
Knowledge of Self-Isolation Rules in the UK for Those Who Have Symptoms of COVID-19: A Repeated Cross-Sectional Survey Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Study Materials
2.3.1. Outcome Measures
2.3.2. Explanatory Factors
2.4. Ethics
2.5. Power
2.6. Analysis
3. Results
Comparison of Item Phrasing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
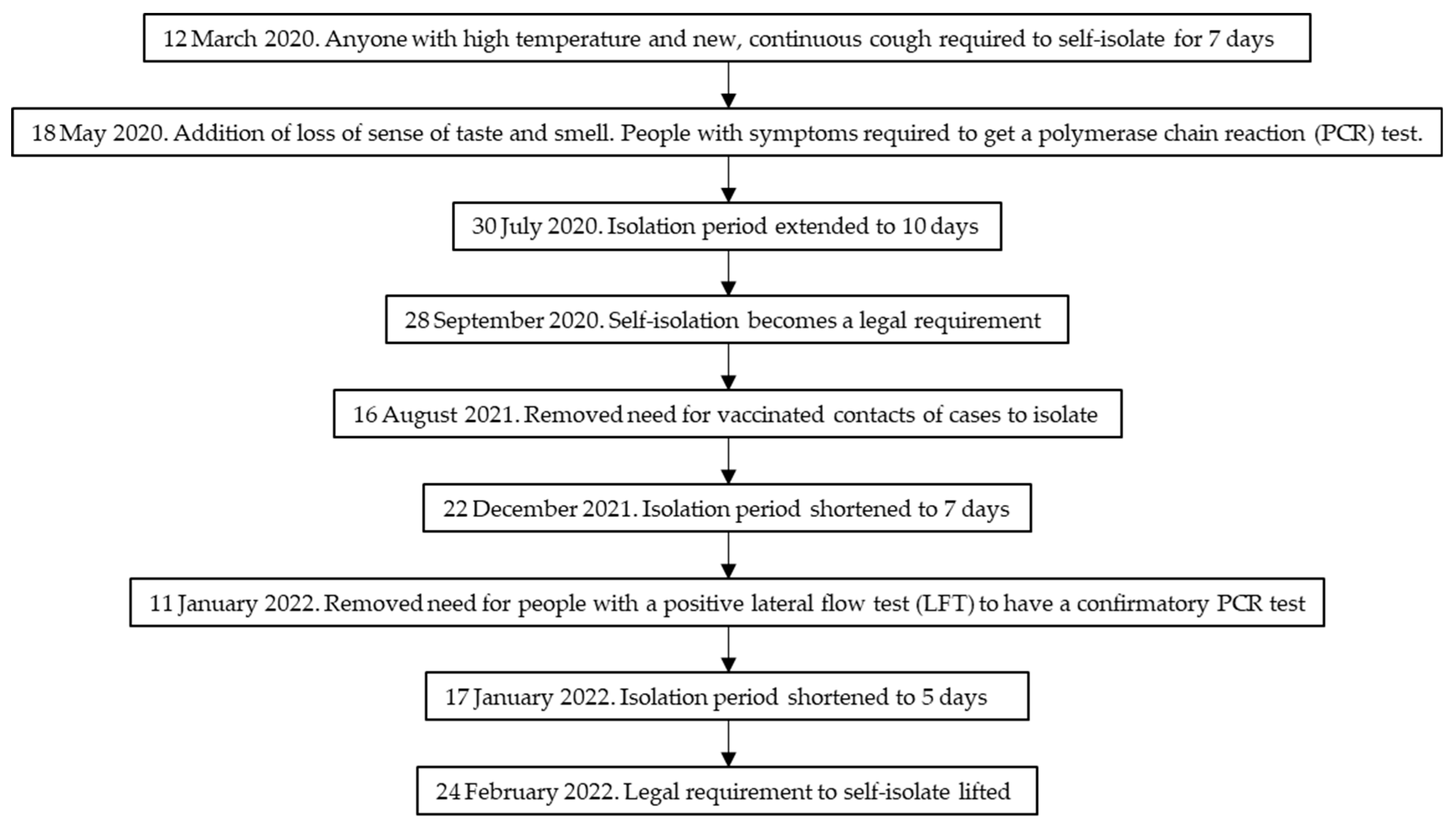
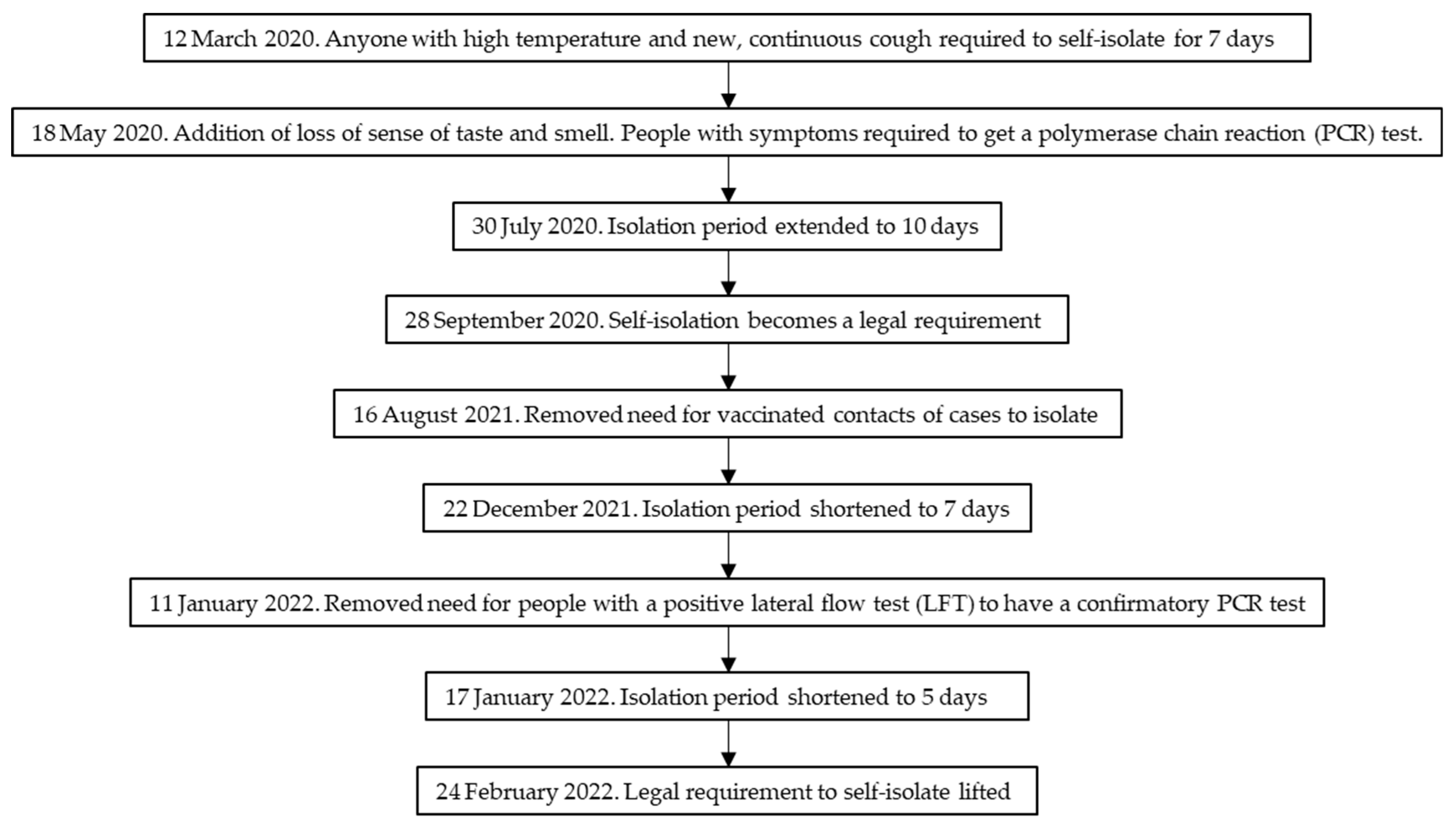
- Johnson, B. Prime Minister’s Statement on Coronavirus (COVID-19): 12 March 2020. 2020. Available online: https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-12-march-2020 (accessed on 2 June 2021).
- Department of Health and Social Care. Statement from the UK Chief Medical Officers on an Update to Coronavirus Symptoms: 18 May 2020. 2020. Available online: https://www.gov.uk/government/news/statement-from-the-uk-chief-medical-officers-on-an-update-to-coronavirus-symptoms-18-may-2020 (accessed on 26 July 2022).
