


Long-Term Care and the State-Family Nexus in Italy and Japan—The Welfare State, Care Policy and Family Caregivers

Abstract
1. Introduction
- What are the characteristics of the welfare state configuration and LTC policy development?
- In what form of benefit does the state provide LTC to older adults and what is the level of access to public LTC for them?
- Who is the main caregiver in the family?
- Given the first and second points, what are the characteristics of the work–family reconciliation of family caregivers?
2. Conceptual Framework—Revisiting the Role of the State and Family in the LTC Provision
3. Welfare State Configurations—The Narrowest Welfare States?
- High levels of spending on compensatory social policies and little on investment-related social policies [32];
- The Japanese national LTC system has been covered by mandatory national insurance since 2000, providing standardized in-kind services for persons in need of care [39]. In Italy, this system does not exist, and remarkable gaps among local governments were identified in the care provisions provided [40];
- In Japan, the national LTC system provides only in-kind services, not cash payments [39]. In contrast, in Italy, cash benefits are much more prevalent than in-kind benefits, and a unique national system for LTC is a cash allowance system called “Indennità di Accompagnamento (Accompanying Allowance)” which has no restrictions on its use [14,15,38];
- The Italian cash-oriented care system encourages the employment of less skilled and cheaper care workers, who are mostly migrants, in the (often grey) market [41]. In contrast, the Japanese in-kind-based public care system, which assigns only 10% of fixed care costs to service recipients, curbs the care services available for purchase on the market [39].
4. LTC Spending, Workers and Recipients
5. Who Are the Primary Family Caregivers?
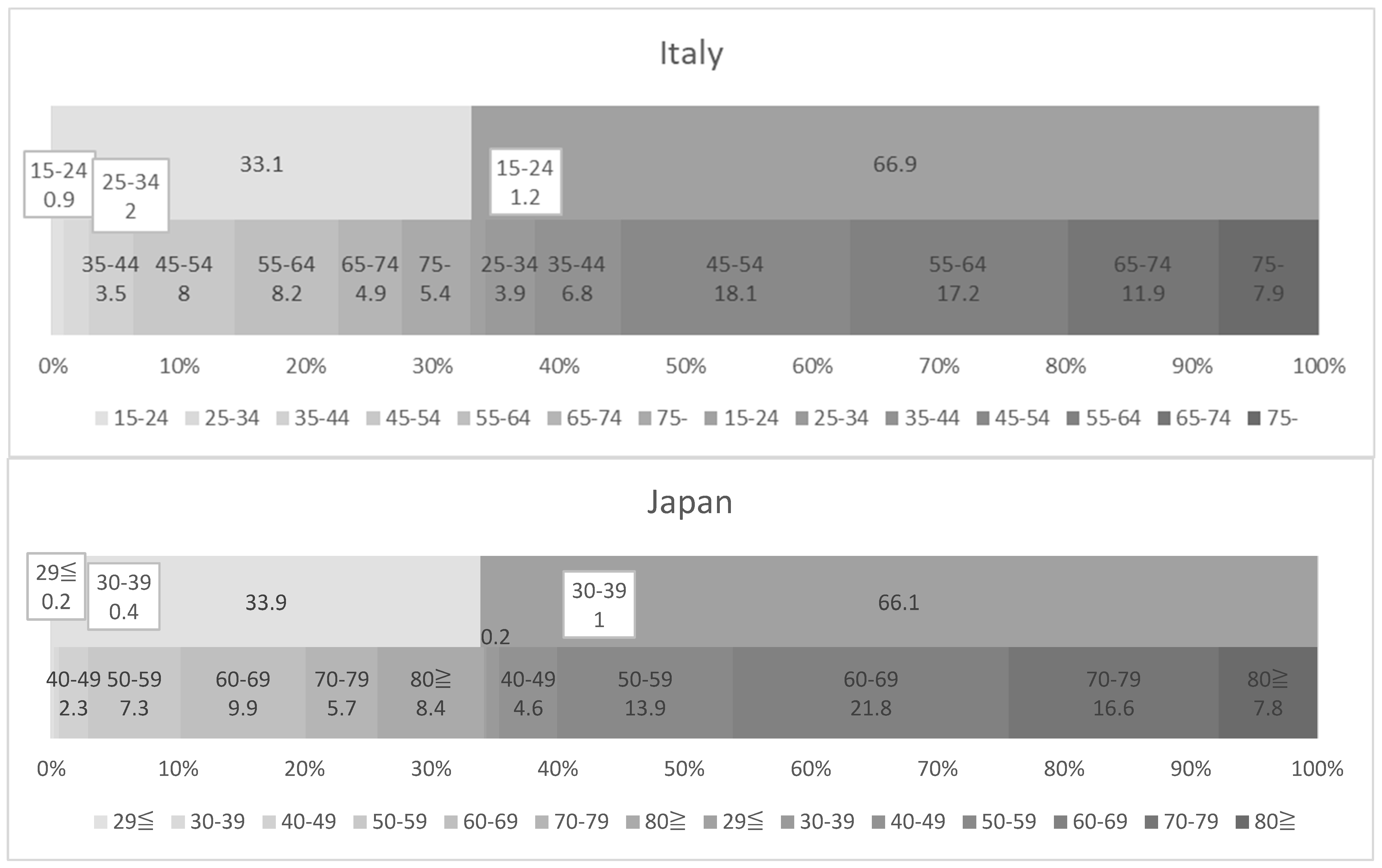
