

Enhancing Visual Exploration through Augmented Gaze: High Acceptance of Immersive Virtual Biking by Oldest Olds

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
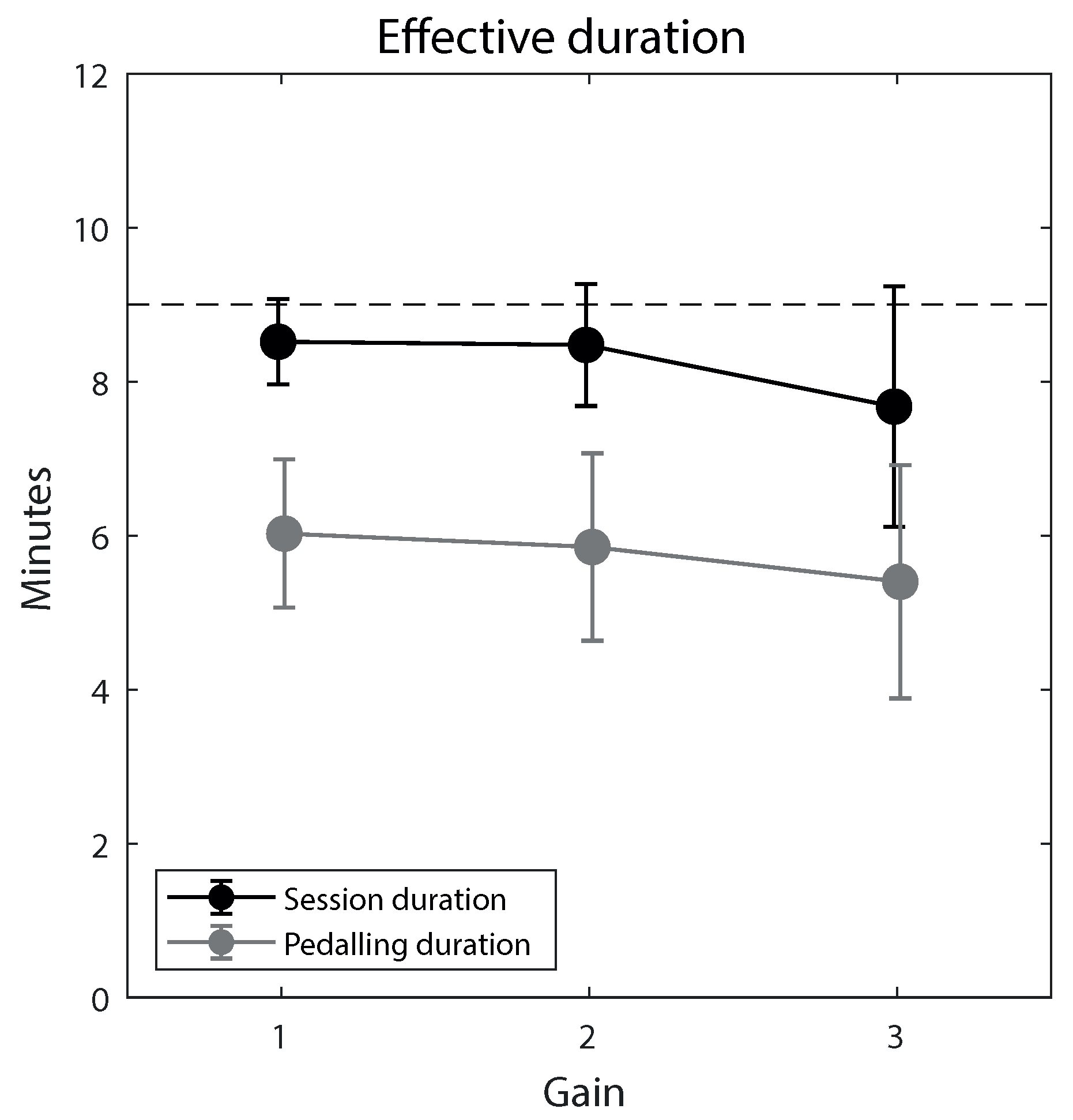
2.3. Session Duration and Pedaling Duration
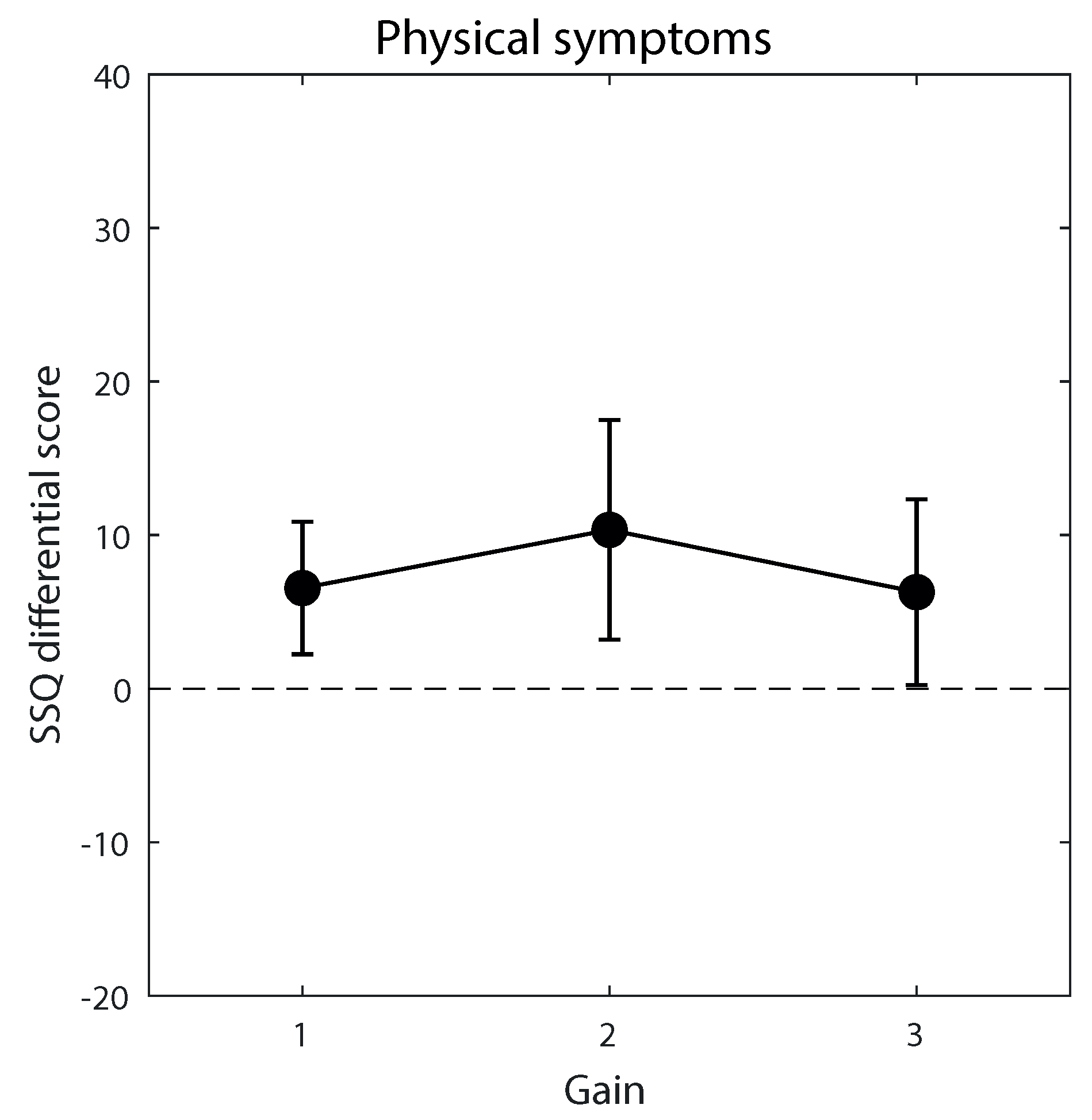
2.4. Cybersickness Symptoms
2.5. User Experience Ratings
2.6. Head Movement
2.7. Data Analysis
3. Results
3.1. Participants’ Acceptance
3.2. Effects of Gain



4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HMD | Head-Mounted Display |
| LW | Leftward |
| MMSE | Mini-Mental State Examination |
| M | Mean |
| RW | Rightward |
| SD | Standard Deviation |
| SSQ | Simulator Sickness Questionnaire |
| TV | Television |
| Vif | Variance Inflation Parameter |
| VR | Virtual Reality |
References
- Sokolov, A.A.; Collignon, A.; Bieler-Aeschlimann, M. Serious video games and virtual reality for prevention and neurorehabilitation of cognitive decline because of aging and neurodegeneration. Curr. Opin. Neurol. 2020, 33, 239–248. [Google Scholar] [CrossRef]
- Vailati Riboni, F.; Comazzi, B.; Bercovitz, K.; Castelnuovo, G.; Molinari, E.; Pagnini, F. Technologically-enhanced psychological interventions for older adults: A scoping review. BMC Geriatr. 2020, 20, 191. [Google Scholar] [CrossRef]
- Høeg, E.R.; Povlsen, T.M.; Bruun-Pedersen, J.R.; Lange, B.; Nilsson, N.C.; Haugaard, K.B.; Faber, S.M.; Hansen, S.W.; Kimby, C.K.; Serafin, S. System Immersion in Virtual Reality-Based Rehabilitation of Motor Function in Older Adults: A Systematic Review and Meta-Analysis. Front. Virtual Real. 2021, 2, 30. [Google Scholar] [CrossRef]
- Nishchyk, A.; Chen, W.; Pripp, A.H.; Bergland, A. The effect of mixed reality technologies for falls prevention among older adults: Systematic review and meta-analysis. JMIR Aging 2021, 4, e27972. [Google Scholar] [CrossRef]
- Sakaki, K.; Nouchi, R.; Matsuzaki, Y.; Saito, T.; Dinet, J.; Kawashima, R. Benefits of VR Physical Exercise on Cognition in Older Adults with and without Mild Cognitive Decline: A Systematic Review of Randomized Controlled Trials. Healthcare 2021, 9, 883. [Google Scholar] [CrossRef]