- NHS. Main Symptoms of Coronavirus (COVID-19). 2021. Available online: https://www.nhs.uk/conditions/coronavirus-covid-19/symptoms/main-symptoms/ (accessed on 19 August 2021).
- Public Health England. Stay at Home: Guidance for Households with Possible or Confirmed Coronavirus (COVID-19) Infection. 2021. Available online: https://www.gov.uk/government/publications/covid-19-stay-at-home-guidance/stay-at-home-guidance-for-households-with-possible-coronavirus-covid-19-infection#symptoms (accessed on 27 September 2021).
- Department of Health and Social Care. Everyone in the United Kingdom with Symptoms Now Eligible for Coronavirus Tests. 2020. Available online: https://www.gov.uk/government/news/everyone-in-the-united-kingdom-with-symptoms-now-eligible-for-coronavirus-tests#:~:text=Everyone%20in%20England%2C%20Scotland%2C%20Wales,can%20now%20get%20a%20test.&text=The%20government%20has%20today%20announced,the%20test%20and%20trace%20service (accessed on 2 June 2021).
- Department of Health and Social Care. Statement from the UK Chief Medical Officers on Extension of Self-Isolation Period: 30 July 2020. 2020. Available online: https://www.gov.uk/government/news/statement-from-the-uk-chief-medical-officers-on-extension-of-self-isolation-period-30-july-2020 (accessed on 11 January 2023).
- Department of Health and Social Care. New Legal Duty to Self-Isolate Comes into Force Today. 2020. Available online: https://www.gov.uk/government/news/new-legal-duty-to-self-isolate-comes-into-force-today (accessed on 2 June 2021).
- Department of Health and Social Care, Sajid Javid. Self-Isolation Removed for Double-Jabbed Close Contacts from 16 August. 2021. Available online: https://www.gov.uk/government/news/self-isolation-removed-for-double-jabbed-close-contacts-from-16-august (accessed on 26 July 2022).
- UK Health Security Agency. Self-isolation for COVID-19 Cases Reduced from 10 to 7 Days following Negative LFD Tests. 2021. Available online: https://www.gov.uk/government/news/self-isolation-for-covid-19-cases-reduced-from-10-to-7-days-following-negative-lfd-tests (accessed on 26 July 2022).
- UK Health Security Agency. Confirmatory PCR Tests to be Temporarily Suspended for Positive Lateral Flow Test Results. 2022. Available online: https://www.gov.uk/government/news/confirmatory-pcr-tests-to-be-temporarily-suspended-for-positive-lateral-flow-test-results (accessed on 26 July 2022).
- UK Health Security Agency. Self-Isolation for those with COVID-19 can end after 5 Full Days following 2 Negative LFD Tests. 2022. Available online: https://www.gov.uk/government/news/self-isolation-for-those-with-covid-19-can-end-after-five-full-days-following-two-negative-lfd-tests (accessed on 26 July 2022).
- Prime Minister’s Office. PM Statement on Living with COVID: 21 February 2022. 2022. Available online: https://www.gov.uk/government/speeches/pm-statement-on-living-with-covid-21-february-2022 (accessed on 18 July 2022).
- Smith, L.E.; Potts, H.W.W.; Amlot, R.; Fear, N.T.; Michie, S.; Rubin, G.J. Adherence to the test, trace, and isolate system in the UK: Results from 37 nationally representative surveys. BMJ 2021, 372, n608. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Amlȏt, R.; Lambert, H.; Oliver, I.; Robin, C.; Yardley, L.; Rubin, G. Factors associated with adherence to self-isolation and lockdown measures in the UK: A cross-sectional survey. Public Health 2020, 187, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Office for National Statistics. Coronavirus and Self-Isolation after Testing Positive in England: 1 February to 13 February 2021. 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/bulletins/coronavirusandselfisolationaftertestingpositiveinengland/1februaryto13february2021 (accessed on 18 July 2021).
- Office for National Statistics. Coronavirus and Self-Isolation after Testing Positive in England: 5 July to 10 July 2021. 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/bulletins/coronavirusandselfisolationaftertestingpositiveinengland/5julyto10july2021 (accessed on 27 September 2021).
- Institute for Government. Coronavirus and Devolution. 2020. Available online: https://www.instituteforgovernment.org.uk/explainers/coronavirus-and-devolution (accessed on 19 August 2021).
- McIntyre, S.; Roy, G. Has Devolution Led to Different Outcomes during the COVID-19 Crisis? 2021. Available online: https://www.economicsobservatory.com/has-devolution-led-to-different-outcomes-during-the-covid-19-crisis (accessed on 19 August 2021).