- In both countries, the gender ratios of the primary family caregivers were equivalent, with 33% males and 66% females;
- Italy has a higher proportion of younger primary carers than Japan: In Italy, 6.2% of all primary family caregivers were under the age of 35, of which 1.1% were men and 5.1% were women. In Japan, those under the age of 40 remained 1.8%, of whom 0.6% were men and 1.2% were women. When looking at the under-45 age group in Italy and the under-50 age group in Japan, there were 6.4% men and 11.9% women, for a total of 18.3% of all family primary caregivers in Italy, compared with 2.9% men and 5.8% women, for a total of 8.7%, in Japan;
- Japan has a higher proportion of much older primary carers than Italy: In Italy, primary caregivers aged 75 and over accounted for 13.3% of all caregivers, of whom 5.4% were men and 7.9% were women. In Japan, on the other hand, primary caregivers aged 80 and over accounted for 16.2% of all primary caregivers, of whom 8.4% were men and 7.8% were women;
- The gender and age group with the highest proportion among all primary caregivers was 18.1% of women aged 45–54 in Italy, followed by 17.2% of women aged 55–64, with these two groups accounting for 35.3% of the total. In Japan, on the other hand, women aged 60–69 accounted for 21.8% of the total, followed by women aged 70–79 with 16.6%, with these two groups making up 38.4% of the total.
- Spouses account for the highest share of all primary family caregivers, at 42.9%, in Japan. In Italy, on the other hand, spouses accounted for the third highest percentage, at 10.9%;
- Children represented 37.1% of coresident family primary caregivers in Japan, the second-largest group. In contrast, children constituted 60.9% of caregivers in Italy, making them the largest group;
- Daughters and/or sons in law represented the third-largest group of caregivers in Japan (16.5%) and the fourth largest in Italy (9.7%).