- Astasio-Picado, Á.; Cobos-Moreno, P.; Gómez-Martín, B.; Verdú-Garcés, L.; Zabala-Baños, M.d.C. Efficacy of Interventions Based on the Use of Information and Communication Technologies for the Promotion of Active Aging. Int. J. Environ. Res. Public Health 2022, 19, 1534. [Google Scholar] [CrossRef]
- Balki, E.; Hayes, N.; Holland, C. Effectiveness of technology interventions in addressing social isolation, connectedness, and loneliness in older adults: Systematic umbrella review. JMIR Aging 2022, 5, e40125. [Google Scholar] [CrossRef]
- Skurla, M.D.; Rahman, A.T.; Salcone, S.; Mathias, L.; Shah, B.; Forester, B.P.; Vahia, I.V. Virtual reality and mental health in older adults: A systematic review. Int. Psychogeriatr. 2022, 34, 143–155. [Google Scholar] [CrossRef]
- Tam, A.C.Y.; Chan, A.W.Y.; Cheung, D.S.K.; Ho, L.Y.W.; Tang, A.S.K.; Christensen, M.; Tse, M.M.Y.; Kwan, R.Y.C. The effects of interventions to enhance cognitive and physical functions in older people with cognitive frailty: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2022, 19, 1–15. [Google Scholar] [CrossRef]
- Bruun-Pedersen, J.R.; Serafin, S.; Kofoed, L.B. Going Outside while Staying Inside-Exercise Motivation with Immersive vs. Non-immersive Recreational Virtual Environment Augmentation for Older Adult Nursing Home Residents. In Proceedings of the 2016 IEEE International Conference on Healthcare Informatics, ICHI 2016, Chicago, IL, USA, 4–7 October 2016; pp. 216–226. [Google Scholar] [CrossRef]
- Pedroli, E.; Greci, L.; Colombo, D.; Serino, S.; Cipresso, P.; Arlati, S.; Mondellini, M.; Boilini, L.; Giussani, V.; Goulene, K.; et al. Characteristics, usability, and users experience of a system combining cognitive and physical therapy in a virtual environment: Positive bike. Sensors 2018, 18, 2343. [Google Scholar] [CrossRef]
- Arlati, S.; Colombo, V.; Spoladore, D.; Greci, L.; Pedroli, E.; Serino, S.; Cipresso, P.; Goulene, K.; Stramba-Badiale, M.; Riva, G.; et al. A social virtual reality-based application for the physical and cognitive training of the elderly at home. Sensors 2019, 19, 261. [Google Scholar] [CrossRef]
