J. Med. Sci. Sports 2021, 31, 1774–1781. [Google Scholar] [CrossRef] [PubMed]
- Steffen, K.; Myklebust, G.; Olsen, O.E.; Holme, I.; Bahr, R. Preventing injuries in female youth football--a cluster-randomized controlled trial. Scand. J. Med. Sci. Sports 2008, 18, 605–614. [Google Scholar] [CrossRef]
- Hammes, D.; Fuenten, K.A.D.; Kaiser, S.; Frisen, E.; Bizzini, M.; Meyer, T. Injury prevention in male veteran football players - a randomised controlled trial using “FIFA 11+”. J Sports Sci. 2015, 33, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Lopes, M.; Simões, D.; Costa, R.; Oliveira, J.; Ribeiro, F. Effects of the FIFA 11+ on injury prevention in amateur futsal players. Scand. J. Med. Sci. Sports 2020, 30, 1434–1441. [Google Scholar] [CrossRef] [PubMed]
- Olsen, O.E.; Myklebust, G.; Engebretsen, L.; Holme, I.; Bahr, R. Exercises to prevent lower limb injuries in youth sports: Cluster randomised controlled trial. BMJ 2005, 330, 449–452. [Google Scholar] [CrossRef]
- Van Beijsterveldt, A.M.C.; Krist, M.R.; Van De Port, I.G.L.; Backx, F.J.G. Effectiveness of an injury prevention program in dutch male amateur soccer. Physiotherapy 2011, 97, eS1277. [Google Scholar] [CrossRef]
- Longo, U.G.; Loppini, M.; Berton, A.; Marinozzi, A.; Maffulli, N.; Denaro, V. The FIFA 11+ program for the prevention of injuries in basketball: A cluster randomized controlled trial. J. Orthop. Traumatol. 2012, 13, S6–S7. [Google Scholar] [CrossRef]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Budtz-Jorgensen, E.; Holmich, P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: A cluster-randomized controlled trial. Am. J. Sports Med. 2011, 39, 2296–2303. [Google Scholar] [CrossRef]
- Gabbe, B.J.; Branson, R.; Bennell, K.L. A pilot randomised controlled trial of eccentric exercise to prevent hamstring injuries in community-level australian football. J. Sci. Med. Sport 2006, 9, 103–109. [Google Scholar] [CrossRef]
- van der Horst, N.; Smits, D.-W.; Petersen, J.; Goedhart, E.A.; Backx, F.J.G. The preventive effect of the Nordic hamstring exercise on hamstring injuries in amateur soccer players: A randomized controlled trial. Am. J. Sports Med. 2015, 43, 1316–1323. [Google Scholar] [CrossRef]
- del Ama Espinosa, G.; Pöyhönen, T.; Aramendi, J.F.; Samaniego, J.C.; Emparanza Knörr, J.I.; Kyröläinen, H. Effects of an eccentric training programme on hamstring strain injuries in women football players. Biomed. Hum. Kinet. 2015, 7. [Google Scholar] [CrossRef]
- Askling, C.M.; Tengvar, M.; Thorstensson, A. Acute hamstring injuries in swedish elite football: A prospective randomised controlled clinical trial comparing two rehabilitation protocols. Br. J. Sports Med. 2013, 47. [Google Scholar] [CrossRef] [PubMed]
- Sebelien, C. Effects of implementing Nordic hamstring exercises for semi-professional soccer players in norway. Phys. Ther. 2014, 26, 90–97. [Google Scholar]
- Saleh A Al Attar, W.; Faude, O.; Husain, M.A.; Soomro, N.; Sanders, R.H. Combining the copenhagen adduction exercise and Nordic hamstring exercise improves dynamic balance among male athletes: A randomized controlled trial. Sports Health 2021, 13, 580–587. [Google Scholar] [CrossRef]
- Grooms, D.R.; Palmer, T.; Onate, J.A.; Myer, G.D.; Grindstaff, T. Soccer-specific warm-up and lower extremity injury rates in collegiate male soccer players. J. Athl. Train. 2013, 48, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Silvers-Granelli, H.J.; Bizzini, M.; Arundale, A.; Mandelbaum, B.R.; Snyder-Mackler, L. Does the FIFA 11+injury prevention program reduce the incidence of acl injury in male soccer players? Clin. Orthop. Relat. Res. 2017, 475, 2447–2455. [Google Scholar] [CrossRef] [PubMed]