- Senedd Research. Coronavirus Timeline: Welsh and UK Governments’ Response. 2022. Available online: https://research.senedd.wales/research-articles/coronavirus-timeline-welsh-and-uk-governments-response/ (accessed on 26 July 2022).
- The Scottish Parliament. Timeline of Coronavirus (COVID-19) in Scotland. 2022. Available online: https://spice-spotlight.scot/2022/06/30/timeline-of-coronavirus-covid-19-in-scotland/ (accessed on 26 July 2022).
- Institute for Government. Coronavirus Lockdown Rules in Each Part of the UK. 2022. Available online: https://www.instituteforgovernment.org.uk/explainers/coronavirus-lockdown-rules-four-nations-uk (accessed on 26 July 2022).
- Wright, L.; Steptoe, A.; Fancourt, D. Patterns of compliance with COVID-19 preventive behaviours: A latent class analysis of 20,000 UK adults. J. Epidemiol. Community Health 2022, 76, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.N.; Armitage, C.J.; Tampe, T.; Dienes, K.A. Public perceptions of non-adherence to pandemic protection measures by self and others: A study of COVID-19 in the United Kingdom. PLoS ONE 2021, 16, e0258781. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Housing Communities and Local Government. The English Indices of Deprivation 2019. 2019. Available online: https://www.gov.uk/government/statistics/english-indices-of-deprivation-2019 (accessed on 2 June 2021).
- Office for National Statistics. Population Estimates for the UK, England and Wales, Scotland and Northern Ireland: Mid-2018. 2019. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/bulletins/annualmidyearpopulationestimates/mid2018 (accessed on 25 August 2020).
- Prime Minister’s Office, 10 Downing Street. New Package to Support and Enforce Self-Isolation. 2020. Available online: https://www.gov.uk/government/news/new-package-to-support-and-enforce-self-isolation (accessed on 2 June 2021).
- Cabinet Office. New Rules on Staying at Home and Away from Others. 2020. Available online: https://www.gov.uk/government/publications/full-guidance-on-staying-at-home-and-away-from-others/full-guidance-on-staying-at-home-and-away-from-others (accessed on 25 April 2020).
- Johnson, B. PM Address to the Nation on Coronavirus: 23 March 2020. 2020. Available online: https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-23-march-2020 (accessed on 25 April 2020).
- GOV.UK. Prime Minister Announces National Lockdown. 2021. Available online: https://www.gov.uk/government/news/prime-minister-announces-national-lockdown (accessed on 21 June 2021).
- Michie, S.; Potts, H.W.W.; West, R.; Amlot, R.; Smith, L.E.; Fear, N.T.; Rubin, G.J. Factors associated with non-essential workplace attendance during the COVID-19 pandemic in the UK in early 2021: Evidence from cross-sectional surveys. Public Health 2021, 198, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, C.; Edmunds, J.; CMMID COVID-19 Working Group. Social Contacts in Workplace the UK from the CoMix Social Contact Survey. 2021. Available online: https://cmmid.github.io/topics/covid19/reports/comix/Comix%20Report%20contacts%20in%20the%20workplace.pdf (accessed on 29 September 2021).
- Smith, L.E.; Potts, H.W.W.; Amlȏt, R.; Fear, N.T.; Michie, S.; Rubin, G.J. Do Members of the Public Think They Should Use Lateral Flow Tests or PCR Tests when they Have COVID-19-Like Symptoms? The COVID-19 Rapid Survey of Adherence to Interventions and Responses [CORSAIR] Study. Public Health 2021, 198, 260–262. [Google Scholar] [CrossRef] [PubMed]
- Office for National Statistics. Population Estimates for the UK, England and Wales, Scotland and Northern Ireland: Mid-2020. 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/bulletins/annualmidyearpopulationestimates/mid2020 (accessed on 15 October 2021).
- Kohler, U.; Possible Uses of Nonprobability Sampling for the Social Sciences. Survey Methods: Insights from the Field. 2019. Available online: https://surveyinsights.org/?p=10981 (accessed on 21 June 2021).