- Høeg, E.R.; Bruun-Pedersen, J.R.; Cheary, S.; Andersen, L.K.; Paisa, R.; Serafin, S.; Lange, B. Buddy biking: A user study on social collaboration in a virtual reality exergame for rehabilitation. Virtual Real. 2021, 1, 1–18. [Google Scholar] [CrossRef]
- Ortet, C.P.; Veloso, A.I.; Vale Costa, L. Cycling through 360° Virtual Reality Tourism for Senior Citizens: Empirical Analysis of an Assistive Technology. Sensors 2022, 22, 6169. [Google Scholar] [CrossRef]
- Ramiro, S.; van Tubergen, A.; Stolwijk, C.; van der Heijde, D.; Royston, P.; Landewé, R. Reference intervals of spinal mobility measures in normal individuals: The MOBILITY study. Ann. Rheum. Dis. 2015, 74, 1218–1224. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Frederiksen, H.; Christensen, K. Back and neck pain in seniors—Prevalence and impact. Eur. Spine J. 2006, 15, 802–806. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.A.; Hoy, D.; Buchbinder, R.; Mansournia, M.A.; Bettampadi, D.; Ashrafi-Asgarabad, A.; Almasi-Hashiani, A.; Smith, E.; Sepidarkish, M.; et al. Global, regional, and national burden of neck pain in the general population, 1990–2017: Systematic analysis of the global burden of disease study 2017. Bmj 2020, 368, m791. [Google Scholar] [CrossRef]
- Knight, J.F.; Baber, C. Effect of head-mounted displays on posture. Hum. Factors 2007, 49, 797–807. [Google Scholar] [CrossRef]
- Ragan, E.D.; Scerbo, S.; Bacim, F.; Bowman, D.A. Amplified Head Rotation in Virtual Reality and the Effects on 3D Search, Training Transfer, and Spatial Orientation. IEEE Trans. Vis. Comput. Graph. 2017, 23, 1880–1895. [Google Scholar] [CrossRef]
- Wright, W.G. Using virtual reality to augment perception, enhance sensorimotor adaptation, and change our minds. Front. Syst. Neurosci. 2014, 8, 56. [Google Scholar] [CrossRef]
- Stratton, G.M. Some preliminary experiments on vision without inversion of the retinal image. Psychol. Rev. 1896, 3, 611. [Google Scholar] [CrossRef]