6. Work–LTC Reconciliation and Family Primary Caregivers
7. Results
- Between Italy and Japan, there exists a similar welfare state configuration, such as the most “old-age-biased” redistribution, lower social spending on the working-age population, and the highest government debt among other OECD countries. Additionally, since the 2000s, both Italy and Japan represent a movement away from the former strong “familialism by default” and or “unsupported familialism” care model, which was common in both countries until the 1990s;
- A contrasting LTC policy and provision, such as the cash-based public system with (grey-)market-based care provision frequently by migrant domestic workers in Italy, and a state-based in-kind care provision in Japan were observed especially since the 2000s. A more detailed comparison of the latest LTC-related data revealed that, despite this different LTC policy developments, both the total LTC expenditure as a percentage of GDP and the ratio of LTC workers to the older population were close, which were also lower than the EU27 average;
- Regarding the types of LTC provided, the largest differences between the two countries were found for LTC cash benefit: Both its share in all LTC recipients and in all public spending for LTC were particularly high in Italy, compared to the EU27 average, as well as to Japan, where they were both 0%. In contrast, in both countries, the proportion of informal carers with longer caregiving hours (more than 20 h per week) was also outstandingly high compared to the EU27 average;
- Intrafamily caregiving roles for the dependent older adults showed relevant differences. While the primary family caregivers’ gender proportion was exactly the same between Italy and Japan, they were consistently younger in Italy, with 44.4% of all primary family caregivers aged under 65, in contrast in Japan with 29.9% even under the age of 60. The primary family caregivers of older people tended to be children of working age in Italy and much older spouses in Japan.
8. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Daly, M. Care as a good for social policy. J. Soc. Policy 2002, 31, 251–270. [Google Scholar] [CrossRef]
- Daly, M. Making policy for care, experience in Europe and its implications in Asia. Int. J. Sociol. Soc. Policy 2012, 32, 623–635. [Google Scholar] [CrossRef]
- Gregory, A.; Milner, S.; Windebank, J. Work-life balance in times of economic crisis and austerity. Int. J. Sociol. Soc. Policy 2013, 33, 528–541. [Google Scholar] [CrossRef]
- León, M.; Pavolini, E. Social Investment’ or Back to ‘Familism’: The Impact of the Economic Crisis on Family and Care Policies in Italy and Spain. South Eur. Soc. Politics 2014, 19, 353–369. [Google Scholar] [CrossRef]
- United Nations. World Population Prospects 2019, Data Booklet; United Nations: New York, NY, USA, 2019.
- Osawa, M. Governance of Livelihood Security; Yuhikaku: Tokyo, Japan, 2013. (In Japanese) [Google Scholar]
- Tepe, M.; Vanhuysse, P. Elderly bias, new social risks and social spending, change and timing in eight programmes across four worlds of welfare, 1980–2003. J. Eur. Soc. Policy 2010, 20, 217–234. [Google Scholar] [CrossRef]
- Bambra, C. Defamilisation and welfare state regimes, a cluster analysis. Int. J. Soc. Welf. 2007, 16, 326–338. [Google Scholar] [CrossRef]
- Uzuhashi, T. Trend in International Welfare Policy and Choice of Japan; Horitsu Bunka-Sha: Kyoto, Japan, 2011. (In Japanese) [Google Scholar]
- Leitner, S. Varieties of Familiarism. Eur. Soc. 2003, 5, 353–375. [Google Scholar] [CrossRef]
- Bettio, F.; Plantenga, J. Comparing care regimes in Europe. Fem. Econ. 2004, 10, 85–113. [Google Scholar] [CrossRef]
- Theobald, H.; Szebehely, M.; Saito, Y.; Ishiguro, N. Marketisation policies in different contexts: Consequences for home-care workers in Germany, Japan and Sweden. Int. J. Soc. Welf. 2018, 27, 215–225. [Google Scholar] [CrossRef]
- Ranci, C.; Pavolini, E. Reforms in Long-Term Care Policies in Europe, Investigating Institutional Change and Social Impacts; Springer: New York, NY, USA, 2013. [Google Scholar]
- Saraceno, C. Varieties of familialism: Comparing four southern European and East Asian welfare regimes. J. Eur. Soc. Policy 2016, 26, 314–326. [Google Scholar] [CrossRef]