{kind=link}
| The Government Has Issued Advice on How People Should Help Prevent the Spread of Coronavirus if They Have Symptoms. If You Have Symptoms of Coronavirus, You: [Total n = 76,562] | True, % (n) | False, % (n) | Don’t Know, % (n) |
|---|---|---|---|
| Should self-isolate | 87.9 (67,288) | 7.5 (5773) | 4.6 (3501) |
| Could be eligible for self-isolation payments (if you are on benefits and/or a lower income and cannot work from home) | 59.6 (45,642) | 11.9 (9120) | 28.5 (21,800) |
| Can go out if your symptoms are mild | 9.0 (6899) | 84.6 (64,780) | 6.4 (4883) |
| Can go to the shops for groceries/pharmacy * | 23.0 (17,593) | 71.6 (54,808) | 5.4 (4160) |
| Can go to the shops for things other than groceries/pharmacy * | 16.2 (12,370) | 78.7 (60,247) | 5.2 (3945) |
| Can go for a walk or some other exercise | 30.4 (23,296) | 62.0 (47,446) | 7.6 (5820) |
| Can go out to work if you cannot work from home | 21.1 (16,185) | 73.3 (56,085) | 5.6 (4292) |
| Can go out to help or provide care for a vulnerable person | 20.5 (15,721) | 71.8 (54,976) | 7.7 (5864) |
| Can go out if you’re wearing a face covering | 20.7 (15,885) | 72.7 (55,643) | 6.6 (5034) |
| Can go out to meet up with friends and/or family that you don’t live with, indoors * | 12.4 (9495) | 83.0 (63,528) | 4.6 (3539) |
| Can go out to meet up with friends and/or family that you don’t live with, outdoors | 16.3 (12,454) | 78.6 (60,147) | 5.2 (3960) |
| Can go out to spend time outdoors for recreational purposes (including to sit in parks, etc.) | 24.7 (18,890) | 68.6 (52,525) | 6.7 (5147) |
| Can have someone who you don’t live with over to your home * | 12.1 (9241) | 82.6 (63,229) | 5.3 (4092) |
| Can go out to get a test to see if you have coronavirus | 66.9 (51,229) | 23.3 (17,822) | 9.8 (7510) |
| Should get a test, but can go out as normal while you are waiting for the result [included in waves 32 to 50, total n = 36,509] | 13.8 (5051) | 79.1 (28,883) | 7.1 (2574) |
| Should take a rapid ‘lateral flow’ coronavirus test (results within 30 min) [included in waves 51 to 52, total n = 4043] | 69.8 (2823) | 14.9 (604) | 15.2 (616) |
| Should take a lab-processed ‘PCR’ coronavirus test (results typically within a day or two) [included in waves 51 to 52, total n = 4043] | 77.0 (3114) | 9.4 (381) | 13.6 (549) |
| Should take a test [included in waves 53 to 68, total n = 36,010] | 89.7 (32,303) | 6.4 (2318) | 3.9 (1389) |
| Factor | Level | Key Knowledge Incorrect (Total n = 28,133), (%) n | Key Knowledge Correct (Total n = 47,345), (%) n | Adjusted Odds Ratio (95% CI) for Getting Key Knowledge Measure Correct † | p |
|---|---|---|---|---|---|
| Survey wave | 9 to 11 November 2020 (wave 32) | 39.6 (801) | 60.4 (1221) | Reference | - |
| 16 to 18 November 2020 (wave 33) | 42.4 (868) | 57.6 (1179) | 0.93 (0.82 to 1.06) | 0.28 | |
| 23 to 25 November 2020 (wave 34) | 40.6 (815) | 59.4 (1194) | 0.98 (0.86 to 1.11) | 0.73 | |
| 30 November to 2 December 2020 (wave 35) | 40.8 (834) | 59.2 (1208) | 0.99 (0.87 to 1.12) | 0.83 | |
| 7 to 9 December 2020 (wave 36) | 46.2 (968) | 53.8 (1126) | 0.73 (0.65 to 0.83) | <0.001 * | |