- Stratton, G.M. Vision without inversion of the retinal image. Psychol. Rev. 1897, 4, 341. [Google Scholar] [CrossRef]
- Fernández-Ruiz, J.; Hall, C.; Vergara, P.; Dıaz, R. Prism adaptation in normal aging: Slower adaptation rate and larger aftereffect. Cogn. Brain Res. 2000, 9, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Seidler, R.D. Differential effects of age on sequence learning and sensorimotor adaptation. Brain Res. Bull. 2006, 70, 337–346. [Google Scholar] [CrossRef]
- Seidler, R.D.; Bernard, J.A.; Burutolu, T.B.; Fling, B.W.; Gordon, M.T.; Gwin, J.T.; Kwak, Y.; Lipps, D.B. Motor control and aging: Links to age-related brain structural, functional, and biochemical effects. Neurosci. Biobehav. Rev. 2010, 34, 721–733. [Google Scholar] [CrossRef]
- Golding, J.F. Motion sickness. In Handbook of Clinical Neurology; Elsevier B.V.: Amsterdam, The Netherlands, 2016; Volume 137, pp. 371–390. [Google Scholar] [CrossRef]
- Howard, M.C.; Van Zandt, E.C. A meta-analysis of the virtual reality problem: Unequal effects of virtual reality sickness across individual differences. Virtual Real. 2021, 25, 1221–1246. [Google Scholar] [CrossRef]
- Jang, W.; Shin, J.H.; Kim, M.; Kim, K.K. Human field of regard, field of view, and attention bias. Comput. Methods Programs Biomed. 2016, 135, 115–123. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Bimberg, P.; Weissker, T.; Kulik, A. On the usage of the simulator sickness questionnaire for virtual reality research. In Proceedings of the 2020 IEEE conference on virtual reality and 3D user interfaces abstracts and workshops (VRW), Atlanta, GA, USA, 22–26 March 2020; pp. 464–467. [Google Scholar]
- Marston, H.R.; Freeman, S.; Bishop, K.A.; Beech, C.L. A Scoping Review of Digital Gaming Research Involving Older Adults Aged 85 and Older. Games Health J. 2016, 5, 157–174. [Google Scholar] [CrossRef]
- He, W.; Goodkind, D.; Kowal, P.R. An Aging World: 2015. 2016. Available online: https://www.census.gov/content/dam/Census/library/publications/2016/demo/p95-16-1.pdf (accessed on 13 November 2022).