- Gilchrist, J.; Mandelbaum, B.R.; Melancon, H.; Ryan, G.W.; Silvers, H.J.; Griffin, L.Y.; Watanabe, D.S.; Dick, R.W.; Dvorak, J. A randomized controlled trial to prevent noncontact anterior cruciate ligament injury in female collegiate soccer players. Am. J. Sports Med. 2008, 36, 1476–1483. [Google Scholar] [CrossRef]
- Steffen, K.; Emery, C.A.; Romiti, M.; Kang, J.; Bizzini, M.; Dvorak, J.; Finch, C.F.; Meeuwisse, W.H. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in canadian youth female football players: A cluster randomised trial. Br. J. Sports Med. 2013, 47, 794–802. [Google Scholar] [CrossRef]
- Crossley, K.M.; Patterson, B.E.; Culvenor, A.G.; Bruder, A.M.; Mosler, A.B.; Mentiplay, B.F. Making football safer for women: A systematic review and meta-analysis of injury prevention programmes in 11 773 female football (soccer) players. Br. J. Sports Med. 2020, 54, 1089–1098. [Google Scholar] [CrossRef]
- Whalan, M.; Lovell, R.; Steele, J.R.; Sampson, J.A. Rescheduling part 2 of the 11+ reduces injury burden and increases compliance in semi-professional football. Scand. J. Med. Sci Sports. 2019, 29, 1941–1951. [Google Scholar] [CrossRef]
- Sayers, C.A.; Sayers, B.E.J.S.; Journal, C. The Nordic eccentric hamstring exercise for injury prevention in soccer players. Strength. Cond. J. 2008, 30, 56–58. [Google Scholar] [CrossRef]
- Milanese, S.; Eston, R. Hamstring injuries and australian rules football: Over-reliance on Nordic hamstring exercises as a preventive measure? Open Access J. Sports Med. 2019, 10, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Cuchna, J.W.; Welsch, L.A.; Meier, T.; Regelski, C.L.; Lunen, B. The effectiveness of Nordic hamstring exercises in reducing hamstring injuries in competitive soccer players: A critically appraised topic. Int. J. Athl. Ther. Train. 2017, 22, 12–17. [Google Scholar] [CrossRef]
- Brughelli, M.; Mendiguchia, J.; Nosaka, K.; Idoate, F.; Arcos, A.L.; Cronin, J. Effects of eccentric exercise on optimum length of the knee flexors and extensors during the preseason in professional soccer players. Phys. Ther. Sport 2010, 11, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Cuthbert, M.; Ripley, N.; McMahon, J.J.; Evans, M.; Haff, G.G.; Comfort, P. The effect of Nordic hamstring exercise intervention volume on eccentric strength and muscle architecture adaptations: A systematic review and meta-analyses. Sports Med. 2020, 50, 83–99. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, C.; Du, Z.; Tao, M.; Song, Y. Effects of Different Hamstring Eccentric Exercise Programs on Preventing Lower Extremity Injuries: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 2057. https://doi.org/10.3390/ijerph20032057
Hu C, Du Z, Tao M, Song Y. Effects of Different Hamstring Eccentric Exercise Programs on Preventing Lower Extremity Injuries: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(3):2057. https://doi.org/10.3390/ijerph20032057
Chicago/Turabian StyleHu, Chenxi, Zhikun Du, Mei Tao, and Yafeng Song. 2023. "Effects of Different Hamstring Eccentric Exercise Programs on Preventing Lower Extremity Injuries: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 3: 2057. https://doi.org/10.3390/ijerph20032057
APA StyleHu, C., Du, Z., Tao, M., & Song, Y. (2023). Effects of Different Hamstring Eccentric Exercise Programs on Preventing Lower Extremity Injuries: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 20(3), 2057. https://doi.org/10.3390/ijerph20032057