| 14 to 16 December 2020 (wave 37) | 47.0 (948) | 53.0 (1068) | 0.74 (0.65 to 0.84) | <0.001 * | |
| 21 to 23 December 2020 (wave 38) | 48.0 (966) | 52.0 (1046) | 0.72 (0.63 to 0.81) | <0.001 * | |
| 28 to 30 December 2020 (wave 39) | 46.5 (909) | 53.5 (1047) | 0.75 (0.66 to 0.85) | <0.001 * | |
| 4 to 6 January 2021 (wave 40) | 42.6 (857) | 57.4 (1153) | 0.85 (0.75 to 0.96) | 0.01 | |
| 11 to 13 January 2021 (wave 41) | 39.9 (797) | 60.1 (1199) | 1.02 (0.90 to 1.16) | 0.73 | |
| 25 to 27 January 2021 (wave 42) | 41.5 (831) | 58.5 (1170) | 0.93 (0.82 to 1.06) | 0.27 | |
| 8 to 9 February 2021 (wave 43) | 39.5 (793) | 60.5 (1215) | 1.05 (0.93 to 1.19) | 0.45 | |
| 22 to 23 February 2021 (wave 44) | 38.0 (764) | 62.0 (1245) | 1.10 (0.97 to 1.25) | 0.12 | |
| 8 to 9 March 2021 (wave 45) | 40.6 (813) | 59.4 (1191) | 1.04 (0.92 to 1.18) | 0.51 | |
| 22 to 23 March 2021 (wave 46) | 41.4 (847) | 58.6 (1200) | 1.00 (0.88 to 1.13) | 0.99 | |
| 6 to 7 April 2021 (wave 47) | 39.2 (392) | 60.8 (607) | 1.08 (0.92 to 1.28) | 0.33 | |
| 19 to 21 April 2021 (wave 48) | 39.2 (389) | 60.8 (604) | 1.11 (0.95 to 1.30) | 0.19 | |
| 4 to 5 May 2021 (wave 49) | 38.6 (775) | 61.4 (1232) | 1.15 (1.01 to 1.31) | 0.03 | |
| 17 to 19 May 2021 (wave 50) | 40.3 (815) | 59.7 (1205) | 1.07 (0.95 to 1.21) | 0.28 | |
| 1 to 2 June 2021 (wave 51) | 40.5 (819) | 59.5 (1203) | 1.04 (0.92 to 1.17) | 0.52 | |
| 14 to 16 June 2021 (wave 52) | 41.0 (822) | 59.0 (1185) | 0.99 (0.88 to 1.12) | 0.89 | |
| 28 to 29 June 2021 (wave 53) | 39.5 (788) | 60.5 (1206) | 1.03 (0.91 to 1.17) | 0.62 | |
| 26 to 27 July 2021 (wave 54) | 40.4 (802) | 59.6 (1185) | 1.06 (0.94 to 1.20) | 0.36 | |
| 9 to 10 August 2021 (wave 55) | 39.1 (785) | 60.9 (1221) | 1.07 (0.95 to 1.21) | 0.26 | |
| 23 to 24 August 2021 (wave 56) | 40.9 (820) | 59.1 (1186) | 1.01 (0.90 to 1.15) | 0.84 | |
| 6 to 7 September 2021 (wave 57) | 41.2 (836) | 58.8 (1193) | 1.05 (0.93 to 1.19) | 0.44 | |
| 20 to 22 September 2021 (wave 58) | 24.7 (465) | 75.3 (1421) | 2.04 (1.79 to 2.32) | <0.001 * | |
| 4 to 6 October 2021 (wave 59) | 28.3 (534) | 71.7 (1350) | 1.80 (1.58 to 2.06) | <0.001 * | |
| 18 to 20 October 2021 (wave 60) | 25.8 (476) | 74.2 (1372) | 1.98 (1.73 to 2.26) | <0.001 * | |
| 1 to 4 November 2021 (wave 61) | 23.4 (506) | 76.6 (1661) | 2.14 (1.89 to 2.43) | <0.001 * | |
| 15 to 17 November 2021 (wave 62) | 31.8 (689) | 68.2 (1477) | 1.54 (1.36 to 1.74) | <0.001 * | |
| 29 November to 1 December 2021 (wave 63) | 32.0 (657) | 68.0 (1397) | 1.62 (1.43 to 1.84) | <0.001 * | |
| 6 to 8 December 2021 (wave 63.5) | 30.6 (625) | 69.4 (1415) | 1.63 (1.44 to 1.85) | <0.001 * | |
| 13 to 16 December 2021 (wave 64) | 31.3 (681) | 68.7 (1493) | 1.46 (1.29 to 1.65) | <0.001 * | |
| 4 to 6 January 2022 (wave 65) | 28.9 (643) | 71.1 (1583) | 1.71 (1.51 to 1.94) | <0.001 * | |
| 17 to 20 January 2022 (wave 66) | 27.0 (608) | 73.0 (1645) | 1.93 (1.70 to 2.19) | <0.001 * | |
| 31 January to 2 February 2022 (wave 67) | 30.8 (676) | 69.2 (1516) | 1.61 (1.42 to 1.82) | <0.001 * | |
| 14 to 16 February 2022 (wave 68) | 32.0 (719) | 68.0 (1527) | 1.48 (1.31 to 1.67) | <0.001 * | |