- Da Roit, B.; Le Bihan, B. Cash for long-term care: Policy debates, visions, and designs on the move. Soc. Policy Adm. 2019, 53, 519–536. [Google Scholar] [CrossRef]
- Timonen, V.; Convery, J.; Cahillt, S. Care revolutions in the making? A comparison of cash-for-care programmes in four European countries. Ageing Soc. 2016, 26, 455–474. [Google Scholar] [CrossRef]
- Tretteteig, S.; Vatne, S.; Rokstad, A.M.M. The influence of day care centres designed for people with dementia on family caregivers—A qualitative study. BMC Geriatr. 2017, 17, 5. [Google Scholar] [CrossRef] [PubMed]
- Bettio, F.; Simonazzi, A.; Villa, P. Change in care regimes and female migration, the ‘care drain’ in the Mediterranean. J. Eur. Soc. Policy 2006, 16, 271–285. [Google Scholar] [CrossRef]
- Saraceno, C.; Keck, W. Can We Identify Intergenerational Policy Regimes in Europe? Eur. Soc. 2010, 12, 675–696. [Google Scholar] [CrossRef]
- Estévez-Abe, M.; Naldini, M. Politics of defamilialization: A comparison of Italy, Japan, Korea and Spain. J. Eur. Soc. Policy 2016, 26, 327–343. [Google Scholar] [CrossRef]
- Ochiai, E.; Abe, A.; Uzuhashi, T.; Tamiya, Y.; Shikata, M. Reconfiguration of Care Diamond in Japan: The Impact of the LTCI on Familialism. Rev. Comp. Soc. Secur. Res. 2010, 170, 4–19. (In Japanese) [Google Scholar]
- Soma, N.; Yamashita, J. Child care and elder care regimes in Japan. J. Comp. Soc. Welf. 2011, 27, 133–142. [Google Scholar] [CrossRef]
- Iwama, O. The position of informal carers in policy documents and public support. Fam. Relat. 2009, 28, 3–16. (In Japanese) [Google Scholar]
- Hiraoka, K. Introduction and Reform of National Long-Term Care Insurance System and Japan’s Care Regime for Older Adults. In Elderly Care in East Asia: State, Region and Family; Suda, Y., Hiraoka, K., Morikawa, M., Eds.; Toshindo: Tokyo, Japan, 2018; pp. 54–80. (In Japanese) [Google Scholar]
- Yeandle, S.; Kröger, T.; Cass, B. Voice and choice for users and carers? Developments in patterns of care for older people in Australia, England and Finland. J. Eur. Soc. Policy 2012, 22, 432–445. [Google Scholar] [CrossRef]
- Ferrera, M. Resemblances that matter: Lessons from the comparison between Southern Europe and East Asia. J. Eur. Soc. Policy 2016, 26, 374–383. [Google Scholar] [CrossRef]
- Peng, I. Shaping and Reshaping Care and Migration in East and Southeast Asia. Crit. Sociol. 2018, 44, 1117–1132. [Google Scholar] [CrossRef]
- OECD. Society at a Glance 2019; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Lynch, J. Age in the Welfare State: The Origins of Social Spending on Pensioners, Workers, and Children; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Scruggs, L.; Allan, J. Welfare-State Decommodification in 18 Oecd Countries: A Replication and Revision. J. Eur. Soc. Policy 2006, 16, 55–72. [Google Scholar] [CrossRef]
- OECD. Government at a Glance 2019; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Nikolai, R. Towards social investment? Patterns of public policy in the OECD world. In Towards a Social Investment Welfare State; Morel, N., Palier, B., Palme, J., Eds.; Policy Press: Bristol, UK, 2012; pp. 91–115. [Google Scholar]
- Budlender, D. Time Use Studies and Unpaid Care Work; Routledge: London, UK, 2010; Volume 7. [Google Scholar]
- OECD. Health at a Glance 2019; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Hank, K.; Buber, I. Grandparents Caring for their Grandchildren, Findings from the 2004 Survey of Health, Ageing, and Retirement in Europe. J. Fam. Issues 2008, 30, 53–73. [Google Scholar] [CrossRef]
- Eurobarometer. Health and Long-Term Care in the European Union; Eurobarometer: Brussels, Belgium, 2007; 283p. [Google Scholar]
- Quattrini, S.; Melchiorre, M.G.; Balducci, C.; Spazzafumo, L.; Lamura, G. Services for Supporting Family Carers of Older Dependent People in Europe, Characteristics, Coverage and Usage. Natl. Surv. Rep. Italy 2006, 6, 1–215. [Google Scholar]
- Pavolini, E.; Ranci, C. Restructuring the welfare state: Reforms in long-term care in Western European countries. J. Eur. Soc. Policy 2008, 18, 246–259. [Google Scholar] [CrossRef]
- MHLW, Overview of the Long-Term Care Insurance System. 2021. (In Japanese). Available online: https://www.mhlw.go.jp/content/000801559.pdf (accessed on 10 May 2022).