- Minsky, M. Telepresence. OMNI Mag. 1980, 2, 44–52. [Google Scholar]
- Peters, D.; Calvo, R.A.; Ryan, R.M. Designing for Motivation, Engagement and Wellbeing in Digital Experience. Front. Psychol. 2018, 9, 797. [Google Scholar] [CrossRef]
- Young, S.D.; Adelstein, B.D.; Ellis, S.R. Demand characteristics in assessing motion sickness in a virtual environment: Or does taking a motion sickness questionnaire make you sick? IEEE Trans. Vis. Comput. Graph. 2007, 13, 422–428. [Google Scholar] [CrossRef] [PubMed]
- de’Sperati, C.; Granato, M.; Moretti, M. If You Are Old, Videos Look Slow. The Paradoxical Effect of Age-Related Motor Decline on the Kinematic Interpretation of Visual Scenes. Front. Hum. Neurosci. 2022, 15, 791. [Google Scholar] [CrossRef]
- Engel-Yeger, B.; Rosenblum, S. Executive dysfunctions mediate between altered sensory processing and daily activity performance in older adults. BMC Geriatr. 2021, 21, 132. [Google Scholar] [CrossRef] [PubMed]
- Emery, N.J. The eyes have it: The neuroethology, function and evolution of social gaze. Neurosci. Biobehav. Rev. 2000, 24, 581–604. [Google Scholar] [CrossRef] [PubMed]
- Csibra, G.; Gergely, G. Natural pedagogy. Trends Cogn. Sci. 2009, 13, 148–153. [Google Scholar] [CrossRef]
- Becchio, C.; Sartori, L.; Castiello, U. Toward you: The social side of actions. Curr. Dir. Psychol. Sci. 2010, 19, 183–188. [Google Scholar] [CrossRef]
- Trujillo, J.P.; Simanova, I.; Bekkering, H.; Özyürek, A. Communicative intent modulates production and comprehension of actions and gestures: A Kinect study. Cognition 2018, 180, 38–51. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Characteristics | M | SD |
|---|---|---|
| AGE (years) | 89.8 | 7.2 |
| MMSE (score) | 22.7 | 4.9 |
| TINETTI (score) | 17.1 | 5.5 |
| STAY TIME (months) | 20.9 | 16.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de’Sperati, C.; Dalmasso, V.; Moretti, M.; Høeg, E.R.; Baud-Bovy, G.; Cozzi, R.; Ippolito, J. Enhancing Visual Exploration through Augmented Gaze: High Acceptance of Immersive Virtual Biking by Oldest Olds. Int. J. Environ. Res. Public Health 2023, 20, 1671. https://doi.org/10.3390/ijerph20031671
de’Sperati C, Dalmasso V, Moretti M, Høeg ER, Baud-Bovy G, Cozzi R, Ippolito J. Enhancing Visual Exploration through Augmented Gaze: High Acceptance of Immersive Virtual Biking by Oldest Olds. International Journal of Environmental Research and Public Health. 2023; 20(3):1671. https://doi.org/10.3390/ijerph20031671
Chicago/Turabian Stylede’Sperati, Claudio, Vittorio Dalmasso, Michela Moretti, Emil Rosenlund Høeg, Gabriel Baud-Bovy, Roberto Cozzi, and Jacopo Ippolito. 2023. "Enhancing Visual Exploration through Augmented Gaze: High Acceptance of Immersive Virtual Biking by Oldest Olds" International Journal of Environmental Research and Public Health 20, no. 3: 1671. https://doi.org/10.3390/ijerph20031671
APA Stylede’Sperati, C., Dalmasso, V., Moretti, M., Høeg, E. R., Baud-Bovy, G., Cozzi, R., & Ippolito, J. (2023). Enhancing Visual Exploration through Augmented Gaze: High Acceptance of Immersive Virtual Biking by Oldest Olds. International Journal of Environmental Research and Public Health, 20(3), 1671. https://doi.org/10.3390/ijerph20031671