| Age (per decade) | Range 16 to over 100 years | M = 43.5, SD = 18.9 | M = 50.2, SD = 17.8 | 1.23 (1.22 to 1.25) | <0.001 * |
| Gender | Male | 45.0 (16,474) | 55.0 (20,167) | Reference | - |
| Female | 30.0 (11,556) | 70.0 (26,995) | 1.94 (1.88 to 2.01) | <0.001 * | |
| Prefer to self-describe | 33.6 (73) | 66.4 (144) | 2.31 (1.67 to 3.19) | <0.001 * | |
| Prefer not to say | 43.7 (31) | 56.3 (40) | 1.62 (0.97 to 2.68) | 0.06 | |
| Nation | England | 38.7 (24,562) | 61.3 (38,860) | Reference | - |
| Scotland | 28.1 (1750) | 71.9 (4468) | 1.55 (1.45 to 1.66) | <0.001 * | |
| Wales | 32.6 (1205) | 67.4 (2492) | 1.16 (1.07 to 1.26) | <0.001 * | |
| Northern Ireland | 28.8 (617) | 71.2 (1525) | 1.55 (1.36 to 1.78) | <0.001 * | |
| Index of multiple deprivation | 1st quartile (least deprived) to 4th quartile (most deprived) | M = 2.6, SD = 1.1 | M = 2.5, SD = 1.1 | 0.97 (0.96 to 0.99) | <0.001 * |
| Information from the Government about COVID-19 can be trusted | Strongly agree | 44.4 (3708) | 55.6 (4642) | Reference | - |
| Agree | 35.0 (8990) | 65.0 (16,691) | 1.39 (1.32 to 1.47) | <0.001 * | |
| Neither agree nor disagree | 38.6 (7591) | 61.4 (12,092) | 1.33 (1.26 to 1.41) | <0.001 * | |
| Disagree | 32.8 (4149) | 67.2 (8489) | 1.68 (1.58 to 1.79) | <0.001 * | |
| Strongly Disagree | 40.4 (2946) | 59.6 (4347) | 1.33 (1.24 to 1.43) | <0.001 * | |
| Don’t know | 46.1 (557) | 53.9 (652) | 1.11 (0.98 to 1.25) | 0.12 | |
| To what extent do you agree or disagree that you have enough information from the Government and other public authorities with regards to…self-isolation | Strongly agree | 34.6 (6885) | 65.4 (13,020) | Reference | - |
| Agree | 34.5 (12,881) | 65.5 (24,504) | 1.00 (0.96 to 1.04) | 0.88 | |
| Neither agree nor disagree | 50.2 (4995) | 49.8 (4952) | 0.63 (0.59 to 0.66) | <0.001 * | |
| Disagree | 36.7 (2173) | 63.3 (3747) | 0.94 (0.88 to 1.01) | 0.08 | |
| Strongly Disagree | 47.9 (820) | 52.1 (893) | 0.69 (0.62 to 0.77) | <0.001 * | |
| Don’t know | 62.3 (379) | 37.7 (229) | 0.45 (0.38 to 0.53) | <0.001 * |
| The Government Has Issued Advice on How People Should Help Prevent the Spread of Coronavirus if They Have Symptoms | If You Have Symptoms of Coronavirus, You [Total n = 1988] | If Someone Develops Symptoms of Coronavirus, They [Total n = 2011] | p | ||||
|---|---|---|---|---|---|---|---|
| True, % (n) | False, % (n) | Don’t Know, % (n) | True, % (n) | False, % (n) | Don’t Know, % (n) | ||
| Should self-isolate | 87.9 (1756) | 7.1 (142) | 5.0 (100) | 87.1 (1751) | 7.5 (150) | 5.5 (110) | 0.72 |
| Should get a test, but can go out as normal while you/they are waiting for the result | 15.3 (305) | 77.5 (1550) | 7.2 (144) | 15.6 (314) | 77.2 (1552) | 7.2 (145) | 0.95 |
| Could be eligible for self-isolation payments (if you/they are on benefits and/or a lower income and cannot work from home) | 61.3 (1225) | 10.7 (214) | 28.0 (560) | 63.1 (1268) | 9.7 (194) | 27.3 (548) | 0.40 |
| Can go out if your/their symptoms are mild | 8.3 (166) | 85.9 (1717) | 5.8 (116) | 7.5 (150) | 85.8 (1725) | 6.8 (136) | 0.30 |