- MLPS (Ministero del Lavoro e delle Politiche Sociali). Rapporto Sulla non Autosufficienza in Italia—2010; Maggiori Editore: Santarcangelo di Romagna, Italy, 2010. [Google Scholar]
- Simonazzi, A. Care regimes and national employment models. Camb. J. Econ. 2009, 33, 211–232. [Google Scholar] [CrossRef]
- European Commission. Long-Term Care Report Trends, Challenges and Opportunities in an Ageing Society Country Profiles; Publications Office of the European Union: Luxembourg, 2021; Volume II.
- MHLW (Ministry of Health Labour and Welfare). The Situation in Long Term Care Sector. Available online: https://www.mhlw.go.jp/content/12300000/000608284.pdf (accessed on 10 May 2022).
- MHLW. Overview of Actual Statistics of Long-Term Care Benefit Costs in 2019. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/kaigo/kyufu/19/dl/11.pdf (accessed on 10 May 2022).
- Istat. Condizioni di Salute e Ricorso ai Servizi Sanitari in Italia e nell’Unione Europea—Indagine Ehis 2015; Istat: Rome, Italy, 2017. [Google Scholar]
- MHLW. Comprehensive Survey of Living Conditions 2016; Kouseiroudou Toukeikyoukai: Tokyo, Japan, 2017. (In Japanese) [Google Scholar]
- Di Rosa, M.; Merchiorre, M.; Lamura, G. I servizi domiciliari tra reti informali ed assistenti famigliari. Psicogeriatria 2010, 3, 61–71. [Google Scholar]
- Morgan, K.J. Caring Time Policies in Western Europe, Trends and Implications. Comp. Eur. Politics 2009, 7, 37–55. [Google Scholar] [CrossRef]
- Mentzakis, E.; McNamee, P.; Ryan, M. Who cares and how much, exploring the determinants of co-residential informal care. Rev. Econ. Househ. 2008, 7, 283–303. [Google Scholar] [CrossRef]
- Pagani, L.; Marenzi, A. The Labor Market Participation of Sandwich Generation Italian Women. J. Fam. Econ. Issues 2008, 29, 427–444. [Google Scholar] [CrossRef]
- OECD. Employment Outlook 2020; OECD Publishing: Paris, France, 2020. [Google Scholar]
- OECD. Labour Force Statistics 2010–2019; OECD Publishing: Paris, France, 2020. [Google Scholar]
- Kröger, T. Defamilisation, dedomestication and care policy. Int. J. Sociol. Soc. Policy 2011, 31, 424–440. [Google Scholar] [CrossRef]
- Takada, H. Current Status of Turnover Due to Long-Term Care; Meiji Yasuda Research Institute: Meiji, Japan, 2020; Available online: https://www.myri.co.jp/publication/myilw/pdf/myri_no100_web_01.pdf (accessed on 10 May 2022). (In Japanese)
- Miyazaki, R. A descriptive analysis of three-generation households and mothers’ employment in Japan, 2002–2019. Int. J. Sociol. Soc. Policy 2021, 41, 34–50. [Google Scholar] [CrossRef]


{kind=link}