| Can go to the shops for groceries/pharmacy † | 25.5 (510) | 69.4 (1387) | 5.1 (102) | 22.0 (442) | 71.5 (1437) | 6.6 (132) | 0.008 * |
| Can go to the shops for things other than groceries/pharmacy † | 19.1 (381) | 75.9 (1516) | 5.1 (101) | 17.8 (358) | 76.2 (1533) | 6.0 (120) | 0.30 |
| Can go for a walk or some other exercise | 29.7 (594) | 62.9 (1256) | 7.4 (148) | 25.6 (515) | 65.9 (1325) | 8.5 (171) | 0.01 * |
| Can go out to work if you/they cannot work from home | 23.5 (469) | 70.1 (1401) | 6.4 (128) | 20.4 (411) | 73.2 (1473) | 6.3 (127) | 0.06 |
| Can go out to help or provide care for a vulnerable person | 23.8 (475) | 69.5 (1390) | 6.7 (134) | 21.1 (425) | 69.5 (1398) | 9.3 (188) | 0.003 * |
| Can go out if you’re/they are wearing a face covering | 23.4 (468) | 70.8 (1415) | 5.8 (115) | 19.9 (401) | 73.5 (1479) | 6.5 (131) | 0.02 * |
| Can go out to meet up with friends and/or family that you/they don’t live with, indoors † | 12.6 (252) | 82.7 (1654) | 4.7 (93) | 12.0 (242) | 83.0 (1670) | 5.0 (100) | 0.78 |
| Can go out to meet up with friends and/or family that you/they don’t live with, outdoors | 22.0 (440) | 73.6 (1471) | 4.4 (88) | 19.4 (391) | 74.9 (1507) | 5.6 (113) | 0.04 * |
| Can go out to spend time outdoors for recreational purposes (including to sit in parks, etc.) | 26.8 (535) | 68.1 (1361) | 5.1 (102) | 24.3 (489) | 69.6 (1400) | 6.1 (123) | 0.10 |
| Can go out to get a test to see if you/they have coronavirus | 67.5 (1350) | 23.2 (463) | 9.3 (186) | 66.9 (1347) | 22.8 (458) | 10.3 (207) | 0.57 |
| Can have someone who you/they don’t live with over to your/their home † | 11.6 (231) | 83.5 (1670) | 4.9 (98) | 11.1 (223) | 82.7 (1663) | 6.2 (125) | 0.18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, L.E.; West, R.; Potts, H.W.W.; Amlȏt, R.; Fear, N.T.; Rubin, G.J.; Michie, S. Knowledge of Self-Isolation Rules in the UK for Those Who Have Symptoms of COVID-19: A Repeated Cross-Sectional Survey Study. Int. J. Environ. Res. Public Health 2023, 20, 1952. https://doi.org/10.3390/ijerph20031952
Smith LE, West R, Potts HWW, Amlȏt R, Fear NT, Rubin GJ, Michie S. Knowledge of Self-Isolation Rules in the UK for Those Who Have Symptoms of COVID-19: A Repeated Cross-Sectional Survey Study. International Journal of Environmental Research and Public Health. 2023; 20(3):1952. https://doi.org/10.3390/ijerph20031952
Chicago/Turabian StyleSmith, Louise E., Robert West, Henry W. W. Potts, Richard Amlȏt, Nicola T. Fear, G. James Rubin, and Susan Michie. 2023. "Knowledge of Self-Isolation Rules in the UK for Those Who Have Symptoms of COVID-19: A Repeated Cross-Sectional Survey Study" International Journal of Environmental Research and Public Health 20, no. 3: 1952. https://doi.org/10.3390/ijerph20031952
APA StyleSmith, L. E., West, R., Potts, H. W. W., Amlȏt, R., Fear, N. T., Rubin, G. J., & Michie, S. (2023). Knowledge of Self-Isolation Rules in the UK for Those Who Have Symptoms of COVID-19: A Repeated Cross-Sectional Survey Study. International Journal of Environmental Research and Public Health, 20(3), 1952. https://doi.org/10.3390/ijerph20031952