| Old-Age Dependency Ratio (1) (2020) | Life Expectancy (2019) | Total Net Public Social Expenditure (2) (2018) | Income Support to the Working Age (2) (2017) | Old-Age Social Spending (2) (2017) | General Government Debt (2) (2017) | |
|---|---|---|---|---|---|---|
| Japan | 52.0 | M:84.4 F:87.4 | 21.9% | 4.1% | 10.88% | 222.1% |
| Italy | 39.5 | M:83.6 F:85.7 | 27.9% | 1.8% | 13.35% | 152.9% |
| OECD | -- | M:81.0 F:83.6 | 20.1% | 8.0% | 9.97% | 110.3% |
| On LTC as % of GDP | On Cash Benefits as % of LTC Spending | On Home Care as % of LTC Spending | On Institutional Care as % of LTC Spending | |
|---|---|---|---|---|
| Italy | 1.7% | 52.3% | 19.5% | 28.2% |
| Japan | 1.8% (1) | 0% | 44.7% | 33.1% |
| EU27 | 1.7% | 26.4% | 25.5% | 48.1% |
| Share of Pop. 65+ Receiving LTC in Institution | Share of Pop. 65+ Receiving LTC at Home | Share of Pop. 65+ Receiving LTC Cash Benefits | |
|---|---|---|---|
| Italy | 3.2% | 4.7% | 10.9% |
| Japan | 2.7% (1) | 10.7% (2) | 0% (3) |
| EU27 | 3.6% | 5.8% | 8.8% |
| LTC Workers as % of Population Aged 65+ | Share of Pop. Providing Informal Care | Share of Informal Carers Providing Care More than 20 h/w | |
|---|---|---|---|
| Italy | 1.7% (2021) | 5.8% (2016) | 40.5% (2016) |
| Japan | 1.8% (2019) | -- | 43.7% |
| EU27 | 3.8% (2016) | 10.3% (2016) | 22.2% (2016) |
| Employment Rate (Aged 15–64) | Unemployment Rate (15–64) | Long-Term Unemployment Rate | Part-Time Employment Share | Women’s Share in Part-Time Employment | ||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |||
| Japan | 84.1 | 70.9 | 2.6 | 2.3 | 41.5 | 19.4 | 25.2 | 68.5 |
| Italy | 68.0 | 50.1 | 9.3 | 11.3 | 57.4 | 56.7 | 18.0 | 74.9 |
| OECD | 76.3 | 61.4 | 5.4 | 5.7 | 25.3 | 26.5 | 16.7 | 68.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyazaki, R. Long-Term Care and the State-Family Nexus in Italy and Japan—The Welfare State, Care Policy and Family Caregivers. Int. J. Environ. Res. Public Health 2023, 20, 2027. https://doi.org/10.3390/ijerph20032027
Miyazaki R. Long-Term Care and the State-Family Nexus in Italy and Japan—The Welfare State, Care Policy and Family Caregivers. International Journal of Environmental Research and Public Health. 2023; 20(3):2027. https://doi.org/10.3390/ijerph20032027
Chicago/Turabian StyleMiyazaki, Rie. 2023. "Long-Term Care and the State-Family Nexus in Italy and Japan—The Welfare State, Care Policy and Family Caregivers" International Journal of Environmental Research and Public Health 20, no. 3: 2027. https://doi.org/10.3390/ijerph20032027
APA StyleMiyazaki, R. (2023). Long-Term Care and the State-Family Nexus in Italy and Japan—The Welfare State, Care Policy and Family Caregivers. International Journal of Environmental Research and Public Health, 20(3), 2027. https://doi.org/10.3390/ijerph20032027